Invasive Coronary Angiography after Chest Pain Presentations to Emergency Departments

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Cohort
2.2. Emergency Department Discharge Pathways
2.3. Invasive Coronary Angiography
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
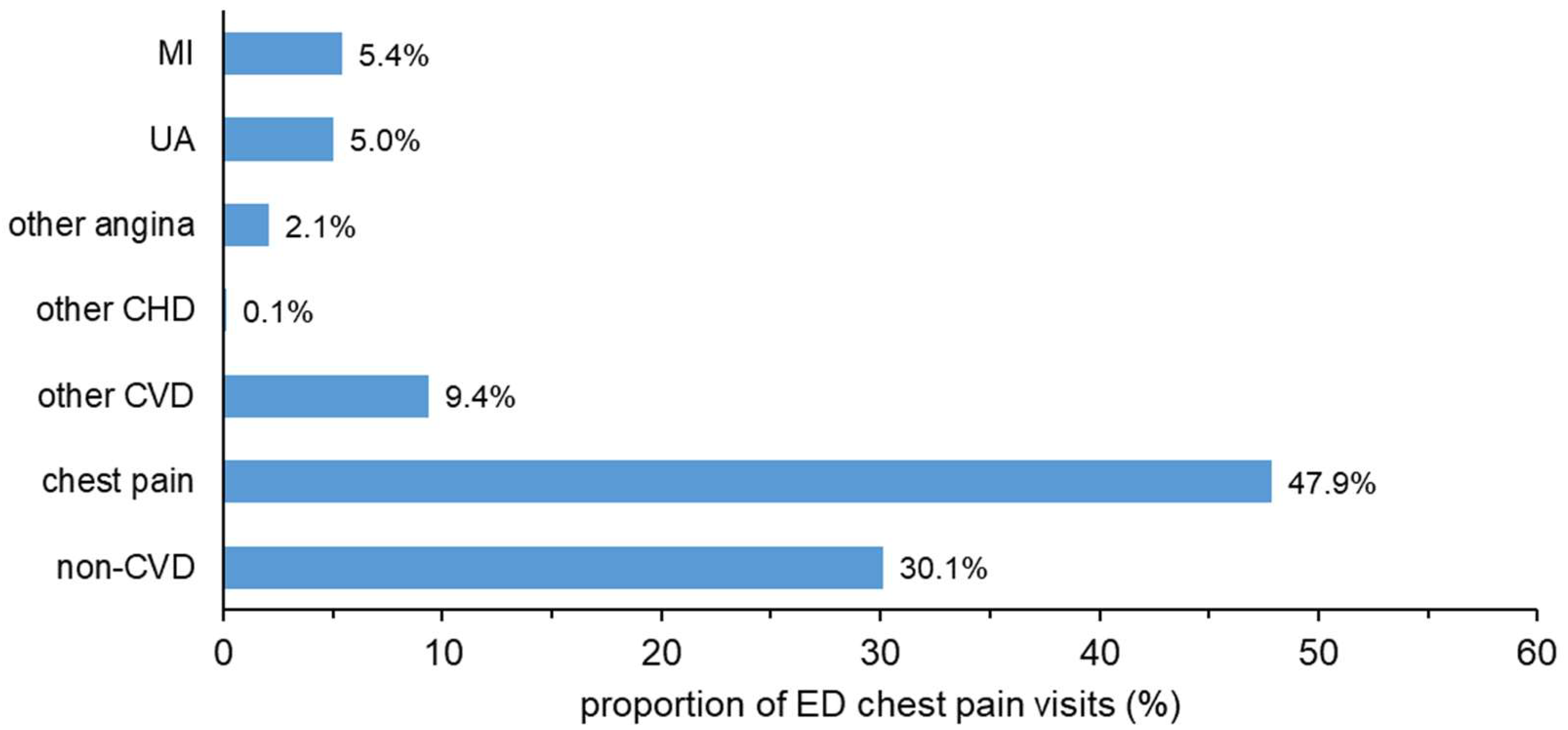
3.2. ED Discharge Diagnosis
3.3. ED Discharge Pathways
3.4. Troponin Tests and Coronary Angiography
3.5. Gender Differences and Other Determinants of Angiography
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Sharing and Accessibility
References
- National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2017 Emergency Department Summary Tables. Available online: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2017_ed_web_tables-508.pdf (accessed on 10 July 2020).
- Emergency Medicine Foundation. New Research: Diagnosing Chest Pain Quickly. Available online: https://emergencyfoundation.org.au/2017/09/04/new-research-diagnosing-chest-pain-quickly/ (accessed on 10 July 2020).
- Australian Institute of Health and Welfare. Emergency Department Care 2017–18: Australian Hospital Statistics; Cat. No: HSE 216; AIHW: Canberra, Australia, 2018.
- Chew, D.P.; Scott, I.A.; Cullen, L.; French, J.K.; Briffa, T.G.; Tideman, P.A.; Woodruffe, S.; Kerr, A.; Branagan, M.; Aylward, P.E. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Heart Lung Circ. 2016, 25, 895–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, L.; Greenslade, J.; Merollini, K.; Graves, N.; Hammett, C.J.; Hawkins, T.; Than, M.P.; Brown, A.F.; Huang, C.B.; Panahi, S.E.; et al. Cost and outcomes of assessing patients with chest pain in an Australian emergency department. Med. J. Aust. 2015, 202, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Andruchow, J.E.; Kavsak, P.A.; McRae, A.D. Contemporary emergency department management of patients with chest pain: A concise review and guide for the high-sensitivity troponin era. Can. J. Cardiol. 2018, 34, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Disease Expenditure in Australia 2015–16; Cat. No: HWE 76; AIHW: Canberra, Australia, 2019.
- Nedkoff, L.; Goldacre, R.; Greenland, M.; Goldacre, M.J.; Lopez, D.; Hall, N.; Knuiman, M.; Hobbs, M.; Sanfilippo, F.M.; Wright, F.L. Comparative trends in coronary heart disease subgroup hospitalisation rates in England and Australia. Heart 2019, 105, 1343–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holman, C.D.A.J.; Bass, J.A.; Rosman, D.L.; Smith, M.B.; Semmens, J.B.; Glasson, E.J.; Brook, E.L.; Trutwein, B.; Rouse, I.L.; Watson, C.R.; et al. A decade of data linkage in Western Australia: Strategic design, applications and benefits of the WA data linkage system. Aust. Health Rev. 2008, 32, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Australian Consortium for Classification Development. International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification, 9th ed.; Independent Hospital Pricing Authority: Darlinghurst, Australia, 2015.
- Brenna, C.T.A.; Afgani, F.J.; Hanneman, K.; Levitan, D.; Udell, J.A.; Sacha Bhatia, R.; Harvey, P.J.; Nguyen, E.T. Chest pain investigation in patients at low or intermediate risk: What is the best first-line test to rule out coronary artery disease? Can. Fam. Phys. 2020, 66, 24–30. [Google Scholar]
- Fordyce, C.B.; Newby, D.E.; Douglas, P.S. Diagnostic strategies for the evaluation of chest pain: Clinical implications from SCOT-HEART and PROMISE. J. Am. Coll. Cardiol. 2016, 67, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. The Australian Statistical Geography Standard (ASGS) Remoteness Structure. Available online: https://www.abs.gov.au/websitedbs/D3310114.nsf/home/remoteness+structure (accessed on 10 July 2020).
- Bhuiya, F.A.; Pitts, S.R.; McCaig, L.F. Emergency Department Visits for Chest Pain and Abdominal Pain: United States, 1999–2008; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2010; pp. 1–8. [Google Scholar]
- Greenslade, J.H.; Carlton, E.W.; Van Hise, C.; Cho, E.; Hawkins, T.; Parsonage, W.A.; Tate, J.; Ungerer, J.; Cullen, L. Diagnostic accuracy of a new high-sensitivity troponin I assay and five accelerated diagnostic pathways for ruling out acute myocardial infarction and acute coronary syndrome. Ann. Emerg. Med. 2018, 71, 439–451.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, G.A.; Kaul, S. How would the reverend Bayes interpret high-sensitivity troponin? Circulation 2010, 121, 1172–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, D.P.; MacIsaac, A.I.; Lefkovits, J.; Harper, R.W.; Slawomirski, L.; Braddock, D.; Horsfall, M.J.; Buchan, H.A.; Ellis, C.J.; Brieger, D.B.; et al. Variation in coronary angiography rates in Australia: Correlations with socio-demographic, health service and disease burden indices. Med. J. Aust. 2016, 205, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.; Bengs, S.; Luu, J.; Osto, E.; Siller-Matula, J.M.; Muka, T.; Gebhard, C. Sex and gender in cardiovascular medicine: Presentation and outcomes of acute coronary syndrome. Eur. Heart J. 2020, 41, 1328–1336. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Count, n (% of Total Patients) | Patients with >1 ED Visit, n (%) |
|---|---|---|
| Number of ED visits | 20,131 | 5115 |
| Number of patients | 16,974 | 1958 (11.5) |
| Sex † Males | 8609 (50.7) | 1013 (51.7) |
| Females | 8364 (49.3) | 945 (48.3) |
| Age, mean (SD) years | 55.6 (19.1) | 59.6 (19.0) |
| Age range (years) | 20–103 | 20–101 |
| Age group (years) | ||
| 20–44 | 5273 (31.1) | 446 (22.8) |
| 45–64 | 5815 (34.3) | 669 (34.2) |
| 65–74 | 2565 (15.1) | 343 (17.5) |
| ≥75 | 3321 (19.6) | 500 (25.5) |
| Indigenous Australians | 809 (4.8) | 162 (8.3) |
| Triage code (of first ED presentation in study period) | ||
| 1. Resuscitation | 129 (0.8) | 10 (0.5) |
| 2. Emergency | 15,780 (93.0) | 1882 (96.1) |
| 3. Urgent | 861 (5.1) | 58 (3.0) |
| 4. Semi-urgent | 189 (1.1) | 7 (0.4) |
| 5. Non-urgent | 15 (0.1) | 1 (0.05) |
| Remoteness area ‡ | ||
| Major cities | 15,767 (92.9) | 1860 (95.0) |
| Inner regional | 173 (1.0) | 14 (0.7) |
| Outer regional | 210 (1.2) | 18 (0.9) |
| Remote | 91 (0.5) | 9 (0.5) |
| Very remote | 69 (0.4) | 6 (0.3) |
| Missing | 664 (3.9) | 51 (2.6) |
| Medical history (10 year lookback) | ||
| Coronary heart disease | 2447 (14.4) | 491 (25.1) |
| Diabetes | 2388 (14.1) | 469 (24.0) |
| Hypertension | 3646 (21.5) | 735 (37.5) |
| Atrial fibrillation | 1619 (9.5) | 332 (17.0) |
| PCI or CABG | 1393 (8.2) | 309 (15.8) |
| Mean time (SD) from most recent PCI/CABG in past 10 years to ED presentation | 1267 (1051) days 3.5 (2.9) years | 1184 (1055) days 3.2 (2.9) years |
| Died within 30 days of ED discharge (in or out of hospital) | 149 (0.9) ¶ | 9 (0.5) |
| Died within 90 days of ED discharge (in or out of hospital) | 311 (1.8) ¶ | 40 (2.0) |
| Covariate | Number of Initial Angiograms (row %) after the First ED Presentation † | p Value | Total (col %) | ||
|---|---|---|---|---|---|
| 0–7 days | 8–30 days | 31–90 days | |||
| Total | 1300 (84.1) | 118 (7.6) | 128 (8.3) | 1546 | |
| Troponin I test result | <0.0001 ‡ | ||||
| No tests | 39 (66.1) | 7 (11.9) | 13 (22.0) | 59 (3.8) | |
| All normal | 392 (69.4) | 81 (14.3) | 92 (16.3) | 565 (36.6) | |
| Elevated § | 869 (94.2) | 30 (3.2) | 23 (2.5) | 922 (59.6) | |
| Sex | 0.28 ‡ | ||||
| Males | 879 (84.2) | 85 (8.1) | 80 (7.7) | 1044 (67.5) | |
| Females | 421 (83.9) | 33 (6.6) | 48 (9.6) | 502 (32.5) | |
| Age group (years) | 0.09 ‡ | ||||
| 20–44 | 92 (86.0) | 8 (7.5) | 7 (6.5) | 107 (6.9) | |
| 45–64 | 576 (84.0) | 59 (8.6) | 51 (7.4) | 686 (44.4) | |
| 65–74 | 342 (83.6) | 21 (5.1) | 46 (11.3) | 409 (26.5) | |
| ≥75 | 290 (84.3) | 30 (8.7) | 24 (7.0) | 344 (22.2) | |
| Remoteness area ¶ | 0.45 £ | ||||
| Major cities | 1165 (84.0) | 106 (7.7) | 115 (8.3) | 1386 (89.6) | |
| Regional | 51 (76.1) | 7 (10.5) | 9 (13.4) | 67 (4.3) | |
| Remote, very remote | 32 (91.4) | 2 (5.7) | 1 (2.9) | 35 (2.3) | |
| Missing | 52 (89.6) | 3 (5.2) | 3 (5.2) | 58 (3.8) | |
| ED discharge diagnosis | <0.0001 ‡ | ||||
| MI | 655 (97.3) | 13 (1.9) | 5 (0.7) | 673 (43.5) | |
| Unstable angina | 224 (85.8) | 21 (8.0) | 16 (6.1) | 261 (16.9) | |
| Other angina | 39 (65.0) | 11 (18.3) | 10 (16.7) | 60 (3.9) | |
| Other CHD | 7 (87.5) | 1 (12.5) | 0 | 8 (0.5) | |
| Other CVD | 76 (76.8) | 10 (10.1) | 13 (13.1) | 99 (6.4) | |
| Chest pain | 237 (67.9) | 46 (13.2) | 66 (18.9) | 349 (22.6) | |
| Non-CVD | 62 (64.6) | 16 (16.7) | 18 (18.8) | 96 (6.2) | |
| Variable | Adjusted Odds Ratio (95% CI) | p Value ‡ |
|---|---|---|
| Age | 0.99 (0.99, 1.00) | 0.0006 |
| Male sex (reference level: females) | 1.89 (1.65, 2.18) | <0.0001 |
| Remoteness area (reference level: major cities) | <0.0001 | |
| Regional (inner/outer) | 2.11 (1.49, 2.99) | |
| Remote, very remote | 2.53 (1.54, 4.16) | |
| Missing | 1.18 (0.83, 1.68) | |
| ED discharge diagnosis (reference level: non-CVD) | <0.0001 | |
| Myocardial infarction | 32.75 (24.95, 42.97) | |
| Unstable angina | 18.47 (14.16, 24.11) | |
| Other angina | 8.93 (6.21, 12.84) | |
| Other CHD | 14.48 (5.36, 39.13) | |
| Other CVD | 2.35 (1.75, 3.17) | |
| Chest pain | 2.02 (1.60, 2.55) | |
| Troponin level (reference: troponin test not done) | <0.0001 | |
| All tests normal | 3.34 (2.52, 4.44) | |
| Elevated † | 14.37 (10.55, 19.58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanfilippo, F.M.; Hillis, G.S.; Rankin, J.M.; Latchem, D.; Schultz, C.J.; Yong, J.; Li, I.W.; Briffa, T.G. Invasive Coronary Angiography after Chest Pain Presentations to Emergency Departments. Int. J. Environ. Res. Public Health 2020, 17, 9502. https://doi.org/10.3390/ijerph17249502
Sanfilippo FM, Hillis GS, Rankin JM, Latchem D, Schultz CJ, Yong J, Li IW, Briffa TG. Invasive Coronary Angiography after Chest Pain Presentations to Emergency Departments. International Journal of Environmental Research and Public Health. 2020; 17(24):9502. https://doi.org/10.3390/ijerph17249502
Chicago/Turabian StyleSanfilippo, Frank M., Graham S. Hillis, Jamie M. Rankin, Donald Latchem, Carl J. Schultz, Jongsay Yong, Ian W. Li, and Tom G. Briffa. 2020. "Invasive Coronary Angiography after Chest Pain Presentations to Emergency Departments" International Journal of Environmental Research and Public Health 17, no. 24: 9502. https://doi.org/10.3390/ijerph17249502