
Validity and Reliability of the Malay Versions of Bloating Severity (BSQ-M) and Quality of Life (BLQoL-M) Questionnaires

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, and Sampling Method
2.2. Questionnaire Translation
2.3. Measures
2.3.1. Demographic Information
2.3.2. BSQ and BLQoL
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Exploratory Factor Analysis
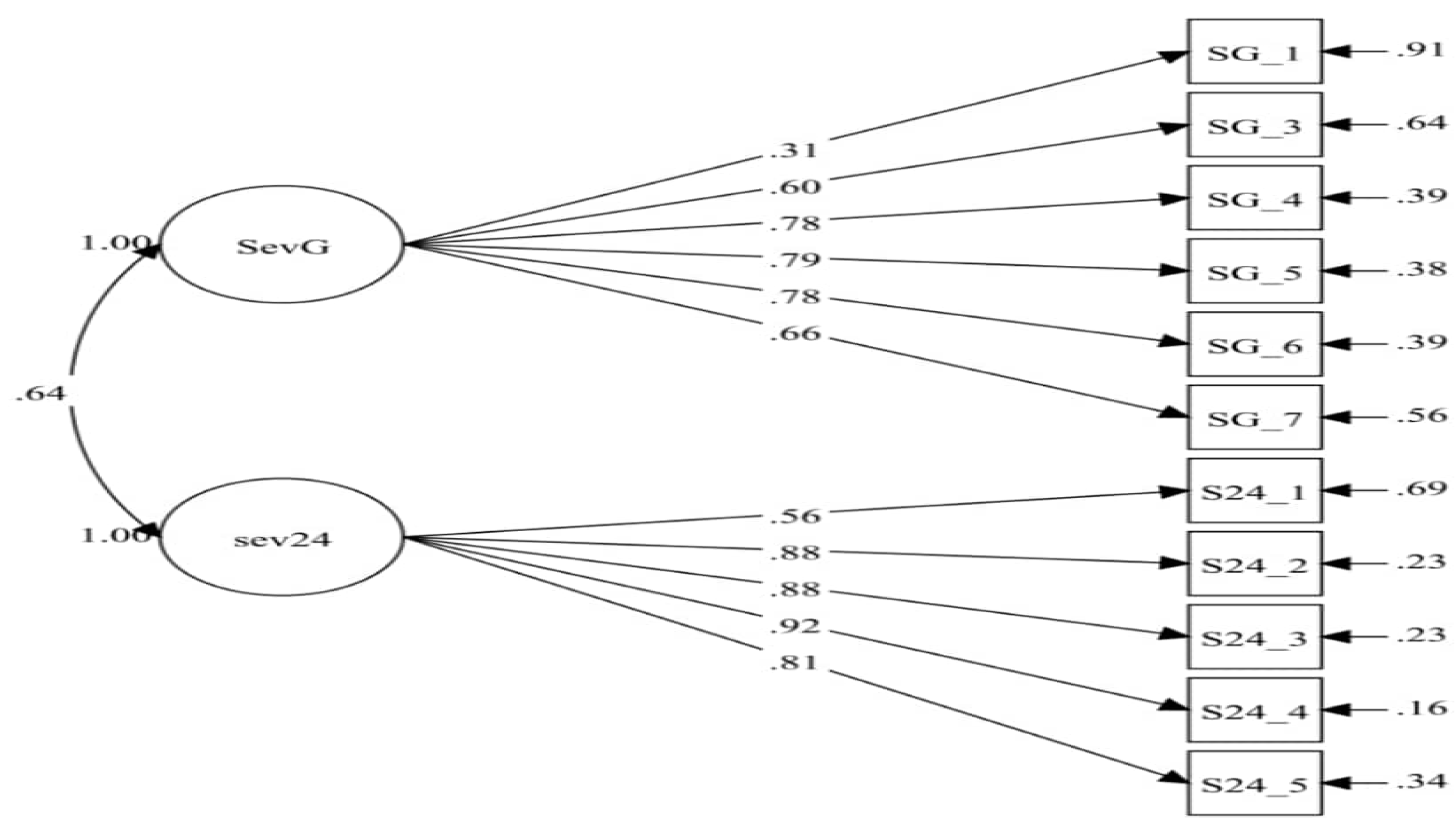
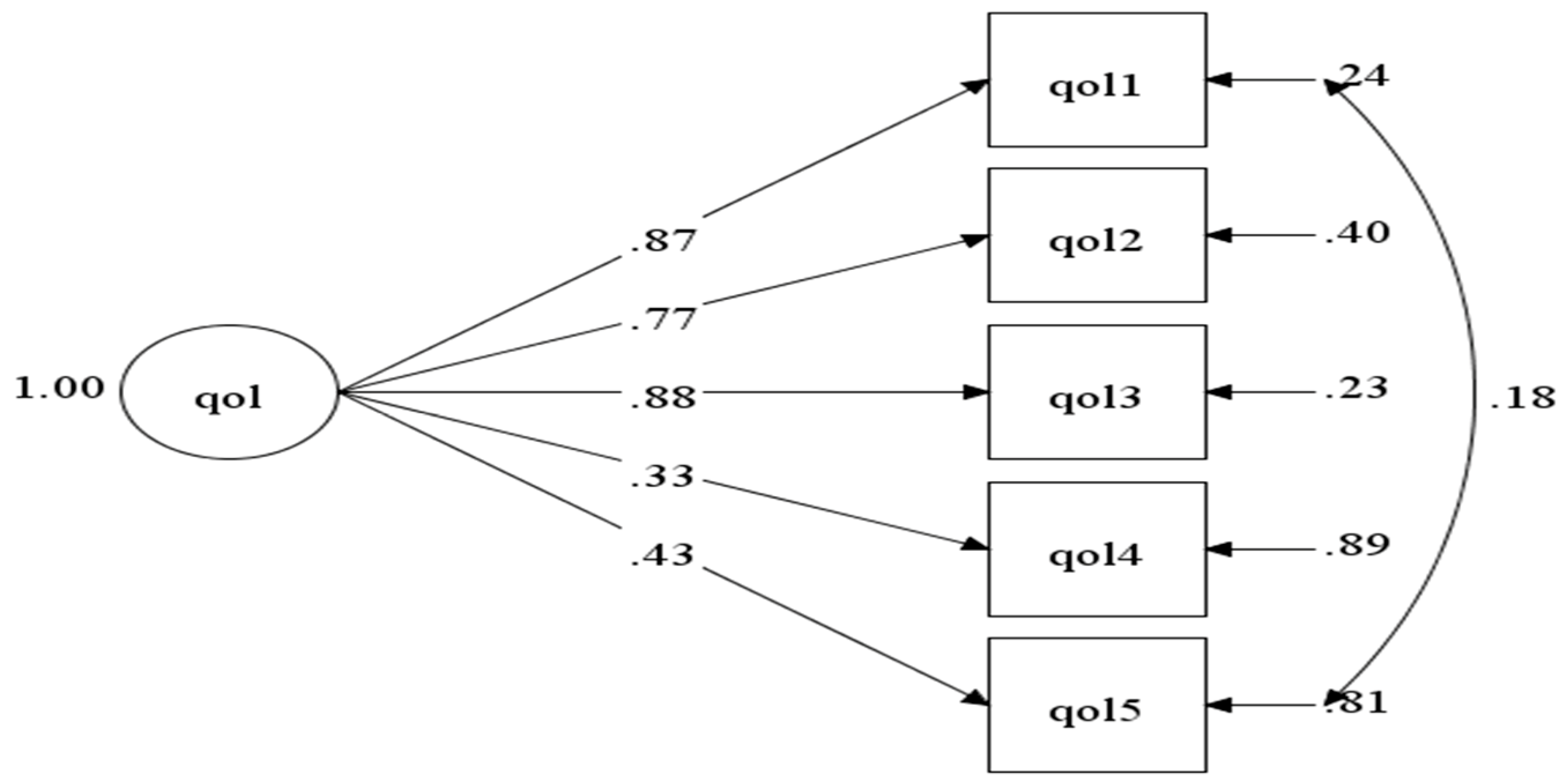
3.2. Confirmatory Factor Analysis
3.3. Discriminant Validity
3.4. The Internal Consistency (ICC)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mari, A.; Backer, F.A.; Mahamid, M.; Amara, H.; Carter, D.; Boltin, D.; Dickman, R. Bloating and abdominal distension: Clinical approach and management. Adv. Ther. 2019, 36, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Azpiroz, F.; Malagelada, J.R. Review article: Abdominal bloating. Gastroenterelogy 2005, 129, 1060–1078. [Google Scholar] [CrossRef]
- Peter, J. Bloating 101: Why You Feel Bloated. Web MD. 2010. Available online: https://www.webmd.com/digestive-disorders/features/bloated-bloating#1 (accessed on 18 April 2020).
- Ringel, Y.; Williams, R.E.; Kalilani, L.; Cook, S.F. Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2009, 7, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Locke, G.R.; Choung, R.S.; Zinsmeister, A.R.; Schleck, C.D.; Talley, N.J. Prevalence and risk factors for abdominal bloating and visible distention: A population-based study. Gut 2008, 57, 756–763. [Google Scholar] [CrossRef]
- Yu, H.; Chan, E.E.; Lingam, P.; Lee, J.; Woon, W.W.L.; Low, J.K.; Shelat, V.G. Index admission laparoscopic cholecystectomy for acute cholecystitis restores Gastrointestinal Quality of Life Index (GIQLI) score. Ann. Hepato-Biliary Pancreat. Surg. 2018, 22, 58–65. [Google Scholar] [CrossRef]
- Agrawal, A.; Whorwell, P.J. Review article: Abdominal bloating and distension in functional gastrointestinal disorders—Epidemiology and exploration of possible mechanisms. Aliment. Pharmacol. Ther. 2008, 27, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.; Spiegel, B.M.R. The relationship between obesity and functional gastrointestinal disorders: Causation, association, or neither? Gastroenterol. Hepatol. 2008, 4, 572–578. [Google Scholar]
- Chang, L.; Lee, O.Y.; Naliboff, B.; Schmulson, M.; Mayer, E.A. Sensation of bloating and visible abdominal distension in patients with irritable bowel syndrome. Am. J. Gastroenterol. 2001, 96, 3341–3347. [Google Scholar] [CrossRef] [PubMed]
- Houghton, L.A.; Lea, R.; Agrawal, A.; Reilly, B.; Whorwell, P.J. Relationship of abdominal bloating to distension in irritable bowel syndrome and effect of bowel habit. Gastroenterology 2006, 131, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Miwa, H.; Nakagawa, A.; Kosako, M.; Akiho, H.; Fukudo, S. Abdominal bloating is the most bothersome symptom in irritable bowel syndrome with constipation (IBS-C): A large population-based Internet survey in Japan. Biopsychosoc. Med. 2016, 10, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dash, S.; Clarke, G.; Berk, M.; Jacka, F.N. The gut microbiome and diet in psychiatry: Focus on depression. Curr. Opin. Psychiatry 2015, 28, 1–6. [Google Scholar] [CrossRef]
- Gwee, K.A.; Wee, S.; Wong, M.L.; Png, D.J.C. The prevalence, symptom characteristics, and impact of irritable bowel syndrome in an Asian urban community. Am. J. Gastroenterol. 2004, 99, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Foley, A.; Burgell, R.; Barrett, J.S.; Gibson, P.R. Management strategies for abdominal bloating and distension. Gastroenterol. Hepatol. 2014, 10, 561–571. [Google Scholar]
- Pimentel, M.; Lembo, A.; Chey, W.D.; Zakko, S.; Ringel, Y.; Yu, J.; Mareya, S.M.; Shaw, A.L.; Bortey, E.; Forbes, W.P. Rifaximin therapy for patients with irritable bowel syndrome without constipation. N. Engl. J. Med. 2011, 364, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäder, U.; Martin, B.W.; Schutz, Y.; Marti, B. Validity of four short physical activity questionnaires in middle-aged persons. Med. Sci. Sports Exerc. 2006, 38, 1255–1266. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Quigley, E.M.M.; Shiff, S.J.; Lavins, B.J.; Kurtz, C.B.; MacDougall, J.E.; Currie, M.G.; Johnston, J.M. Effect of Linaclotide on severe abdominal symptoms in patients with irritable bowel syndrome with constipation. Clin. Gastroenterol. Hepatol. 2014, 12, 616–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, K.C.; Headstrom, P.; Jarrett, M.E.; Motzer, S.A.; Park, H.; Burr, R.L.; Surawicz, C.M.; Heitkemper, M.M. Abdominal pain impacts quality of life in women with irritable bowel syndrome. Am. J. Gastroenterol. 2006, 101, 124–132. [Google Scholar] [CrossRef]
- Tuteja, A.K.; Talley, N.J.; Joos, S.K.; Tolman, K.G.; Hickam, D.H. Abdominal bloating in employed adults: Prevalence, risk factors, and association with other bowel disorders. Am. J. Gastroenterol. 2008, 103, 1241–1248. [Google Scholar] [CrossRef]
- Spiegel, B.; Bolus, R.; Harris, L.A.; Lucak, S.; Naliboff, B.; Esrailian, E.; Chey, W.D.; Lembo, A.; Karsan, H.; Tillisch, K.; et al. Measuring irritable bowel syndrome patient-reported outcomes with an abdominal pain numeric rating scale. Aliment. Pharmacol. Ther. 2009, 30, 1159–1170. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (Sf-36): I. conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Drossman, D.A.; Li, Z.; Toner, B.B.; Diamant, N.E.; Creed, F.H.; Thompson, D.; Read, N.W.; Babbs, C.; Barreiro, M.; Bank, L.; et al. Functional bowel disorders. a multicenter comparison of health status and development of illness severity index. Dig. Dis. Sci. 1995, 40, 986–995. [Google Scholar] [CrossRef]
- Spiegel, B.; Camilleri, M.; Bolus, R.; Andresen, V.; Chey, W.D.; Fehnel, S.; Mangel, A.; Talley, N.J.; Whitehead, W.E. Psychometric evaluation of patient-reported outcomes in irritable bowel syndrome randomized controlled trials: A Rome Foundation Report. Gastroenterology 2009, 137, 1944–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, D.L.; Drossman, D.A.; Frederick, I.O.; Dicesare, J.; Puder, K.L. Quality of life in persons with irritable bowel syndrome: Development and validation of a new measure. Dig. Dis. Sci. 1998, 43, 400–411. [Google Scholar] [CrossRef]
- Hahn, B.A.; Kirchdoerfer, L.J.; Fullerton, S.; Mayer, E. Evaluation of a new quality of life questionnaire for patients with irritable bowel syndrome. Aliment. Pharmacol. Ther. 1997, 11, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Gusi, N.; Olivares, P.R.; Rajendram, R. The EQ-5D Health-Related Quality of Life Questionnaire. In Handbook of Disease Burdens and Quality of Life Measures; Springer: New York, NY, USA, 2010; pp. 87–99. [Google Scholar]
- Feng, Y.S.; Jiang, R.; Kohlmann, T.; Pickard, A.S. Exploring the internal structure of the EQ-5D using non–preference-based methods. Value Health 2019, 22, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Drossman, D.A.; Leserman, J.; Li, Z.; Mitchell, C.M.; Zagami, E.A.; Patrick, D.L. The rating form of IBD patient concerns: A new measure of health status. Psychosom. Med. 1991, 53, 701–712. [Google Scholar] [CrossRef] [PubMed]
- EuroQoL. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy (N. Y.) 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Chang, L.; Lembo, A.; Sultan, S. American Gastroenterological Association Institute Technical Review on the pharmacological management of irritable bowel syndrome. Gastroenterology 2014, 147, 1149–1172. [Google Scholar] [CrossRef] [Green Version]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Chassany, O.; Tugaut, B.; Marrel, A.; Guyonnet, D.; Arbuckle, R.; Duracinsky, M.; Whorwell, P.J.; Azpiroz, F. The intestinal gas questionnaire: Development of a new instrument for measuring gas-related symptoms and their impact on daily life. Neurogastroenterol. Motil. 2015, 27, 885–898. [Google Scholar] [CrossRef]
- Jowett, S.L.; Seal, C.J.; Barton, J.; Welfare, M.R. The short inflammatory bowel disease questionnaire (SIBDQ) is reliable and responsive to clinically important change in UC. Gastroenterology 2001, 120, 273–274. [Google Scholar] [CrossRef]
- Adelstein, B.A.; Irwig, L.; Macaskill, P.; Katelaris, P.H.; Jones, D.B.; Bokey, L. A self administered reliable questionnaire to assess lower bowel symptoms. BMC Gastroenterol. 2008, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Han, S.W.; Mccoll, E.; Steen, N.; Barton, J.R.; Welfare, M.R. The inflammatory bowel disease questionnaire: A valid and reliable measure in ulcerative colitis patients in the north east of England. Scand. J. Gastroenterol. 1998, 33, 961–966. [Google Scholar] [PubMed]
- Cheung, W.Y.; Garratt, A.M.; Russell, I.T.; Williams, J.G. The UK IBDQ-A British version of the inflammatory bowel disease questionnaire: Development and validation. J. Clin. Epidemiol. 2000, 53, 297–306. [Google Scholar] [CrossRef]
- Talley, N.J.; Phillips, S.F.; Melton, L.J.; Wiltgen, A.R.; Zinsmeister, A.R. A patient questionnaire to identify bowel disease. Ann. Intern. Med. 1989, 111, 671–674. [Google Scholar] [CrossRef]
- Talley, N.J.; Phillips, S.F.; Wiltgen, C.M.; Zinsmeister, A.R.; Melton, L.J. Assessment of functional gastrointestinal disease: The bowel disease questionnaire. Mayo Clin. Proc. 1990, 65, 1456–1479. [Google Scholar] [CrossRef] [Green Version]
- Thiwan, S. Abdominal Bloating: A mysterious Symptom. Available online: www.moam.info_abdominal-bloating-a-mysterious-symptom_59fb6f621723dd2d662356db.pdf (accessed on 18 April 2020).
- Thiwan, S.M.; Whitehead, W.E.; Palsson, O. Bloating Severity Questionnaire (BSQ). 2004. Available online: http://www.medpubinc.com/abfiles/AMS2004/AMS2004_100.PDF (accessed on 18 April 2020).
- Thiwan, S.; Palsson, O.S.; Turner, M.J.; Whitehead, W.E. Responsiveness of the bloating severity Questionnaire (BLSQ). Gastroenterology 2005, 128, A462. [Google Scholar]
- Palsson, O.S.; Thiwan, S.; Whitehead, W.; Turner, M. Development of a bloating questionnaire. Am. J. Gatroenterol. 2004, 99, S286. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation Background and Rationale. Value Health 2005, 8. Available online: http://www.ispor.org (accessed on 1 March 2020). [CrossRef] [Green Version]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 187–216. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA; London, UK, 2011. [Google Scholar]
- Taber, K.S. The use of cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- George, D.; Paul Mallery, W. SPSS for Windows Step by Step A Simple Guide and Reference Fourth Edition (11.0 Update) Answers to Selected Exercises. Allyn & Bacon. 2003. Available online: https://wps.ablongman.com/wps/media/objects/385/394732/george4answers.pdf (accessed on 10 January 2020).
- Hinton, P.; Brownlow, C.; McMurray, I. SPSS Explained; Taylor & Francis: Boca Raton, FL, USA, 2004. [Google Scholar]
- Karin, S.-E.; Sabine, L.; Marcel, S. Reliability of an Item Set Assessing Indoor Climate in Offices-Results From Field Studies and Laboratory Research. Front. Built Environ. 2019, 5, 117. [Google Scholar] [CrossRef]
- Devon, H.A.; Block, M.E.; Wright, P.M.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. Psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Raykov, T.; Marcoulides, G.A. Scale reliability evaluation under multiple assumption violations. Struct. Equ. Model. 2016, 23, 1–12. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Market. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Maret. Sci. 1988, 16, 74–79. [Google Scholar] [CrossRef]
- Tseng, W.T.; Dornyei, Z.; Schmitt, N. A new approach to assessing strategic learning: The case of self-regulation in vocabulary acquisition. Appl. Linguist. 2006, 27, 78–102. [Google Scholar] [CrossRef]
- Koo, T.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul Wahab, P.; Mohd Yusoff, D.; Abdul Kadir, A.; Ali, S.H.; Lee, Y.Y.; Kueh, Y.C. Psychometric evaluation of a newly developed elderly-constipation impact scale. PeerJ 2020, 8, e8581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVellis, R. Scale Development: Theory and Applications. 2016. Available online: https://books.google.com/books?hl=en&lr=&id=9yfYCwAAQBAJ&oi=fnd&pg=PP1&ots=HoJDSfRdhn&sig=-hhcdAGoWJZ8deROn2hqv_VKaMs (accessed on 18 April 2020).



{kind=link}
{kind=link}
| No. Abbreviated Item Content | Mean | SD | Factor Loading | |
|---|---|---|---|---|
| Factor 1 | Factor 2 | |||
| SEVG1 (“In the last month, how many days total would estimate you have had any type of bloating?” “Pada bulan lepas, berapa jumlah anggaran hari anda mengalami apa-apa jenis kembung perut?”) | 1.91 | 1.16 | −0.246 | |
| SEVG2 * (“On days that you have bloating, how often does it usually happen?” “Pada hari anda mengalami kembung perut, berapa kerapkah ia biasa berlaku?”) | 2.14 | 1.07 | 0.176 | |
| SEVG3 (“How long does the bloating typically last each time it is present?” “Berapa lama selalunya kembung perut berlarutan pada setiap kali ia berlaku?”) | 2.07 | 0.80 | 0.422 | |
| SEVG4 (“How severe is your bloating typically?” “Berapa terukkah kembung perut anda selalunya?”) | 2.14 | 0.80 | 0.536 | |
| SEVG5 (“How often do you have pain along with the bloating?” “Berapa kerap anda berasa sakit dengan kembung perut?”) | 2.22 | 0.70 | 0.790 | |
| SEVG6 (“When you have pain with your bloating, how severe is your pain typically?” “Apabila anda mengalami kesakitan semasa kembung perut, betapa terukkah sakit anda selalunya?”) | 2.09 | 0.65 | 0.693 | |
| SEVG7 (“How often do you have discomfort other than pain along with the bloating?” “Berapa kerapkah anda berasa tidak selesa selain daripada kesakitan semasa kembung perut?”) | 2.26 | 0.75 | 0.554 | |
| SEV241 * (“How often have you had bloating over the past 24 h?” “Berapa kerapkah anda mengalami kembung perut sejak 24 jam yang lepas?”) | 4.03 | 1.17 | 0.655 | |
| SEV242 (“How severe was your bloating, in terms of its effects on you, in the past 24 h?” “Berapa terukkah kesan kembung perut ke atas anda dalam masa 24 jam yang lepas?”) | 1.59 | 0.63 | 0.904 | |
| SEV243 (“How much pain that was related to the bloating did you have in the past 24 h?” “Sejauh mana kesakitan yang berkaitan dengan kembung perut yang anda rasai pada 24 jam yang lepas?”) | 1.52 | 0.68 | 0.803 | |
| SEV244 (“How much discomfort other than pain did you have related to your bloating in the past 24 h?” “Sejauh mana ketidakselesaan selain daripada sakit yang anda alami berkaitan dengan kembung perut pada 24 jam yang lepas?”) | 1.63 | 0.69 | 0.931 | |
| SEV245 (“What proportion of your total waking time did you have any bloating in the past 24 h (adding together the length of all bloating episodes you had during that time)?” “Apakah pecahan jumlah masa jaga yang mana anda mengalami kembung perut pada 24 jam lalu (dengan menambah tempoh masa kembung perut yang anda alami pada masa itu?”) | 1.97 | 1.19 | 0.738 | |
| Eigenvalue | 4.32 | 2.07 | ||
| Variance explained (%) | 36.01 | 17.25 | ||
| Cumulative variance (%) | 36.01 | 53.26 | ||
| Cronbach’s alpha | 0.86 | 0.52 | ||
| No. Abbreviated Item Content | Mean | SD | Factor Loading |
|---|---|---|---|
| QOL1 (“When you are bloated, how often does the bloating limit or restrict your ability to work or attend school?” “Apabila perut anda berasa kembung, berapa kerapkah ia mengehadkan keupayaan anda untuk bekerja atau belajar?”) | 2.24 | 1.00 | 0.818 |
| QOL2 (“When you are bloated, how often does the bloating limit or restrict your ability to participate in social activities?” “Apabila perut anda berasa kembung, berapa kerapkah ia mengehadkan keupayaan anda untuk mengambil bahagian dalam aktiviti sosial?”) | 2.10 | 1.01 | 0.878 |
| QOL3 (“When you are bloated, how often does the bloating limit or restrict your ability to enjoy hobbies or recreational activities?” “Apabila perut anda berasa kembung, berapa kerapkah ia mengehadkan anda daripada menikmati hobi atau aktiviti rekreasi?”) | 1.91 | 0.97 | 0.842 |
| QOL4 (“When you are bloated, how often does the bloating limit or restrict your ability to enjoy intimate relationships?” “Apabila perut anda berasa kembung, berapa kerapkah ia mengehadkan anda daripada menikmati hubungan intim?”) | 1.72 | 1.11 | 0.448 |
| QOL5 (“When you are bloated, how often does the bloating affect you emotionally?” ”Apabila perut anda berasa kembung, berapa kerapkah ia menggangu emosi anda?”) | 2.26 | 0.70 | 0.458 |
| Eigenvalue | 2.94 | ||
| Variance explained (%) | 58.79 | ||
| Cumulative variance (%) | 58.79 | ||
| Cronbach’s alpha | 0.81 | ||
| Path Model * | RMSEA (90% CI) | CFI | TLI | SRMR |
|---|---|---|---|---|
| Severity | ||||
| Model 1 | 0.129 (0.116, 0.143) | 0.776 | 0.721 | 0.084 |
| Model 2 | 0.050 (0.031, 0.067) | 0.966 | 0.956 | 0.051 |
| QoL | ||||
| Model 1 | 0.079 (0.036, 0.127) | 0.975 | 0.949 | 0.021 |
| Model 2 | 0.071 (0.019, 00.125) | 0.985 | 0.962 | 0.021 |
| Constructs/Items | Mean | SD | λ | AVE | CR |
|---|---|---|---|---|---|
| Severity General | 0.550 | 0.831 | |||
| SEVG1 | 1.46 | 0.64 | 0.307 | ||
| SEVG2 * | 2.06 | 0.85 | - | ||
| SEVG3 | 1.79 | 0.75 | 0.604 | ||
| SEVG4 | 2.27 | 0.82 | 0.784 | ||
| SEVG5 | 2.37 | 0.73 | 0.788 | ||
| SEVG6 | 2.31 | 0.72 | 0.783 | ||
| SEVG7 | 2.41 | 0.91 | 0.662 | ||
| Severity 24 h | 0.673 | 0.889 | |||
| SEV241 * | 2.45 | 1.31 | 0.557 | ||
| SEV242 | 1.87 | 0.91 | 0.877 | ||
| SEV243 | 1.76 | 0.86 | 0.877 | ||
| SEV244 | 1.78 | 0.88 | 0.919 | ||
| SEV245 | 2.12 | 1.19 | 0.813 |
| Constructs/Items | Mean | SD | λ | AVE | CR |
|---|---|---|---|---|---|
| Quality of Life | 0.543 | 0.796 | |||
| QOL1 | 2.19 | 0.91 | 0.871 | ||
| QOL2 | 2.17 | 0.90 | 0.774 | ||
| QOL3 | 2.22 | 0.98 | 0.878 | ||
| QOL4 | 3.30 | 1.61 | 0.325 | ||
| QoL5 | 1.44 | 1.01 | 0.433 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahd-Ab.lah, N.; Kueh, Y.C.; Kuan, G.; Yahaya, F.H.; Wong, M.S.; Abd Samat, N.A.; Hamid, N.; Mohamad Nor, N.; Whitehead, W.E.; Thiwan, S.I.; et al. Validity and Reliability of the Malay Versions of Bloating Severity (BSQ-M) and Quality of Life (BLQoL-M) Questionnaires. Int. J. Environ. Res. Public Health 2021, 18, 2487. https://doi.org/10.3390/ijerph18052487
Mahd-Ab.lah N, Kueh YC, Kuan G, Yahaya FH, Wong MS, Abd Samat NA, Hamid N, Mohamad Nor N, Whitehead WE, Thiwan SI, et al. Validity and Reliability of the Malay Versions of Bloating Severity (BSQ-M) and Quality of Life (BLQoL-M) Questionnaires. International Journal of Environmental Research and Public Health. 2021; 18(5):2487. https://doi.org/10.3390/ijerph18052487
Chicago/Turabian StyleMahd-Ab.lah, Nurzulaikha, Yee Cheng Kueh, Garry Kuan, Fatan Hamamah Yahaya, Mung Seong Wong, Nor Aslina Abd Samat, Nurhazwani Hamid, Nurhayati Mohamad Nor, William E. Whitehead, Syed Ismail Thiwan, and et al. 2021. "Validity and Reliability of the Malay Versions of Bloating Severity (BSQ-M) and Quality of Life (BLQoL-M) Questionnaires" International Journal of Environmental Research and Public Health 18, no. 5: 2487. https://doi.org/10.3390/ijerph18052487