
Cardiorespiratory Fitness: Reference on the Six-Minute Walk Test and Oxygen Consumption in Adolescents from South-Central Chile

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Adiposity
3.2. Physical Tests
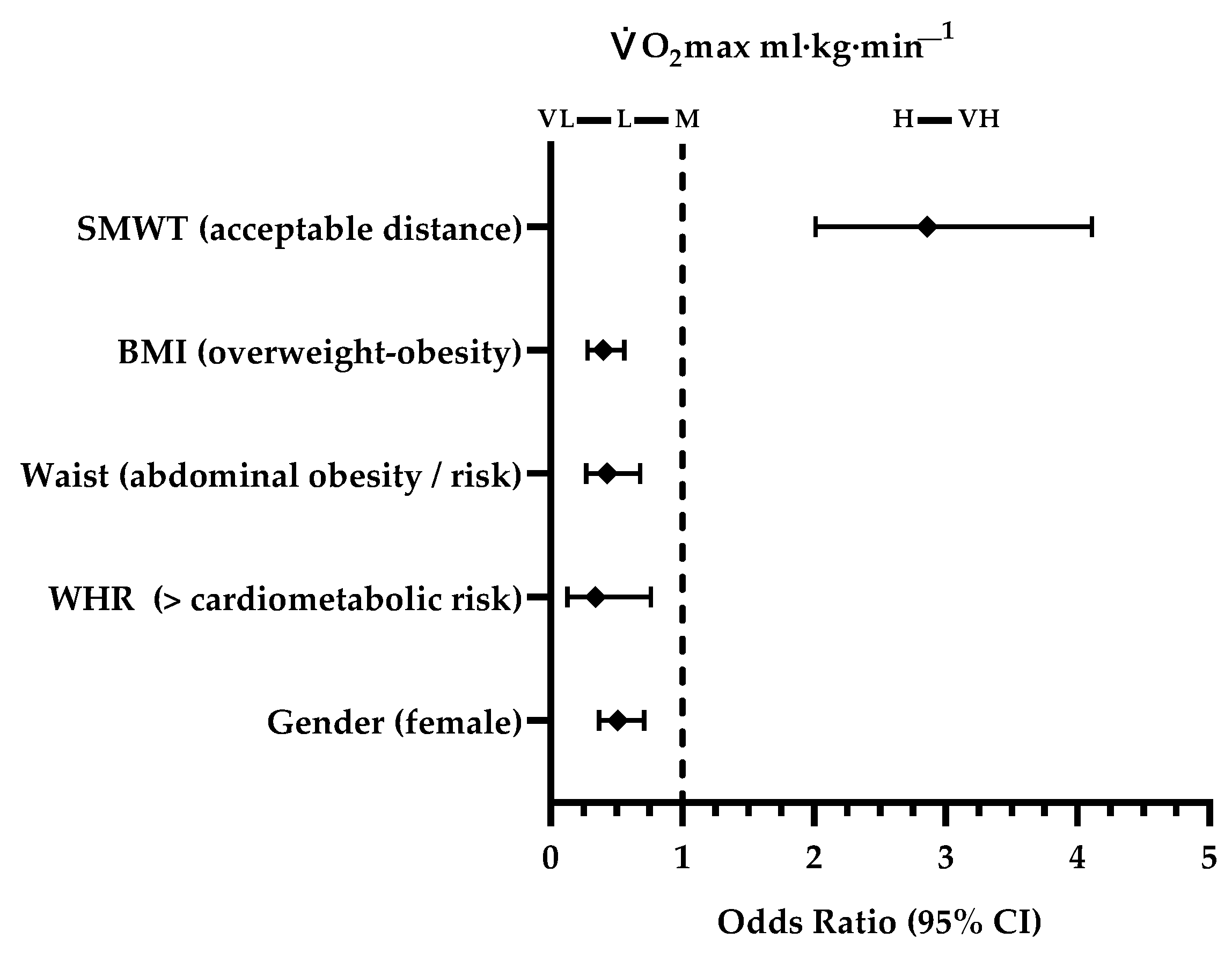
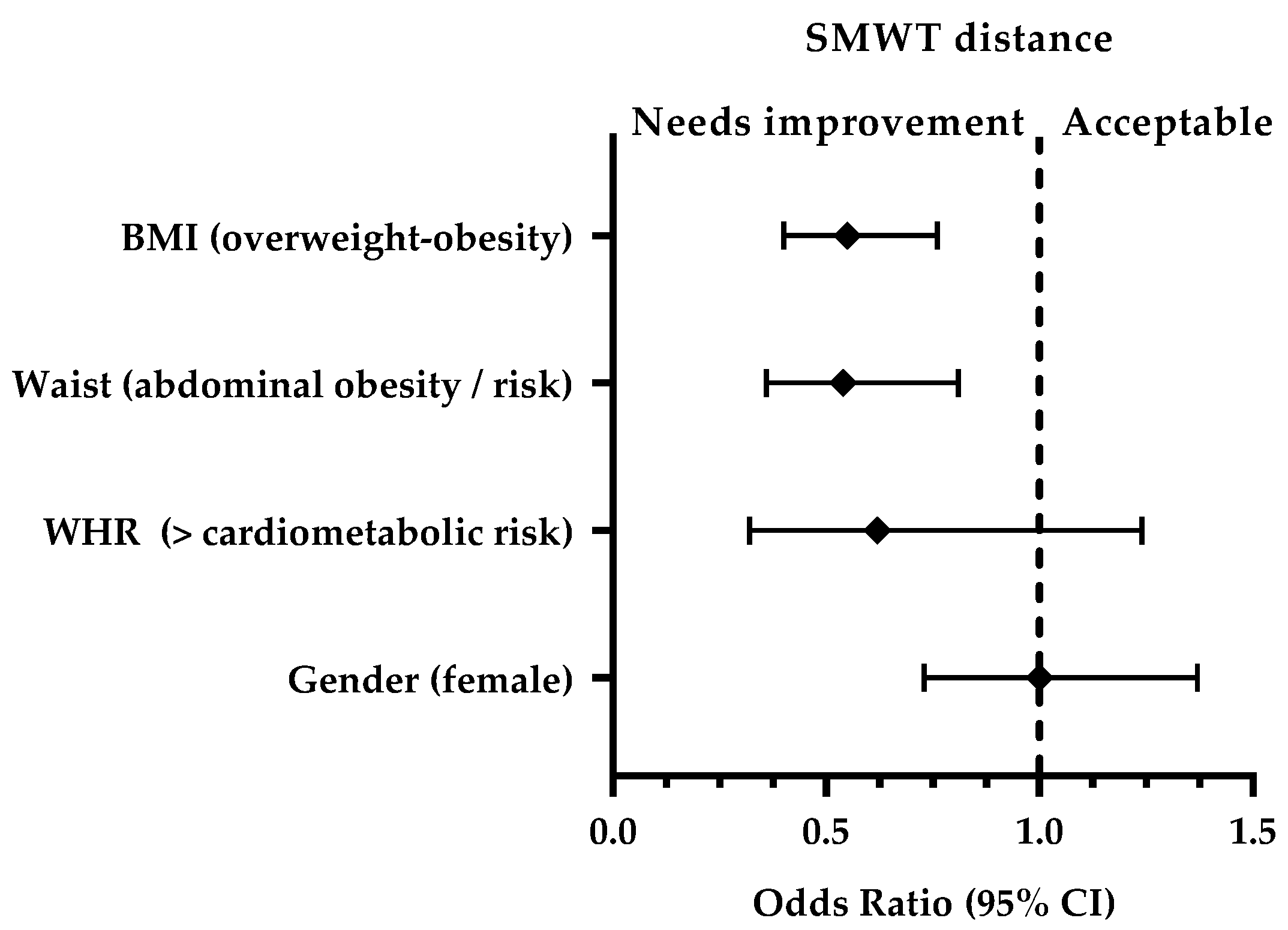
3.3. Cardiorespiratory Fitness and Association with Sociodemographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; Leblanc, A.G.; Belanger, K.; Ortega, F.B.; Léger, L. International normative 20 m shuttle run values from 1,142,026 children and youth representing 50 countries. Br. J. Sports. Med. 2017, 51, 1545–1554. [Google Scholar] [CrossRef] [Green Version]
- De Souza, C.G.; Kaminsky, L.A.; Arena, R.; Christle, J.W.; Arau, C.G.S.; Lima, R.M.; Ashley, E.A.; Myers, J. A reference equation for maximal aerobic power for treadmill and cycle ergometer exercise testing: Analysis from the FRIEND registry. Eur. J. Prev. Cardiol. 2018, 25, 742–750. [Google Scholar] [CrossRef]
- Myers, J.; Kaminsky, L.A.; Lima, R.; Chistle, J.; Ashley, E.; Arena, R. A Reference Equation for Normal Standards for VO2 max: Analysis from the Fitness Registry and the Importance of Exercise National Database (FRIEND Registry). Prog. Cardiovasc. Dis. 2017, 60, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Neto, G.A.M.; Cunha, R.; Pedreiro, D.M.; Oliveira, A.; Machado, S. Estimativa da aptidão cardiorrespiratória da população brasileira de 20 a 59 anos: Abordagem através de modelo sem exercício com variáveis auto-relatadas. J. Phys. Educ. 2019, 30, e3068. [Google Scholar] [CrossRef]
- Peterman, J.E.; Arena, R.; Myers, J.; Marzolini, S.; Ross, R.; Lavie, C.J.; Wisløff, U.; Stensvold, D.; Kaminsky, L.A. Development of Global Reference Standards for Directly Measured Cardiorespiratory Fitness: A Report from the Fitness Registry and Importance of Exercise National Database (FRIEND). Mayo Clin. Proc. 2020, 95, 255–264. [Google Scholar] [CrossRef]
- Ekblom-bak, E.; Ekblom, B.; Söderling, J.; Börjesson, M.; Blom, V.; Kallings, L.V.; Hemmingsson, E.; Andersson, G.; Wallin, P.; Ekblom, Ö. Sex- and age-specific associations between cardiorespiratory fitness, CVD morbidity and all-cause mortality in 266.109 adults. Prev. Med. 2019, 127, e105779. [Google Scholar] [CrossRef]
- Cristi-Montero, C.; Ramírez-Campillo, R.; Álvarez, C.; Garrido, A.; Martínez, M.A.; Díaz, X.; Leiva, A.M.; Salas, C.; Gutiérrez, M.; Sanzana-Inzunza, R.; et al. Fitness cardiorrespiratorio se asocia a una mejora en marcadores metabólicos en adultos chilenos. Rev. Med. Chil. 2016, 144, 980–989. [Google Scholar] [CrossRef] [Green Version]
- Lang, J.J.; Tremblay, M.S.; Ortega, F.B.; Ruiz, J.R.; Tomkinson, G.R. Review of criterion-referenced standards for cardiorespiratory fitness: What percentage of 1 142 026 international children and youth are apparently healthy? Br. J. Sports. Med. 2019, 53, 953–958. [Google Scholar] [CrossRef]
- Prieto-Benavides, D.H.; García-Hermoso, A.; Izquierdo, M.; Alonso-Martínez, A.M.; Agostinis-Sobrinho, C.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Cardiorespiratory fitness cut-points are related to body adiposity parameters in Latin American adolescents. Medicina 2019, 55, 508. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Menezes-Junior, F.J.; Jesus, Í.C.; Mota, J.; Lopes, M.F.A.; Corazza, P.R.P.; Tadiotto, M.C.; Tozo, T.A.A.; Purim, K.S.M.; Ronque, E.R.V.; Leite, N. Validation of equations to estimate the peak oxygen uptake in adolescents from 20 metres shuttle run test. J. Sports. Sci. 2020, 38, 2588–2596. [Google Scholar] [CrossRef]
- Mänttäri, A.; Suni, J.; Sievänen, H.; Husu, P.; Vähä-Ypyä, H.; Valkeinen, H.; Tokola, K.; Vasankari, T. Six-minute walk test: A tool for predicting maximal aerobic power (VO2 max) in healthy adults. Clin. Physiol. Funct Imaging. 2018, 38, 1038–1045. [Google Scholar] [CrossRef]
- Rodríguez-Núñez, I.; Mondaca, F.; Casas, B.; Ferreira, C.; Zenteno, D. Normal values of 6-minute walk test in healthy children and adolescents: A systematic review and meta-analysis. Rev. Chil. Pediatr. 2018, 89, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Mylius, C.F.; Paap, D.; Takken, T. Reference value for the 6-minute walk test in children and adolescents: A systematic review. Expert. Rev. Respir. Med. 2016, 10, 1335–13352. [Google Scholar] [CrossRef]
- Ministerio de Salud. Norma para la Evaluación Nutricional de niños, niñas y Adolescentes de 5 años a 19 años de edad. Subsecretaría de salud pública, División de Políticas Públicas Saludables y Promoción. Departamento de Nutrición y Alimentos. División de Políticas Públicas Saludables y Promoción, Departamento de Nutrición y Alimentos. Available online: https://www.previenesalud.cl/assets/PDF/normas/2016-norma-evaluacion-nutricional.pdf (accessed on 20 June 2020).
- Food and Nutrition Technical Assistance. Tablas de IMC y Tablas de IMC para la Edad, de niños(as) y Adolescentes de 5 a 18 años de edad y Tablas de IMC para Adultos(as) no Embarazadas, no Lactantes ≥ 19 años de edad. Available online: https://www.saludquillota.cl/biblioteca/unidad_infantil/FANTA-BMI-charts-Enero2013-ESPANOL.pdf (accessed on 14 June 2020).
- Aerican Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care. Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Rodríguez-Núñez, I. Measurement scale of child perceived exertion (EPInfant): Validation Chilean children and adolescents. Rev. Chil. Pediatr. 2016, 87, 211–212. [Google Scholar] [CrossRef] [Green Version]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports. Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Cacau, L.D.A.P.; Santana-Filho, D.V.J.; Maynard, L.G.; Neto, M.G.; Fernandes, M.; Carvalho, V.O. Reference values for the six-minute walk test in healthy children and adolescents: A systematic review. Braz. J. Cardiovasc. Surg. 2016, 31, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Saad, H.B.; Prefaut, C.; Missaoui, R.; Mohamed, I.H.; Tabka, Z.; Hayot, M. Reference equation for 6-min walk distance in healthy North African children 6-16 years old. Pediatr. Pulmonol. 2009, 44, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, S.; Hildenbrand, F.F.; Treder, U.; Fischler, M.; Keusch, S.; Speich, R.; Fasnacht, M. Reference values for the 6-minute walk test in healthy children and adolescents in Switzerland. BMC Pulm. Med. 2013, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Kleinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-minute walk test in children and adolescents. J. Pediatr. 2007, 150, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Gatica, D.; Puppo, H.; Villarroel, G.; Martín, I.S.; Lagos, R.; Montecino, J.J.; Lara, C.; Zenteno, D. Valores de referencia del test de marcha de seis minutos en niños sanos. Rev. Med. Chil. 2012, 140, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Buchan, D.S.; Knox, G.; Jones, A.M.; Tomkinson, G.R.; Baker, J.S. Utility of international normative 20 m shuttle run values for identifying youth at increased cardiometabolic risk. J. Sports. Sci. 2019, 37, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Vélez, R.; García-Hermoso, A.; Alonso-Martínez, A.M.; Agostinis-Sobrinho, C.; Correa-Bautista, J.E.; Triana-Reina, H.R.; Izquierdo, M. Cardiorespiratory fitness normative values in latin-american adolescents: Role of fatness parameters. Int. J. Environ. Res. Public Health 2019, 16, 3889. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Miguel, P.A.; Sánchez-Oliva, D.; Vaquero-Solís, M.; Pulido, J.J.; Tapia-Serrano, M.A. Relationship between the average slope in the active commuting to and from school and fitness in adolescents: The mediator role of fatness. PeerJ. 2020, 8, e8824. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Vélez, R.; García-Alonso, Y.; Alonso-Martínez, A.M.; Izquierdo, M. Association of cardiorespiratory fitness levels during youth with health risk later in life. JAMA Pediatr. 2020, 174, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Isasi, C.R.; Strizich, G.M.; Kaplan, R.; Daviglus, M.L.; Sotres-Alvarez, D.; Vidot, D.C.; Llabre, M.M.; Talavera, G.; Carnethon, M. The association of cardiorespiratory fitness with cardiometabolic factors, markers of inflammation, and endothelial dysfunction in Latino youth: Findings from the Hispanic Community Children’s Health Study/Study of Latino Youth. Ann Epidemiol. 2018, 28, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Zapico, A.G.; Fuentes, D.; Rojo-Tirado, M.A.; Calderón, F.J.; Rosenzweig, E.B.; Garofano, R.P. Predicting peak oxygen uptake from the 6-minute walk test in patients with pulmonary hypertension. J. Cardiopulm. Rehabil. Prev. 2016, 36, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmahgoub, S.S.; Van De Velde, A.; Peersman, W.; Cambier, D.; Calders, P. Reproducibility, validity and predictors of six-minute walk test in overweight and obese adolescents with intellectual disability. Disabil. Rehabil. 2012, 34, 846–851. [Google Scholar] [CrossRef]
- Limsuwan, A.; Wongwandee, R.; Khowsathit, P. Correlation between 6-min walk test and exercise stress test in healthy children. Acta. Paediatr. 2010, 99, 438–441. [Google Scholar] [CrossRef]
- Lesser, D.J.; Fleming, M.M.; Maher, C.A.; Kim, S.B.; Woo, M.S.; Keens, T.G. Does the 6-min walk test correlate with the exercise stress test in children? Pediatr Pulmonol. 2010, 45, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Makni, E.; Moalla, W.; Trabelsi, Y.; Lac, G.; Brun, J.F.; Tabka, Z.; Elloumi, M. Six-minute walking test predicts maximal fat oxidation in obese children. Int. J. Obes. 2012, 36, 908–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalili, M.; Nazem, F.; Sazvar, A.; Ranjbar, K. Prediction of maximal oxygen uptake by six-minute walk test and body mass index in healthy boys. J. Pediatr. 2018, 200, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Vanhelst, J.; Fardy, P.S.; Salleron, J.; Béghin, L. The six-minute walk test in obese youth: Reproducibility, validity, and prediction equation to assess aerobic power. Disabil. Rehabil. 2013, 35, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Labonté, J.; Caru, M.; Lemay, V.; Alos, N.; Drouin, S.; Bertout, L.; Andelfinger, G.; Krajinovic, M.; Laverdière, C.; Sinnett, D.; et al. Developing and validating equations to predict O2 peak from the 6MWT in Childhood ALL Survivors. Disabil. Rehabil. 2020, 42, 1–8. [Google Scholar] [CrossRef]
- Vásquez-Gómez, J.A.; Souza de Carvalho, R.; Faundez-Casanova, C.; Castillo-Retamal, F.; Gatica-Mandiola, P.; Castillo-Retamal, M. Capacidad cardiopulmonar en sujetos sanos medida por método directo y prueba de campo. Medicina (B. Aires) 2020, 80, 339–347. [Google Scholar]
- Zebrowska, A.; Zwierzchowska, A. Spirometric values and aerobic efficency of children and adolescents with hearing loss. J. Physiol. Pharmacol. 2006, 57, 443–447. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total (741) | Male (330) | Female (411) | p-Value a | ||||
|---|---|---|---|---|---|---|---|
| Variables | Mean SD | CI | Mean SD | CI | Mean SD | CI | |
| Age (years) | 15.7 (1.1) | (15.7; 15.8) | 15.7 (1.1) | (15.6; 15.9) | 15.8 (1.1) | (15.6; 15.9) | 0.61t |
| Weight (kg) | 62.7 (12.4) | (61.8; 63.6) | 65.7 (13.6) | (64.2; 67.1) | 60.3 (10.9) | (59.3; 61.4) | <0.001u |
| Height (m) | 1.64 (0.08) | (1.63; 1.65) | 1.70 (0.06) | (1.69; 1.71) | 1.59 (0.06) | (1.59; 1.6) | <0.001u |
| BMI (kg·m−2) | 23.1 (3.9) | (22.8; 23.4) | 22.5 (4) | (22.1; 23) | 23.5 (3.8) | (23.2; 23.9) | <0.001u |
| Waist (cm) | 76.1 (9.7) | (75.2; 76.8) | 78.5 (10.6) | (77.2; 79.8) | 74 (8.4) | (73.1; 75) | <0.001u |
| Normal (n, %) | 459 (76.9) | (73.2; 80.2) | 187 (70.3) | (64.4; 75.7) | 272 (82.2) | (77.6; 86.1) | |
| Abdominal obesity (n, %) | 30 (5) | (3.4; 7.1) | 21 (7.9) | (4.9; 11.8) | 9 (2.7) | (1.2; 5) | |
| Obesity risk ab (n, %) | 108 (18.1) | (15.1; 21.4) | 58 (21.8) | (16.9; 27.2) | 50 (15.1) | (11.4; 19.4) | |
| Total (n, %) | 597 (100) | 266 (100) | 331 (100) | ||||
| WHR | 0.46 (0.05) | (0.46; 0.47) | 0.45 (0.06) | (0.45; 0.47) | 0.46 (0.05) | (0.46; 0.47) | 0.09u |
| <CM risk (n, %) | 554 (92.8) | (90.4; 94.7) | 244 (91.7) | (87.7; 94.7) | 310 (93.7) | (90.4; 96) | |
| >CM risk (n, %) | 43 (7.2) | (5.2; 9.5) | 22 (8.3) | (5.2; 12.2) | 21 (6.3) | (3.9; 9.5) | |
| Total (n, %) | 597 (100) | 266 (100) | 331 (100) | ||||
| Total (741) | Male (330) | Female (411) | p-Value a | ||||
|---|---|---|---|---|---|---|---|
| Variables | Mena SD | CI | Mena SD | CI | Mena SD | CI | |
| SMWT | |||||||
| Distance (m) | 668.2 (82.7) | (662.2; 674.1) | 699.8 (84.8) | (690.6; 709) | 642.8 (71.7) | (635.8; 649.7) | <0.001u |
| HR (beats·min−1) | 138 (27) | (136; 140) | 138 (27) | (135.2; 141) | 138 (28) | (135.6; 141) | 0.985u |
| HR (%) | 67.7 (13.6) | (66.7; 68.7) | 67.6 (13.3) | (66.2; 69.1) | 67.7 (13.8) | (66.4; 69.1) | 0.994u |
| RPE | 3.7 (1.7) * | (3.6; 3.8) | 3.6 (1.8) ** | (3.4; 3.8) | 3.8 (1.6) *** | (3.7; 4) | 0.039u |
| Distance (category) | |||||||
| Acceptable (n, %) | 472 (63.7) | (0.6; 0.67) | 210 (63.6) | (58.1; 68.8) | 262 (63.8) | (58.8; 68.4) | |
| Needs improvement (n, %) | 269 (36.3) | (0.32; 0.39) | 120 (36.4) | (31.1; 41.8) | 149 (36.2) | (31.5; 41.1) | |
| Course Navette | |||||||
| Bearing | 4.8 (2.1) | (4.6; 4.9) | 6.1 (2) | (5.8; 6.3) | 3.7 (1.5) | (3.6; 3.9) | <0.001u |
| Speed (km·h−1) | 10.3 (1.2) | (10.2; 10.4) | 11 (1.) | (10.9; 11.2) | 9.7 (1) | (9.6; 9.8) | <0.001u |
| V̇O2max (ml·kg·min−1) | 38.3 (7.1) | (37.8; 38.8) | 42.5 (6.4) | (41.8; 43.2) | 35 (5.7) | (34.4; 35.5) | <0.001u |
| V̇O2max (L·min−1) | 2.4 (0.6) | (2.3; 2.4) | 2.7 (0.6) | (2.7; 2.8) | 2.1 (0.4) | (2; 2.1) | <0.001u |
| RPE | 8 (1.6) + | (7.8; 8.1) | 8 (1.5) ++ | (7.8; 8.3) | 7.9 (1.7) +++ | (7.7; 8.1) | 0.57u |
| V̇O2max (category) ml·kg·min−1 | |||||||
| Very low (n, %) | 166 (22.4) | (0.19; 0.25) | 78 (23.6) | (19.1; 28.5) | 88 (21.4) | (17.5; 25.6) | |
| Low (n, %) | 291 (39.3) | (0.35; 0.42) | 88 (26.6) | (21.9; 31.7) | 203 (49.4) | (44.4; 54.3) | |
| Moderate (n, %) | 18 (2.4) | (1.4; 3.8) | 18 (5.5) | (3.2; 8.4) | 0 | 0 | |
| High (n, %) | 202 (27.3) | (24; 30) | 126 (38.2) | (32.9; 43.6) | 76 (18.5) | (14.8; 22.5) | |
| Very high (n, %) | 64 (8.6) | (6.7; 10.8) | 20 (6.1) | (3.7; 9.2) | 44 (10.7) | (7.8; 14.1) | |
| Age | p10 | CI | p20 | CI | p30 | CI | p40 | CI | p50 | CI | p60 | CI | p70 | CI | p80 | CI | p90 | CI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | ||||||||||||||||||
| 13 | 430 | 390; 613 | 578 | 390; 623 | 612 | 418; 630 | 621 | 519; 666 | 630 | 604; 686 | 642 | 617; 726 | 676 | 622; 760 | 700 | 630; 768 | 757 | 673; 768 |
| 14 | 551 | 522; 580 | 600 | 570; 610 | 612 | 600; 630 | 630 | 612; 640 | 644 | 630; 660 | 660 | 648; 670 | 675 | 660; 690 | 690 | 678; 700 | 707 | 690; 761 |
| 15 | 570 | 541; 600 | 610 | 600; 621 | 622 | 611; 630 | 630 | 624; 640 | 643 | 630; 660 | 660 | 645; 690 | 690 | 660; 700 | 705 | 690; 720 | 720 | 714; 756 |
| 16 | 552 | 540; 580 | 590 | 566; 609 | 609 | 592; 615 | 616 | 609; 639 | 639 | 615; 660 | 660 | 638; 672 | 672 | 660; 690 | 690 | 673; 711 | 720 | 700; 755 |
| 17 | 549 | 506; 570 | 594 | 562; 610 | 610 | 600; 627 | 627 | 610; 642 | 641 | 627; 660 | 660 | 640; 680 | 680 | 660; 696 | 698 | 680; 716 | 720 | 710; 769 |
| Male | ||||||||||||||||||
| 13 | 497 | 480; 585 | 576 | 480; 600 | 586 | 503; 610 | 598 | 572; 653 | 607 | 585; 744 | 620 | 591; 759 | 730 | 603; 785 | 756 | 610; 880 | 810 | 740; 880 |
| 14 | 600 | 585; 620 | 631 | 602; 651 | 658 | 636; 675 | 675 | 658; 695 | 690 | 675; 720 | 720 | 690; 646 | 745 | 720; 780 | 780 | 750; 810 | 826 | 802; 867 |
| 15 | 630 | 609; 656 | 660 | 637; 690 | 690 | 660; 702 | 702 | 690; 730 | 730 | 700; 750 | 750 | 730; 758 | 758 | 750; 786 | 790 | 763; 810 | 836 | 800; 916 |
| 16 | 582 | 560; 614 | 630 | 590; 641 | 644 | 630; 670 | 670 | 643; 690 | 690 | 670; 696 | 695 | 689; 716 | 715 | 695; 727 | 729 | 716; 750 | 759 | 730; 781 |
| 17 | 605 | 542; 633 | 650 | 612; 665 | 664 | 645; 680 | 678 | 661; 690 | 690 | 674; 707 | 700 | 690; 745 | 735 | 699; 770 | 770 | 731; 786 | 790 | 770; 800 |
| Age | p10 | CI | p20 | CI | p30 | CI | p40 | CI | p50 | CI | p60 | CI | p70 | CI | p80 | CI | p90 | CI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | ||||||||||||||||||
| 13 | 30.8 | 30.8; 37.4 | 36.1 | 30.8; 37.5 | 37.4 | 30.8; 37.6 | 37.5 | 32.6; 37.7 | 37.5 | 37.4; 38.2 | 37.6 | 37.5; 42.6 | 37.7 | 37.5; 44.1 | 39.6 | 37.6; 44.2 | 44.1 | 37.4; 44.2 |
| 14 | 29.3 | 29.2; 29.8 | 30.1 | 29.6; 35.5 | 35.7 | 30.3; 35.9 | 35.9 | 35.7; 36.2 | 36.2 | 35.9; 36.3 | 36.3 | 36.2; 36.7 | 36.8 | 36.3; 37.2 | 37.2 | 36.8; 42.7 | 43.1 | 42.4; 43.6 |
| 15 | 27.6 | 27.4; 27.8 | 28.3 | 27.9; 33.8 | 33.9 | 28.4; 34.5 | 34.5 | 34; 34.7 | 34.8 | 34.5; 35.2 | 35.2 | 34.9; 35.4 | 35.4 | 35.2; 40.9 | 41.1 | 40.7; 41.6 | 41.8 | 41.3; 45.7 |
| 16 | 25.7 | 25.2; 26.5 | 26.7 | 26; 32.3 | 32.3 | 28.7; 32.9 | 32.9 | 32.3; 33.2 | 33.2 | 32.9; 39 | 37.9 | 33.2; 39.4 | 39.4 | 38.1; 39.8 | 40 | 39.4; 41.1 | 46 | 40.3; 46.6 |
| 17 | 24 | 23.8; 30.5 | 30.6 | 24.3; 31 | 31 | 30.7; 31.2 | 31.2 | 31; 31.5 | 31.5 | 31.2; 31.7 | 31.6 | 31.5; 37.9 | 37.9 | 31.6; 38.4 | 38.5 | 37.9; 38.6 | 38.6 | 38.5; 38.8 |
| Male | ||||||||||||||||||
| 13 | 30.9 | 30.8; 37.5 | 33.5 | 30.8; 43.7 | 37.5 | 30.8; 43.9 | 42.5 | 31.8; 44.1 | 43.9 | 37.4; 47 | 44 | 38.6; 50.4 | 44.1 | 43.9; 50.5 | 50.3 | 44; 50.6 | 50.5 | 45; 50.6 |
| 14 | 35.8 | 35.5; 36.1 | 36.3 | 35.9; 36.2 | 36.6 | 36.3; 42.4 | 42.4 | 36.7; 42.9 | 42.9 | 42.3; 43.5 | 43.4 | 42.9; 49.1 | 49.1 | 43.4; 49.3 | 49.3 | 49.2; 49.6 | 49.7 | 49.4; 49.9 |
| 15 | 35 | 34.5; 40.6 | 40.7 | 35.2; 41 | 41.1 | 40.7; 41.4 | 41.4 | 41.1; 42 | 41.9 | 41.4; 47.6 | 47.6 | 41.9; 48 | 48 | 47.6; 48.3 | 48.3 | 48; 48.4 | 48.4 | 48.3; 49.7 |
| 16 | 32.7 | 26.1; 33.3 | 33.4 | 32.9; 39.1 | 39.1 | 33.4; 39.7 | 39.7 | 39.1; 40.1 | 40.1 | 39.7; 46.3 | 46.3 | 40.1; 46.5 | 46.5 | 46.3; 46.9 | 46.9 | 46.5; 47.3 | 47.3 | 47; 53.6 |
| 17 | 31.4 | 30.9; 37.9 | 37.9 | 31.4; 38.4 | 38.4 | 37.9; 39.2 | 38.8 | 38.3; 45 | 45 | 38.7; 45.3 | 45.2 | 44.9; 45.5 | 45.5 | 45.2; 45.6 | 45.6 | 45.5; 45.9 | 49 | 45.5; 52.5 |
| Non-Standardized Coefficients | 95% CI for B | |||||
|---|---|---|---|---|---|---|
| B | Standard Error | t | p-Value | Lower Limit | UPPER LIMIT | |
| Constant | −7.21133 | 0.4261 | −16.921 | <0.001 | −8.0483 | −6.3743 |
| Gender | 0.24301 | 0.0427 | 5.684 | <0.001 | 0.159 | 0.3269 |
| HRr | −0.00257 | 0.0005 | −4.555 | <0.001 | −0.0036 | −0.0014 |
| Height | 3.97109 | 0.2574 | 15.424 | <0.001 | 3.4654 | 4.4767 |
| Distance | 0.00148 | 0.0002 | 7.054 | <0.001 | 0.0011 | 0.0018 |
| WHR | 4.52351 | 0.2912 | 15.533 | <0.001 | 3.9515 | 5.0954 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Gómez, J.; Gatica Salas, N.; Jiménez Villarroel, P.; Rojas-Araya, L.; Faundez-Casanova, C.; Castillo-Retamal, M. Cardiorespiratory Fitness: Reference on the Six-Minute Walk Test and Oxygen Consumption in Adolescents from South-Central Chile. Int. J. Environ. Res. Public Health 2021, 18, 2474. https://doi.org/10.3390/ijerph18052474
Vásquez-Gómez J, Gatica Salas N, Jiménez Villarroel P, Rojas-Araya L, Faundez-Casanova C, Castillo-Retamal M. Cardiorespiratory Fitness: Reference on the Six-Minute Walk Test and Oxygen Consumption in Adolescents from South-Central Chile. International Journal of Environmental Research and Public Health. 2021; 18(5):2474. https://doi.org/10.3390/ijerph18052474
Chicago/Turabian StyleVásquez-Gómez, Jaime, Nelson Gatica Salas, Pedro Jiménez Villarroel, Luis Rojas-Araya, Cesar Faundez-Casanova, and Marcelo Castillo-Retamal. 2021. "Cardiorespiratory Fitness: Reference on the Six-Minute Walk Test and Oxygen Consumption in Adolescents from South-Central Chile" International Journal of Environmental Research and Public Health 18, no. 5: 2474. https://doi.org/10.3390/ijerph18052474