The Mediating Effect of Marital Intimacy on the Relationship between Spouse-Related Stress and Prenatal Depression in Pregnant Couples: An Actor–Partner Interdependent Model Test

Abstract
:1. Introduction
1.1. Background
1.2. Objectives
- To assess the level of spouse-related stress, marital intimacy, and prenatal depression among expectant parents.
- To assess the correlation between spouse-related stress, marital intimacy, and prenatal depression among expectant parents.
- To assess the actor–partner interdependent effects of spouse-related stress and marital intimacy on the prenatal depression in expectant parents.
- To assess the mediating effects of marital intimacy on the relationship between spouse-related stress and prenatal depression in expectant parents.
2. Methods
2.1. Study Design
2.2. Participants
2.3. Measurement
2.3.1. Spouse-Related Stress
2.3.2. Marital Intimacy
2.3.3. Prenatal Depression
2.4. Statistical Methods
3. Results
3.1. General Characteristics
3.2. Descriptive Statistics and Validity Verification of Measurement Variables
3.3. Test of Measurement Invariance
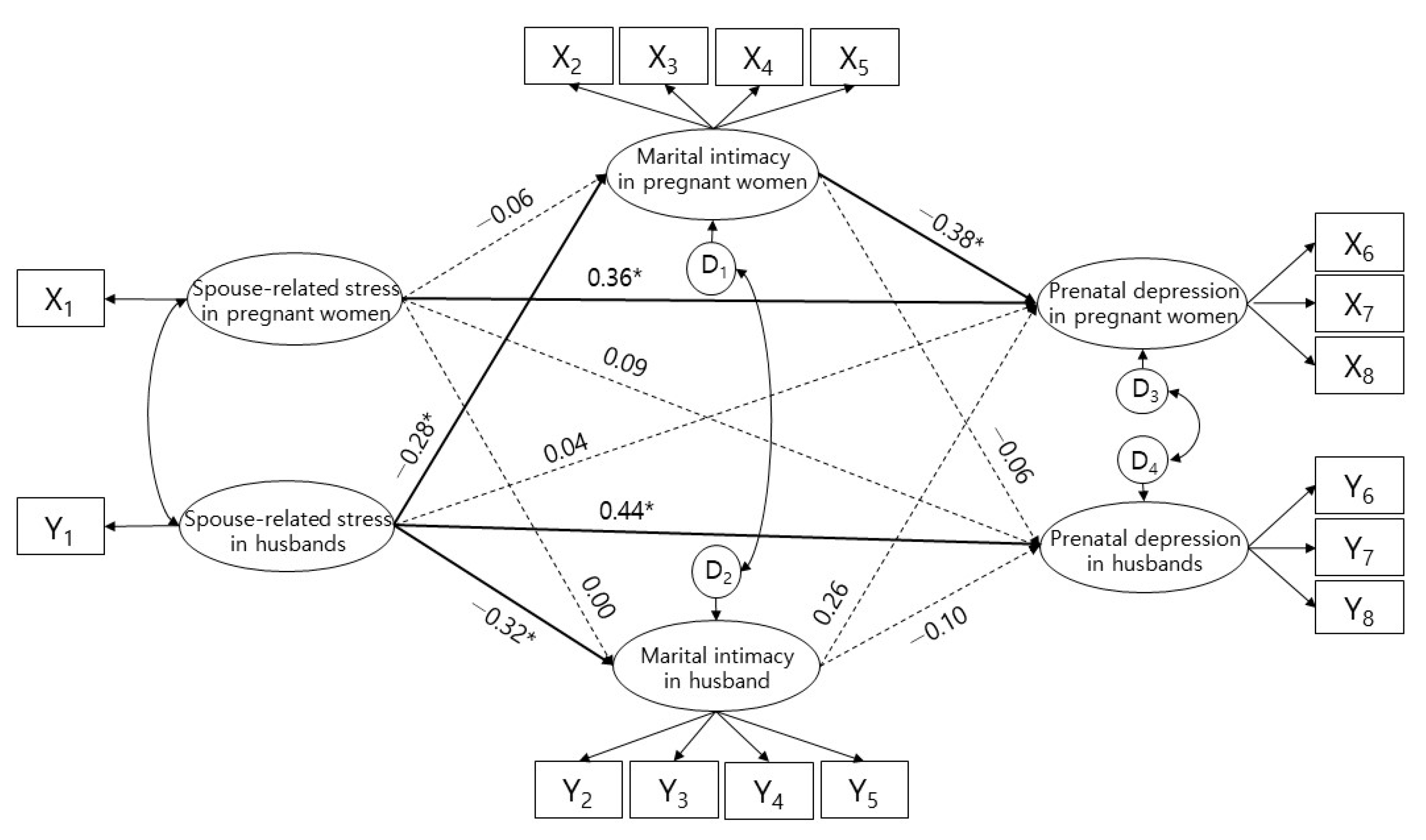
3.4. Research Model Verification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gordon, T.E.; Cardone, I.A.; Kim, J.J.; Gordon, S.M.; Silver, R.K. Universal perinatal depression screening in an Academic Medical Center. Obstet. Gynecol. 2006, 107, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Underwood, L.; Waldie, K.; D’Souza, S.; Peterson, E.R.; Morton, S. A review of longitudinal studies on antenatal and postnatal depression. Arch. Womens Ment. Health 2016, 19, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ahn, S.; Shin, J.; Jang, D. A clinical study of depressive symptoms during pregnancy. Obstet. Gynecol. Sci. 2009, 52, 1102–1108. [Google Scholar]
- Kim, Y.; Chung, C. Factors of Prenatal Depression by Stress-vulnerability and Stress-coping Models. Korean J. Women Health Nur. 2014, 20, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Darwin, Z.; Galdas, P.; Hinchliff, S.; Littlewood, E.; McMillan, D.; McGowan, L.; Gilbody, S.; BaBY team. Fathers’ views and experiences of their own mental health during pregnancy and the first postnatal year: A qualitative interview study of men participating in the UK Born and Bred in Yorkshire (BaBY) cohort. BMC Pregnancy Childbirth 2017, 17, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Divney, A.A.; Sipsma, H.; Gordon, D.; Niccolai, L.; Magriples, U.; Kershaw, T. Depression during Pregnancy among Young Couples: The Effect of Personal and Partner Experiences of Stressors and the Buffering Effects of Social Relationships. J. Pediatr. Adolesc. Gynecol. 2012, 25, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, W.W.; Zhu, X.M.; Zong, Q.Q.; Zhang, Q.; Hall, B.J.; Ungvari, G.S.; Xiang, Y. Prevalence of prenatal and postpartum depression in fathers: A comprehensive meta-analysis of observational surveys. J. Affect. Disord. 2020, 263, 491–499. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Menezes, P.R. Antenatal depression strongly predicts postnatal depression in primary health care. Rev. Bras. Psiquiatr. 2012, 34, 446–450. [Google Scholar] [CrossRef]
- Paulson, J.F.; Bazemore, S.D.; Goodman, J.H.; Leiferman, J.A. The course and interrelationship of maternal and paternal perinatal depression. Arch. Womens Ment. Health 2016, 19, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Cameron, E.E.; Sedov, I.D.; Tomfohr-Madsen, L.M. Prevalence of paternal depression in pregnancy and the postpartum: An updated meta-analysis. J. Affect. Disord. 2016, 206, 189–203. [Google Scholar] [CrossRef]
- Da Costa, D.; Zelkowitz, P.; Dasgupta, K.; Sewitch, M.; Lowensteyn, I.; Cruz, R.; Hennegen, K.; Khalifé, S. Dads Get Sad Too: Depressive Symptoms and Associated Factors in Expectant First-Time Fathers. Am. J. Mens Health 2017, 11, 1376–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulson, J.F.; Bazemore, S.D. Prenatal and postpartum depression in fathers and its association with maternal depression: A meta-analysis. JAMA 2010, 303, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Underwood, L.; Waldie, K.E.; Peterson, E.; D’Souza, S.; Verbiest, M.; McDaid, F.; Morton, S. Paternal Depression Symptoms During Pregnancy and After Childbirth Among Participants in the Growing Up in New Zealand Study. JAMA Psychiatry 2017, 74, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Underwood, L.; Waldie, K.E.; D’Souza, S.; Peterson, E.R.; Morton, S. A longitudinal study of pre-pregnancy and pregnancy risk factors associated with antenatal and postnatal symptoms of depression: Evidence from growing up in New Zealand. Matern. Child Health J. 2017, 21, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, J.; McDermott, B.; Li, W. Risk factors for paternal perinatal depression and anxiety: A systematic review and meta-analysis. Psychol. Men Masc. 2020, 21, 593–611. [Google Scholar] [CrossRef] [Green Version]
- Dadi, A.F.; Miller, E.R.; Mwanri, L. Antenatal depression and its association with adverse birth outcomes in low and middle-income countries: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0227323. [Google Scholar] [CrossRef]
- Lynn, F.A.; Alderdice, F.A.; Crealey, G.E.; McElnay, J.C. Associations between maternal characteristics and pregnancy-related stress among low-risk mothers: An observational cross-sectional study. Int. J. Nurs. Stud. 2011, 48, 620–627. [Google Scholar] [CrossRef]
- Waring, E.M.; Tillman, M.P.; Frelick, L.; Russell, L.; Weisz, G. Concepts of intimacy in the general population. J. Nerv. Ment. Dis. 1980, 168, 471–474. [Google Scholar] [CrossRef]
- Kim, H.J. Comparison of the Level of Marital Intimacy according to the Level of Stress among Middle-aged Women. J. Korean Soc. Matern. Child Health 2001, 5, 123–136. [Google Scholar]
- Patton, D.; Waring, E. The quality and quantity of marital intimacy in the marriages of psychiatric patients. J. Sex Marital Ther. 1984, 10, 201–206. [Google Scholar] [CrossRef]
- Gallagher, R.W.; Hobfoll, S.E.; Ritter, C.; Lavin, J. Marriage, intimate support and depression during pregnancy: A study of inner-city women. J. Health Psychol. 1997, 2, 457–469. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Yu, M. Influence of marital intimacy, family support, and fatigue on the stress of pregnant woman. J Korea Acad. Industr. Coop. Soc. 2014, 15, 2179–2188. [Google Scholar]
- Raymond, J.E. ‘Creating a safety net’: Women’s experiences of antenatal depression and their identification of helpful community support and services during pregnancy. Midwifery 2009, 25, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Chapman, H.A.; Hobfoll, S.E.; Ritter, C.J. Partners’ stress underestimations lead to women’s distress: A study of pregnant inner-city women. J. Pers. Soc. Psychol. 1997, 73, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Kenny, D.A. Models of non-independence in dyadic research. J. Soc. Pers. Relat. 1996, 13, 279–294. [Google Scholar] [CrossRef]
- Kang, H.C. Structural Equation Model Analysis and Application (Using SPSS/AMOS); Freeacademy: Paju, Korea, 2019. [Google Scholar]
- Ahn, H. An experimental study of the effects of husband’s supportive behavior reinforcement education on stress relief of primigravidas. J. Nurses Acad. Soc. 1985, 15, 5–16. [Google Scholar] [CrossRef]
- Lee, H.; Seo, M. Validity and Reliability Evaluation of Pregnancy Related Stress Scale. J. Korea Acad. Industr. Coop. Soc. 2017, 18, 503–512. [Google Scholar] [CrossRef]
- Jung, H.S. A study of development of the Korean-marital satisfaction scale. J. Korean Home Econ. Assoc. 2001, 39, 205–224. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Gibson, J.; McKenzie-McHarg, K.; Shakespeare, J.; Price, J.; Gray, R. A systematic review of studies validating the Edinburgh Postnatal Depression Scale in antepartum and postpartum women. Acta Psychiatr. Scand. 2009, 119, 350–364. [Google Scholar] [CrossRef]
- Rhee, Y.S.; Park, J.H.; Cha, H.J.; Kim, K.H. The Psychometric Validation of the EPDS-K Among Korean Women: Does It Only Measure Depressive Symptoms? Perspect. Psychiatr. Care 2018, 54, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.P. Concept and Understanding of the Equations Model; Han Na-rae: Seoul, Korea, 2012. [Google Scholar]
- Costa, E.C.; Castanheira, E.; Moreira, L.; Correia, P.; Ribeiro, D.; Graça Pereira, M. Predictors of emotional distress in pregnant women: The mediating role of relationship intimacy. J. Ment. Health 2020, 29, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Choi, H. Factors influencing happiness among pregnant women in the ecological systems theory. J. Korean Acad. Community Health Nurs. 2019, 30, 11–24. [Google Scholar] [CrossRef]
- Røsand, G.M.B.; Slinning, K.; Eberhard-Gran, M.; Røysamb, E.; Tambs, K. Partner relationship satisfaction and maternal emotional distress in early pregnancy. BMC Public Health 2011, 11, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Categories | N (%) | |||
|---|---|---|---|---|---|
| Pregnant Wives (120) | Husbands (120) | ||||
| Age (years) | 32.54 (3.83) | 34.73 (3.90) | |||
| Education | High school | 13 | (10.8) | 14 | (11.7) |
| College | 85 | (70.8) | 79 | (65.8) | |
| Graduate | 22 | (18.3) | 27 | (22.5) | |
| Religion | Yes | 56 | (46.7) | 49 | (40.8) |
| No | 64 | (53.3) | 71 | (59.2) | |
| Depressed | 11 | (9.2) | 8 | (6.7) | |
| Depression | Sometimes depressed | 40 | (33.3) | 27 | (22.5) |
| Not depressed | 69 | (57.5) | 85 | (70.8) | |
| Marital satisfaction | Satisfied | 111 | (92.5) | 117 | (97.5) |
| Dissatisfied | 9 | (7.5) | 3 | (2.5) | |
| Variables | Range | Pregnant Wives (n = 120) | Husbands (n = 120) | ||||
|---|---|---|---|---|---|---|---|
| M ± SD | Skewness | Kurtosis | M ± SD | Skewness | Kurtosis | ||
| Spouse-related stress | 0–5 | 1.97 ± 0.70 | 0.56 | −0.07 | 1.74 ± 0.72 | 0.95 | 0.88 |
| Marital intimacy | 0–4 | 3.07 ± 0.60 | −0.47 | −0.01 | 3.10 ± 0.54 | −0.65 | 1.25 |
| Respect | 3.02 ± 0.66 | −0.40 | −0.14 | 2.91 ± 0.65 | −0.27 | −0.08 | |
| Spending free time together | 3.27 ± 0.63 | −0.94 | 1.61 | 3.26 ± 0.60 | −0.96 | 1.70 | |
| Caring for spouse | 3.16 ± 0.72 | −0.83 | 0.27 | 3.19 ± 0.60 | −0.57 | 0.76 | |
| Expression of affection | 2.92 ± 0.74 | −0.32 | −0.38 | 2.96 ± 0.76 | −0.54 | 0.07 | |
| Depression | 0–3 | 0.80 ± 0.52 | 1.08 | 1.58 | 0.55 ± 0.40 | 0.76 | 0.08 |
| Depression | 0.55 ± 0.63 | 1.35 | 1.93 | 0.25 ± 0.42 | 1.93 | 3.46 | |
| Anxiety | 0.65 ± 0.52 | 1.19 | 1.21 | 0.56 ± 0.49 | 0.88 | 0.62 | |
| Suicidal thoughts | 1.21 ± 0.67 | 0.29 | −0.52 | 0.86 ± 0.65 | 0.40 | −0.68 | |
| Variables | Spouse-Related Stress in Pregnant Women | Marital Intimacy in Pregnant Women | Prenatal Depression in Pregnant Women | Spouse-Related Stress in Husbands | Martial Intimacy in Husbands | Prenatal Depression in Husbands |
|---|---|---|---|---|---|---|
| Spouse-related stress in pregnant women | 1 | |||||
| Marital intimacy in pregnant women | −0.08 | 1 | ||||
| Prenatal depression in pregnant women | 0.30 ** | −0.22 * | 1 | |||
| Spouse-related stress in husbands | 0.14 | −0.10 | 0.02 | 1 | ||
| Martial intimacy in husbands | 0.01 | 0.58 ** | −0.02 | −0.12 | 1 | |
| Prenatal depression in husbands | −0.02 | −0.23 * | 0.19 * | 0.20 * | −0.29 ** | 1 |
| CR | 0.82 | 0.94 | 0.91 | 0.78 | 0.94 | 0.90 |
| AVE | 0.61 | 0.89 | 0.77 | 0.50 | 0.79 | 0.74 |
| Index | Base (A) | Constrained (B) |
|---|---|---|
| 166.26 | 172.35 | |
| df | 111 (p = 0.001) | 117 (p = 0.001) |
| /df | 1.50 | 1.47 |
| SRMR | 0.07 | 0.07 |
| CFI | 0.94 | 0.94 |
| TLI | 0.92 | 0.92 |
| RMSEA | 0.07 | 0.06 |
| /p | 6.08/0.414 | |
| Endogenous Variable | Exogenous Variable | SE | CR (p) | SMC | Direct Effect | Indirect Effect | Total Effect |
|---|---|---|---|---|---|---|---|
| Martial intimacy in pregnant women | Spouse-related stress in pregnant women | 0.09 | −0.60 (0.548) | 0.082 | −0.06 (0.608) | −0.06 (0.608) | |
| Spouse-related stress in husbands | 0.13 | −2.53 (0.011) | −0.28 (0.031) | −0.28 (0.031) | |||
| Marital intimacy in husbands | Spouse-related stress in pregnant women | 0.07 | 0.03 (0.975) | 0.101 | 0.00 (0.990) | 0.00 (0.990) | |
| Spouse-related stress in husbands | 0.12 | −2.79 (0.005) | −0.32 (0.010) | −0.32 (0.010) | |||
| Prenatal depression in pregnant women | Spouse-related stress in pregnant women | 0.08 | 3.24 (0.001) | 0.238 | 0.36 (0.010) | 0.02 (0.591) | 0.29 (0.010) |
| Spouse-related stress in husbands | 0.12 | 0.32 (0.749) | 0.04 (0.858) | 0.02 (0.549) | 0.06 (0.705) | ||
| Marital intimacy in pregnant women | 0.12 | −2.71 (0.007) | −0.38 (0.030) | −0.38 (0.030) | |||
| Marital intimacy in husbands | 0.14 | 1.83 (0.067) | 0.26 (0.112) | 0.26 (0.112) | |||
| Prenatal depression in husbands | Spouse-related stress in pregnant women | 0.05 | 0.80 (0.427) | 0.263 | 0.09 (0.378) | 0.00 (0.903) | 0.04 (0.384) |
| Spouse-related stress in husbands | 0.09 | 3.06 (0.002) | 0.44 (0.020) | 0.03 (0.410) | 0.30 (0.010) | ||
| Marital intimacy in pregnant women | 0.08 | −0.41 (0.681) | −0.06 (0.679) | −0.06 (0.679) | |||
| Marital intimacy in husbands | 0.09 | −0.65 (0.517) | −0.10 (0.712) | −0.10 (0.712) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Kim, Y.-S.; Lee, M.-K. The Mediating Effect of Marital Intimacy on the Relationship between Spouse-Related Stress and Prenatal Depression in Pregnant Couples: An Actor–Partner Interdependent Model Test. Int. J. Environ. Res. Public Health 2021, 18, 487. https://doi.org/10.3390/ijerph18020487
Lee M, Kim Y-S, Lee M-K. The Mediating Effect of Marital Intimacy on the Relationship between Spouse-Related Stress and Prenatal Depression in Pregnant Couples: An Actor–Partner Interdependent Model Test. International Journal of Environmental Research and Public Health. 2021; 18(2):487. https://doi.org/10.3390/ijerph18020487
Chicago/Turabian StyleLee, Miyoung, Yeon-Suk Kim, and Mi-Kyoung Lee. 2021. "The Mediating Effect of Marital Intimacy on the Relationship between Spouse-Related Stress and Prenatal Depression in Pregnant Couples: An Actor–Partner Interdependent Model Test" International Journal of Environmental Research and Public Health 18, no. 2: 487. https://doi.org/10.3390/ijerph18020487