Validity of Consumer Activity Monitors and an Algorithm Using Smartphone Data for Measuring Steps during Different Activity Types

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Collection and Analysis
3. Results
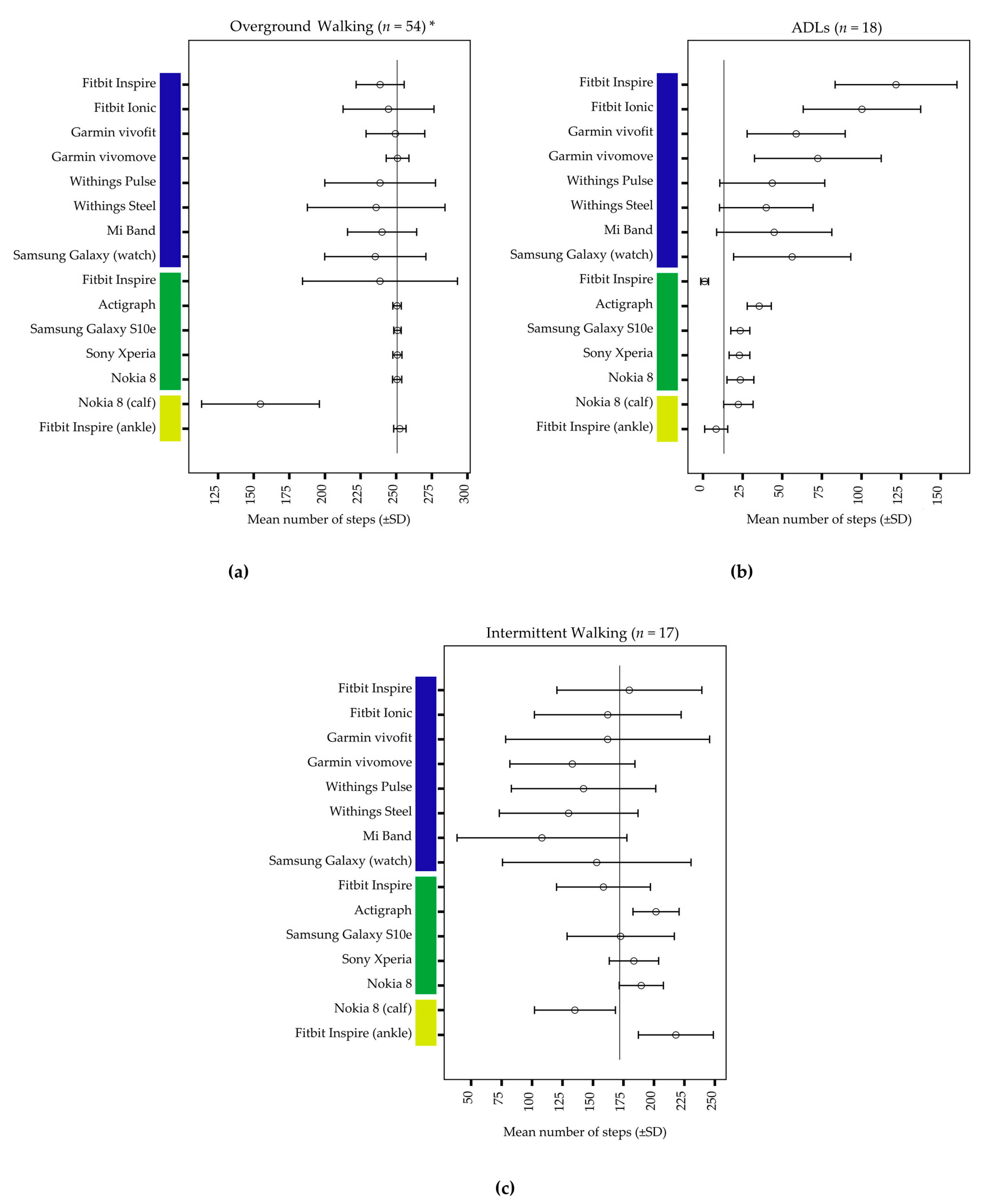
3.1. Overground Walking
3.2. Activities of Daily Living
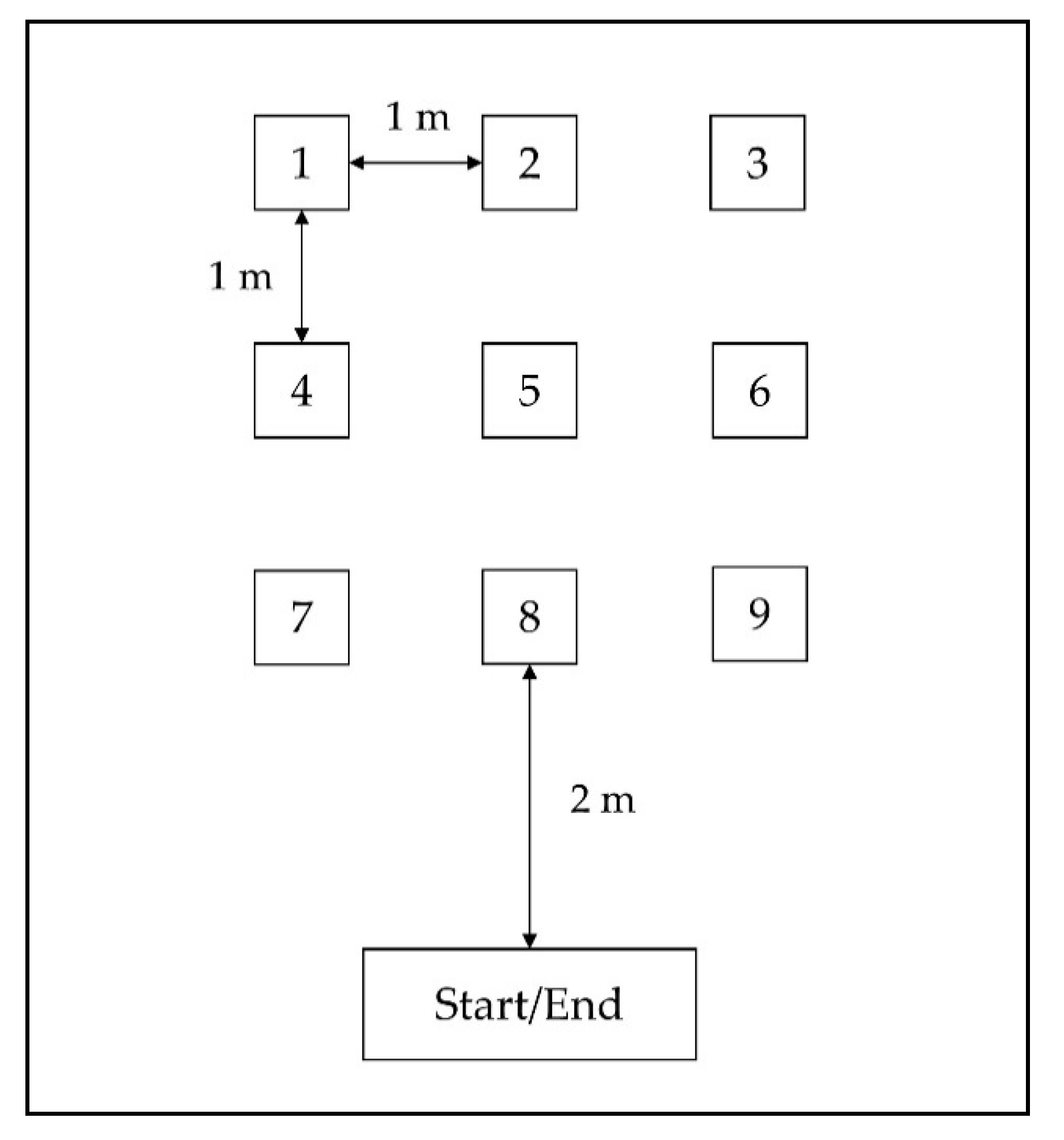
3.3. Intermittent Walking
4. Discussion
4.1. Overground Walking
4.2. Activities of Daily Living
4.3. Intermittent Walking
4.4. Observations on Device Level
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
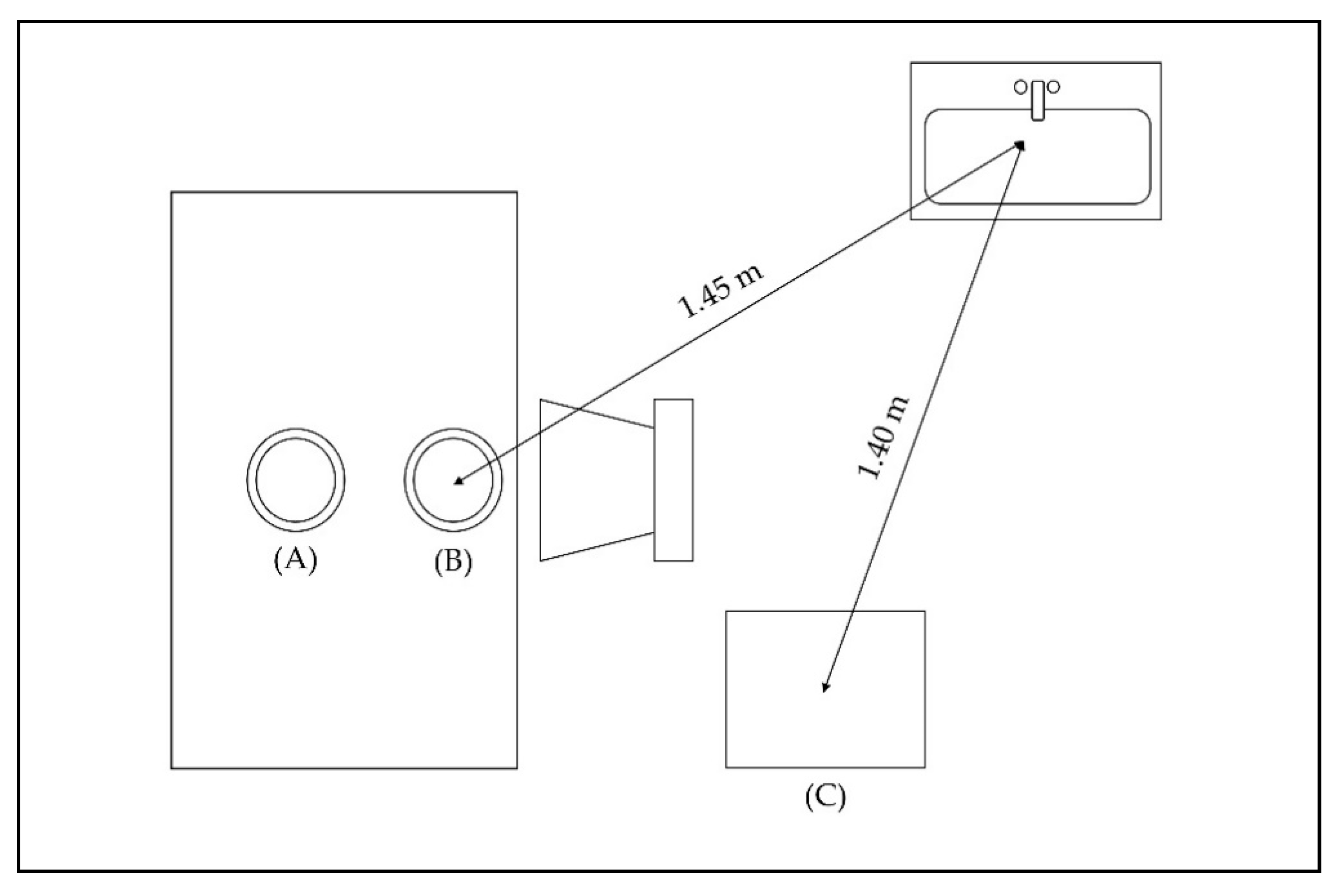
Appendix A

- Stand at the starting point.
- Turn around and walk to the hand wash basin to wash your hands with water and soap. Dry your hands with a towel.
- Walk to the table and sit down on the chair next to the table.
- Take five white plates and put them on the right side of the stack (one at a time), while using both hands together.
- Repeat the same task for the other five white plates, but this time, put them on the left side of the stack.
- Take 10 candies from the bowl (one at a time) with your right hand and then put them on the red plate.
- Repeat the same task with your left hand.
- Bring 10 candies (one at a time) with your right hand to your mouth (just acting like eating them) and then put them on the table next to the red plate.
- Repeat the task with your left hand.
- Stand up, take the red plate to the hand wash basin, wash it up, and then dry it with the towel.
- Come back to the table, sit down again on the chair next to the table, and put the red plate back where it was before.
- Take all five plates from the right side of the red plate (one at a time) and place them on the red plate, while using both hands together.
- Repeat the same task for the other five white plates.
- Stand up and walk to the finishing point.
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Bauman, A.; Phongsavan, P.; Schoeppe, S.; Owen, N. Physical activity measurement—a primer for health promotion. Promot. Educ. 2006, 13, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Marshall, S.J.; Barreira, T.V.; Lee, J.-O. Effect of pedometer-based physical activity interventions: A meta-analysis. Res. Q. Exerc. Sport 2009, 80, 648–655. [Google Scholar] [CrossRef]
- Wright, S.P.; Hall Brown, T.S.; Collier, S.R.; Sandberg, K. How consumer physical activity monitors could transform human physiology research. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R358–R367. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. Guide to the assessment of physical activity: Clinical and research applications: A scientific statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef]
- Silfee, V.J.; Haughton, C.F.; Jake-Schoffman, D.E.; Lopez-Cepero, A.; May, C.N.; Sreedhara, M.; Rosal, M.C.; Lemon, S.C. Objective measurement of physical activity outcomes in lifestyle interventions among adults: A systematic review. Prev. Med. Rep. 2018, 11, 74–80. [Google Scholar] [CrossRef]
- Plasqui, G.; Westerterp, K.R. Physical activity assessment with accelerometers: An evaluation against doubly labeled water. Obesity (Silver Spring) 2007, 15, 2371–2379. [Google Scholar] [CrossRef]
- Gresham, G.; Schrack, J.; Gresham, L.M.; Shinde, A.M.; Hendifar, A.E.; Tuli, R.; Rimel, B.J.; Figlin, R.; Meinert, C.L.; Piantadosi, S. Wearable activity monitors in oncology trials: Current use of an emerging technology. Contemp. Clin. Trials 2018, 64, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, A.; Mikalsen, M.H.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef]
- Shin, G.; Jarrahi, M.H.; Fei, Y.; Karami, A.; Gafinowitz, N.; Byun, A.; Lu, X. Wearable activity trackers, accuracy, adoption, acceptance and health impact: A systematic literature review. J. Biomed. Inform. 2019, 93, 103153. [Google Scholar] [CrossRef] [PubMed]
- Dobkin, B.H.; Martinez, C. Wearable Sensors to Monitor, Enable Feedback, and Measure Outcomes of Activity and Practice. Curr. Neurol. Neurosci. Rep. 2018, 18, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuah, S.H.-W.; Rauschnabel, P.A.; Krey, N.; Nguyen, B.; Ramayah, T.; Lade, S. Wearable technologies: The role of usefulness and visibility in smartwatch adoption. Comput. Human Behav. 2016, 65, 276–284. [Google Scholar] [CrossRef]
- Imboden, M.T.; Nelson, M.B.; Kaminsky, L.A.; Montoye, A.H. Comparison of four Fitbit and Jawbone activity monitors with a research-grade ActiGraph accelerometer for estimating physical activity and energy expenditure. Br. J. Sports Med. 2018, 52, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Mercer, K.; Li, M.; Giangregorio, L.; Burns, C.; Grindrod, K. Behavior Change Techniques Present in Wearable Activity Trackers: A Critical Analysis. JMIR Mhealth Uhealth 2016, 4, e40. [Google Scholar] [CrossRef] [Green Version]
- Höchsmann, C.; Knaier, R.; Infanger, D.; Schmidt-Trucksäss, A. Validity of smartphones and activity trackers to measure steps in a free-living setting over three consecutive days. Physiol. Meas. 2020, 41, 15001. [Google Scholar] [CrossRef]
- Pew Research Center. Smartphone Ownership Is Growing Rapidly Around the World, but Not Always Equally, 5 February 2019. Available online: https://www.pewresearch.org/global/2019/02/05/smartphone-ownership-is-growing-rapidly-around-the-world-but-not-always-equally/ (accessed on 4 June 2020).
- Dwyer, T.; Pezic, A.; Sun, C.; Cochrane, J.; Venn, A.; Srikanth, V.; Jones, G.; Shook, R.P.; Shook, R.; Sui, X.; et al. Objectively Measured Daily Steps and Subsequent Long Term All-Cause Mortality: The Tasped Prospective Cohort Study. PLoS ONE 2015, 10, e0141274. [Google Scholar] [CrossRef]
- Wattanapisit, A.; Thanamee, S. Evidence Behind 10,000 Steps Walking. J. Health Res. 2017, 31, 241–248. [Google Scholar]
- Case, M.A.; Burwick, H.A.; Volpp, K.G.; Patel, M.S. Accuracy of smartphone applications and wearable devices for tracking physical activity data. JAMA 2015, 313, 625–626. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Spade, C.L. Review of Validity and Reliability of Garmin Activity Trackers. J. Meas. Phys. Behav. 2020, 3, 170–185. [Google Scholar] [CrossRef]
- Feehan, L.M.; Geldman, J.; Sayre, E.C.; Park, C.; Ezzat, A.M.; Yoo, J.Y.; Hamilton, C.B.; Li, L.C. Accuracy of Fitbit Devices: Systematic review and narrative syntheses of quantitative data. JMIR Mhealth Uhealth 2018, 6, e10527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunn, J.A.; Navalta, J.W.; Fountaine, C.J.; Reece, J.D. Current state of commercial wearable technology in physical activity monitoring 2015–2017. Int. J. Exerc. Sci. 2018, 11, 503–515. [Google Scholar] [PubMed]
- Moore, C.C.; McCullough, A.K.; Aguiar, E.J.; Ducharme, S.W.; Tudor-Locke, C. Toward harmonized treadmill-based validation of step-counting wearable technologies: A scoping review. J. Phys. Act. Health 2020, 17, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Toth, L.P.; Park, S.; Springer, C.M.; Feyerabend, M.D.; Steeves, J.A.; Bassett, D.R. Video-recorded validation of wearable step counters under free-living conditions. Med. Sci. Sports Exerc. 2018, 50, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-D.; Kuo, C.-C.; Pellegrini, C.A.; Hsu, M.-J. Accuracy of Wristband activity monitors during ambulation and activities. Med. Sci. Sports Exerc. 2016, 48, 1942–1949. [Google Scholar] [CrossRef]
- Alinia, P.; Cain, C.; Fallahzadeh, R.; Shahrokni, A.; Cook, D.; Ghasemzadeh, H. How accurate is your activity tracker? A comparative study of step counts in low-intensity physical activities. JMIR Mhealth Uhealth 2017, 5, e106. [Google Scholar] [CrossRef]
- Nelson, M.B.; Kaminsky, L.A.; Dickin, D.C.; Montoye, A.H.K. Validity of WAS. Med. Sci. Sports Exerc. 2016, 48, 1619–1628. [Google Scholar] [CrossRef] [Green Version]
- Toth, L.P.; Park, S.; Pittman, W.L.; Sarisaltik, D.; Hibbing, P.R.; Morton, A.L.; Springer, C.M.; Crouter, S.E.; Bassett, D.R. Effects of Brief Intermittent Walking Bouts on Step Count Accuracy of Wearable Devices. J. Meas. Phys. Behav. 2019, 2, 13–21. [Google Scholar] [CrossRef]
- Degroote, L.; Hamerlinck, G.; Poels, K.; Maher, C.; Crombez, G.; Bourdeaudhuij, I.D.; Vandendriessche, A.; Curtis, R.G.; DeSmet, A. Low-cost consumer-based trackers to measure physical activity and sleep duration among adults in free-living conditions: Validation study. JMIR Mhealth Uhealth 2020, 8, e16674. [Google Scholar] [CrossRef]
- Stampfer, C.; Heinke, H.; Staacks, S. A lab in the pocket. Nat. Rev. Mater. 2020, 5, 169–170. [Google Scholar] [CrossRef]
- Shammas, L. Objective Assessment of Motor and Gait Parameters of Patients with Multiple Sclerosis. Ph.D. Thesis, Karlsruhe Institute of Technology, Karlsruhe, Germany, 15 February 2018. [Google Scholar]
- De Vet, H.C.W.; Terwee, C.B.; Knol, D.L.; Bouter, L.M. When to use agreement versus reliability measures. J. Clin. Epidemiol. 2006, 59, 1033–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Andover, UK, 2019. [Google Scholar]
- Höchsmann, C.; Knaier, R.; Eymann, J.; Hintermann, J.; Infanger, D.; Schmidt-Trucksäss, A. Validity of activity trackers, smartphones, and phone applications to measure steps in various walking conditions. Scand. J. Med. Sci. Sports 2018, 28, 1818–1827. [Google Scholar] [CrossRef] [PubMed]
- Riel, H.; Rathleff, C.R.; Kalstrup, P.M.; Madsen, N.K.; Pedersen, E.S.; Pape-Haugaard, L.B.; Villumsen, M. Comparison between Mother, ActiGraph wGT3X-BT, and a hand tally for measuring steps at various walking speeds under controlled conditions. PeerJ 2016, 4, e2799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Brooks, D.; Thomas, S.; Eysenbach, G.; Nolan, R.P. Lifesource XL-18 pedometer for measuring steps under controlled and free-living conditions. J. Sports Sci. 2015, 33, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Battenberg, A.K.; Donohoe, S.; Robertson, N.; Schmalzried, T.P. The accuracy of personal activity monitoring devices. Semin. Arthroplasty 2017, 28, 71–75. [Google Scholar] [CrossRef]
- Gaz, D.V.; Rieck, T.M.; Peterson, N.W.; Ferguson, J.A.; Schroeder, D.R.; Dunfee, H.A.; Henderzahs-Mason, J.M.; Hagen, P.T. Determining the validity and accuracy of multiple activity-tracking devices in controlled and free-walking conditions. Am. J. Health Promot. 2018, 32, 1671–1678. [Google Scholar] [CrossRef]
- Wong, C.K.; Mentis, H.M.; Kuber, R. The bit doesn’t fit: Evaluation of a commercial activity-tracker at slower walking speeds. Gait Posture 2018, 59, 177–181. [Google Scholar] [CrossRef]
- Presset, B.; Laurenczy, B.; Malatesta, D.; Barral, J. Accuracy of a smartphone pedometer application according to different speeds and mobile phone locations in a laboratory context. J. Exerc. Sci. Fit. 2018, 16, 43–48. [Google Scholar] [CrossRef]
- Beltrán-Carrillo, V.J.; Jiménez-Loaisa, A.; Alarcón-López, M.; Elvira, J.L.L. Validity of the “Samsung Health” application to measure steps: A study with two different samsung smartphones. J. Sports Sci. 2019, 37, 788–794. [Google Scholar] [CrossRef]
- Brodie, M.A.; Pliner, E.M.; Ho, A.; Li, K.; Chen, Z.; Gandevia, S.C.; Lord, S.R. Big data vs accurate data in health research: Large-scale physical activity monitoring, smartphones, wearable devices and risk of unconscious bias. Med. Hypotheses 2018, 119, 32–36. [Google Scholar] [CrossRef]
- Montes, J.; Tandy, R.; Young, J.; Lee, S.-P.; Navalta, J.W. Step Count reliability and validity of five wearable technology devices while walking and jogging in both a free motion setting and on a treadmill. Int. J. Exerc. Sci. 2020, 13, 410–426. [Google Scholar] [PubMed]
- Tudor-Locke, C.; Sisson, S.B.; Lee, S.M.; Craig, C.L.; Plotnikoff, R.C.; Bauman, A. Evaluation of quality of commercial pedometers. Can. J. Public Health 2006, 97, S10–S15. [Google Scholar] [CrossRef] [PubMed]
- Redmayne, M. Where’s your phone? A survey of where women aged 15–40 carry their smartphone and related risk perception: A survey and pilot study. PLoS ONE 2017, 12, e0167996. [Google Scholar] [CrossRef] [PubMed]
- Redmayne, M. New Zealand adolescents’ cellphone and cordless phone user-habits: Are they at increased risk of brain tumours already? A cross-sectional study. Environ. Health 2013, 12, 5. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
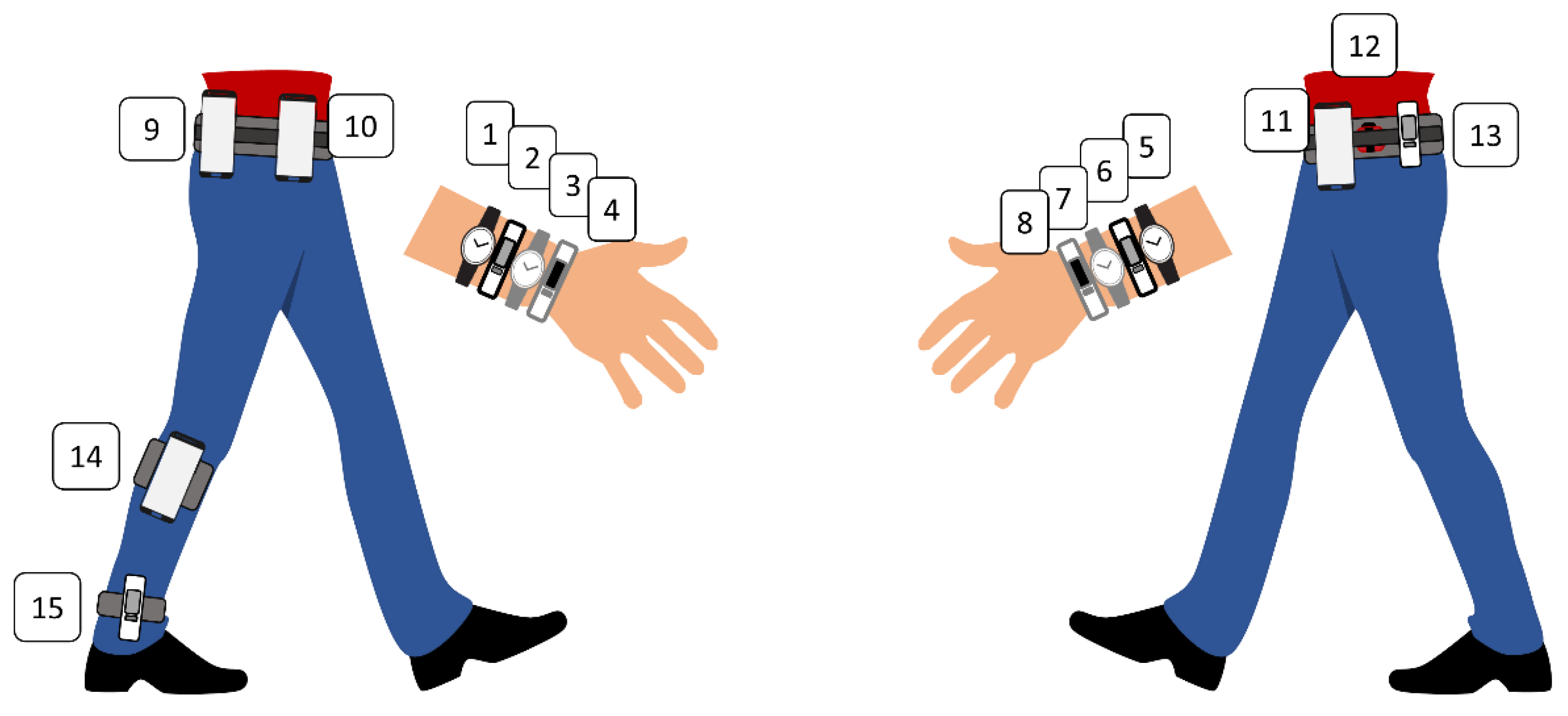
| Manufacturer | Device (Type) | Sensors | Price 1 (€) | Placement | |||
|---|---|---|---|---|---|---|---|
| Wrist | Hip | Calf | Ankle 2 | ||||
| Fitbit Inc., San Francisco, CA, USA | Inspire (CAM) | 3-axis accelerometer | 76 | x | x | x2 | |
| Ionic (CAM) | 3-axis accelerometer, altimeter, gyroscope, PPG, GPS, ambient light sensor | 229 | x | ||||
| Garmin Ltd., Olathe, KS, USA | vivofit 4 (CAM) | Accelerometer | 60 | x | |||
| vivomove HR (CAM) | Accelerometer, barometer, PPG, ambient light sensor | 163 | x | ||||
| Withings, Issy-les-Mouline-aux, France | Pulse HR (CAM) | 3-axis accelerometer, PPG, ambient light sensor | 100 | x | |||
| Steel HR (CAM) | 3-axis accelerometer, day and night motion sensor | 145 | x | ||||
| Xiaomi Corp. Beijing, China | Mi Band 3 (CAM) | 3-axis accelerometer, PPG | 27 | x | |||
| Samsung, Seoul, South Korea | Galaxy Watch Active (CAM) | Accelerometer, barometer, gyroscope, PPG, light sensor | 187 | x | |||
| ActiGraph LLC, Pensacola, FL, USA | wGT3X-BT (RGAM) | 3-axis accelerometer, wear time sensor, ambient light sensor | 239 3 | x | |||
| Samsung, Seoul, South Korea | Galaxy S10e (smartphone) | Accelerometer, barometer, gyroscope, proximity sensor, hall sensor, geomagnetic sensor, light sensor | 564 | x | |||
| Nokia Corporation, Espoo, Finland | Nokia 8 (smartphone) | Accelerometer, barometer, gyroscope, proximity sensor, e-compass, hall sensor, light sensor | 250 | x | x | ||
| Sony Corporation, Tokyo, Japan | Xperia 10 (smartphone) | Accelerometer, barometer, gyroscope, proximity sensor, e-compass, hall sensor, magnetometer, step counter, significant motion detector, light sensor | 285 | x | |||
| Characteristics | N = 18 |
|---|---|
| Male/Female (n) | 7/11 |
| Age (years) | 28.8 (5.0) |
| Height (cm) | 173.9 (10.4) |
| Weight (kg) | 70.2 (17.1) |
| Dominance foot (r/l) (n) | 14/4 |
| Dominance hand (r/l) (n) | 17/1 |
| Activity Monitors | Overground Walking | ADLs | Intermittent Walking | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean Difference (SD) | MAPE (%) | n | Mean Difference (SD) | MAPE (%) | n | Mean Difference (SD) | MAPE (%) | |
| Fitbit Inspire | 54 | −12.0 (17.0) | 5.3 | 18 | 108.6 (38.5) | 861.2 | 17 | 7.9 (59.1) | 28.8 |
| Fitbit Ionic | 54 | −6.1 (32.1) | 8.4 | 18 | 87.1 (37.5) | 704.9 | 17 | −9.8 (60.0) | 30.8 |
| Garmin vivofit | 49 | −1.2 (20.6) | 2.9 * | 18 | 45.6 (30.6) | 379.7 | 17 | −9.9 (80.2) | 37.6 |
| Garmin vivomove | 54 | 0.3 (7.8) | 1.7 * | 18 | 59.2 (41.1) | 491.9 | 17 | −38.8 (51.1) | 28.3 |
| Withings Pulse | 54 | −12.0 (38.8) | 5.7 | 17 | 30.5 (31.9) | 239.9 | 17 | −29.6 (59.1) | 30.2 |
| Withings Steel | 54 | −14.7 (48.2) | 6.6 | 18 | 26.7 (28.5) | 208.6 | 17 | −41.9 (58.3) | 30.3 |
| Mi Band 3 | 54 | −10.6 (24.1) | 4.9 | 18 | 31.7 (35.3) | 269.6 | 17 | −63.8 (73.9) | 47.3 |
| Samsung Galaxy | 53 | −15.4 (35.5) | 6.3 | 18 | 43.1 (37.2) | 358.6 | 17 | −18.8 (80.3) | 39.5 |
| Fibit Inspire (hip) | 54 | −12.1 (54.5) | 5.8 | 18 | −12.2 (4.1) | 91.3 | 17 | −13.3 (42.9) | 19.3 |
| Fitbit Inspire (ankle) | 54 | 1.9 (4.2) | 0.9 * | 18 | −4.9 (5.7) | 48.2 | 17 | 46.1 (32.0) | 31.2 |
| Samsung Galaxy S10e | 54 | 0.2 (2.0) | 0.3 * | 18 | 10.3 (6.9) | 86.6 | 17 | 0.8 (41.7) | 12.3 |
| Nokia 8 | 54 | −0.1 (2.8) | 0.4 * | 18 | 10.4 (9.3) | 89.0 | 17 | 17.8 (16.6) | 11.2 |
| Sony Xperia | 54 | 0.1 (3.0) | 0.6 * | 18 | 9.8 (7.1) | 86.1 | 17 | 11.7 (24.3) | 12.5 |
| Nokia 8 (calf) | 54 | −95.9 (41.5) | 38.2 | 18 | 9.1 (8.6) | 83.8 | 17 | −36.7 (38.7) | 26.3 |
| ActiGraph | 54 | −0.1 (2.4) | 0.5 * | 18 | 22.3 (7.3) | 177.3 | 17 | 29.8 (19.4) | 17.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartung, V.; Sarshar, M.; Karle, V.; Shammas, L.; Rashid, A.; Roullier, P.; Eilers, C.; Mäurer, M.; Flachenecker, P.; Pfeifer, K.; et al. Validity of Consumer Activity Monitors and an Algorithm Using Smartphone Data for Measuring Steps during Different Activity Types. Int. J. Environ. Res. Public Health 2020, 17, 9314. https://doi.org/10.3390/ijerph17249314
Hartung V, Sarshar M, Karle V, Shammas L, Rashid A, Roullier P, Eilers C, Mäurer M, Flachenecker P, Pfeifer K, et al. Validity of Consumer Activity Monitors and an Algorithm Using Smartphone Data for Measuring Steps during Different Activity Types. International Journal of Environmental Research and Public Health. 2020; 17(24):9314. https://doi.org/10.3390/ijerph17249314
Chicago/Turabian StyleHartung, Verena, Mustafa Sarshar, Viktoria Karle, Layal Shammas, Asarnusch Rashid, Paul Roullier, Caroline Eilers, Mathias Mäurer, Peter Flachenecker, Klaus Pfeifer, and et al. 2020. "Validity of Consumer Activity Monitors and an Algorithm Using Smartphone Data for Measuring Steps during Different Activity Types" International Journal of Environmental Research and Public Health 17, no. 24: 9314. https://doi.org/10.3390/ijerph17249314