
Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture

 ,
,  ,
,
Abstract
:1. Introduction
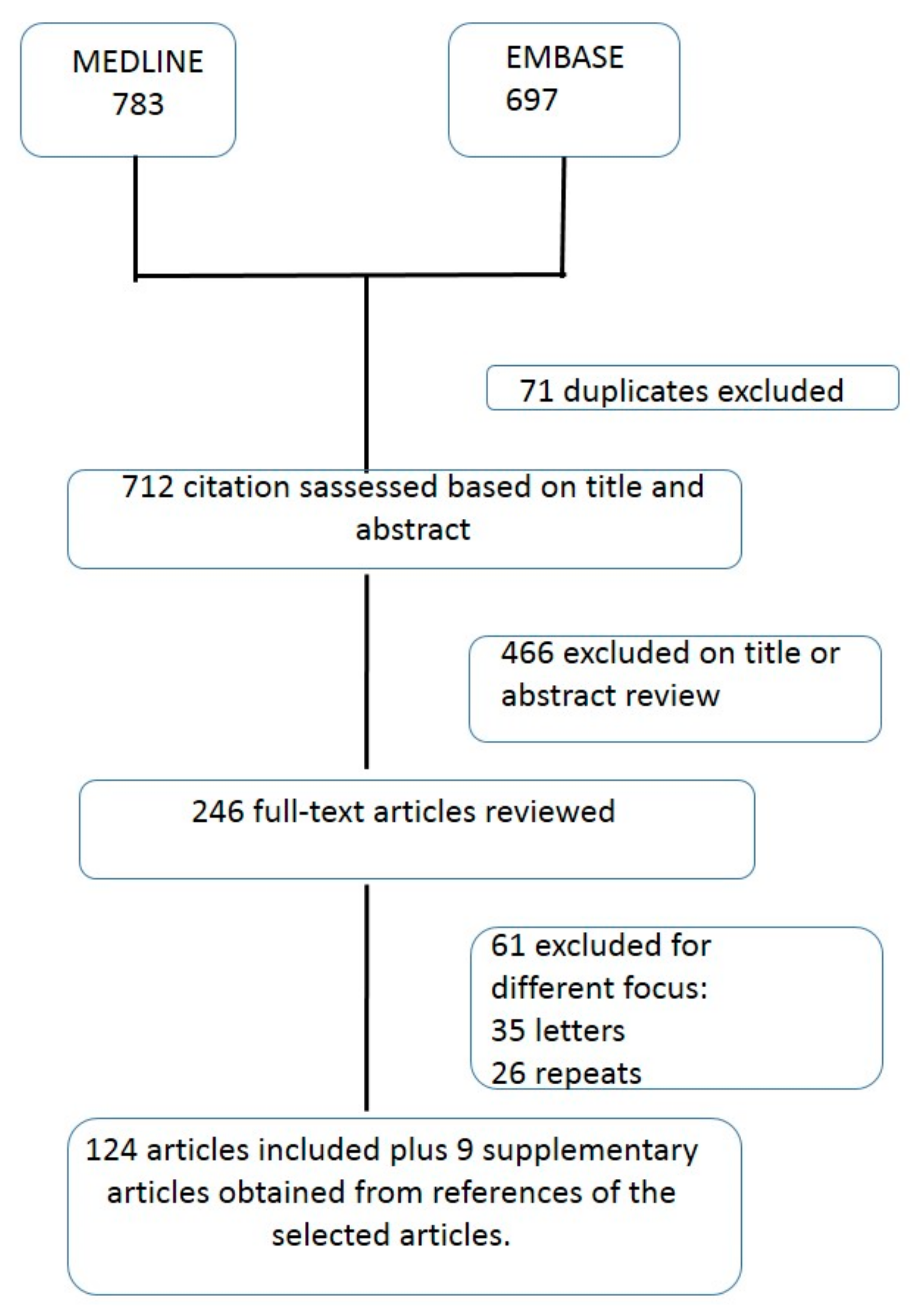
2. Methods
3. Results
3.1. Geriatric Syndromes
Delirium
3.2. Cognitive Impairment
3.3. Mood Disorders and Depression
3.3.1. Urinary Incontinence
3.3.2. Constipation
4. Malnutrition
4.1. Sarcopenia
4.2. Frailty
4.3. Pressure Sores
5. Polypharmacy
6. Perioperative Care
6.1. Renal Function
6.2. Anemia and Patients Blood Management
6.3. Pain Management
Functional Recovery
7. Prognostic Factors and Mortality
8. Costs
9. Future Perspectives and Lines of Research
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnell, O.; Kanis, J.A. An Estimate of the Worldwide Prevalence, Mortality and Disability Associated with Hip Fracture. Osteoporos. Int. 2004, 15, 897–902. [Google Scholar] [CrossRef]
- Cooper, C.; Campion, G.; Melton, L.J. Hip Fractures in the Elderly: A World-Wide Projection. Osteoporos. Int. 1992, 2, 285–289. [Google Scholar] [CrossRef]
- Lauritzen, J.B.; Schwarz, P.; Lund, B.; McNair, P.; Transbøl, I. Changing Incidence and Residual Lifetime Risk of Common Osteoporosis-Related Fractures. Osteoporos. Int. 1993, 3, 127–132. [Google Scholar] [CrossRef]
- Aschkenasy, M.T.; Rothenhaus, T.C. Trauma and Falls in the Elderly. Emerg. Med. Clin. N. Am. 2006, 24, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Roche, J.J.W.; Wenn, R.T.; Sahota, O.; Moran, C.G. Effect of Comorbidities and Postoperative Complications on Mortality after Hip Fracture in Elderly People: Prospective Observational Cohort Study. BMJ 2005, 331, 1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, A.H.; Zuckerman, J.D.; AAOS Council of Health Policy and Practice, USA. American Academy of Orthopaedic Surgeons National Consensus Conference on Improving the Continuum of Care for Patients with Hip Fracture. J. Bone Jt. Surg. Am. 2002, 84, 670–674. [Google Scholar] [CrossRef]
- Hawley, S.; Javaid, M.K.; Prieto-Alhambra, D.; Lippett, J.; Sheard, S.; Arden, N.K.; Cooper, C.; Judge, A.; REFReSH Study Group. Clinical Effectiveness of Orthogeriatric and Fracture Liaison Service Models of Care for Hip Fracture Patients: Population-Based Longitudinal Study. Age Ageing 2016, 45, 236–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigoryan, K.V.; Javedan, H.; Rudolph, J.L. Orthogeriatric Care Models and Outcomes in Hip Fracture Patients: A Systematic Review and Meta-Analysis. J. Orthop. Trauma 2014, 28, e49–e55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertram, M.; Norman, R.; Kemp, L.; Vos, T. Review of the Long-Term Disability Associated with Hip Fractures. Inj. Prev. 2011, 17, 365–370. [Google Scholar] [CrossRef]
- Braithwaite, R.S.; Col, N.F.; Wong, J.B. Estimating Hip Fracture Morbidity, Mortality and Costs. J. Am. Geriatr. Soc. 2003, 51, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Magaziner, J.; Hawkes, W.; Hebel, J.R.; Zimmerman, S.I.; Fox, K.M.; Dolan, M.; Felsenthal, G.; Kenzora, J. Recovery from Hip Fracture in Eight Areas of Function. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M498–M507. [Google Scholar] [CrossRef]
- Leibson, C.L.; Tosteson, A.N.A.; Gabriel, S.E.; Ransom, J.E.; Melton, L.J. Mortality, Disability, and Nursing Home Use for Persons with and without Hip Fracture: A Population-Based Study. J. Am. Geriatr. Soc. 2002, 50, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Devas, M. Geriatric Orthopaedics; Academic Press: London, UK, 1977. [Google Scholar]
- Sabharwal, S.; Wilson, H. Orthogeriatrics in the Management of Frail Older Patients with a Fragility Fracture. Osteoporos. Int. 2015, 26, 2387–2399. [Google Scholar] [CrossRef] [PubMed]
- Khasraghi, F.A.; Christmas, C.; Lee, E.J.; Mears, S.C.; Wenz, J.F. Effectiveness of a Multidisciplinary Team Approach to Hip Fracture Management. J. Surg. Orthop. Adv. 2005, 14, 27–31. [Google Scholar]
- Vidán, M.; Serra, J.A.; Moreno, C.; Riquelme, G.; Ortiz, J. Efficacy of a Comprehensive Geriatric Intervention in Older Patients Hospitalized for Hip Fracture: A Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2005, 53, 1476–1482. [Google Scholar] [CrossRef]
- Friedman, S.M.; Mendelson, D.A.; Bingham, K.W.; Kates, S.L. Impact of a Comanaged Geriatric Fracture Center on Short-Term Hip Fracture Outcomes. Arch. Intern. Med. 2009, 169, 1712–1717. [Google Scholar] [CrossRef] [Green Version]
- Tarazona-Santabalbina, F.J.; Belenguer-Varea, Á.; Rovira, E.; Cuesta-Peredó, D. Orthogeriatric Care: Improving Patient Outcomes. Clin. Interv. Aging 2016, 11, 843–856. [Google Scholar] [CrossRef] [Green Version]
- De Rui, M.; Veronese, N.; Manzato, E.; Sergi, G. Role of Comprehensive Geriatric Assessment in the Management of Osteoporotic Hip Fracture in the Elderly: An Overview. Disabil. Rehabil. 2013, 35, 758–765. [Google Scholar] [CrossRef]
- Pillai, A.; Eranki, V.; Shenoy, R.; Hadidi, M. Age Related Incidence and Early Outcomes of Hip Fractures: A Prospective Cohort Study of 1177 Patients. J. Orthop. Surg. Res. 2011, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, H.; Harding, K.; Sahota, O. Best Practice Tariff for Hip Fracture-Making Ends Meet. British Geriatrics Society Newsletter. June 2010. Available online: https://www.bgs.org.uk/?option=com_content&view=article&id=700%3Atariffhipfracture&catid=47%3Afallsandbones&Itemid=307 (accessed on 12 October 2020).
- Payment by Results Guidance for 2013–2014. Available online: https://www.gov.uk/government/publications/payment-by-results-pbr-operational-guidance-and-tariffs (accessed on 12 October 2020).
- National Institute for Health and Care Excellence Quality Standards for Hip Fracture 2012. Available online: https://www.nice.org.uk/guidance/qs16 (accessed on 9 November 2020).
- Fernandez, M.A.; Griffin, X.L.; Costa, M.L. Management of Hip Fracture. Br. Med. Bull. 2015, 115, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Komadina, R.; Wendt, K.W.; Holzer, G.; Kocjan, T. Outcome Parameters in Orthogeriatric Co-management—A Mini-Review. Wien. Klin. Wochenschr. 2016, 128, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Liem, I.S.; Kammerlander, C.; Suhm, N.; Blauth, M.; Roth, T.; Gosch, M.; Hoang-Kim, A.; Mendelson, D.; Zuckerman, J.; Leung, F.; et al. Identifying a Standard Set of Outcome Parameters for the Evaluation of Orthogeriatric Co-Management for Hip Fractures. Injury 2013, 44, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Baroni, M.; Serra, R.; Boccardi, V.; Ercolani, S.; Zengarini, E.; Casucci, P.; Valecchi, R.; Rinonapoli, G.; Caraffa, A.; Mecocci, P.; et al. The Orthogeriatric Comanagement Improves Clinical Outcomes of Hip Fracture in Older Adults. Osteoporos. Int. 2019, 30, 907–916. [Google Scholar] [CrossRef]
- Ojeda-Thies, C.; Sáez-López, P.; Currie, C.T.; Tarazona-Santalbina, F.J.; Alarcón, T.; Muñoz-Pascual, A.; Pareja, T.; Gómez-Campelo, P.; Montero-Fernández, N.; Mora-Fernández, J.; et al. Spanish National Hip Fracture Registry (RNFC): Analysis of Its First Annual Report and International Comparison with Other Established Registries. Osteoporos. Int. 2019, 30, 1243–1254. [Google Scholar] [CrossRef] [PubMed]
- Pincus, D.; Ravi, B.; Wasserstein, D.; Huang, A.; Paterson, J.M.; Nathens, A.B.; Kreder, H.J.; Jenkinson, R.J.; Wodchis, W.P. Association Between Wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery. JAMA 2017, 318, 1994–2003. [Google Scholar] [CrossRef] [Green Version]
- Aletto, C.; Aicale, R.; Pezzuti, G.; Bruno, F.; Maffulli, N. Impact of an Orthogeriatrician on Length of Stay of Elderly Patient with Hip Fracture. Osteoporos. Int. 2020, 31, 2161–2166. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-N.; Su, S.-F.; Yeh, W.-T. Meta-Analysis: Effectiveness of Comprehensive Geriatric Care for Elderly Following Hip Fracture Surgery. West. J. Nurs. Res. 2020, 42, 293–305. [Google Scholar] [CrossRef]
- Talevski, J.; Sanders, K.M.; Duque, G.; Connaughton, C.; Beauchamp, A.; Green, D.; Millar, L.; Brennan-Olsen, S.L. Effect of Clinical Care Pathways on Quality of Life and Physical Function After Fragility Fracture: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 926.e1–926.e11. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, X.; Gao, L.; Wang, Y.; Wang, J. Incidence and Associated Factors of Delirium after Orthopedic Surgery in Elderly Patients: A Systematic Review and Meta-Analysis. Aging Clin. Exp. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Poeran, J.; Cozowicz, C.; Zubizarreta, N.; Weinstein, S.M.; Deiner, S.G.; Leipzig, R.M.; Friedman, J.I.; Liu, J.; Mazumdar, M.; Memtsoudis, S.G. Modifiable Factors Associated with Postoperative Delirium after Hip Fracture Repair: An Age-Stratified Retrospective Cohort Study. Eur. J. Anaesthesiol. 2020, 37, 649–658. [Google Scholar] [CrossRef]
- Tao, L.; Xiaodong, X.; Qiang, M.; Jiao, L.; Xu, Z. Prediction of Postoperative Delirium by Comprehensive Geriatric Assessment among Elderly Patients with Hip Fracture. Ir. J. Med. Sci. 2019, 188, 1311–1315. [Google Scholar] [CrossRef]
- Aldwikat, R.K.; Manias, E.; Nicholson, P. Incidence and Risk Factors for Acute Delirium in Older Patients with a Hip Fracture: A Retrospective Cohort Study. Nurs. Health Sci. 2020, 22, 958–966. [Google Scholar] [CrossRef]
- Pioli, G.; Bendini, C.; Giusti, A.; Pignedoli, P.; Cappa, M.; Iotti, E.; Ferri, M.A.; Bergonzini, E.; Sabetta, E. Surgical Delay Is a Risk Factor of Delirium in Hip Fracture Patients with Mild-Moderate Cognitive Impairment. Aging Clin. Exp. Res. 2019, 31, 41–47. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, X.; Dong, T.; Yang, Z.; Zhang, Q.; Zhang, Y. Risk Factors for Postoperative Delirium Following Hip Fracture Repair in Elderly Patients: A Systematic Review and Meta-Analysis. Aging Clin. Exp. Res. 2017, 29, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.O.; Cooper, A.; Peryer, G.; Griffiths, R.; Fox, C.; Cross, J. Factors Predicting Incidence of Post-Operative Delirium in Older People Following Hip Fracture Surgery: A Systematic Review and Meta-Analysis. Int. J. Geriatr. Psychiatry 2017, 32, 386–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, G.M.; Wheeler, K.; Di Michele, J.; Lalu, M.M.; McIsaac, D.I. A Systematic Review and Meta-Analysis Examining the Impact of Incident Postoperative Delirium on Mortality. Anesthesiology 2017, 127, 78–88. [Google Scholar] [CrossRef]
- Mazzola, P.; Ward, L.; Zazzetta, S.; Broggini, V.; Anzuini, A.; Valcarcel, B.; Brathwaite, J.S.; Pasinetti, G.M.; Bellelli, G.; Annoni, G. Association Between Preoperative Malnutrition and Postoperative Delirium After Hip Fracture Surgery in Older Adults. J. Am. Geriatr. Soc. 2017, 65, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Monacelli, F.; Pizzonia, M.; Signori, A.; Nencioni, A.; Giannotti, C.; Minaglia, C.; Granello di Casaleto, T.; Podestà, S.; Santolini, F.; Odetti, P. The In-Hospital Length of Stay after Hip Fracture in Octogenarians: Do Delirium and Dementia Shape a New Care Process? J. Alzheimers Dis. 2018, 66, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Radinovic, K.S.; Markovic-Denic, L.; Dubljanin-Raspopovic, E.; Marinkovic, J.; Jovanovic, L.B.; Bumbasirevic, V. Effect of the Overlap Syndrome of Depressive Symptoms and Delirium on Outcomes in Elderly Adults with Hip Fracture: A Prospective Cohort Study. J. Am. Geriatr. Soc. 2014, 62, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Shields, L.; Henderson, V.; Caslake, R. Comprehensive Geriatric Assessment for Prevention of Delirium after Hip Fracture: A Systematic Review of Randomized Controlled Trials. J. Am. Geriatr. Soc. 2017, 65, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tang, J.; Zhou, F.; Yang, L.; Wu, J. Comprehensive Geriatric Care Reduces Acute Perioperative Delirium in Elderly Patients with Hip Fractures: A Meta-Analysis. Medicine (Baltimore) 2017, 96, e7361. [Google Scholar] [CrossRef]
- Ravi, B.; Pincus, D.; Choi, S.; Jenkinson, R.; Wasserstein, D.N.; Redelmeier, D.A. Association of Duration of Surgery With Postoperative Delirium Among Patients Receiving Hip Fracture Repair. JAMA Netw. Open 2019, 2, e190111. [Google Scholar] [CrossRef] [Green Version]
- Hack, J.; Eschbach, D.; Aigner, R.; Oberkircher, L.; Ruchholtz, S.; Bliemel, C.; Buecking, B. Medical Complications Predict Cognitive Decline in Nondemented Hip Fracture Patients-Results of a Prospective Observational Study. J. Geriatr. Psychiatry Neurol. 2018, 31, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Seitz, D.P.; Adunuri, N.; Gill, S.S.; Rochon, P.A. Prevalence of Dementia and Cognitive Impairment among Older Adults with Hip Fractures. J. Am. Med. Dir. Assoc. 2011, 12, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Yiannopoulou, K.G.; Anastasiou, I.P.; Ganetsos, T.K.; Efthimiopoulos, P.; Papageorgiou, S.G. Prevalence of Dementia in Elderly Patients with Hip Fracture. Hip. Int. 2012, 22, 209–213. [Google Scholar] [CrossRef]
- Delgado, A.; Cordero, G.-G.E.; Marcos, S.; Cordero-Ampuero, J. Influence of Cognitive Impairment on Mortality, Complications and Functional Outcome after Hip Fracture: Dementia as a Risk Factor for Sepsis and Urinary Infection. Injury 2020, 51 (Suppl. 1), S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Tarazona-Santabalbina, F.J.; Belenguer-Varea, Á.; Rovira Daudi, E.; Salcedo Mahiques, E.; Cuesta Peredó, D.; Doménech-Pascual, J.R.; Gac Espínola, H.; Avellana Zaragoza, J.A. Severity of Cognitive Impairment as a Prognostic Factor for Mortality and Functional Recovery of Geriatric Patients with Hip Fracture. Geriatr. Gerontol. Int. 2015, 15, 289–295. [Google Scholar] [CrossRef]
- Tang, V.L.; Sudore, R.; Cenzer, I.S.; Boscardin, W.J.; Smith, A.; Ritchie, C.; Wallhagen, M.; Finlayson, E.; Petrillo, L.; Covinsky, K. Rates of Recovery to Pre-Fracture Function in Older Persons with Hip Fracture: An Observational Study. J. Gen. Intern. Med. 2017, 32, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshii, I.; Satake, Y.; Kitaoka, K.; Komatsu, M.; Hashimoto, K. Relationship between Dementia Degree and Gait Ability after Surgery of Proximal Femoral Fracture: Review from Clinical Pathway with Regional Alliance Data of Rural Region in Japan. J. Orthop. Sci. 2016, 21, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Zerah, L.; Cohen-Bittan, J.; Raux, M.; Meziere, A.; Tourette, C.; Neri, C.; Verny, M.; Riou, B.; Khiami, F.; Boddaert, J. Association between Cognitive Status before Surgery and Outcomes in Elderly Patients with Hip Fracture in a Dedicated Orthogeriatric Care Pathway. J. Alzheimers Dis. 2017, 56, 145–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibasaki, K.; Asahi, T.; Mizobuchi, K.; Akishita, M.; Ogawa, S. Rehabilitation Strategy for Hip Fracture, Focused on Behavioral Psychological Symptoms of Dementia for Older People with Cognitive Impairment: A Nationwide Japan Rehabilitation Database. PLoS ONE 2018, 13, e0200143. [Google Scholar] [CrossRef] [PubMed]
- Romero Pisonero, E.; Mora Fernández, J. Multidisciplinary geriatric rehabilitation in the patient with hip fracture and dementia. Rev. Esp. Geriatr. Gerontol. 2019, 54, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Ogunwale, A.N.; Colon-Emeric, C.S.; Sloane, R.; Adler, R.A.; Lyles, K.W.; Lee, R.H. Acetylcholinesterase Inhibitors Are Associated with Reduced Fracture Risk among Older Veterans with Dementia. J. Bone Miner. Res. 2020, 35, 440–445. [Google Scholar] [CrossRef]
- Wu, Q.; Liu, J.; Gallegos-Orozco, J.F.; Hentz, J.G. Depression, Fracture Risk, and Bone Loss: A Meta-Analysis of Cohort Studies. Osteoporos. Int. 2010, 21, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- van de Ree, C.L.P.; de Munter, L.; Biesbroeck, B.H.H.; Kruithof, N.; Gosens, T.; de Jongh, M.A.C. The Prevalence and Prognostic Factors of Psychological Distress in Older Patients with a Hip Fracture: A Longitudinal Cohort Study. Injury 2020, 51, 2668–2675. [Google Scholar] [CrossRef] [PubMed]
- Charles-Lozoya, S.; Cobos-Aguilar, H.; Barba-Gutiérrez, E.; Brizuela-Ventura, J.M.; Chávez-Valenzuela, S.; García-Hernández, A.; Tamez-Montes, J.C. Depression and Geriatric Assessment in Older People Admitted for Hip Fracture. Rev. Med. Chil. 2019, 147, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Tseng, M.-Y.; Shyu, Y.-I.L.; Liang, J.; Tsai, W.-C. Interdisciplinary Intervention Reduced the Risk of Being Persistently Depressive among Older Patients with Hip Fracture. Geriatr. Gerontol. Int. 2016, 16, 1145–1152. [Google Scholar] [CrossRef]
- Zusman, E.Z.; McAllister, M.M.; Chen, P.; Guy, P.; Hanson, H.M.; Merali, K.; Brasher, P.M.A.; Cook, W.L.; Ashe, M.C. Incontinence and Nocturia in Older Adults After Hip Fracture: Analysis of a Secondary Outcome for a Parallel Group, Randomized Controlled Trial. Gerontol. Geriatr. Med. 2017, 3. [Google Scholar] [CrossRef] [Green Version]
- Schluter, P.J.; Askew, D.A.; Jamieson, H.A.; Arnold, E.P. Urinary and Fecal Incontinence Are Independently Associated with Falls Risk among Older Women and Men with Complex Needs: A National Population Study. Neurourol. Urodyn. 2020, 39, 945–953. [Google Scholar] [CrossRef]
- Nuotio, M.S.; Luukkaala, T.; Tammela, T. Elevated Post-Void Residual Volume in a Geriatric Post-Hip Fracture Assessment in Women-Associated Factors and Risk of Mortality. Aging Clin. Exp. Res. 2019, 31, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cialic, R.; Shvedov, V.; Lerman, Y. Risk Factors for Urinary Retention Following Surgical Repair of Hip Fracture in Female Patients. Geriatr. Orthop. Surg. Rehabil. 2017, 8, 39–43. [Google Scholar] [CrossRef] [Green Version]
- Morri, M.; Chiari, P.; Forni, C.; Orlandi Magli, A.; Gazineo, D.; Franchini, N.; Marconato, L.; Giamboi, T.; Cotti, A. What Factors Are Associated With the Recovery of Autonomy After a Hip Fracture? A Prospective, Multicentric Cohort Study. Arch. Phys. Med. Rehabil. 2018, 99, 893–899. [Google Scholar] [CrossRef]
- Trads, M.; Pedersen, P.U. Constipation and Defecation Pattern the First 30 Days after Hip Fracture. Int. J. Nurs. Pract. 2015, 21, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Trads, M.; Deutch, S.R.; Pedersen, P.U. Supporting Patients in Reducing Postoperative Constipation: Fundamental Nursing Care—A Quasi-Experimental Study. Scand. J. Caring Sci. 2018, 32, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Bohl, D.D.; Shen, M.R.; Hannon, C.P.; Fillingham, Y.A.; Darrith, B.; Della Valle, C.J. Serum Albumin Predicts Survival and Postoperative Course Following Surgery for Geriatric Hip Fracture. J. Bone Jt. Surg. Am. 2017, 99, 2110–2118. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Reginster, J.-Y.; Cabrerizo, S.; Bruyère, O.; Kanis, J.A.; Martinez, J.A.; Zulet, M.A. Nutritional Status and Nutritional Treatment Are Related to Outcomes and Mortality in Older Adults with Hip Fracture. Nutrients 2018, 10, 555. [Google Scholar] [CrossRef] [Green Version]
- Nuotio, M.; Tuominen, P.; Luukkaala, T. Association of Nutritional Status as Measured by the Mini-Nutritional Assessment Short Form with Changes in Mobility, Institutionalization and Death after Hip Fracture. Eur. J. Clin. Nutr. 2016, 70, 393–398. [Google Scholar] [CrossRef]
- Díaz de Bustamante, M.; Alarcón, T.; Menéndez-Colino, R.; Ramírez-Martín, R.; Otero, Á.; González-Montalvo, J.I. Prevalence of Malnutrition in a Cohort of 509 Patients with Acute Hip Fracture: The Importance of a Comprehensive Assessment. Eur. J. Clin. Nutr. 2018, 72, 77–81. [Google Scholar] [CrossRef]
- Helminen, H.; Luukkaala, T.; Saarnio, J.; Nuotio, M.S. Predictive Value of the Mini-Nutritional Assessment Short Form (MNA-SF) and Nutritional Risk Screening (NRS2002) in Hip Fracture. Eur. J. Clin. Nutr. 2019, 73, 112–120. [Google Scholar] [CrossRef]
- Inoue, T.; Misu, S.; Tanaka, T.; Kakehi, T.; Ono, R. Acute Phase Nutritional Screening Tool Associated with Functional Outcomes of Hip Fracture Patients: A Longitudinal Study to Compare MNA-SF, MUST, NRS-2002 and GNRI. Clin. Nutr. 2019, 38, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Koren-Hakim, T.; Weiss, A.; Hershkovitz, A.; Otzrateni, I.; Anbar, R.; Gross Nevo, R.F.; Schlesinger, A.; Frishman, S.; Salai, M.; Beloosesky, Y. Comparing the Adequacy of the MNA-SF, NRS-2002 and MUST Nutritional Tools in Assessing Malnutrition in Hip Fracture Operated Elderly Patients. Clin. Nutr. 2016, 35, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Wakabayashi, H.; Momosaki, R. Nutritional Status Changes and Activities of Daily Living after Hip Fracture in Convalescent Rehabilitation Units: A Retrospective Observational Cohort Study from the Japan Rehabilitation Nutrition Database. J. Acad. Nutr. Diet 2018, 118, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, G.; Katz, Y.; Shahar, D.R.; Bar, O.; Lehman, Y.; Spiegel, D.; Ochayon, Y.; Shavit, N.; Mimran Nahon, D.; Radinski, Y.; et al. Nutritional Status and Osteoporotic Fracture Rehabilitation Outcomes in Older Adults. J. Nutr. Gerontol. Geriatr. 2018, 37, 231–240. [Google Scholar] [CrossRef]
- Inoue, T.; Misu, S.; Tanaka, T.; Sakamoto, H.; Iwata, K.; Chuman, Y.; Ono, R. Pre-Fracture Nutritional Status Is Predictive of Functional Status at Discharge during the Acute Phase with Hip Fracture Patients: A Multicenter Prospective Cohort Study. Clin. Nutr. 2017, 36, 1320–1325. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp-Chalifour, P.; Belzile, E.L.; Racine, L.-C.; Nolet, M.-P.; Lemire, S.; Jean, S.; Pelet, S. The Long-Term Postoperative Trajectory of Geriatric Patients Admitted for a Hip Fracture: A Prospective Observational Cohort Study. Orthop. Traumatol. Surg. Res. 2020, 106, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Torbergsen, A.C.; Watne, L.O.; Frihagen, F.; Wyller, T.B.; Mowè, M. Effects of Nutritional Intervention upon Bone Turnover in Elderly Hip Fracture Patients. Randomized Controlled Trial. Clin. Nutr. ESPEN 2019, 29, 52–58. [Google Scholar] [CrossRef]
- Malafarina, V.; Malafarina, C.; Biain Ugarte, A.; Martinez, J.A.; Abete Goñi, I.; Zulet, M.A. Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study. Nutrients 2019, 11, 2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Montalvo, J.I.; Alarcón, T.; Gotor, P.; Queipo, R.; Velasco, R.; Hoyos, R.; Pardo, A.; Otero, A. Prevalence of Sarcopenia in Acute Hip Fracture Patients and Its Influence on Short-Term Clinical Outcome. Geriatr. Gerontol. Int. 2016, 16, 1021–1027. [Google Scholar] [CrossRef]
- Ha, Y.-C.; Won Won, C.; Kim, M.; Chun, K.-J.; Yoo, J.-I. SARC-F as a Useful Tool for Screening Sarcopenia in Elderly Patients with Hip Fractures. J. Nutr. Health Aging 2020, 24, 78–82. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Santoro, L.; Santoliquido, A.; Sisto, A.; Picca, A.; Marzetti, E. The Association between Sarcopenia and Functional Outcomes among Older Patients with Hip Fracture Undergoing In-Hospital Rehabilitation. Osteoporos. Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef]
- van de Ree, C.L.P.; Landers, M.J.F.; Kruithof, N.; de Munter, L.; Slaets, J.P.J.; Gosens, T.; de Jongh, M.A.C. Effect of Frailty on Quality of Life in Elderly Patients after Hip Fracture: A Longitudinal Study. BMJ Open 2019, 9, e025941. [Google Scholar] [CrossRef] [Green Version]
- Rajeev, A.; Anto, J. The Role of Edmonton Frailty Scale and Asa Grade in the Assessment of Morbidity and Mortality after Fracture Neck of Femur in Elderly. Acta Orthop. Belg. 2019, 85, 346–351. [Google Scholar]
- Winters, A.M.; Hartog, L.C.; Roijen, H.; Brohet, R.M.; Kamper, A.M. Relationship between Clinical Outcomes and Dutch Frailty Score among Elderly Patients Who Underwent Surgery for Hip Fracture. Clin. Interv. Aging 2018, 13, 2481–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuckin, D.G.; Mufti, S.; Turner, D.J.; Bond, C.; Moonesinghe, S.R. The Association of Peri-Operative Scores, Including Frailty, with Outcomes after Unscheduled Surgery. Anaesthesia 2018, 73, 819–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kua, J.; Ramason, R.; Rajamoney, G.; Chong, M.S. Which Frailty Measure Is a Good Predictor of Early Post-Operative Complications in Elderly Hip Fracture Patients? Arch. Orthop. Trauma Surg. 2016, 136, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Chen, H.-L.; Zha, M.-L.; Zhou, Z.-Y. Diabetes and Pressure Ulcer Risk in Hip Fracture Patients: A Meta-Analysis. J. Wound Care 2017, 26, 519–527. [Google Scholar] [CrossRef]
- Klestil, T.; Röder, C.; Stotter, C.; Winkler, B.; Nehrer, S.; Lutz, M.; Klerings, I.; Wagner, G.; Gartlehner, G.; Nussbaumer-Streit, B. Impact of Timing of Surgery in Elderly Hip Fracture Patients: A Systematic Review and Meta-Analysis. Sci. Rep. 2018, 8, 13933. [Google Scholar] [CrossRef] [Green Version]
- Gazineo, D.; Chiari, P.; Chiarabelli, M.; Morri, M.; D’Alessandro, F.; Sabattini, T.; Ambrosi, E.; Forni, C. Predictive Factors for Category II Pressure Ulcers in Older Patients with Hip Fractures: A Prospective Study. J. Wound Care 2019, 28, 593–599. [Google Scholar] [CrossRef]
- Magny, E.; Vallet, H.; Cohen-Bittan, J.; Raux, M.; Meziere, A.; Verny, M.; Riou, B.; Khiami, F.; Boddaert, J. Pressure Ulcers Are Associated with 6-Month Mortality in Elderly Patients with Hip Fracture Managed in Orthogeriatric Care Pathway. Arch. Osteoporos. 2017, 12, 77. [Google Scholar] [CrossRef]
- Galivanche, A.R.; Kebaish, K.J.; Adrados, M.; Ottesen, T.D.; Varthi, A.G.; Rubin, L.E.; Grauer, J.N. Postoperative Pressure Ulcers After Geriatric Hip Fracture Surgery Are Predicted by Defined Preoperative Comorbidities and Postoperative Complications. J. Am. Acad. Orthop. Surg. 2020, 28, 342–351. [Google Scholar] [CrossRef]
- Chiari, P.; Forni, C.; Guberti, M.; Gazineo, D.; Ronzoni, S.; D’Alessandro, F. Predictive Factors for Pressure Ulcers in an Older Adult Population Hospitalized for Hip Fractures: A Prognostic Cohort Study. PLoS ONE 2017, 12, e0169909. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, E.D.D.L.; Mendivil, L.L.L.; Garza, D.P.S.; Hermosillo, H.G.; Chavez, J.H.M.; Corona, R.P. Low Handgrip Strength Is Associated with a Higher Incidence of Pressure Ulcers in Hip Fractured Patients. Acta Orthop. Belg. 2018, 84, 284–291. [Google Scholar] [PubMed]
- Wu, X.; Tian, M.; Zhang, J.; Yang, M.; Gong, X.; Liu, Y.; Li, X.; Lindley, R.I.; Anderson, M.; Peng, K.; et al. The Effect of a Multidisciplinary Co-Management Program for the Older Hip Fracture Patients in Beijing: A “Pre- and Post-” Retrospective Study. Arch. Osteoporos. 2019, 14, 43. [Google Scholar] [CrossRef]
- Forni, C.; D’Alessandro, F.; Genco, R.; Mini, S.; Notarnicola, T.; Vitulli, A.; Capezzali, D.; Morri, M. Prospective Prognostic Cohort Study of Pressure Injuries in Older Adult Patients with Hip Fractures. Adv. Skin Wound Care 2018, 31, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Correa-Pérez, A.; Delgado-Silveira, E.; Martín-Aragón, S.; Rojo-Sanchís, A.M.; Cruz-Jentoft, A.J. Fall-Risk Increasing Drugs and Prevalence of Polypharmacy in Older Patients Discharged from an Orthogeriatric Unit after a Hip Fracture. Aging Clin. Exp. Res. 2019, 31, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Heltne, M.; Saltvedt, I.; Lydersen, S.; Prestmo, A.; Sletvold, O.; Spigset, O. Patterns of Drug Prescriptions in an Orthogeriatric Ward as Compared to Orthopaedic Ward: Results from the Trondheim Hip Fracture Trial—A Randomised Clinical Trial. Eur. J. Clin. Pharmacol. 2017, 73, 937–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pajulammi, H.M.; Luukkaala, T.H.; Pihlajamäki, H.K.; Nuotio, M.S. Decreased Glomerular Filtration Rate Estimated by 2009 CKD-EPI Equation Predicts Mortality in Older Hip Fracture Population. Injury 2016, 47, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.; Nowak, L.; Melo, L.; Ward, S.; Atrey, A.; Schemitsch, E.H.; Nauth, A.; Khoshbin, A. Anemia at Presentation Predicts Acute Mortality and Need for Readmission Following Geriatric Hip Fracture. JB JS Open Access 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.-J.; Wang, J.-Q.; Zhang, W.-J.; Wang, W.-K.; Xu, D.; Luo, P. Hidden Blood Loss and Its Risk Factors after Hip Hemiarthroplasty for Displaced Femoral Neck Fractures: A Cross-Sectional Study. Clin. Interv. Aging 2018, 13, 1639–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arshi, A.; Lai, W.C.; Iglesias, B.C.; McPherson, E.J.; Zeegen, E.N.; Stavrakis, A.I.; Sassoon, A.A. Blood Transfusion Rates and Predictors Following Geriatric Hip Fracture Surgery. Hip. Int. 2020. [Google Scholar] [CrossRef]
- Yombi, J.C.; Putineanu, D.C.; Cornu, O.; Lavand’homme, P.; Cornette, P.; Castanares-Zapatero, D. Low Haemoglobin at Admission Is Associated with Mortality after Hip Fractures in Elderly Patients. Bone Jt. J. 2019, 101-B, 1122–1128. [Google Scholar] [CrossRef]
- Mueller, M.M.; Van Remoortel, H.; Meybohm, P.; Aranko, K.; Aubron, C.; Burger, R.; Carson, J.L.; Cichutek, K.; De Buck, E.; Devine, D.; et al. Patient Blood Management: Recommendations From the 2018 Frankfurt Consensus Conference. JAMA 2019, 321, 983–997. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Yin, J.; Wang, B.; Xue, Q.; Gao, S.; Xing, L.; Wang, H.; Liu, W.; Liu, X. Restrictive versus Liberal Strategy for Red Blood-Cell Transfusion in Hip Fracture Patients: A Systematic Review and Meta-Analysis. Medicine (Baltimore) 2019, 98, e16795. [Google Scholar] [CrossRef] [PubMed]
- Zerah, L.; Dourthe, L.; Cohen-Bittan, J.; Verny, M.; Raux, M.; Mézière, A.; Khiami, F.; Tourette, C.; Neri, C.; Le Manach, Y.; et al. Retrospective Evaluation of a Restrictive Transfusion Strategy in Older Adults with Hip Fracture. J. Am. Geriatr. Soc. 2018, 66, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.M.; DeMario, V.M.; Best, M.J.; Shafiq, B.; Hasenboehler, E.A.; Sterling, R.S.; Frank, S.M.; Khanuja, H.S. A Restrictive Hemoglobin Transfusion Threshold of Less Than 7 g/DL Decreases Blood Utilization without Compromising Outcomes in Patients With Hip Fractures. J. Am. Acad. Orthop. Surg. 2019, 27, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Li, L.; Xiang, Z.; Li, H.; Hou, X.-L. Association of Iron Supplementation with Risk of Transfusion, Hospital Length of Stay, and Mortality in Geriatric Patients Undergoing Hip Fracture Surgeries: A Meta-Analysis. Eur. Geriatr. Med. 2020. [Google Scholar] [CrossRef]
- Yoon, B.-H.; Lee, B.S.; Won, H.; Kim, H.-K.; Lee, Y.-K.; Koo, K.-H. Preoperative Iron Supplementation and Restrictive Transfusion Strategy in Hip Fracture Surgery. Clin. Orthop. Surg. 2019, 11, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Pareja Sierra, T.; Bartolome Martín, I.; Rodríguez Solis, J.; Morales Sanz, M.D.; Torralba Gonzalez de Suso, M.; Barcena Goitiandia, L.Á.; Hornillos Calvo, M. Results of an Anaemia Treatment Protocol Complementary to Blood Transfusion in Elderly Patients with Hip Fracture. Rev. Esp. Geriatr. Gerontol. 2019, 54, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Wang, T.; Liu, J.; Duan, X.; Xiang, Z. Clinical study of recombinant human erythropoietin combined with iron to correct perioperative anemia in elderly patients with intertrochanteric fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2019, 33, 662–665. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.-H.; Ko, Y.S.; Jang, S.-H.; Ha, J.K. Feasibility of Hip Fracture Surgery Using a No Transfusion Protocol in Elderly Patients: A Propensity Score-Matched Cohort Study. J. Orthop. Trauma 2017, 31, 414–419. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, L.; Wu, P.; Lang, J.; Chen, L. Intervention with Erythropoietin in Sarcopenic Patients with Femoral Intertrochanteric Fracture and Its Potential Effects on Postoperative Rehabilitation. Geriatr. Gerontol. Int. 2020, 20, 150–155. [Google Scholar] [CrossRef]
- Xiao, C.; Zhang, S.; Long, N.; Yu, W.; Jiang, Y. Is Intravenous Tranexamic Acid Effective and Safe during Hip Fracture Surgery? An Updated Meta-Analysis of Randomized Controlled Trials. Arch. Orthop. Trauma Surg. 2019, 139, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Baskaran, D.; Rahman, S.; Salmasi, Y.; Froghi, S.; Berber, O.; George, M. Effect of Tranexamic Acid Use on Blood Loss and Thromboembolic Risk in Hip Fracture Surgery: Systematic Review and Meta-Analysis. Hip. Int. 2018, 28, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.-M.; Wang, H.-P.; Li, Y.-J.; Ma, B.-B.; Xie, T.; Wang, C.; Chen, H.; Rui, Y.-F. The Efficacy and Safety of Intravenous Tranexamic Acid in Hip Fracture Surgery: A Systematic Review and Meta-Analysis. J. Orthop. Translat. 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Haj-Younes, B.; Sivakumar, B.S.; Wang, M.; An, V.V.; Lorentzos, P.; Adie, S. Tranexamic Acid in Hip Fracture Surgery: A Systematic Review and Meta-Analysis. J. Orthop. Surg. (Hong Kong) 2020, 28. [Google Scholar] [CrossRef]
- Luo, X.; Huang, H.; Tang, X. Efficacy and Safety of Tranexamic Acid for Reducing Blood Loss in Elderly Patients with Intertrochanteric Fracture Treated with Intramedullary Fixation Surgery: A Meta-Analysis of Randomized Controlled Trials. Acta Orthop. Traumatol. Turc. 2020, 54, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Sanzone, A.G. Current Challenges in Pain Management in Hip Fracture Patients. J. Orthop. Trauma 2016, 30 (Suppl. 1), S1–S5. [Google Scholar] [CrossRef] [Green Version]
- Oberkircher, L.; Schubert, N.; Eschbach, D.-A.; Bliemel, C.; Krueger, A.; Ruchholtz, S.; Buecking, B. Prehospital Pain and Analgesic Therapy in Elderly Patients with Hip Fractures. Pain Pract. 2016, 16, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Orive, M.; Anton-Ladislao, A.; García-Gutiérrez, S.; Las Hayas, C.; González, N.; Zabala, J.; Quintana, J.M. Prospective Study of Predictive Factors of Changes in Pain and Hip Function after Hip Fracture among the Elderly. Osteoporos. Int. 2016, 27, 527–536. [Google Scholar] [CrossRef]
- Riddell, M.; Ospina, M.; Holroyd-Leduc, J.M. Use of Femoral Nerve Blocks to Manage Hip Fracture Pain among Older Adults in the Emergency Department: A Systematic Review. CJEM 2016, 18, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guay, J.; Kopp, S. Peripheral Nerve Blocks for Hip Fractures in Adults. Cochrane Database Syst. Rev. 2020, 11, CD001159. [Google Scholar] [CrossRef]
- Elboim-Gabyzon, M.; Andrawus Najjar, S.; Shtarker, H. Effects of Transcutaneous Electrical Nerve Stimulation (TENS) on Acute Postoperative Pain Intensity and Mobility after Hip Fracture: A Double-Blinded, Randomized Trial. Clin. Interv. Aging 2019, 14, 1841–1850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganczak, M.; Chrobrowski, K.; Korzeń, M. Predictors of a Change and Correlation in Activities of Daily Living after Hip Fracture in Elderly Patients in a Community Hospital in Poland: A Six-Month Prospective Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 95. [Google Scholar] [CrossRef] [Green Version]
- Morandi, A.; Mazzone, A.; Bernardini, B.; Suardi, T.; Prina, R.; Pozzi, C.; Gentile, S.; Trabucchi, M.; Bellelli, G. Association between Delirium, Adverse Clinical Events and Functional Outcomes in Older Patients Admitted to Rehabilitation Settings after a Hip Fracture: A Multicenter Retrospective Cohort Study. Geriatr. Gerontol. Int. 2019, 19, 404–408. [Google Scholar] [CrossRef]
- Selakovic, I.; Dubljanin-Raspopovic, E.; Markovic-Denic, L.; Marusic, V.; Cirkovic, A.; Kadija, M.; Tomanovic-Vujadinovic, S.; Tulic, G. Can Early Assessment of Hand Grip Strength in Older Hip Fracture Patients Predict Functional Outcome? PLoS ONE 2019, 14, e0213223. [Google Scholar] [CrossRef] [Green Version]
- Kronborg, L.; Bandholm, T.; Palm, H.; Kehlet, H.; Kristensen, M.T. Physical Activity in the Acute Ward Following Hip Fracture Surgery Is Associated with Less Fear of Falling. J. Aging Phys. Act. 2016, 24, 525–532. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, P.D.; Shields, N.; Blackstock, F.; Wintle, E.; Taylor, N.F. Motivational Interviewing Increases Physical Activity and Self-Efficacy in People Living in the Community after Hip Fracture: A Randomized Controlled Trial. Clin. Rehabil. 2016, 30, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ambrosini, E.; Brunati, R.; Capone, A.; Pagliari, G.; Secci, C.; Zatti, G.; Ferrante, S. How Balance Task-Specific Training Contributes to Improving Physical Function in Older Subjects Undergoing Rehabilitation Following Hip Fracture: A Randomized Controlled Trial. Clin. Rehabil. 2018, 32, 340–351. [Google Scholar] [CrossRef]
- Briggs, R.A.; Houck, J.R.; Drummond, M.J.; Fritz, J.M.; LaStayo, P.C.; Marcus, R.L. Muscle Quality Improves with Extended High-Intensity Resistance Training after Hip Fracture. J. Frailty Aging 2018, 7, 51–56. [Google Scholar] [CrossRef]
- Lee, S.Y.; Yoon, B.-H.; Beom, J.; Ha, Y.-C.; Lim, J.-Y. Effect of Lower-Limb Progressive Resistance Exercise after Hip Fracture Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Am. Med. Dir. Assoc. 2017, 18, 1096.e19–1096.e26. [Google Scholar] [CrossRef] [PubMed]
- Mohammad Ismail, A.; Borg, T.; Sjolin, G.; Pourlotfi, A.; Holm, S.; Cao, Y.; Wretenberg, P.; Ahl, R.; Mohseni, S. β-Adrenergic Blockade Is Associated with a Reduced Risk of 90-Day Mortality after Surgery for Hip Fractures. Trauma Surg. Acute Care Open 2020, 5, e000533. [Google Scholar] [CrossRef]
- van der Zwaard, B.C.; Stein, C.E.; Bootsma, J.E.M.; van Geffen, H.J.A.A.; Douw, C.M.; Keijsers, C.J.P.W. Fewer Patients Undergo Surgery When Adding a Comprehensive Geriatric Assessment in Older Patients with a Hip Fracture. Arch. Orthop. Trauma Surg. 2020, 140, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Zerah, L.; Hajage, D.; Raux, M.; Cohen-Bittan, J.; Mézière, A.; Khiami, F.; Le Manach, Y.; Riou, B.; Boddaert, J. Attributable Mortality of Hip Fracture in Older Patients: A Retrospective Observational Study. J. Clin. Med. 2020, 9, 2370. [Google Scholar] [CrossRef] [PubMed]
- Daraphongsataporn, N.; Saloa, S.; Sriruanthong, K.; Philawuth, N.; Waiwattana, K.; Chonyuen, P.; Pimolbutr, K.; Sucharitpongpan, W. One-Year Mortality Rate after Fragility Hip Fractures and Associated Risk in Nan, Thailand. Osteoporos. Sarcopenia 2020, 6, 65–70. [Google Scholar] [CrossRef]
- Capkin, S.; Guler, S.; Ozmanevra, R. C-Reactive Protein to Albumin Ratio May Predict Mortality for Elderly Population Who Undergo Hemiarthroplasty Due to Hip Fracture. J. Investig. Surg. 2020, 1–6. [Google Scholar] [CrossRef]
- Huette, P.; Abou-Arab, O.; Djebara, A.-E.; Terrasi, B.; Beyls, C.; Guinot, P.-G.; Havet, E.; Dupont, H.; Lorne, E.; Ntouba, A.; et al. Risk Factors and Mortality of Patients Undergoing Hip Fracture Surgery: A One-Year Follow-up Study. Sci. Rep. 2020, 10, 9607. [Google Scholar] [CrossRef]
- Drevet, S.; Bornu, B.-J.C.; Boudissa, M.; Bioteau, C.; Mazière, S.; Merloz, P.; Couturier, P.; Tonetti, J.; Gavazzi, G. One-year mortality after a hip fracture: Prospective study of a cohort of patients aged over 75 years old. Geriatr. Psychol. Neuropsychiatr. Vieil. 2019, 17, 369–376. [Google Scholar] [CrossRef]
- Menéndez-Colino, R.; Gutiérrez Misis, A.; Alarcon, T.; Díez-Sebastián, J.; Díaz de Bustamante, M.; Queipo, R.; Otero, A.; González-Montalvo, J.I. Development of a New Comprehensive Preoperative Risk Score for Predicting 1-Year Mortality in Patients with Hip Fracture: The HULP-HF Score. Comparison with 3 Other Risk Prediction Models. Hip. Int. 2020. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-Y.; Cho, K.-J.; Kim, S.-W.; Yoon, S.-J.; Kang, M.-G.; Kim, K.-I.; Lee, Y.-K.; Koo, K.-H.; Kim, C.-H. Prediction of Mortality and Postoperative Complications Using the Hip-Multidimensional Frailty Score in Elderly Patients with Hip Fracture. Sci. Rep. 2017, 7, 42966. [Google Scholar] [CrossRef] [Green Version]
- Chesser, T.J.S.; Inman, D.; Johansen, A.; Belluati, A.; Pari, C.; Contini, A.; Voeten, S.C.; Hegeman, J.H.; Ponsen, K.J.; Montero-Fernández, N.; et al. Hip Fracture Systems—European Experience. OTA Int. 2020, 3, e050. [Google Scholar] [CrossRef]
- Williamson, S.; Landeiro, F.; McConnell, T.; Fulford-Smith, L.; Javaid, M.K.; Judge, A.; Leal, J. Costs of Fragility Hip Fractures Globally: A Systematic Review and Meta-Regression Analysis. Osteoporos. Int. 2017, 28, 2791–2800. [Google Scholar] [CrossRef]
- Tan, L.T.J.; Wong, S.J.; Kwek, E.B.K. Inpatient Cost for Hip Fracture Patients Managed with an Orthogeriatric Care Model in Singapore. Singap. Med. J. 2017, 58, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Bartra, A.; Caeiro, J.-R.; Mesa-Ramos, M.; Etxebarría-Foronda, I.; Montejo, J.; Carpintero, P.; Sorio-Vilela, F.; Gatell, S.; Canals, L.; en representación de los investigadores del estudio PROA. Cost of Osteoporotic Hip Fracture in Spain per Autonomous Region. Rev. Esp. Cir. Ortop. Traumatol. 2019, 63, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, A.; Delhougne, G. Incidence and Economic Burden of Intertrochanteric Fracture: A Medicare Claims Database Analysis. JB JS Open Access 2019, 4, e0045. [Google Scholar] [CrossRef] [PubMed]
- Arshi, A.; Rezzadeh, K.; Stavrakis, A.I.; Bukata, S.V.; Zeegen, E.N. Standardized Hospital-Based Care Programs Improve Geriatric Hip Fracture Outcomes: An Analysis of the ACS NSQIP Targeted Hip Fracture Series. J. Orthop. Trauma 2019, 33, e223–e228. [Google Scholar] [CrossRef] [PubMed]
- Reyes, B.J.; Mendelson, D.A.; Mujahid, N.; Mears, S.C.; Gleason, L.; Mangione, K.K.; Nana, A.; Mijares, M.; Ouslander, J.G. Postacute Management of Older Adults Suffering an Osteoporotic Hip Fracture: A Consensus Statement From the International Geriatric Fracture Society. Geriatr. Orthop. Surg. Rehabil. 2020, 11. [Google Scholar] [CrossRef]
- González Montalvo, J.I.; Gotor Pérez, P.; Martín Vega, A.; Alarcón Alarcón, T.; Mauleón Álvarez de Linera, J.L.; Gil Garay, E.; García Cimbrelo, E.; Alonso Biarge, J. La Unidad de Ortogeriatría de Agudos. Evaluación de Su Efecto En El Curso Clínico de Los Pacientes Con Fractura de Cadera y Estimación de Su Impacto Económico. Rev. Esp. Geriatr. Gerontol. 2011, 46, 193–199. [Google Scholar] [CrossRef]
- Ginsberg, G.; Adunsky, A.; Rasooly, I. A Cost-Utility Analysis of a Comprehensive Orthogeriatric Care for Hip Fracture Patients, Compared with Standard of Care Treatment. Hip. Int. 2013, 23, 570–575. [Google Scholar] [CrossRef]
- Eamer, G.; Taheri, A.; Chen, S.S.; Daviduck, Q.; Chambers, T.; Shi, X.; Khadaroo, R.G. Comprehensive Geriatric Assessment for Older People Admitted to a Surgical Service. Cochrane Database Syst. Rev. 2018, 1, CD012485. [Google Scholar] [CrossRef]
- Leal, J.; Gray, A.M.; Hawley, S.; Prieto-Alhambra, D.; Delmestri, A.; Arden, N.K.; Cooper, C.; Javaid, M.K.; Judge, A.; REFReSH Study Group. Cost-Effectiveness of Orthogeriatric and Fracture Liaison Service Models of Care for Hip Fracture Patients: A Population-Based Study. J. Bone Miner. Res. 2017, 32, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Eamer, G.; Saravana-Bawan, B.; van der Westhuizen, B.; Chambers, T.; Ohinmaa, A.; Khadaroo, R.G. Economic Evaluations of Comprehensive Geriatric Assessment in Surgical Patients: A Systematic Review. J. Surg. Res. 2017, 218, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Mesa Ramos, M.; Caeiro-Rey, J.R. Orthogeriatric Units. They Are Really Necessary. Glob. J. Ortho. Res. 2020, 2, 4. [Google Scholar]
- Allsop, S.; Morphet, J.; Lee, S.; Cook, O. Exploring the Roles of Advanced Practice Nurses in the Care of Patients Following Fragility Hip Fracture: A Systematic Review. J. Adv. Nurs. 2020. [Google Scholar] [CrossRef]
- Van Camp, L.; Dejaeger, M.; Tournoy, J.; Gielen, E.; Laurent, M.R. Association of Orthogeriatric Care Models with Evaluation and Treatment of Osteoporosis: A Systematic Review and Meta-Analysis. Osteoporos. Int. 2020, 31, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, K.J.; Fitzgerald, L.; Hatherley, S.; Potter, C.; Ayis, S.; Martin, F.C.; Gregson, C.L.; Cameron, I.D.; Beaupre, L.A.; Wyatt, D.; et al. Inequity in Rehabilitation Interventions after Hip Fracture: A Systematic Review. Age Ageing 2019, 48, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, R.S. Gender and Race/Ethnicity Differences in Hip Fracture Incidence, Morbidity, Mortality, and Function. Clin. Orthop. Relat. Res. 2011, 469, 1913–1918. [Google Scholar] [CrossRef] [Green Version]
- Nayar, S.K.; Marrache, M.; Ali, I.; Bressner, J.; Raad, M.; Shafiq, B.; Srikumaran, U. Racial Disparity in Time to Surgery and Complications for Hip Fracture Patients. Clin. Orthop. Surg. 2020, 12, 430–434. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Year | Country | Sample Size | Inclusion Criteria | Exclusion Criteria | Study Design | Conclusion Summary | Level of Evidence |
|---|---|---|---|---|---|---|---|---|
| Zusman [61] | 2017 | Canada | 53 | Hip fracture aged 65 years or older with a recent hip fracture (3–12 months). | older adults who, prior to the fracture, were unable to walk 10 m, dementia, and/or older adults moved to a residential care facility. | RCT | 44% of study participants self-reported UI. | Ib |
| Morri [65] | 2018 | Italy | 840 | 65 years of age or older hospitalized | The absence of a legal guardian to sign the consent form in cases of cognitive deficit, and a diagnosis of periprosthetic or pathological fracture | Prospective cohort study | 50% sample studied unable to recover their prefracture autonomy levels. Risk factors: increased number of days with diapers (B = 0.003; p < 0.001), urinary catheter (B = 0.03; p < 0.001) | IIb |
| Díaz de Bustamante [71] | 2017 | Spain | 509 | Patients aged ≥ 65 yo admitted due to hip fracture | Cohort study | 81.2% protein malnutrition. 17.1% energy and protein malnutrition. 93% Low vitamin D levels. Sarcopenia prevalence 17.1% | IIb | |
| Inoue [73] | 2019 | Japan | 205 | Patients aged ≥ 65 yo, fractures caused by falling and surgical treatment. | Terminal malignant disease, uncontrolled chronic liver disease and/or pre-fracture ambulation difficulty | Longitudinal cohort study | MNA-SF had a significant association with discharge motor-FIM, efficiency on the motor-FIM and 10-m walking speed. GNRI significantly associated with 10-m walking speed. | IIb |
| Inoue [77] | 2017 | Japan | 204 | Age ≥ 65 yo, fractures incurred as a result of falls and required surgery. | Terminal malignant disease, uncontrolled chronic liver disease, and/or pre-fracture ambulation difficulty, partial or no weight-bearing indications during postoperative rehabilitation | Multicentre cohort study | MNA-SF was a significant independent predictor for FIM at discharge (well-nourished vs. malnourished, β = 0.86, p < 0.01). | IIb |
| Beauchamp-Chalifour [78] | 2020 | Canada | 209 | Geriatric patients (>65 yo) admitted for a hip fracture. | Subtrochanteric fracture, pathologic hip fracture and polytrauma patients | Cohort study | Deceased patients had lower MNA scores (mean 19.9 (SD 5.2), p < 0.001) and lower MMSE scores (mean 16.0 (SD 10.9, p < 0.001). | IIb |
| Torbergsen [79] | 2019 | Norway | 71 patients (31 in the intervention group and 40 controls) | Fracture resulted of a low energy trauma. | Moribund at admittance. | RCT | Intervention group: Vitamin K1 K1: 1.0 (SD 1.2) vs 0.6 (SD 0.6) ng/mL, p = 0.09; 25(OH)D: 60 (SD 29) vs 43 (SD 22) nmol/L, p = 0.01 | Ib |
| Landi [83] | 2017 | Italy | 127 | Age ≥ 70 yo admitted to in-hospital Geriatric Rehabilitation Unit with hip fracture. | Longitudinal cohort study | Sarcopenia 33.9%. Sarcopenia increased risk of incomplete functional recovery: OR 3.07, 95%CI 1.07–8.75. Sarcopenia showed lower Barthel index scores at discharge: 69.2 versus 58.9; p < 0.001); and after 3 months of follow-up (90.9 versus 80.5; p = 0.02). | IIb | |
| van de Ree [84] | 2019 | Netherlands | 696 | Patients ≥ 65 yo with hip fracture | Pathological hip fractures. | Multicentre longitudinal cohort study | 53.3% were frail. Frailty was negatively associated with HS (β −0.333; 95%CI −0.366 to −0.299), self-rated health (β −21.9; 95%CI −24.2 to −19.6) and capability well-being (β −0.296; 95%CI −0.322 to −0.270) in elderly patients 1 year after hip fracture. After adjusting for confounders, associations were weakened but remained significant. | IIb |
| Wei [89] | 2017 | China | 8 studies (22,180 patients) | Types of studies: observational studies; Types of participants: patients with hip fracture; Comorbidity: compared patients with diabetes with those without diabetes | Meta-analysis | Mean PU incidence: 15.1% in group with diabetes compared to 7.5% without diabetes group. Diabetes PU OR 1.825 (95%CI: 1.373–2.425; p < 0.001). Subgroup analysis by PU stage: OR 1.474 [95%CI 0.984–2.207] for ≥category II PU, and 2.814 [95%CI: 2.115–3.742] for ≥category I PU. | Ia | |
| Klestil [90] | 2018 | Austria | 28 prospective studies (31,242 patients). | Randomised controlled trials, non-randomised controlled trials, and prospective controlled cohort studies. Adults aged 60 years or older undergoing surgery for acute intra- and extracapsular hip fracture. | Meta-analysis | 48 h surgery: RR dying within 12 months (RR) 0.80, 95%CI 0.66–0.97. Adjusted data: fewer complications (8% vs. 17%) in patients who had early surgery. | Ia | |
| Ganizeo [91] | 2019 | Italy | 761 | Fragility hip fracture patients aged ≥65 years. | Patients with periprosthetic or pathological fractures. | Prospective cohort study | The incidence of category II or higher PUs was 12%. Five factors independently associated with category ≥II PU development: Higher preoperative Braden score (Hazard Ratio [HR]: 0.884; 95% confidence interval [CI]: 0.806–0.969), surgical procedure with internal fixation (HR 1.876; 95%CI: 1.183–2.975), a higher percentage of days with the presence of foam valve before surgery (HR: 1.010; 95%CI: 1.010–1.023) and a urinary catheter (HR: 1.013; 95%CI: 1.006–1.019) and diaper (HR: 1.007; 95%CI 1.001–1.013) in the postoperative period. | IIb |
| Chiari [94] | 2017 | Italy | 1083 | Patients ≥ 65 years of age with fragility hip fracture. | Patients with periprosthetic or pathological fractures, and patients who presented with pressure ulcers. | Prospective cohort study | Pressure ulcers incidence: 22.7%. Two risk factors: age > 80 years (odds ratio (OR) 1.03; 95%IC 1.006; 1.054, p = 0.015), the length of time a urinary catheter was used (OR 1.013; 95%IC 1.008; 1.018, p < 0.001. | IIb |
| Forni [97] | 2018 | Italy | 467 | Prospective cohort study | Of these, 27% (n = 127) developed a pressure injury. Multivariate analysis identified the following predictive factors: age older than 81 years, type of surgery, and placing the limb in a foam rubber splint. | IIb |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarazona-Santabalbina, F.J.; Ojeda-Thies, C.; Figueroa Rodríguez, J.; Cassinello-Ogea, C.; Caeiro, J.R. Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture. Int. J. Environ. Res. Public Health 2021, 18, 3049. https://doi.org/10.3390/ijerph18063049
Tarazona-Santabalbina FJ, Ojeda-Thies C, Figueroa Rodríguez J, Cassinello-Ogea C, Caeiro JR. Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture. International Journal of Environmental Research and Public Health. 2021; 18(6):3049. https://doi.org/10.3390/ijerph18063049
Chicago/Turabian StyleTarazona-Santabalbina, Francisco José, Cristina Ojeda-Thies, Jesús Figueroa Rodríguez, Concepción Cassinello-Ogea, and José Ramón Caeiro. 2021. "Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture" International Journal of Environmental Research and Public Health 18, no. 6: 3049. https://doi.org/10.3390/ijerph18063049