
Functional Upper Airway Space Endoscopy: A Prognostic Indicator in Obstructive Sleep Apnea Treatment with Mandibular Advancement Devices

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Patients Evaluation
2.4. Endoscopy and Evaluation Methods
- -
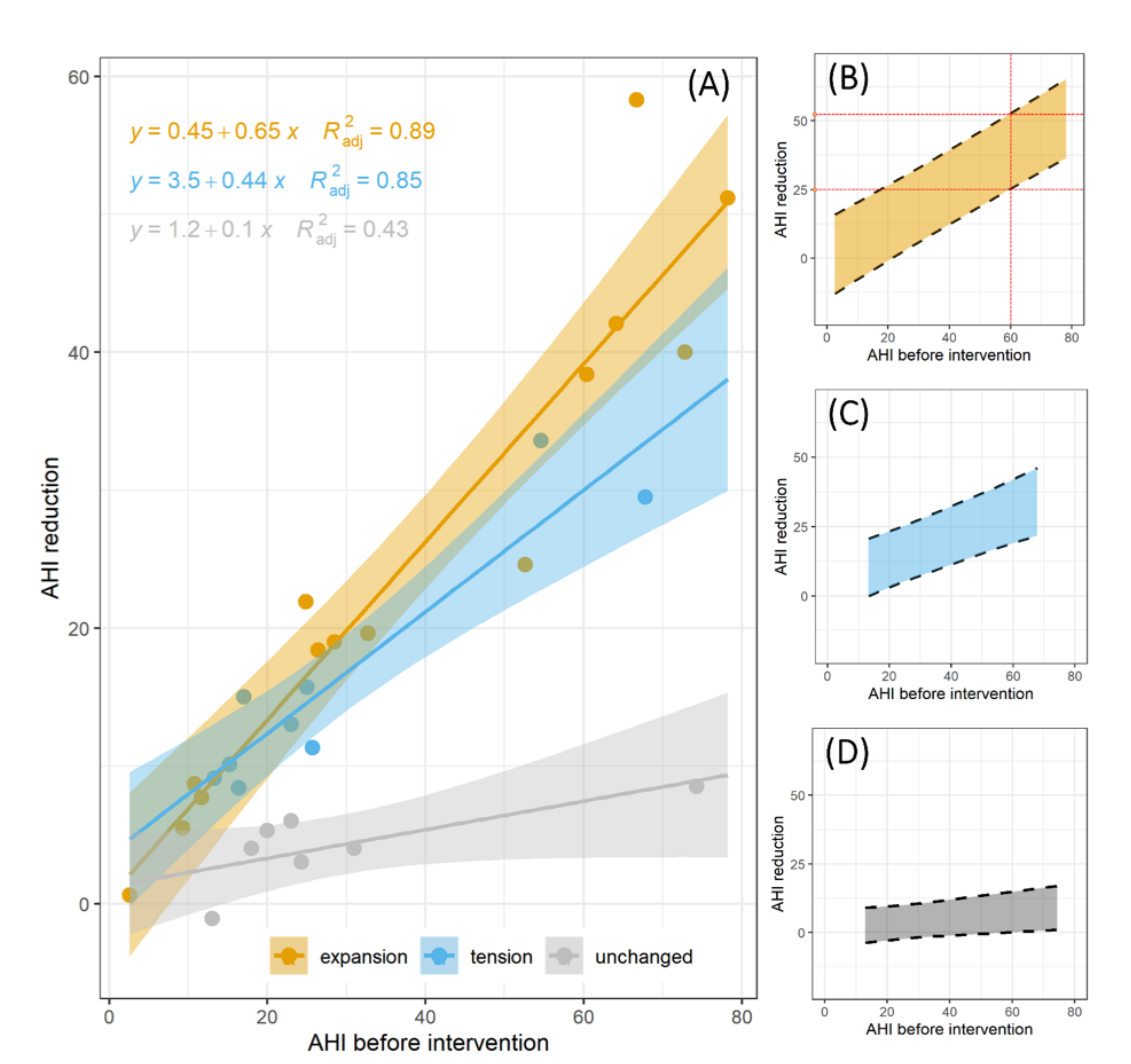
- with a significant (>25%) widening of the airspace [enlargement-expansion (e)];
- -
- with a stretch (<25%) of tissue only slightly affecting the airspace [stretch (s)];
- -
- without a response, i.e., the airway’s volume remains unchanged [unchanged (U)].
2.5. Polysomnography
2.6. Oral Device
2.7. Statistical Analysis
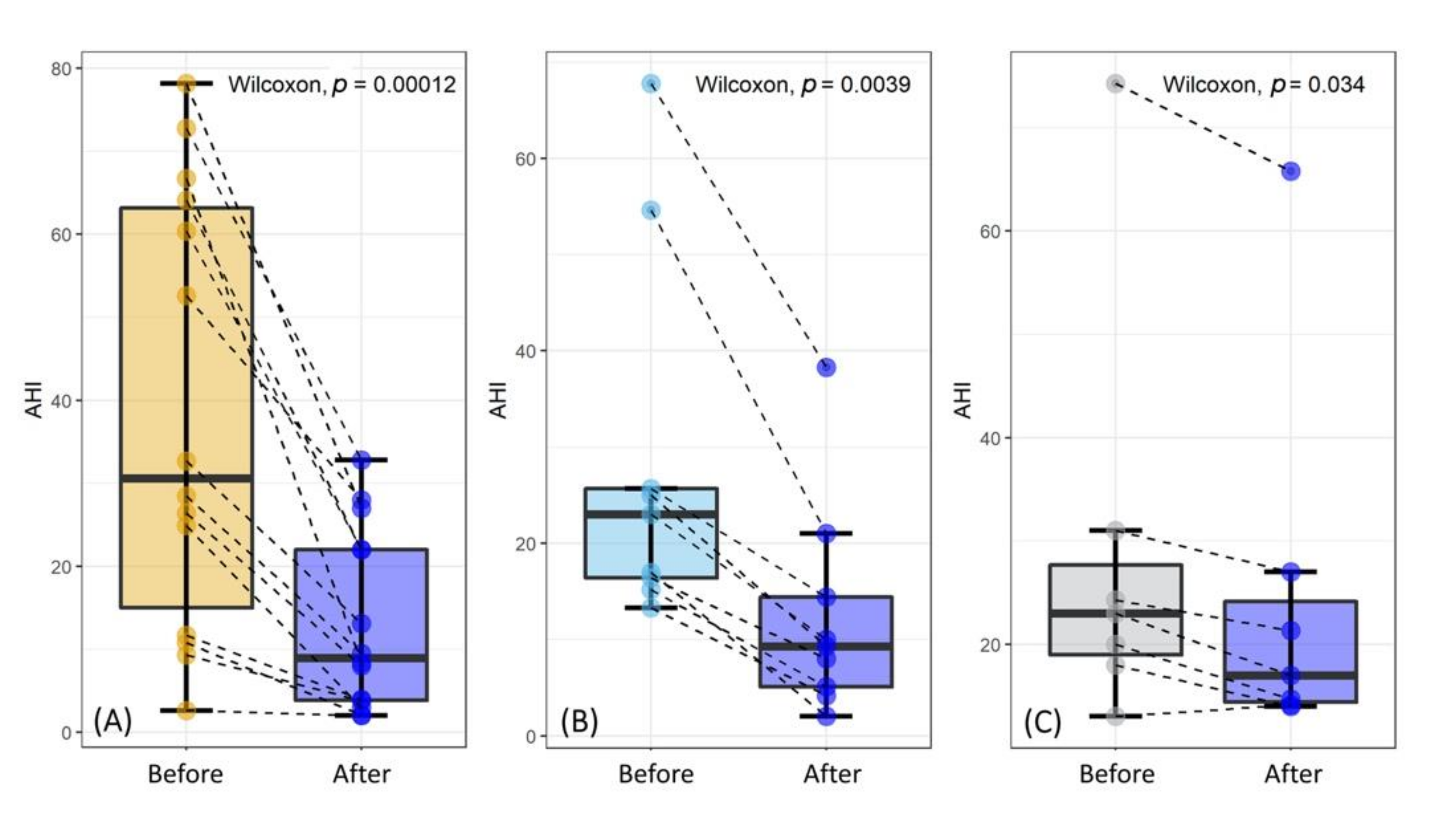
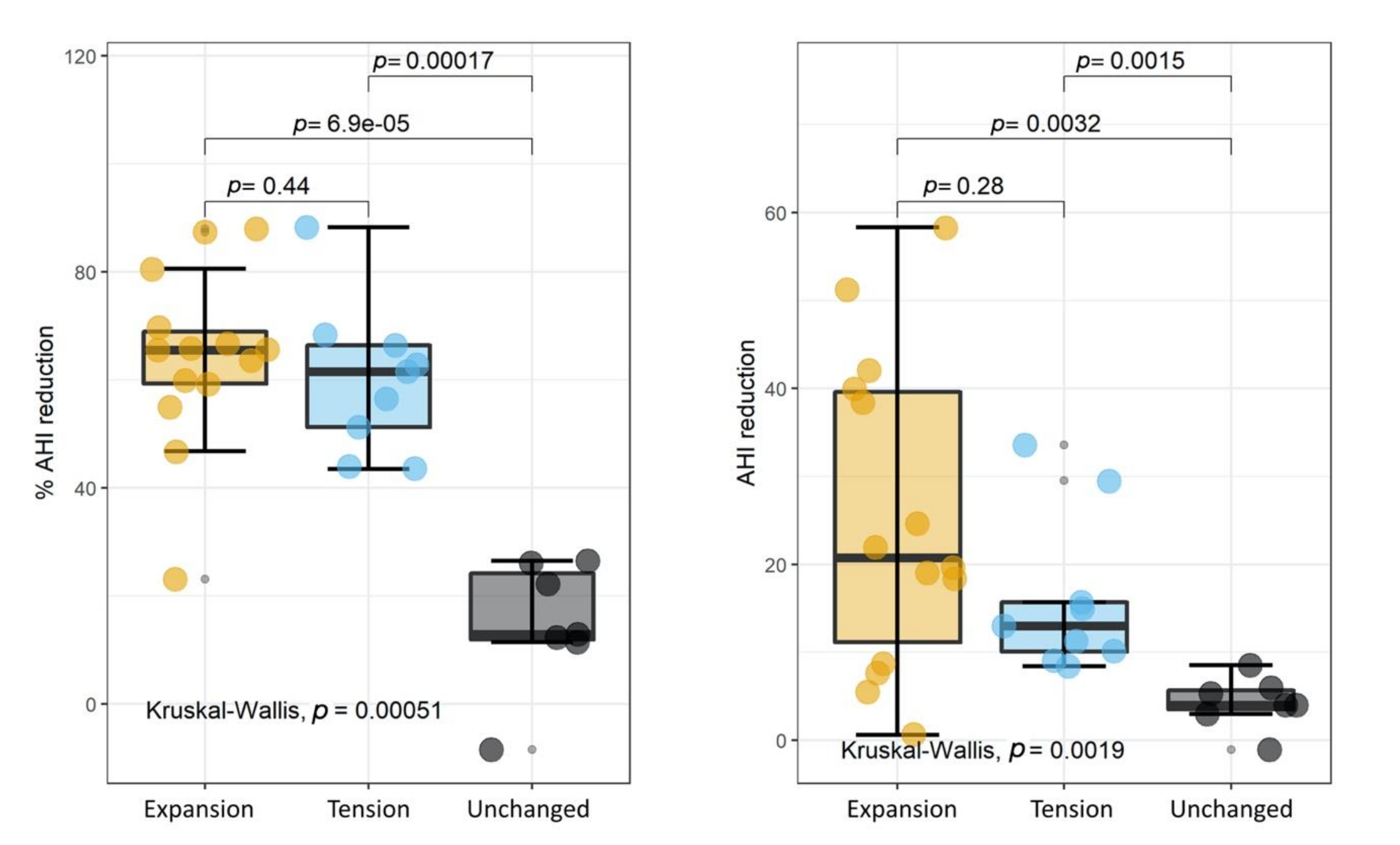
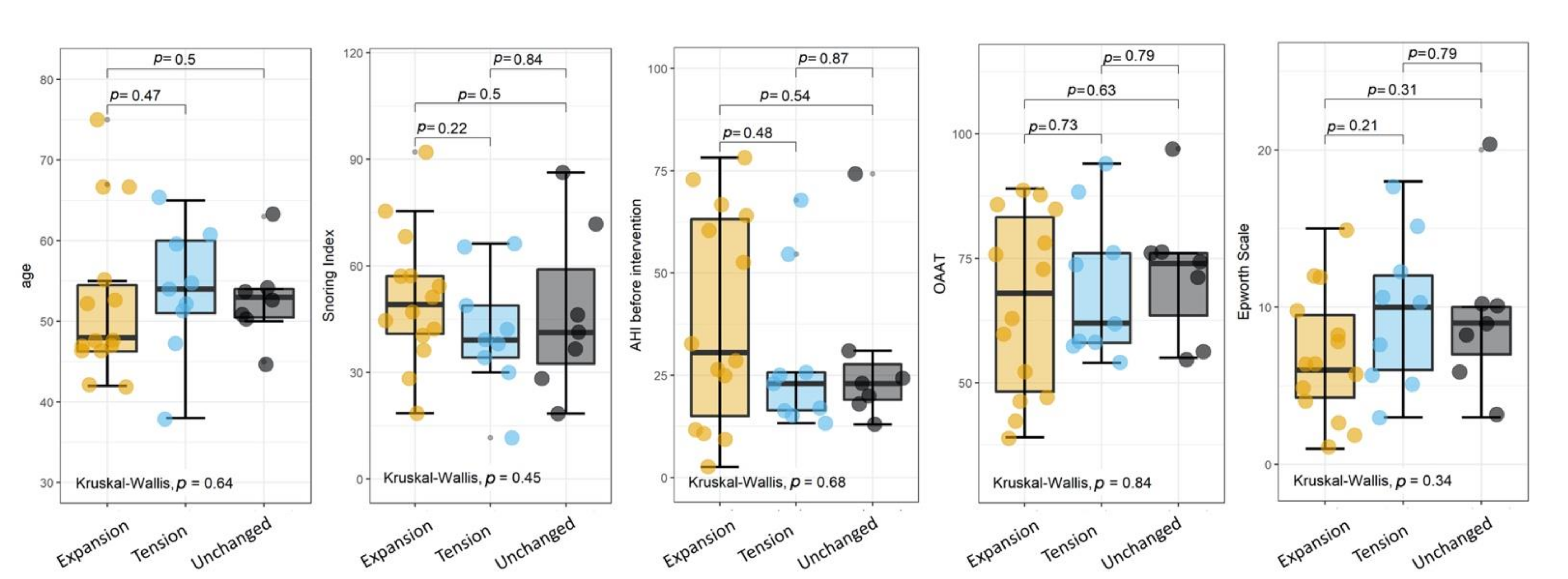
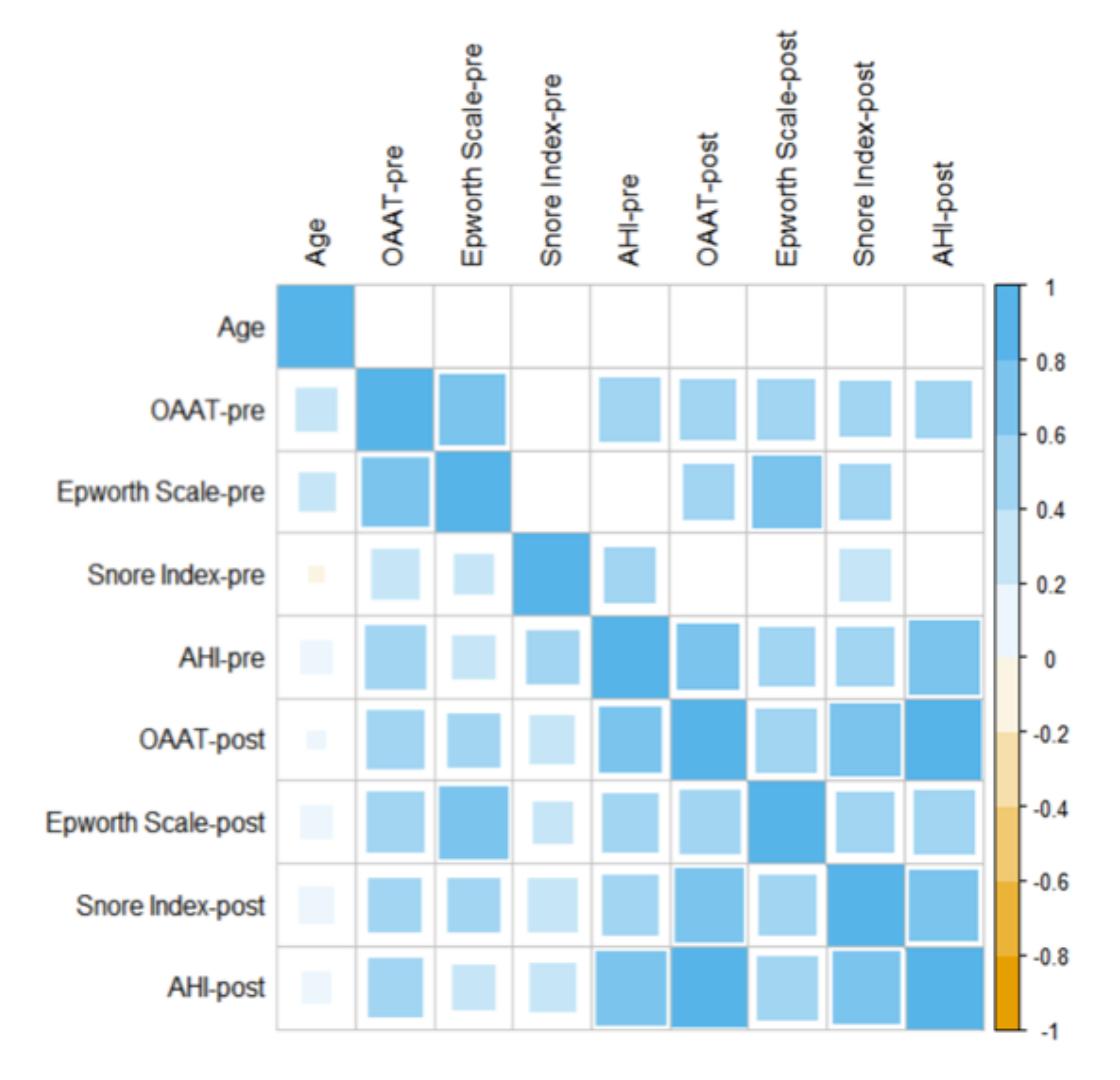
3. Results
4. Discussion
- -
- it is based on drug-induced sleep, and there are documented problems and concerns about the safety, efficacy, and methods of administration of these drugs;
- -
- patient hospitalization is needed for procedure execution;
- -
- it is performed during an intermittent short sleep cycle and does not permit examination of multiple airway levels simultaneously during the same cycle;
- -
- there are no clear standards for therapy with MAD planning based on data of the degree/pattern of obstruction;
- -
- the validity and reliability of DISE results are yet uncertain;
- -
- it is costly and not widely available for many patients.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mantovani, M.; Rinaldi, V.; Torretta, S.; Carioli, D.; Salamanca, F.; Pignataro, L. Barbed Roman blinds technique for the treatment of obstructive sleep apnea: How we do it? Eur. Arch. Otorhinolaryngol. 2016, 273, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Magliulo, G.; Di Luca, M.; De Vito, A.; Meccariello, G.; Cammaroto, G.; Pelucchi, S.; Bonsembiante, A.; Maniaci, A.; Vicini, C. Lateral pharyngoplasty techniques for obstructive sleep apnea syndrome: A comparative experimental stress test of two different techniques. Eur. Arch. Otorhinolaryngol. 2020, 277, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, M.; Carioli, D.; Torretta, S.; Rinaldi, V.; Ibba, T.; Pignataro, L. Barbed snore surgery for concentric collapse at the velum: The Alianza technique. J. Craniomaxillofac. Surg. 2017, 45, 1794–1800. [Google Scholar] [CrossRef]
- Di Luca, M.; Iannella, G.; Montevecchi, F.; Magliulo, G.; De Vito, A.; Cocuzza, S.; Maniaci, A.; Meccariello, G.; Cammaroto, G.; Sgarzani, R.; et al. Use of the transoral robotic surgery to treat patients with recurrent lingual tonsillitis. Int. J. Med. Robot. 2020, 16, e2106. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Vallicelli, B.; Magliulo, G.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Greco, A.; Pelucchi, S.; Sgarzani, R.; Corso, R.M.; et al. Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment. Int. J. Environ. Res. Public Health 2020, 27, 1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: An American Academy of Sleep Medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Carvalho, F.R.; Lentini-Oliveira, D.A.; Prado, L.B.; Prado, G.F.; Carvalho, L.B. Oral appliances and functional orthopaedic appliances for obstructive sleep apnoea in children. Cochrane Database Syst. Rev. 2016, 5, CD005520. [Google Scholar] [CrossRef]
- Vicini, C.; Colabianchi, V.; Giorgio Marrano, G.; Barbanti, F.; Spedicato, G.A.; Lombardo, L.; Siciliani, G. Description of the relationship between NOHL classification in drug-induced sleep endoscopy and initial AHI in patients with moderate to severe OSAS, and evaluation of the results obtained with oral appliance therapy. Acta Otorhinolaryngol. Ital. 2020, 40, 50–56. [Google Scholar] [CrossRef]
- Vito, A.; Cammaroto, G.; Chong, K.B.; Carrasco-Llatas, M.; Vicini, C. Drug-Induced Sleep Endoscopy: Clinical Application and Surgical Outcomes. Healthcare 2019, 25, 100. [Google Scholar] [CrossRef] [Green Version]
- Gasparini, G.; Vicini, C.; De Benedetto, M.; Salamanca, F.; Sorrenti, G.; Romandini, M.; Bosi, M.; Saponaro, G.; Foresta, E.; Laforì, A.; et al. Diagnostic Accuracy of Obstructive Airway Adult Test for Diagnosis of Obstructive Sleep Apnea. Biomed. Res. Int. 2015, 2015, 915185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicini, C.; De Vito, A.; Benazzo, M.; Frassineti, S.; Campanini, A.; Frasconi, P.; Mira, E. The nose oropharynx hypopharynx and larynx (NOHL) classification: A new system of diagnostic standardized examination for OSAHS patients. Eur. Arch. Otorhinolaryngol. 2012, 269, 1297–1300. [Google Scholar] [CrossRef] [PubMed]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.; Quan, S.F.; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 15, 597–619. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R software: Version 3.5.1. R Found Stat Comput Published Online First: 2018. [CrossRef] [Green Version]
- Gulli, F.; Napodano, C.; Marino, M.; Ciasca, G.; Pocino, K.; Basile, V.; Visentini, M.; Stefanile, A.; Todi, L.; De Spirito, M.; et al. Serum immunoglobulin free light chain levels in systemic autoimmune rheumatic diseases. Clin. Exp. Immunol. 2020, 199, 163–171. [Google Scholar] [CrossRef]
- Taiyun, W.; Simko, V. corrplot: Visualization of a Correlation Matrix; R Package Version 0.73 230.231. Available online: https://github.com/taiyun/corrplotx (accessed on 28 February 2020).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef] [Green Version]
- Petri, N.; Christensen, I.J.; Svanholt, P.; Sonnesen, L.; Wildschiødtz, G.; Berg, S. Mandibular advancement device therapy for obstructive sleep apnea: A prospective study on predictors of treatment success. Sleep Med. 2019, 54, 187–194. [Google Scholar] [CrossRef]
- Askar, S.M.; Quriba, A.S.; Hassan, E.M.; Awad, A.M. Positional Awake Endoscopy Versus DISE in Assessment of OSA: A Comparative Study. Laryngoscope 2019, 130, 2269–2274. [Google Scholar] [CrossRef]
- Vroegop, A.V.; Vanderveken, O.M.; Verbraecken, J.A. Drug-Induced Sleep Endoscopy: Evaluation of a Selection Tool for Treatment Modalities for Obstructive Sleep Apnea. Respiration 2020, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kastoer, C.; Op de Beeck, S.; Dom, M.; Neirinckx, T.; Verbraecken, J.; Braem, M.J.; Van de Heyning, P.H.; Nadjmi, N.; Vanderveken, O.M. Drug-Induced Sleep Endoscopy Upper Airway Collapse Patterns and Maxillomandibular Advancement. Laryngoscope 2020, 130, E268–E274. [Google Scholar] [CrossRef] [PubMed]
- Sasao, Y.; Nohara, K.; Okuno, K.; Nakamura, Y.; Sakai, T. Videoendoscopic diagnosis for predicting the response to oral appliance therapy in severe obstructive sleepapnea. Sleep Breath. 2014, 18, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Okuno, K.; Sasao, Y.; Nohara, K.; Sakai, T.; Pliska, B.T.; Lowe, A.A.; Ryan, C.F.; Almeida, F.R. Endoscopy evaluation to predict oral appliance outcomes in obstructive sleep apnoea. Eur. Respir. J. 2016, 47, 1410–1419. [Google Scholar] [CrossRef] [PubMed]
- Okuno, K.; Ikai, K.; Matsumura-Ai, E.; Araie, T. Titration technique using endoscopy for an oral appliance treatment of obstructive sleep apnea. J. Prosthet. Dent. 2018, 119, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Tanyeri, H.; La Rosa, M.; Landsberg, R.; Vaidyanathan, K.; Pieri, S.; Caldarelli, D. Clinical predictors of obstructive sleep apnea. Laryngoscope 1999, 109, 1901–1907. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Enlargement | Stretch | Unchanged | p-Value | ||
|---|---|---|---|---|---|---|
| 1 | Number | 30 | 14 | 9 | 7 | 0.273 |
| 2 | Age, years [median (IQR)] | 52 (8) | 48 (8.25) | 54 (9) | 53 (3.5) | 0.640 |
| 3 | Male [N (%)]–Female [N (%)] | 23 (77)–7 (23) | 11 (79)–3 (21) | 5 (56)–4 (44) | 7 (100)–0 (0) | 0.173 |
| 4 | Pre-treatment AHI [median (IQR)] | 25,35 (39.2) | 42,65 (42.25) | 23 (9.3) | 23 (8.65) | 0.680 |
| 5 | Post-treatment AHI [median (IQR)] | 14 (14) | 8,95 (18.15) | 9.65 (8775) | 17 (9.75) | 0.130 |
| 6 | Pre-treatment Epworth Scale [median (IQR)] | 8 (5.5) | 6 (5.25) | 10 (6) | 9 (3) | 0.340 |
| 7 | Post-treatment Epworth Scale [median (IQR)] | 5 (4) | 4 (3.25) | 7 (6) | 5 (0.5) | 0.420 |
| 8 | Pre-treatment Snoring Index [median (IQR)] | 43.45 (20.775) | 49.15 (16.225) | 39.2 (14.7) | 41.3 (26.5) | 0.450 |
| 9 | Post-treatment Snoring Index [median (IQR)] | 21.24 (24.55) | 16 (12.15) | 11.3 (17.8) | 36.2 (25.4) | 0.011 |
| 10 | Pre-treatment OAAT [median (IQR)] | 72 (21.25) | 68 (35) | 62 (18) | 74 (1.,5) | 0.840 |
| 11 | Post-treatment OAAT [median (IQR)] | 40.5 (27.5) | 39 (24) | 34 (19) | 58 (26.5) | 0.037 |
| Group | Regression Coefficient | p |
|---|---|---|
| Expansion | 4.7 e–7 | |
| Tension | 0.00044 | |
| Unchanged | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparini, G.; Saponaro, G.; Todaro, M.; Ciasca, G.; Cigni, L.; Doneddu, P.; Azzuni, C.; Foresta, E.; De Angelis, P.; Barbera, G.; et al. Functional Upper Airway Space Endoscopy: A Prognostic Indicator in Obstructive Sleep Apnea Treatment with Mandibular Advancement Devices. Int. J. Environ. Res. Public Health 2021, 18, 2393. https://doi.org/10.3390/ijerph18052393
Gasparini G, Saponaro G, Todaro M, Ciasca G, Cigni L, Doneddu P, Azzuni C, Foresta E, De Angelis P, Barbera G, et al. Functional Upper Airway Space Endoscopy: A Prognostic Indicator in Obstructive Sleep Apnea Treatment with Mandibular Advancement Devices. International Journal of Environmental Research and Public Health. 2021; 18(5):2393. https://doi.org/10.3390/ijerph18052393
Chicago/Turabian StyleGasparini, Giulio, Gianmarco Saponaro, Mattia Todaro, Gabriele Ciasca, Lorenzo Cigni, Piero Doneddu, Camillo Azzuni, Enrico Foresta, Paolo De Angelis, Giorgio Barbera, and et al. 2021. "Functional Upper Airway Space Endoscopy: A Prognostic Indicator in Obstructive Sleep Apnea Treatment with Mandibular Advancement Devices" International Journal of Environmental Research and Public Health 18, no. 5: 2393. https://doi.org/10.3390/ijerph18052393