Understanding the Self-Perceived Barriers and Enablers toward Adopting a Mediterranean Diet in Australia: An Application of the Theory of Planned Behaviour Framework


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Approval
3. Results
3.1. Participant Characteristics
3.2. Advantages and Disadvantages of the Mediterranean Diet
3.2.1. Advantages
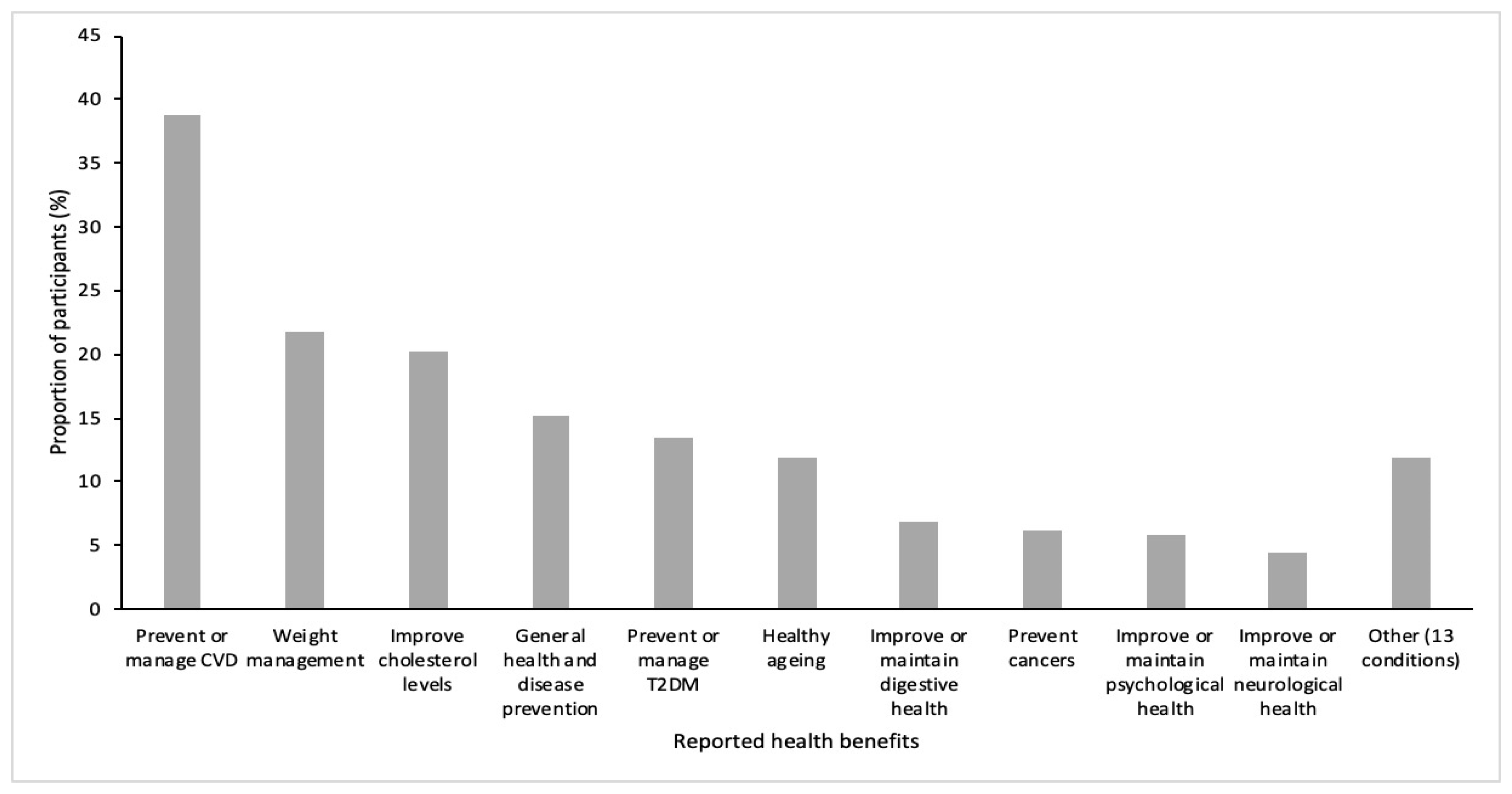
Health Benefits
Diet Quality
Appeal and Lifestyle
Affordability
Environment
3.2.2. Disadvantages
Ability to Adhere
Food Literacy
“Healthfulness”
Convenience
Taste
Culture
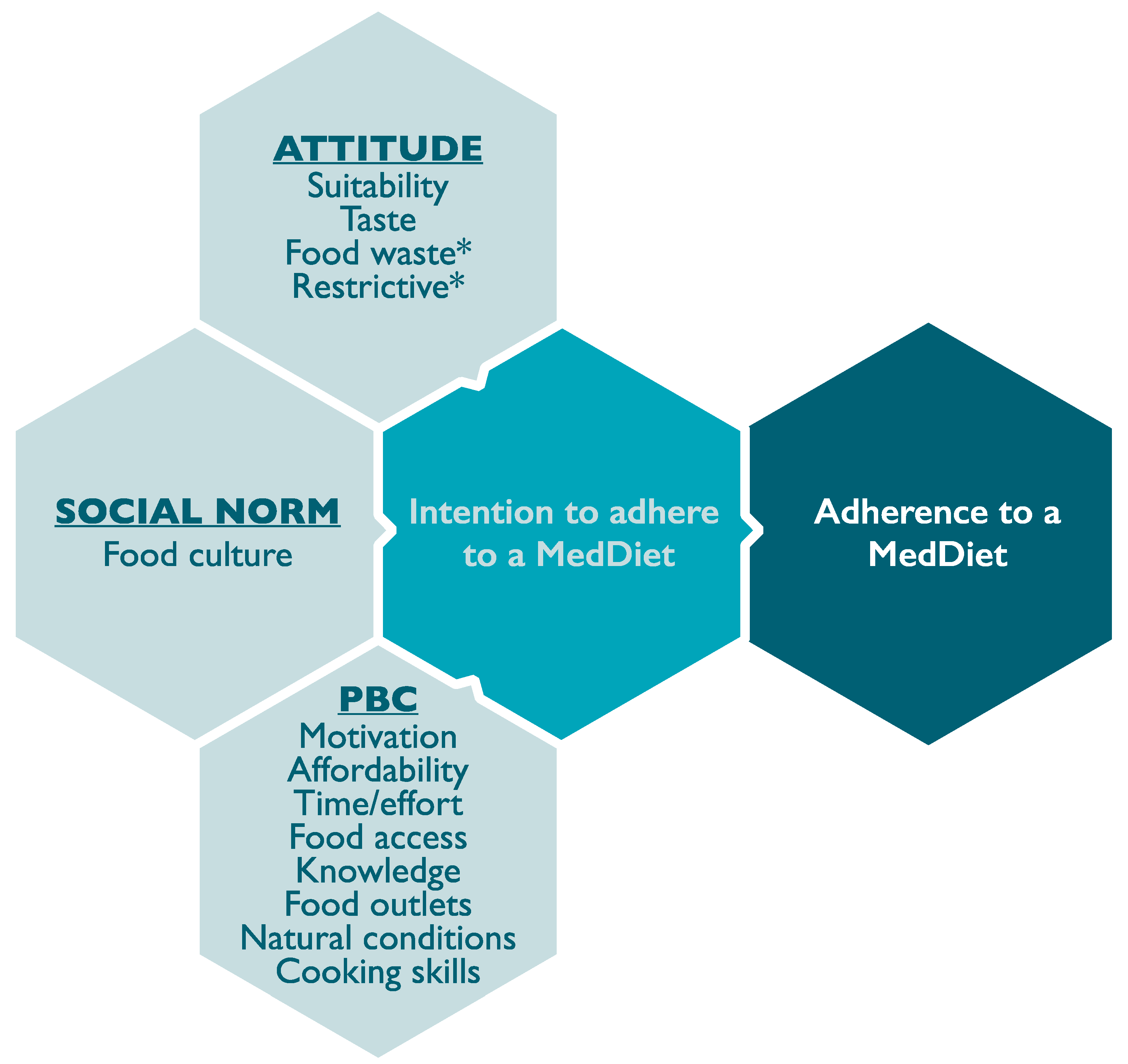
3.3. Barriers and Enablers to Following a Mediterranean Diet
3.3.1. Construct 1: Attitudes
3.3.2. Construct 2: Social Norms
3.3.3. Construct 3: Perceived Behavioural Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haapasalo, V.; de Vries, H.; Vandelanotte, C.; Rosenkranz, R.R.; Duncan, M.J. Cross-sectional associations between multiple lifestyle behaviours and excellent well-being in Australian adults. Prev. Med. 2018, 116, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Krokstad, S.; Ding, D.; Grunseit, A.C.; Sund, E.R.; Holmen, T.L.; Rangul, V.; Bauman, A. Multiple lifestyle behaviours and mortality, findings from a large population-based Norwegian cohort study—The hunt study. BMC Public Health 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosland, P.; Ananthapavan, J.; Davison, J.; Lambert, M.; Carter, R. The health burden of preventable disease in Australia: A systematic review. Aust. N. Z. J. Public Health 2019, 43, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Martin, J. Australia’s progress in improving diets and preventing obesity: Clear opportunities for action. Curr. Obes. Rep. 2018, 7, 220–226. [Google Scholar] [CrossRef]
- Melaku, Y.A.; Renzaho, A.; Gill, T.K.; Taylor, A.W.; Dal Grande, E.; de Courten, B.; Baye, E.; Gonzalez-Chica, D.; Hyppönen, E.; Shi, Z.; et al. Burden and trend of diet-related non-communicable diseases in Australia and comparison with 34 OECD countries, 1990–2015: Findings from the Global Burden of Disease Study 2015. Eur. J. Nutr. 2019, 58, 1299–1313. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- García-Fernández, E.; Rico-Cabanas, L.; Rosgaard, N.; Estruch, R.; Bach-Faig, A. Mediterranean diet and cardiodiabesity: A review. Nutrients 2014, 6, 3474–3500. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [Green Version]
- Franquesa, M.; Pujol-Busquets, G.; Garcia-Fernandez, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martinez, A.; Medina, F.X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean diet and cardiodiabesity: A systematic review through evidence-based answers to key clinical questions. Nutrients 2019, 11, 655. [Google Scholar] [CrossRef] [Green Version]
- Itsiopoulos, C.; Brazionis, L.; Kaimakamis, M.; Cameron, M.; Best, J.D.; O’Dea, K.; Rowley, K. Can the Mediterranean diet lower Hba1c in type 2 diabetes? Results from a randomized cross-over study. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Jannasch, F.; Kroger, J.; Schulze, M.B. Dietary patterns and type 2 diabetes: A systematic literature review and meta-analysis of prospective studies. J. Nutr. 2017, 147, 1174–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic Longitudinal Investigation of Ageing and Diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ntanasi, E.; Yannakoulia, M.; Kosmidis, M.H.; Anastasiou, C.A.; Dardiotis, E.; Hadjigeorgiou, G.; Sakka, P.; Scarmeas, N. Adherence to Mediterranean diet and frailty. J. Am. Med. Dir. Assoc. 2018, 19, 315–322. [Google Scholar] [CrossRef]
- Villani, A.; Sultana, J.; Doecke, J.; Mantzioris, E. Differences in the interpretation of a modernized Mediterranean diet prescribed in intervention studies for the management of type 2 diabetes: How closely does this align with a traditional Mediterranean diet? Eur. J. Nutr. 2018, 58, 1369–1380. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.A.; Hershey, M.S.; Zazpe, I.; Trichopoulou, A. Transferability of the Mediterranean Diet to non-Mediterranean countries. What is and what is not the Mediterranean Diet. Nutrients 2017, 9, 1226. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Donini, L.M.; Serra-Majem, L.; Bulló, M.; Gil, A.; Salas-Salvadó, J. The Mediterranean Diet: Culture, health and science. Br. J. Nutr. 2015, 113, S1–S3. [Google Scholar] [CrossRef] [Green Version]
- George, E.S.; Kucianski, T.; Mayr, H.L.; Moschonis, G.; Tierney, A.C.; Itsiopoulos, C. A Mediterranean Diet model in Australia: Strategies for translating the Traditional Mediterranean Diet into a multicultural setting. Nutrients 2018, 10, 465. [Google Scholar] [CrossRef] [Green Version]
- Noah, A.; Truswell, A.S. There are many Mediterranean Diets. Asia Pac. J. Clin. Nutr. 2001, 10, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A. Diversity v. globalization: Traditional foods at the epicentre. Public Health Nutr. 2012, 15, 951–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barley, E.; Lawson, V. Using health psychology to help patients: Theories of behaviour change. Br. J. Nurs. 2016, 25, 924–927. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.S.; Oliver, M.; Simnadis, T.; Beck, E.J.; Coltman, T.; Iverson, D.; Caputi, P.; Sharma, R. The Theory of Planned Behaviour and dietary patterns: A systematic review and meta-analysis. Prev. Med. 2015, 81, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Johnston, M. Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychol. Rev. 2012, 6, 1–6. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Close, M.A.; Lytle, L.A.; Chen, D.G.; Viera, A.J. Using the Theory of Planned Behavior to explain intention to eat a healthful diet among Southeastern United States office workers. Nutr. Food Sci. 2018, 48, 365–374. [Google Scholar] [CrossRef]
- Rahmati-Najarkolaei, F.; Pakpour, A.H.; Saffari, M.; Hosseini, M.S.; Hajizadeh, F.; Chen, H.; Yekaninejad, M.S. Determinants of lifestyle behavior in Iranian adults with prediabetes: Applying the Theory of Planned Behavior. Arch. Iran. Med. 2017, 20, 198–204. [Google Scholar]
- Wright, H.H.; Kickbusch, H.; Swanepoel, E.; Gray, N. Factors influencing low sodium intake in people with non-dialysis dependent chronic kidney disease. J. Ren. Care 2019, 46, 95–105. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean Diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [Green Version]
- Mantzioris, E.; Villani, A. Translation of a Mediterranean-style diet into the Australian Dietary Guidelines: A nutritional, ecological and environmental perspective. Nutrients 2019, 11, 2507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aridi, Y.S.; Walker, J.L.; Roura, E.; Wright, O.R.L. Adherence to the Mediterranean Diet and chronic disease in Australia: National Nutrition and Physical Activity Survey Analysis. Nutrients 2020, 12, 1251. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Wilson, C.; Murphy, C.J. Older Australians can adhere to a Traditional Mediterranean style diet over two weeks: A pilot dietary intervention study. BMC Nutr. 2015, 1, 28. [Google Scholar] [CrossRef] [Green Version]
- Zacharia, K.; Patterson, A.J.; English, C.; MacDonald-Wicks, L. Feasibility of the Ausmed Diet program: Translating the Mediterranean Diet for older Australians. Nutrients 2020, 12, 1044. [Google Scholar] [CrossRef] [Green Version]
- Middleton, G.; Keegan, R.; Smith, M.F.; Alkhatib, A.; Klonizakis, M. Implementing a Mediterranean diet intervention into a rct: Lessons learned from a non-Mediterranean based country. J. Nutr. Health Aging 2015, 19, 1019–1022. [Google Scholar] [CrossRef] [Green Version]
- Bottcher, M.R.; Marincic, P.Z.; Nahay, K.L.; Baerlocher, B.E.; Willis, A.W.; Park, J.; Gaillard, P.; Greene, M.W. Nutrition knowledge and Mediterranean diet adherence in the Southeast United States: Validation of a field-based survey instrument. Appetite 2017, 111, 166–176. [Google Scholar] [CrossRef]
- Haigh, L.; Bremner, S.; Houghton, D.; Henderson, E.; Avery, L.; Hardy, T.; Hallsworth, K.; McPherson, S.; Anstee, Q.M. Barriers and facilitators to Mediterranean diet adoption by patients with nonalcoholic fatty liver disease in Northern Europe. J. Clin. Gastroenterol. Hepatol. 2019, 17, 1364–1371. [Google Scholar] [CrossRef] [Green Version]
- Francis, J.; Eccles, M.P.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers; Centre for Health Services Research: Newcastle upon Tyne, UK, 2004. [Google Scholar]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Aros, F.; Gomez-Gracia, E. A 14-Item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The Predimed Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Ely, M. On Writing Qualitative Research: Living by Words, 1st ed.; Falmer Press: London, UK, 1997; pp. 207–220. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Fade, S.A.; Swift, J.A. Qualitative research in Nutrition and Dietetics: Data analysis issues. J. Hum. Nutr. Diet. 2011, 24, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Bryman, A. Qualitative research. In Social Research Methods, 5th ed.; Oxford University Press: Oxford, UK, 2016; pp. 373–618. [Google Scholar]
- Kretowicz, H.; Hundley, V.; Tsofliou, F. Exploring the perceived barriers to following a Mediterranean style diet in childbearing age: A qualitative study. Nutrients 2018, 10, 1694. [Google Scholar] [CrossRef] [Green Version]
- Lara, J.; McCrum, L.A.; Mathers, J.C. Association of Mediterranean diet and other health behaviours with barriers to healthy eating and perceived health among British adults of retirement age. Maturitas 2014, 79, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.E.; McEvoy, C.T.; Prior, L.; Lawton, J.; Patterson, C.C.; Kee, F.; Cupples, M.; Young, I.S.; Appleton, K.; McKinley, M.C.; et al. Barriers to adopting a Mediterranean diet in Northern European adults at high risk of developing cardiovascular disease. J. Hum. Nutr. Diet. 2018, 31, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonhäuser, I.U.; Dorandt, S.; Willmund, E.; Honsel, J. The benefit of the Mediterranean Diet--considerations to modify German food patterns. Eur. J. Nutr. 2004, 43, 31–38. [Google Scholar] [CrossRef]
- Martínez-González, M.A. Benefits of the Mediterranean Diet beyond the Mediterranean Sea and beyond food patterns. BMC Med. 2016, 14, 157. [Google Scholar] [CrossRef] [Green Version]
- Kouris-Blazos, A.; Gnardellis, C.; Wahlqvist, M.L.; Trichopoulos, D.; Lukito, W.; Trichopoulou, A. Are the advantages of the Mediterranean Diet transferable to other populations? A cohort study in Melbourne, Australia. Br. J. Nutr. 1999, 82, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Tong, T.; Nicholas, Y.N.; Wareham, J.; Khaw, K.T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean Diet with Cardiovascular Disease incidence and mortality and its population impact in a Non-Mediterranean population: The Epic-Norfolk Study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Macdiarmid, J.; Loe, J.; Kyle, J.; McNeill, G. “It was an education in portion size”. Experience of eating a healthy diet and barriers to long term dietary change. Appetite 2013, 71, 411–419. [Google Scholar] [CrossRef]
- Pridgeon, A.; Whitehead, K. A qualitative study to investigate the drivers and barriers to healthy eating in two public sector workplaces. J. Hum. Nutr. Diet. 2013, 26, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Knight, C.J.; Jackson, O.; Rahman, I.; Burnett, D.O.; Frugé, A.D.; Greene, M.W. The Mediterranean Diet in the stroke belt: A cross-sectional study on adherence and perceived knowledge, barriers, and benefits. Nutrients 2019, 11, 1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government, Australia. Age Pension: Payment Rates; Commonwealth of Australia: Canberra, Australia, 2018. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.; Diclemente, C. Trans-Theoretical Therapy—Toward a more integrative model of change. Psychother. Theory Res. Pract. 1982, 19, 276–288. [Google Scholar] [CrossRef]
- Råberg Kjøllesdal, M.K.; Hjellset, V.T.; Bjørge, B.; Holmboe-Ottesen, G.; Wandel, M. Barriers to healthy eating among Norwegian-Pakistani women participating in a culturally adapted intervention. Scand. J. Public Health 2010, 38, 52–59. [Google Scholar] [CrossRef]
- Papadaki, A.; Thanasoulias, A.; Pound, R.; Sebire, S.J.; Jago, R. Employees’ expectations of internet-based, workplace interventions promoting the Mediterranean diet: A qualitative study. J. Nutr. Educ. Behav. 2016, 48, 706–715. [Google Scholar] [CrossRef] [Green Version]
- Middleton, G.; Keegan, R.; Smith, M.F.; Alkhatib, A.; Klonizakis, M. Exploring barriers and facilitators to eating the Mediterranean diet in England: A qualitative study. Proc. Nutr. Soc. 2015, 74, E143. [Google Scholar] [CrossRef] [Green Version]
- Greiner, B.H.; Croff, J.; Wheeler, D.; Miller, B. Mediterranean diet adherence in cardiac patients: A cross-sectional study. Am. J. Health Behav. 2018, 42, 3–10. [Google Scholar] [CrossRef]
- Leblanc, V.; Bégin, C.; Hudon, A.M.; Royer, M.M.; Corneau, L.; Dodin, S.; Lemieux, S. Effects of a nutritional intervention program based on the Self-Determination Theory and promoting the Mediterranean diet. Health Psychol. Open 2016, 3, 2055102915622094. [Google Scholar] [CrossRef] [Green Version]
- Bonaccio, M.; Bonanni, A.E.; Di Castelnuovo, A.; De Lucia, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Low income is associated with poor adherence to a Mediterranean diet and a higher prevalence of obesity: Cross-sectional results from the Moli-Sani Study. BMJ Open 2012, 2, e001685. [Google Scholar] [CrossRef] [Green Version]
- Mayr, H.L.; Kostjasyn, S.P.; Campbell, K.L.; Palmer, M.; Hickman, I.J. Investigating whether the Mediterranean dietary pattern is integrated in routine Dietetic practice for management of chronic conditions: A national survey of Dietitians. Nutrients 2020, 12, 3395. [Google Scholar] [CrossRef] [PubMed]
- Gibson, I.; Flaherty, G.; Cormican, S.; Jones, J.; Kerins, C.; Walsh, A.M.; Costello, C.; Windle, J.; Connolly, S.; Crowley, J. Translating guidelines to practice: Findings from a multidisciplinary preventive Cardiology programme in the West of Ireland. Eur. J. Prev. Cardiol. 2014, 21, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.N.; Imamura, F.; Monsivais, P.; Brage, S.; Griffin, S.J.; Wareham, N.J.; Forouhi, N.G. Dietary cost associated with adherence to the Mediterranean diet, and its variation by socio-economic factors in the UK Fenland Study. Br. J. Nutr. 2018, 119, 685–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, R.E.; Hausenblas, H.A. Exercise and diet determinants of overweight women participating in an exercise and diet program: A prospective examination of the Theory of Planned Behavior. Women Health 2006, 42, 37–62. [Google Scholar] [CrossRef] [PubMed]
- Malek, L.; Umberger, W.J.; Makrides, M.; Shaojia, Z. Predicting healthy eating intention and adherence to dietary recommendations during pregnancy in Australia using the Theory of Planned Behaviour. Appetite 2017, 116, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11, S579–S585. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘Smiles’ Trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.M.; Davis, C.R.; Murphy, K.J. The Mediterranean diet and cognitive function among healthy older adults in a 6-Month randomised controlled trial: The Medley Study. Nutrients 2016, 8, 579. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-Style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (Helfimed). Nutr. Neurosci. 2017, 22, 474–487. [Google Scholar] [CrossRef] [Green Version]
- Nestle, M.; Wing, R.; Birch, L.; DiSogra, L.; Drewnowski, A.; Middleton, S.; Sigman-Grant, M.; Sobal, J.; Winston, M.; Economos, C. Behavioral and social influences on food choice. Nutr. Rev. 1998, 56, 50–64. [Google Scholar] [CrossRef] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves markers of cardiovascular risk: Results from the Meddairy randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 1166–1682. [Google Scholar] [CrossRef] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Murphy, K.J. Effects of Mediterranean diet supplemented with lean pork on blood pressure and markers of cardiovascular risk: Findings from the Medpork trial. Br. J. Nutr. 2019, 122, 873–883. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean diet with fresh, lean pork improves processing speed and mood: Cognitive findings from the Medpork randomised controlled trial. Nutrients 2019, 11, 1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves mood and processing speed in an Australian sample: Results from the Meddairy randomized controlled trial. Nutr. Neurosci. 2020, 23, 646–658. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; Bagordo, F.; Panico, A.; Giorgi, M.D.; Idolo, A.; Serio, F.; Tumolo, M.R.; Donno, A.D. Adherence to Mediterranean Diet of children living in small southern Italian villages. Int. J. Food Sci. Nutr. 2020, 71, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Marventano, S.; Buscemi, S.; Scuderi, A.; Matalone, M.; Platania, A.; Giorgianni, G.; Rametta, S.; Nolfo, F.; Galvano, F. Factors associated with adherence to the Mediterranean Diet among adolescents living in Sicily, Southern Italy. Nutrients 2013, 5, 4908–4923. [Google Scholar] [CrossRef] [Green Version]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccles, M. From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Woodman, R.; Murphy, K.J. A Mediterranean diet reduces F2-Isoprostanes and triglycerides among older Australian men and women after 6 months. J. Nutr. 2017, 147, 1348–1355. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the Medley randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| No. | Question |
|---|---|
| 1 | What do you believe are the advantages of following a Mediterranean-style diet? |
| 2 | What do you believe are the disadvantages of following a Mediterranean-style diet? |
| 3 | What factors or circumstances would enable (make it easier) for you to follow a Mediterranean-style diet? |
| 4 | What factors or circumstances would make it difficult (harder) for you to follow a Mediterranean-style diet? |
| 5 | Is there anything else you associate with your own views about following a Mediterranean-style diet? |
| Variable | |
|---|---|
| Gender, n (%) | |
| Males | 80 (13.2) |
| Females | 526 (86.8) |
| Age Category (years), n (%) | |
| 18–24 | 57 (9.4) |
| 25–34 | 149 (24.6) |
| 35–44 | 163 (26.9) |
| 45–54 | 93 (15.3) |
| 55–64 | 84 (13.9) |
| 65–74 | 46 (7.6) |
| Greater than 75 | 13 (2.1) |
| Not reported | 1 (0.2) |
| BMI (kg/m2) * | 26.1 ± 5.9 |
| Country of birth, n (%) | |
| Australia | 479 (79.0) |
| United Kingdom | 31 (5.1) |
| New Zealand | 19 (3.1) |
| South Africa | 9 (1.5) |
| Germany | 6 (1.0) |
| Combined 38 other countries | 62 (10.3) |
| Highest level of education, n (%) | |
| No schooling | 1 (0.2) |
| Secondary schooling | 53 (8.7) |
| Trade/technical/vocational training | 39 (6.4) |
| Diploma/Advanced diploma | 69 (11.4) |
| Bachelor’s degree | 243 (40.1) |
| Postgraduate degree or doctorate | 201 (33.2) |
| Household Income AUD/year, n (%) | |
| 0–24,999 | 30 (5.0) |
| 25,000–74,999 | 135 (22.3) |
| 75,000–124,999 | 178 (29.4) |
| 125,000–199,999 | 151 (24.9) |
| 200,000 or greater | 60 (9.9) |
| Prefer not to disclose | 52 (8.6) |
| Number of persons over 18 years in the household | 2.2 ± 0.9 |
| Reported medical conditions, n (%) | |
| No medical conditions, otherwise healthy | 246 (40.6) |
| Depression | 72 (11.9) |
| Arthritis | 58 (9.6) |
| High cholesterol | 47 (7.8) |
| High blood pressure | 42 (6.9) |
| Type 2 diabetes mellitus | 20 (3.3) |
| Heart disease | 13 (2.1) |
| Osteoporosis | 12 (2.0) |
| Neurological disease | 6 (1.0) |
| Type 1 diabetes mellitus | 6 (1.0) |
| Other | 134 (22.1) |
| Not reported | 83 (13.7) |
| Nutrition or health related qualification, n (%) | |
| Nutrition related qualification | 71 (11.7) |
| Other health related qualification | 83 (13.7) |
| Currently studying for nutrition related qualification | 50 (8.3) |
| Currently studying for other health related qualification | 16 (2.6) |
| None | 372 (61.4) |
| Unreported | 21 (3.5) |
| n (% of Total Participants) | Theme | n (% of Responses) | Representative Quote * | ||
|---|---|---|---|---|---|
| Advantages | 582 (96.0) | Health benefits | 445 | (76.5) |
|
| Diet quality | 224 | (38.5) |
| ||
| Appeal | 110 | (18.9) |
| ||
| Lifestyle | 46 | (7.9) |
| ||
| Affordability | 15 | 2.6 |
| ||
| Environment | 13 | 2.2 |
| ||
| Disadvantages | 370 (61.1) | Abilityto adhere | 147 | 39.7 |
|
| Food literacy | 114 | 30.8 |
| ||
| Healthfulness | 109 | 29.5 |
| ||
| Convenience | 107 | 28.9 |
| ||
| Taste | 21 | 5.7 |
| ||
| Culture | 18 | 4.9 |
| ||
| Barrier n = 474 (78.2%) | Enabler n = 507 (83.5%) | Representative Quote * | |||
|---|---|---|---|---|---|
| TBP Construct | Theme | n (%) | n (%) | Barrier | Enabler |
| Attitude | Suitability | 48 (10.1) | 14 (2.8) |
|
|
| Taste | 18 (3.8) | 10 (2.0) |
|
| |
| Restrictive | 9 (1.9) | - |
| ||
| Food waste | 4 (0.8) | - |
| ||
| Social Norms | Food culture | 7 (1.5) | 3 (0.6) |
|
|
| PBC | Motivation | 175 (36.9) | 102 (20.1) |
|
|
| Affordability | 119 (25.1) | 92 (18.2) |
|
| |
| Time/effort | 106 (22.4) | 67 (13.2) |
|
| |
| Food access | 96 (20.3) | 162 (32.0) |
|
| |
| Knowledge | 51 (10.8) | 227 (44.8) |
|
| |
| Food outlets | 19 (4.0) | 13 (2.6) |
|
| |
| Cooking skills/equipment | 13 (2.7) | 28 (5.5) |
|
| |
| Natural conditions | 5 (1.1) | 7 (1.4) |
|
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scannell, N.; Villani, A.; Mantzioris, E.; Swanepoel, L. Understanding the Self-Perceived Barriers and Enablers toward Adopting a Mediterranean Diet in Australia: An Application of the Theory of Planned Behaviour Framework. Int. J. Environ. Res. Public Health 2020, 17, 9321. https://doi.org/10.3390/ijerph17249321
Scannell N, Villani A, Mantzioris E, Swanepoel L. Understanding the Self-Perceived Barriers and Enablers toward Adopting a Mediterranean Diet in Australia: An Application of the Theory of Planned Behaviour Framework. International Journal of Environmental Research and Public Health. 2020; 17(24):9321. https://doi.org/10.3390/ijerph17249321
Chicago/Turabian StyleScannell, Nicole, Anthony Villani, Evangeline Mantzioris, and Libby Swanepoel. 2020. "Understanding the Self-Perceived Barriers and Enablers toward Adopting a Mediterranean Diet in Australia: An Application of the Theory of Planned Behaviour Framework" International Journal of Environmental Research and Public Health 17, no. 24: 9321. https://doi.org/10.3390/ijerph17249321