Healthy Pregnancies Project: Cluster Randomized Controlled Trial of a Community Intervention to Reduce Tobacco Use among Alaska Native Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
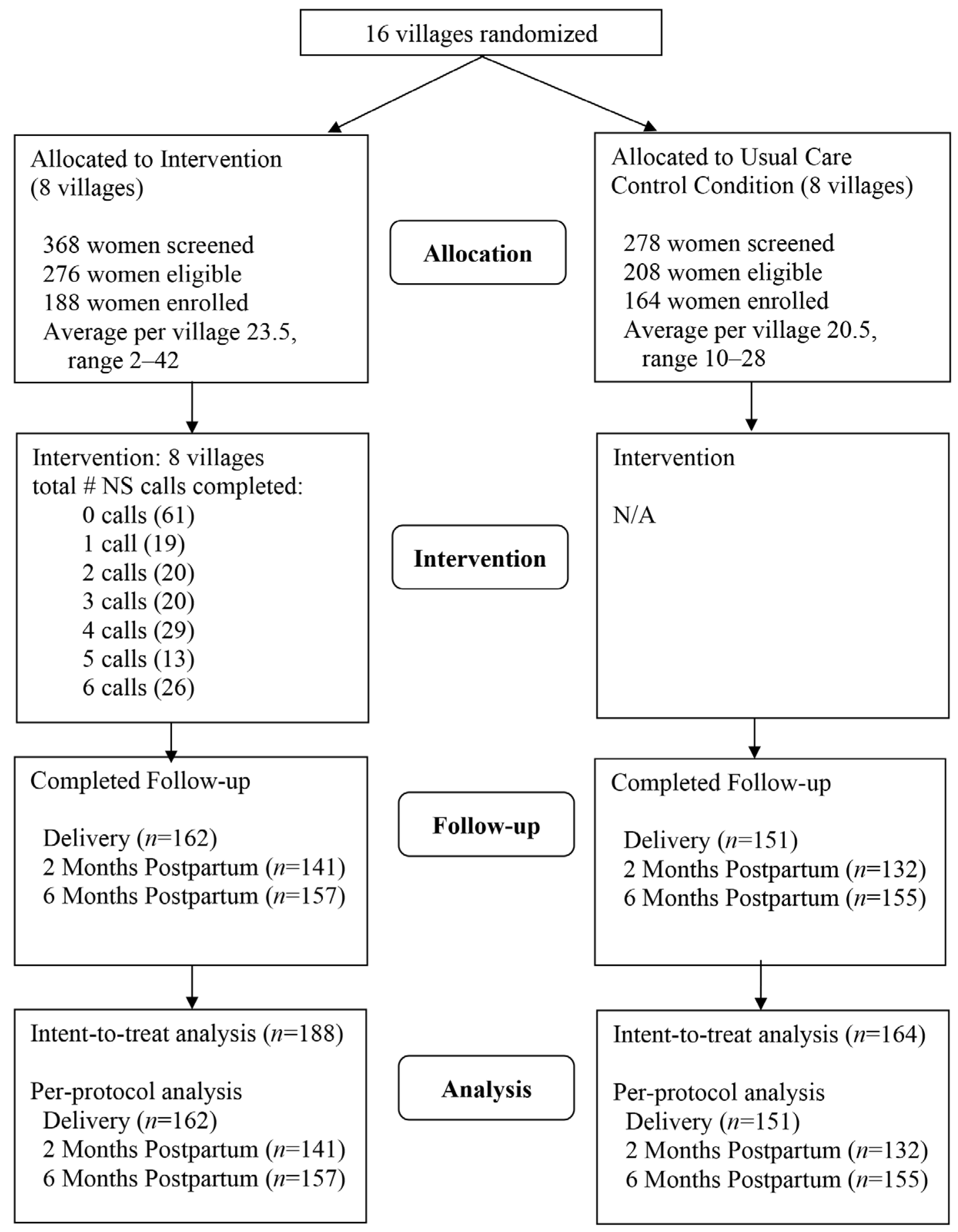
2.2. Study Design
2.3. Participants
2.4. Treatments
2.4.1. Usual Care Components Common to All Study Villages
2.4.2. Control Villages
2.4.3. Intervention Villages
2.5. Measures
2.6. Statistical Methods
3. Results
3.1. Participants
3.2. Intervention Implementation
3.3. Tobacco Use
3.4. Participant Feedback
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gould, G.S.; Patten, C.; Glover, M.; Kira, A.; Jayasinghe, H. Smoking in pregnancy among Indigenous women in high-income countries: A narrative review. Nicotine Tob. Res. 2017, 19, 506–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, C.; O’Mara-Eves, A.; Porter, J.; Coleman, T.; Perlen, S.M.; Thomas, J.; McKenzie, J.E. Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Database Syst. Rev. 2017, 2, CD001055. [Google Scholar] [CrossRef] [PubMed]
- Alaska Department of Health and Social Services. Division of Public Health. Section of Chronic Disease Prevention and Health Promotion. Alaska Tobacco Facts-2019 Update. Available online: http://dhss.alaska.gov/dph/Chronic/Documents/Tobacco/PDF/2019_AKTobaccoFacts.pdf (accessed on 18 November 2020).
- Hurt, R.D.; Renner, C.C.; Patten, C.A.; Ebbert, J.O.; Offord, K.P.; Schroeder, D.R.; Enoch, C.C.; Gill, L.; Angstman, S.E.; Moyer, T.P. Iqmik—A form of smokeless tobacco used by pregnant Alaska Natives: Nicotine exposure in their neonates. J. Matern. Fetal Neonatal. Med. 2005, 17, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Renner, C.C.; Patten, C.A.; Enoch, C.; Petraitis, J.; Offord, K.P.; Angstman, S.; Garrison, A.; Nevak, C.; Croghan, I.T.; Hurt, R.D. Focus groups of Y-K Delta Alaska Natives: Attitudes toward tobacco use and tobacco dependence interventions. Prev. Med. 2004, 38, 421–431. [Google Scholar] [CrossRef]
- Patten, C.A.; Windsor, R.A.; Renner, C.C.; Enoch, C.; Hochreiter, A.; Nevak, C.; Smith, C.A.; Decker, P.A.; Bonnema, S.; Hughes, C.A.; et al. Feasibility of a tobacco cessation intervention for pregnant Alaska Native women. Nicotine Tob. Res. 2010, 12, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Patten, C.; Lando, H.; Desnoyers, C.; Barrows, Y.; Klejka, J.; Decker, P.; Hughes, C.; Bock, M.; Boyer, R.; Resnicow, K.; et al. The Healthy Pregnancies Project: Study protocol and baseline characteristics for a cluster-randomized controlled trial of a community intervention to recduce tobacco use among Alaska Native pregnant women. Contemp. Clin. Trials 2019, 78, 116–125. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Best Practices for Comprehensive Tobacco Control Programs-2014. Available online: https://www.cdc.gov/tobacco/stateandcommunity/best_practices/pdfs/2014/comprehensive.pdf (accessed on 15 March 2020).
- Burhansstipanov, L.; Dignan, M.B.; Schumacher, A.; Krebs, L.U.; Alfonsi, G.; Apodaca, C.C. Breast screening navigator programs within three settings that assist underserved women. J. Cancer Educ. 2010, 25, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Burhansstipanov, L.; Krebs, L.U.; Dignan, M.B.; Jones, K.; Harjo, L.D.; Watanabe-Galloway, S.; Petereit, D.G.; Pingatore, N.L.; Isham, D. Findings from the Native Navigators and the Cancer Continuum (NNACC) study. J. Cancer Educ. 2014, 29, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Patten, C.A.; Renner, C.C.; Decker, P.A.; O’Campo, E.; Larsen, K.; Enoch, C.; Offord, K.P.; Hurt, R.D.; Lanier, A.; Kaur, J. Tobacco use and cessation among pregnant Alaska Natives from Western Alaska enrolled in the WIC program, 2001–2002. Matern Child Health J. 2008, 12, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Patten, C.A.; Lando, H.; Resnicow, K.; Decker, P.A.; Smith, C.M.; Hanza, M.M.; Burhansstipanov, L.; Scott, M. Developing health communication messaging for a social marketing campaign to reduce tobacco use in pregnancy among Alaska Native women. J. Commun. Healthc. 2018, 11, 252–262. [Google Scholar] [CrossRef]
- Fiore, M.C.; Jaen, C.R.; Baker, T.B.; Bailey, W.C.; Benowitz, N.L.; Curry, S.J.; Dorfman, S.F.; Froelicher, E.S.; Goldstein, M.G.; Healton, C.G.; et al. Treating Tobacco Use and Dependence: 2008 Update Clinical Practice Guideline; Public Health Service; U.S. Department of Health and Human Services: Rockville, MD, USA, 2008.
- Patten, C.A.; Enoch, C.; Renner, C.C.; Larsen, K.; Decker, P.A.; Anderson, K.J.; Nevak, C.; Glasheen, A.; Offord, K.P.; Lanier, A. Evaluation of a tobacco educational intervention for pregnant Alaska Native women. J. Health Dispar. Res. Pract. 2008, 2, 33–50. [Google Scholar] [PubMed]
- Eiden, R.D.; Molnar, D.S.; Leonard, K.E.; Colder, C.R.; Homish, G.G.; Maiorana, N.; Schuetze, P.; Connors, G.J. Sources and frequency of secondhand smoke exposure during pregnancy. Nicotine Tob. Res. 2011, 13, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Finnegan, J.R., Jr.; Murray, D.M.; Kurth, C.; McCarthy, P. Measuring and tracking education program implementation: The Minnesota Heart Health Program experience. Health Educ. Q. 1989, 16, 77–90. [Google Scholar] [CrossRef]
- Morris, D.S.; Rooney, M.P.; Wray, R.J.; Kreuter, M.W. Measuring exposure to health messages in community-based intervention studies: A systematic review of current practices. Health Educ. Behav. 2009, 36, 979–998. [Google Scholar] [CrossRef]
- Piper, M.E.; Bullen, C.; Krishnan-Sarin, S.; Rigotti, N.A.; Steinberg, M.L.; Streck, J.M.; Joseph, A.M. Defining and measuring abstinence in clinical trials of smoking cessation interventions: An updated review. Nicotine Tob. Res. 2019, ntz110. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Bernert, J.T.; Foulds, J.; Hecht, S.S.; Jacob, P.; Jarvis, M.J.; Joseph, A.; Oncken, C.; Piper, M.E. Biochemical Verification of tobacco use and abstinence: 2019 Update. Nicotine Tob. Res. 2019. [Google Scholar] [CrossRef]
- Cooke, F.; Bullen, C.; Whittaker, R.; McRobbie, H.; Chen, M.H.; Walker, N. Diagnostic accuracy of NicAlert cotinine test strips in saliva for verifying smoking status. Nicotine Tob. Res. 2008, 10, 607–612. [Google Scholar] [CrossRef]
- Georgescu, I.M.; Tarcea, M.; Marginean, C.; Ruta, F.; Rus, V.; Sipos, R.; Abram, Z. Relationship between high levels of salivary cotinine test and demographic characteristics of pregnant smokers from Mures County. Acta Medica Marisiensis 2017, 63, 31–35. [Google Scholar] [CrossRef] [Green Version]
- Zeger, S.L.; Liang, K.Y.; Albert, P.S. Models for longitudinal data: A generalized estimating equation approach. Biometrics 1988, 44, 1049–1060. [Google Scholar] [CrossRef] [Green Version]
- Krippendorff, K.H. Content Analysis: An Introduction to Its Methodology, 4th ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2019; ISBN 978-1-50639-566-1. [Google Scholar]
- Patten, C.A.; Koller, K.R.; Flanagan, C.A.; Hiratsuka, V.Y.; Hughes, C.A.; Wolfe, A.W.; Decker, P.A.; Fruth, K.; Brockman, T.A.; Korpela, M.; et al. Biomarker feedback intervention for smoking cessation among Alaska Native pregnant women: Randomized pilot study. Patient Educ. Couns. 2019, 102, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Glover, M.; Kira, A.; Walker, N.; Bauld, L. Using incentives to encourage smoking abstinence among pregnant Indigenous women? A feasibility study. Matern. Child Health J. 2015, 19, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Glover, M.; Kira, A.; Smith, C. Enlisting “Aunties” to support Indigenous pregnant women to stop smoking: Feasibility study results. Nicotine Tob. Res. 2016, 18, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Bovill, M.; Pollock, L.; Bonevski, B.; Gruppetta, M.; Atkins, L.; Carson-Chahhoud, K.; Boydell, K.M.; Gribbin, G.R.; Oldmeadow, C.; et al. Feasibility and acceptability of Indigenous Counselling and Nicotine (ICAN) QUIT in pregnancy multicomponent implementation intervention and study design for Australian Indigenous pregnant women: A pilot cluster randomised step-wedge trial. Addict. Behav. 2019, 90, 176–190. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.; Pullon, S.; Benn, C.; Cookson, T.; Dowell, A.; Viccars, A.; White, S.; Green, R.; Crooke, M. Can support and education for smoking cessation and reduction be provided effectively by midwives within primary maternity care? Midwifery 2004, 20, 37–50. [Google Scholar] [CrossRef]
- Eades, S.J.; Sanson-Fisher, R.W.; Wenitong, M.; Panaretto, K.; D’Este, C.; Gilligan, C.; Stewart, J. An intensive smoking intervention for pregnant Aboriginal and Torres Strait Islander women: A randomised controlled trial. Med. J. Aust. 2012, 197, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riaz, M.; Lewis, S.; Naughton, F.; Ussher, M. Predictors of smoking cessation during pregnancy: A systematic review and meta-analysis. Addiction 2018, 113, 610–622. [Google Scholar] [CrossRef]
- Tappin, D.; Bauld, L.; Purves, D.; Boyd, K.; Sinclair, L.; MacAskill, S.; McKell, J.; Friel, B.; McConnachie, A.; de Caestecker, L.; et al. Financial incentives for smoking cessation in pregnancy: Randomised controlled trial. BMJ 2015, 350, h134. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, C.A.; Koller, K.R.; Wolfe, A.W.; Thomas, T.K.; Benowitz, N.L.; Renner, C.C.; Hughes, C.; Hatsukami, D.K.; Bronars, C.; Murphy, N.J.; et al. Fetal exposure to carcinogens with tobacco use in pregnancy: Phase 1 MAW study findings. Nicotine Tob. Res. 2016, 18, 2162–2168. [Google Scholar] [CrossRef] [Green Version]
- Berard, A.; Zhao, J.P.; Sheehy, O. Success of smoking cessation interventions during pregnancy. Am. J. Obstet. Gynecol. 2016, 215, 611.e1–611.e8. [Google Scholar] [CrossRef]
- Haddad, A.; Davis, A.M. Tobacco smoking cessation in adults and pregnant women: Behavioral and pharmacotherapy interventions. JAMA 2016, 315, 2011–2012. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.R.; Mason, M.J.; Brown, A.R.; Garcia, C.M.; Seibers, A.D.; Stephens, C.J. Remote biochemical verification of tobacco use: Reducing costs and improving methodological rigor with mailed oral cotinine swabs. Addict Behav. 2018, 87, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Thrul, J.; Meacham, M.C.; Ramo, D.E. A novel and remote biochemical verification method of smoking abstinence: Predictors of participant compliance. Tob. Prev. Cessat. 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, P.S.; Koller, K.R.; Prochaska, J.J.; Hughes, C.A.; Bock, M.J.; Decker, P.A.; Flanagan, C.A.; Merritt, Z.T.; Meade, C.D.; Willetto, A.L.; et al. Social media intervention to promote smoking treatment utilization and cessation among Alaska Native people who smoke: Protocol for the Connecting Alaska Native People to Quit Smoking (CAN Quit) pilot study. JMIR Res. Protoc. 2019, 8, e15155. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Time Point | |||
|---|---|---|---|
| Campaign Component | Delivery (n = 156) % | 2 Months Postpartum (n = 139) % | 6 Months Postpartum (n = 156) % |
| 1. How much of the brochure did you read? | |||
| None of it | 20.5 | 23.7 | 13.5 |
| Some | 21.8 | 19.4 | 22.6 |
| Most | 14.7 | 12.2 | 12.3 |
| All | 34.0 | 41.7 | 43.2 |
| Did not receive it | 9.0 | 2.9 | 8.4 |
| 2. How much of the digital stories DVD did you watch? | |||
| None of it | 51.3 | 43.2 | 39.1 |
| Some | 9.6 | 7.9 | 9.0 |
| Most | 4.5 | 6.5 | 5.8 |
| All | 25.6 | 36.0 | 37.2 |
| Did not receive it | 9.0 | 6.5 | 9.0 |
| 3. Did you share the digital stories DVD, brochure, or promotional items (baby bibs) with family members or anyone else in your community? | |||
| Yes | 35.3 | 52.5 | 49.7 |
| No | 64.7 | 47.5 | 50.3 |
| 4. Did you talk about what you have learned in this study with anyone else? | |||
| Yes | 39.1 | 56.1 | 58.7 |
| No | 60.9 | 43.9 | 41.3 |
| 5. Have you seen a poster in your community about the Native Sisters program? | |||
| Yes | 62.2 | 73.4 | 79.5 |
| No | 37.8 | 26.6 | 20.5 |
| 6. Have others in your village talked about the posters, promotional items (hoodies, baby bibs), or Native Sisters program? | |||
| Yes | 23.7 | 38.8 | 33.8 |
| No | 76.3 | 61.2 | 67.2 |
| Total Score (mean ± SD, range) 2 | 3.5 ± 2.1 0–8 | 4.4 ± 2.3 0–8 | 4.5 ± 2.3 0–8 |
| Time Point 2 | Intervention n = 188 %, (n) | Usual Care Control n = 164 % (n) | p-Value 1,2 |
|---|---|---|---|
| Baseline | 63.8 (120/188) | 69.5 (114/164) | 0.37 |
| Delivery | |||
| Per protocol | 59.3 (96/162) | 64.9 (98/151) | 0.11 |
| Intent-to-treat | 64.9 (122/188) | 67.7 (111/164) | 0.45 |
| 2 months postpartum | |||
| Per protocol | 60.3 (85/141) | 65.2 (86/132) | 0.45 |
| Intent-to-treat | 70.2 (132/188) | 72.0 (118/164) | 0.73 |
| 6 months postpartum | |||
| Self-report | |||
| Per protocol | 66.9 (105/157) | 65.2 (101/155) | 0.74 |
| Intent-to-treat | 72.3 (136/188) | 67.1 (110/164) | 0.30 |
| Biochemically confirmed | |||
| Per protocol | 82.8 (130/157) | 81.3 (126/155) | 0.73 |
| Intent-to-treat | 85.6 (161/188) | 82.3 (135/164) | 0.38 |
| Baseline Tobacco Users | Baseline Non-Tobacco Users | |||||
|---|---|---|---|---|---|---|
| Time Point | Intervention Group n = 120 %, (n) | Usual Care Control Group n = 114 % (n) | p-Value 1 | Intervention Group n = 68 %, (n) | Usual Care Control Group n = 50 % (n) | p-Value 1,2 |
| Delivery | ||||||
| Per protocol | 78.9 (82/104) | 84.9 (90/106) | 0.15 | 24.1 (14/58) | 17.8 (8/45) | 0.51 (0.40) |
| Intent-to-treat | 81.7 (98/120) | 86.0 (98/114) | 0.30 | 35.3 (24/68) | 26.0 (13/50) | 0.36 (0.56) |
| 2 months postpartum | ||||||
| Per protocol | 81.4 (70/86) | 88.0 (81/92) | 0.24 | 27.3 (15/55) | 12.5 (5/40) | 0.075 (0.05) |
| Intent-to-treat | 86.7 (104/120) | 90.4 (103/114) | 0.38 | 41.2 (28/68) | 30.0 (15/50) | 0.20 (0.45) |
| 6 months postpartum | ||||||
| Self-report | ||||||
| Per protocol | 83.7 (82/98) | 84.7 (94/111) | 0.88 | 39.0 (23/59) | 15.9 (7/44) | 0.015 (0.04) |
| Intent-to-treat | 86.7 (104/120) | 85.1 (97/114) | 0.74 | 47.1 (32/68) | 26.0 (13/50) | 0.040 (0.09) |
| Biochemically confirmed | ||||||
| Per protocol | 94.9 (93/98) | 97.3 (108/111) | 0.35 | 62.7 (37/59) | 40.9 (18/44) | 0.014 (0.18) |
| Intent-to-treat | 95.8 (115/120) | 97.4 (111/114) | 0.51 | 67.7 (46/68) | 48.0 (24/50) | 0.043 (0.19) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patten, C.A.; Lando, H.A.; Desnoyers, C.A.; Bock, M.J.; Alexie, L.; Decker, P.A.; Hughes, C.A.; Resnicow, K.; Burhansstipanov, L.; Boyer, R.; et al. Healthy Pregnancies Project: Cluster Randomized Controlled Trial of a Community Intervention to Reduce Tobacco Use among Alaska Native Women. Int. J. Environ. Res. Public Health 2020, 17, 9302. https://doi.org/10.3390/ijerph17249302
Patten CA, Lando HA, Desnoyers CA, Bock MJ, Alexie L, Decker PA, Hughes CA, Resnicow K, Burhansstipanov L, Boyer R, et al. Healthy Pregnancies Project: Cluster Randomized Controlled Trial of a Community Intervention to Reduce Tobacco Use among Alaska Native Women. International Journal of Environmental Research and Public Health. 2020; 17(24):9302. https://doi.org/10.3390/ijerph17249302
Chicago/Turabian StylePatten, Christi A., Harry A. Lando, Chris A. Desnoyers, Martha J. Bock, Lucinda Alexie, Paul A. Decker, Christine A. Hughes, Kenneth Resnicow, Linda Burhansstipanov, Rahnia Boyer, and et al. 2020. "Healthy Pregnancies Project: Cluster Randomized Controlled Trial of a Community Intervention to Reduce Tobacco Use among Alaska Native Women" International Journal of Environmental Research and Public Health 17, no. 24: 9302. https://doi.org/10.3390/ijerph17249302