Development and External Validity of a Short-Form Version of the INICIARE Scale to Classify Nursing Care Dependency Level in Acute Hospitals

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
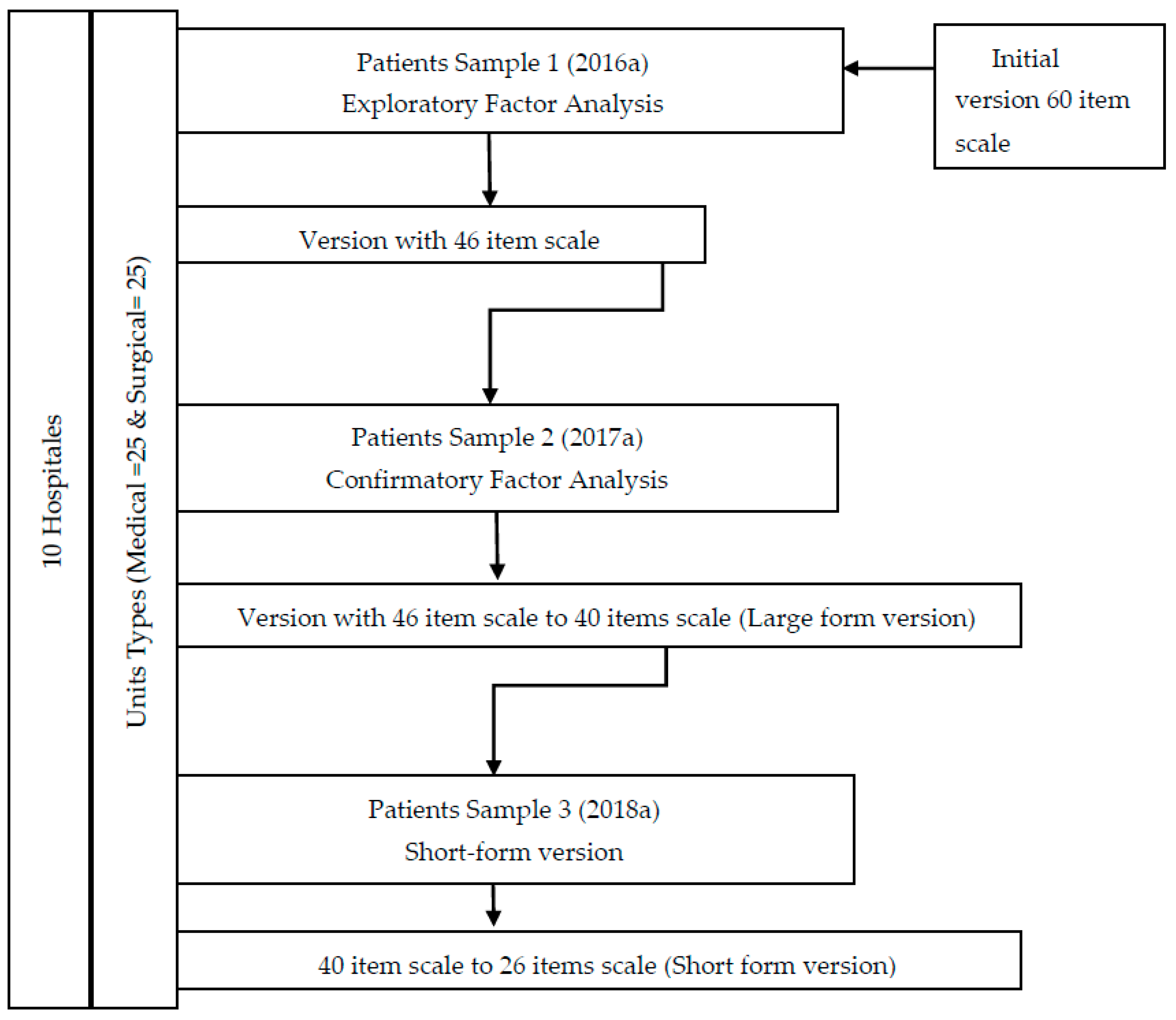
2.1. Study Design and Participants
2.2. Sampling and Sample
2.2.1. Sample 1
2.2.2. Sample 2
2.2.3. Sample 3
2.3. Data Collection Procedures
2.3.1. Recruitment
2.3.2. Training
2.3.3. Registration
2.4. Study Variables and Measures
2.4.1. Participant Characteristics
2.4.2. Hospital Characteristics
2.4.3. Instruments: INICIARE Scale and Care Dependency Scale (CDS)
2.5. Ethical Approvals
2.6. Data Analysis
Psychometric Testing
3. Results
3.1. Participant Characteristics
3.2. Psychometric Testing
3.2.1. Sample 1 (Initial 60-Item Scale to 46-Item Version Scale)
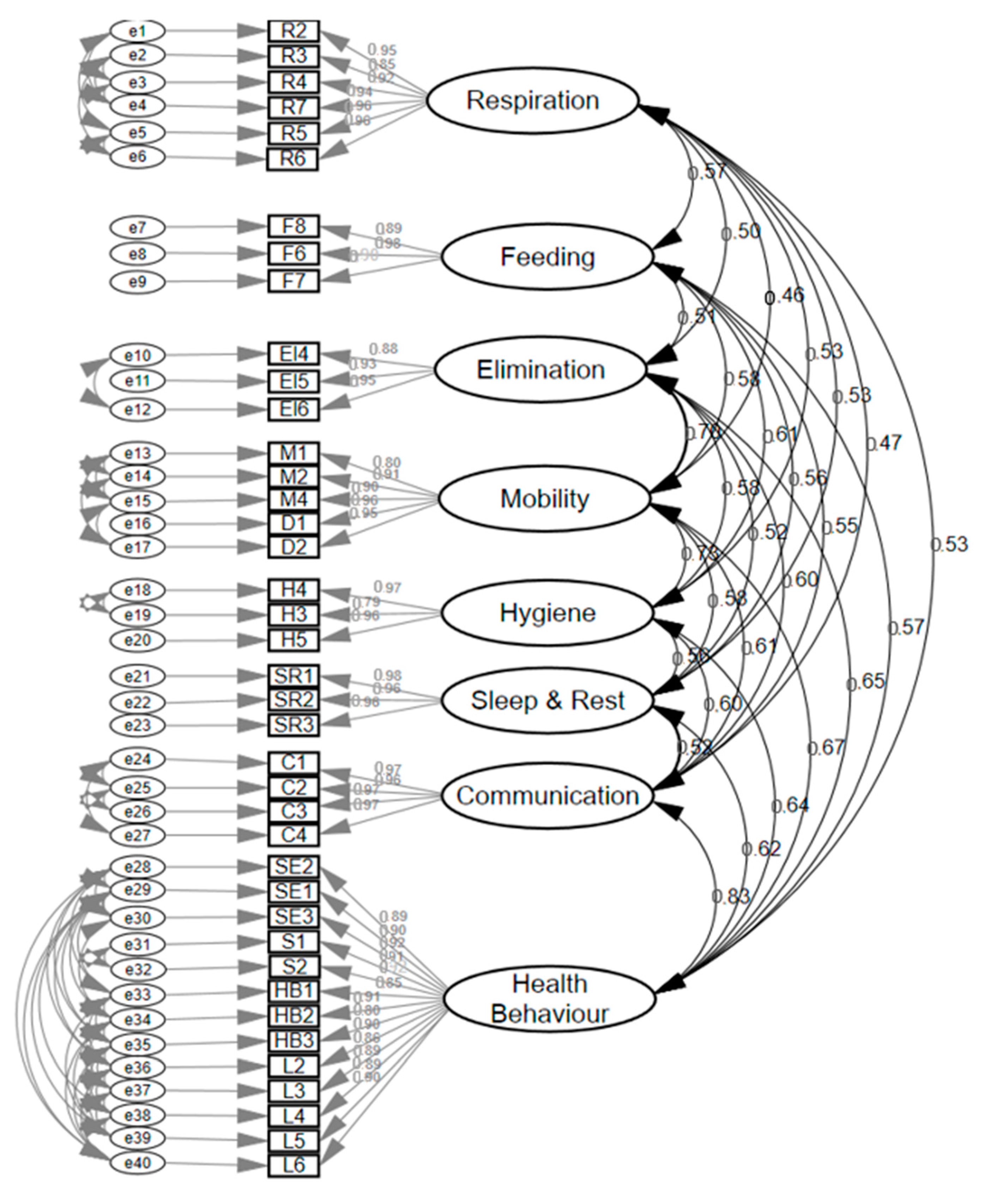
3.2.2. Sample 2 (46-Item Version Scale to 40-Item Scale)
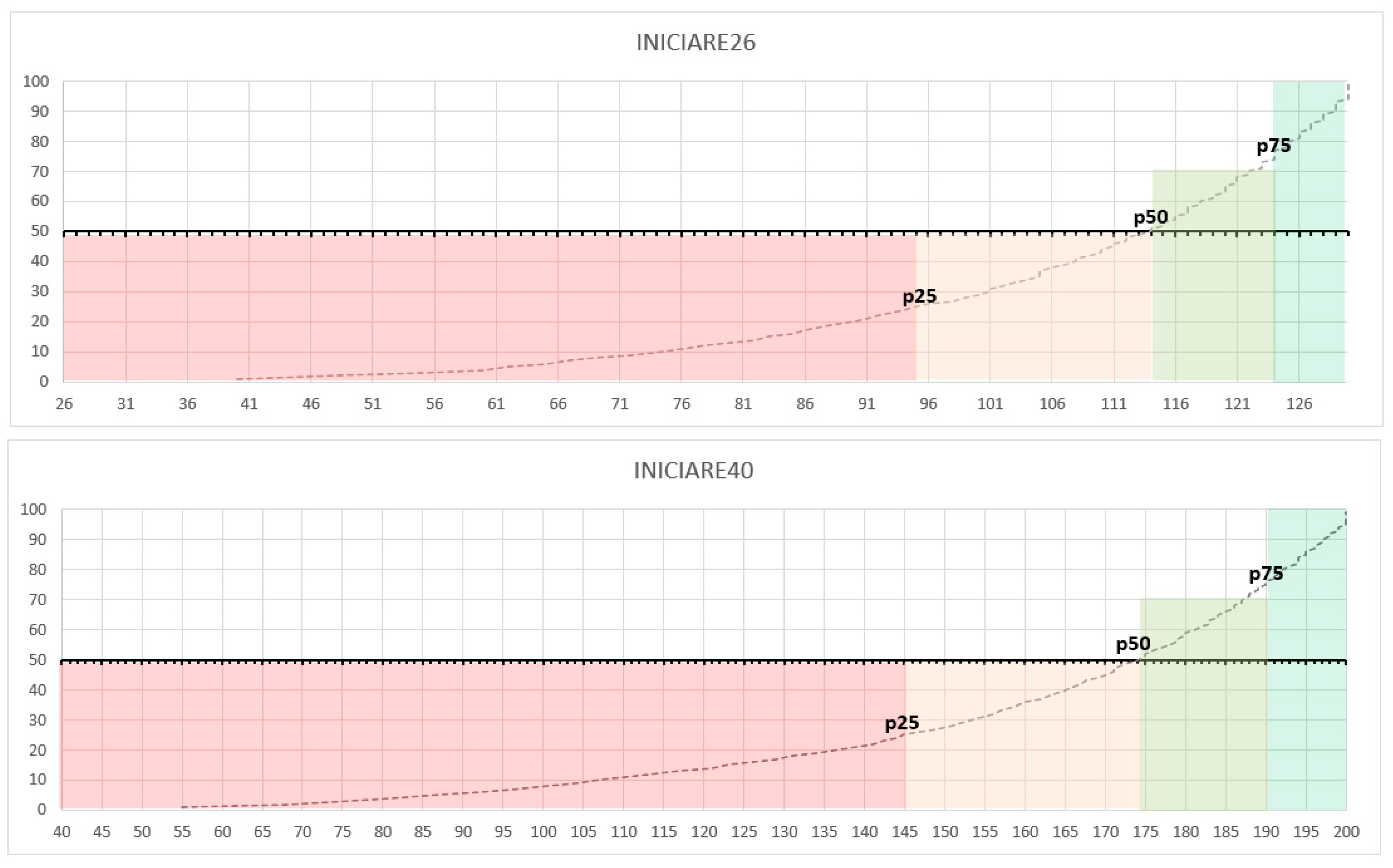
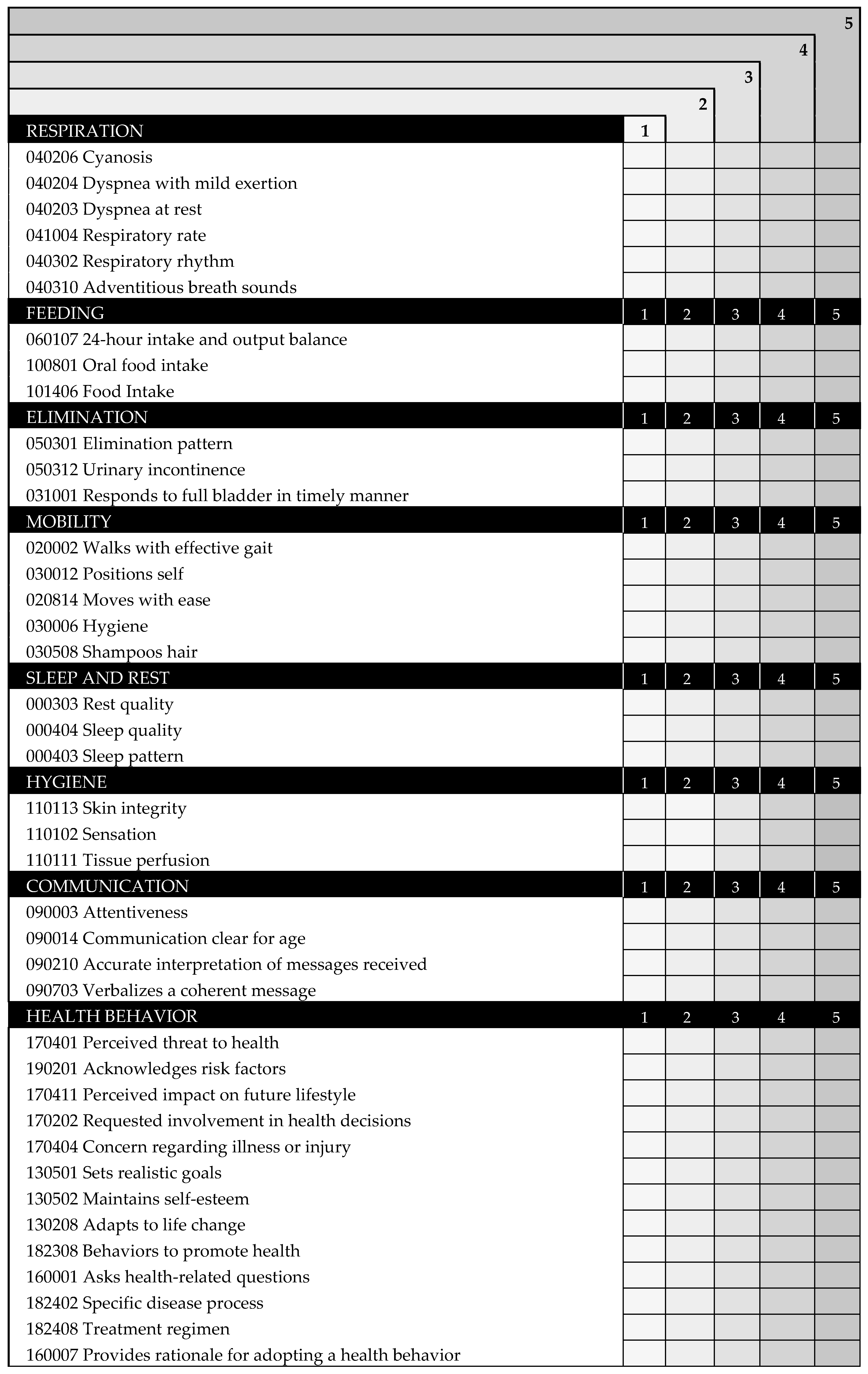
3.2.3. Sample 3 (40-Item Version Scale to 26-Item Scale)
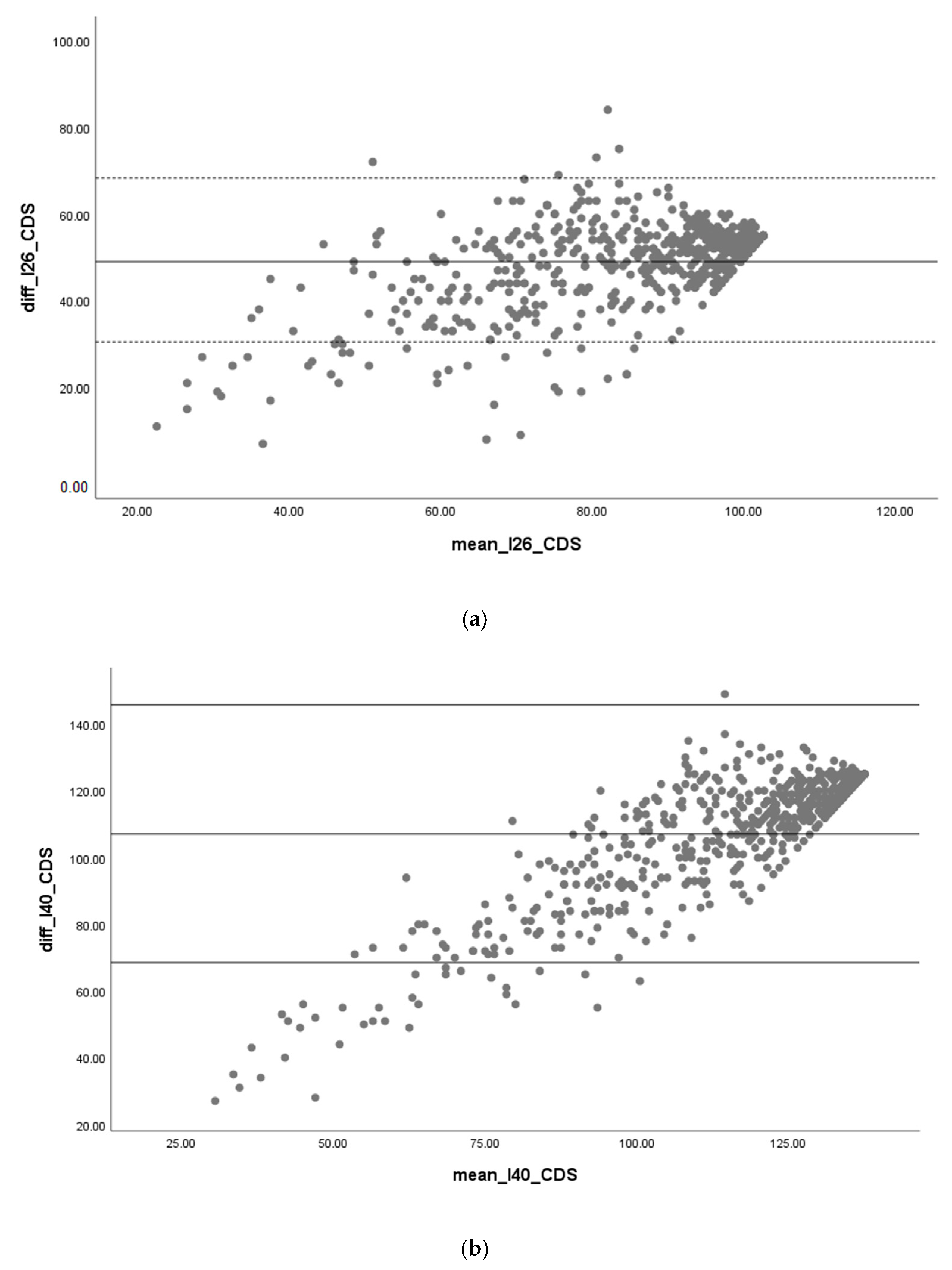
3.2.4. Large form Version (40-Item Scale) vs. Short Form Version (26-Item Scale)
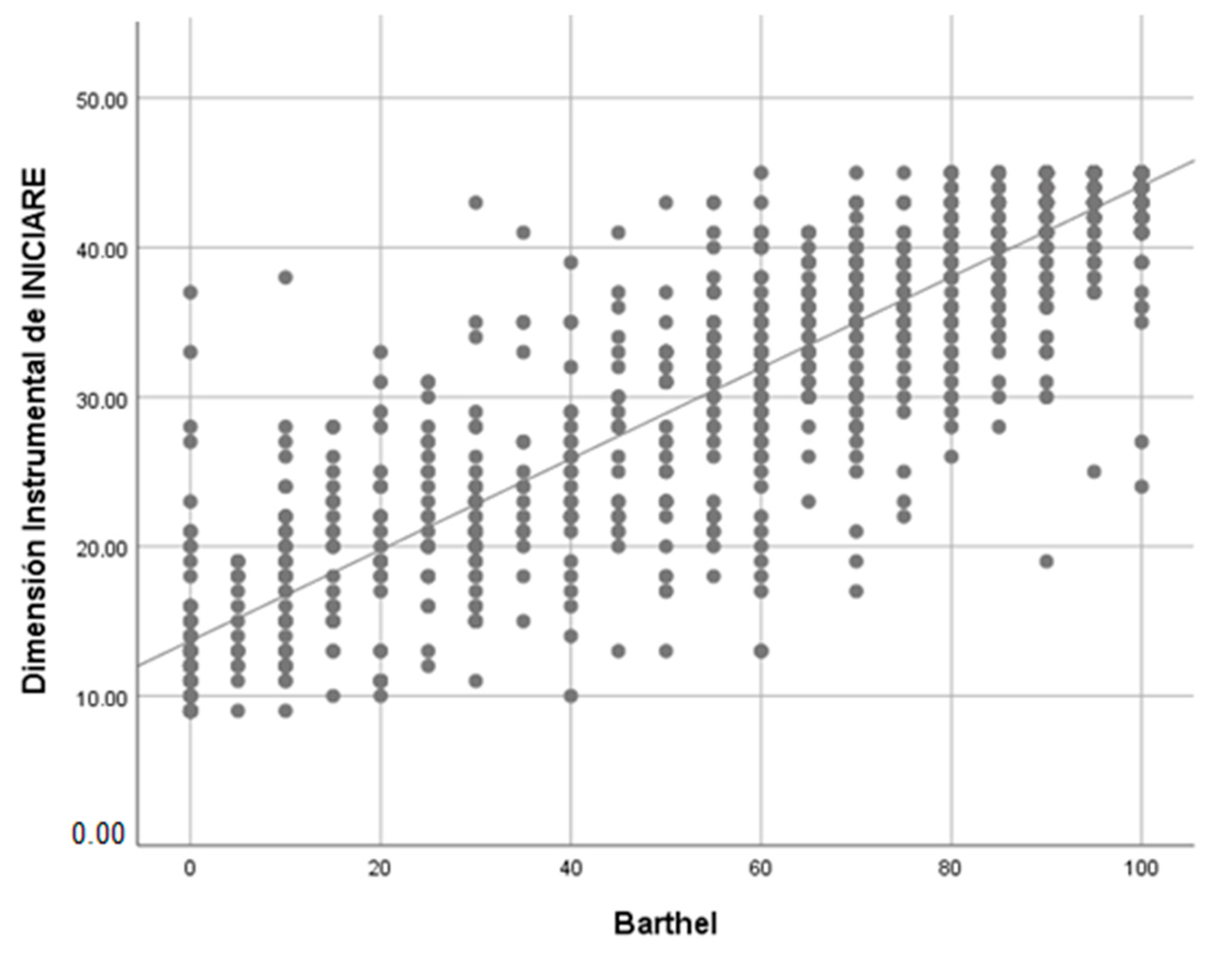
3.2.5. Concurrent Criterion Validity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Good Health Adds Life to Years. In Global Brief for World Health Day 2012; World Health Organization: Geneva, Switzerland, 2012; Volume 1, pp. 1–30. [Google Scholar]
- Viña-García, M.; Román-Medina, I. The role of the geriatric nurse specialist as a key response in the care of the elderly, chronicity, complex chronicity and its consequences on dependence. Enferm. Clín. (Engl. Ed.) 2019, 22, 380–383. [Google Scholar]
- Martins, A.; Da Silva, L.; Corrêa, L.; Rosset, I.; Peroni, C.; Partezani, R. Functional dependency of older individuals and Caregiver Burden. Rev. Esc. Enferm. USP 2013, 47, 134–141. [Google Scholar]
- Santana, M.J.; Manalili, K.; Jolley, R.J.; Zelinsky, S.; Lu, M. How to practice person-centred care: A conceptual framework. Health Expect. 2018, 21, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Morales-Asencio, J.M.; Martin-Santos, F.J.; Kaknani, S.; Morilla-Herrera, J.C.; Cuevas Fernández-Gallego, M.; García-Mayor, S.; León-Campos, A.; Morales-Gil, I.M. Living with chronicity and complexity: Lessons for redesigning case management from patients’ life stories—A qualitative study. J. Eval. Clin. Prac. 2016, 22, 122–132. [Google Scholar] [CrossRef]
- Wilson, M.G.; Lavis, J.N.; Gauvin, F.-P. Designing Integrated Approaches to Support People with Multimorbidity: Key Messages from Systematic Reviews, Health System Leaders and Citizens. Healthc. Policy Polit. Sante 2016, 12, 91–104. [Google Scholar] [CrossRef] [Green Version]
- Fasoli, D.R.; Fincke, B.G.; Haddock, K.S. Going beyond Patient Classification Systems to Create an Evidence-Based Staffing Methodology. J. Nurs. Adm. 2011, 41, 434–439. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, P.; Saville, C.; Ball, J.; Jones, J.; Pattison, N.; Monks, T. Nursing workload, nurse staffing methodologies and tools: A systematic scoping review and discussion. Int. J. Nurs. Stud. 2020, 103, 103487. [Google Scholar] [CrossRef]
- Subirana Casacuberta, M.; Solà Arnau, I. Revisión sistemática de los instrumentos que miden la actividad de Enfermería y su repercusión sobre los resultados en salud. Metas Enferm. 2006, 9, 22–27. [Google Scholar]
- Barrientos-Trigo, S. Validez Externa y Convergencia de la Escala INICIARE 2.0 y Care Dependency Scale: Estudio Multicéntrico; University of Seville: Seville, Spain, 2015. [Google Scholar]
- Dijkstra, A.; Coleman, M.; Tomas, C.; Välimäki, M.; Dassen, T. Cross-cultural psychometric testing of the Care Dependency Scale with data. J. Adv. Nurs. 2003, 43, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, A.; Yönt, G.H.; Korhan, E.A.; Muszalik, M.; Kędziora-Kornatowska, K.; Suzuki, M. The Care Dependency Scale for measuring basic human needs: An international comparison. J. Adv. Nurs. 2012, 68, 2341–2348. [Google Scholar] [CrossRef] [PubMed]
- Zürcher, S.J.; Vangelooven, C.; Borter, N.; Schnyder, D.; Hahn, S. Psychometric testing of the Italian and French versions of the Care Dependency Scale. J. Adv. Nurs. 2016, 72, 3207–3215. [Google Scholar] [CrossRef] [PubMed]
- Morales-Asencio, J.M.; Porcel-Gálvez, A.M.; Oliveros-Valenzuela, R.; Rodríguez-Gómez, S.; Sánchez-Extremera, L.; Serrano-López, F.A.; Aranda-Gallardo, M.; Canca-Sánchez, J.C.; Barrientos-Trigo, S. Design and validation of the INICIARE instrument, for the assessment of dependency level in acutely ill hospitalised patients. J. Clin. Nurs. 2015, 24, 761–777. [Google Scholar] [CrossRef] [PubMed]
- Moorhead, S.; Johnson, M.; Maas, M.L.; Swanson, E. Clasificación de Resultados de Enfermería (NOC); Elsevier: Amsterdam, The Netherlands, 2014; pp. 1–22. [Google Scholar]
- Scherb, C.A.; Head, B.J.; Hertzog, M.; Swanson, E.; Reed, D.; Maas, M.L.; Weinberg, B. Evaluation of outcome change scores for patients with pneumonia or heart failure. West. J. Nurs. Res. 2013, 35, 117–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.; Lee, E. Incorporating Standardized Nursing Languages into an Electronic Nursing Documentation System in Korea: A Pilot Study. Int. J. Nurs. Know. 2015, 26, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Ranegger, R.; Hackl, W.O.; Ammenwerth, E. Implementation of the Austrian Nursing Minimum Data Set (NMDS-AT): A Feasibility Study. BMC Med. Inform. Decis. Mak. 2015, 15, 116. [Google Scholar]
- Hoi, S.Y.; Ismail, N.; Ong, L.C.; Kang, J. Determining nurse staffing needs: The workload intensity measurement system. J. Nurs. Manag. 2010, 18, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Consejería de Igualdad, Salud y Políticas Sociales. Conjunto Mínimo Básico de Datos al Alta Hospitalaria. 2014. Available online: https://www.juntadeandalucia.es/servicios/publicaciones/detalle/65044.htm (accessed on 4 December 2014).
- Servicio Andaluz de Salud. Consejería de Salud; Servicio Andaluz de Salud: Andalucia, Spain, 2016.
- Goicoechea, J.; Díaz, A.; Jiménez, M. Conjunto Mínimo Básico de Datos al Alta Hospitalaria: Grupos Relacionados por el Diagnóstico: Andalucía 2009; Servicio Andaluz de Salud: Andalucia, Spain, 2010; Volume 312.
- Iacobucci, D.; Duhachek, A. Advancing Alpha: Measuring reliability with confidence. J. Cons. Psych. 2003, 13, 478–487. [Google Scholar] [CrossRef]
- Rouquette, A.; Falissard, B. Sample size requirements for the internal validation of psychiatric scales. Int. J. Methods Psychiatr. Res. 2011, 20, 235–249. [Google Scholar] [CrossRef] [Green Version]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psych. Meth. 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Porcel Gálvez, A.M. Construcción y Validación de un Sistema de Evaluación del Nivel de Dependencia para Pacientes Hospitalizados; University of Granada: Granada, Spain, 2011. [Google Scholar]
- IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0.; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Arbuckle, J.L. Amos (Version 23.0) [Computer Program]; IBM SPSS: Chicago, IL, USA, 2014. [Google Scholar]
- StatSoft, Inc. Electronic Statistics Textbook; StatSoft.: Tulsa, OK, USA, 2012. [Google Scholar]
- Li, C.-H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Meth. 2016, 48, 936–949. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Mod. Multi. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN Checklist Manual; University Medical Center: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Cantero-Garlito, P.A.; Flores-Martos, J.A.; Moruno-Miralles, P. Dependency and Care: Perspectives from the Point of View of Professionals Assessing Situations of Dependency in Spain. Int. J. Environ. Res. Public Health 2020, 17, 1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrientos-Trigo, S.; Gil-García, E.; Romero-Sánchez, J.M.; Badanta-Romero, B.; Porcel-Gálvez, A.M. Evaluation of psychometric properties of instruments measuring nursing-sensitive outcomes: A systematic review. Int. Nurs. Rev. 2019, 66, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Turner-Stokes, L.; Tonge, P.; Nyein, K.; Hunter, M.; Nielson, S.; Robinson, I. The Northwick Park Dependency Score (NPDS): A measure of nursing dependency in rehabilitation. Clin. Rehabil. 1998, 12, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Rauhala, A.; Fagerström, L. Determining optimal nursing intensity: The RAFAELA method. J. Adv. Nurs. 2004, 45, 351–359. [Google Scholar] [CrossRef]
- Reeves, S.; Clark, E.; Lawton, S.; Ream, M.; Ross, F. Examining the nature of interprofessional interventions designed to promote patient safety: A narrative review. Int. J. Qual. Health Care 2017, 29, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Gijon-Nogueron, G.; Montes-Alguacil, J.; Alfageme-Garcia, P.; Cervera-Marin, J.A.; Morales-Asencio, J.M.; Martinez-Nova, A. Establishing normative foot posture index values for the pediatric population: A cross-sectional study. J. Foot Ankle Res. 2016, 9, 24. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, E.; Tugwell, P.; Fries, J.F. Percentile benchmarks in patients with rheumatoid arthritis: Health Assessment Questionnaire as a quality indicator (QI). Arthritis Res. Ther. 2004, 6, R505. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.; Bredow, T. Middle Range Theories. Aplication tu Nursing Research, 2nd ed.; Lippincott Williams Wilkins: Philadelphia, PA, USA, 2009; pp. 9–12. [Google Scholar]
- Rosnay, J. Le Macroscope; Éditions du Seuil: Paris, France, 1975. [Google Scholar]
- Phaneuf, M. La Planificación de Los Cuidados Enfermeiros; McGraw Hill/Interamericana: Mexico City, Mexico, 1999. [Google Scholar]
- Da CLinch, G.F.; Rabelo-Silva, E.R.; Keenan, G.M.; Moraes, M.A.; Stifter, J.; Müller-Staub, M. Validation of the quality of diagnoses, interventions, and outcomes (Q-DIO) instrument for use in Brazil and the United States. Int. J. Nurs. Know. 2015, 26, 19–25. [Google Scholar]
- Porcel-Gálvez, A.M.; Hörner Schlindwein-Meirelles, B.; Gil-García, E.; Morales-Asencio, J.M.; Guerra-Martín, M.D. Opinions and nurse’ satisfaction with INICIARE 2.0 scale: A qualitative study in a hospital setting. Enferm. Clín. 2016, 26, 374–380. [Google Scholar]
- Porcel Gálvez, A.M.; Morales Asencio, J.; Villaverde Gutiérrez, C. Medida del nivel de dependencia en cuidados enfermeros. Preliminares de una propuesta metodológica. Scentia Rev. Mult. Cien. Salud 2008, 13, 131–135. [Google Scholar]
- Herdman, T.H.; Kamitsuru, S. NANDA International Nursing Diagnoses: Definitions and Classification 2018–2020, 11th ed.; Thieme New York: New York, NY, USA, 2017. [Google Scholar]
- Avena, M.J.; da Luz Gonçalves Pedreira, M.; Herdman, T.H.; Gutiérrez, M.G.R. Respiratory Nursing Diagnoses: Presenting Evidence for Identification of the Defining Characteristics in Neonatal and Pediatric Populations. Int. J. Nurs. Know. 2016, 27, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-López, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [Green Version]
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J. Adv. Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Johnson, M.; Moorhead, S.; Reed, D.; Sweeney, S. Evaluation of the reliability and validity of nursing outcomes classification patient outcomes and measures. J. Nurs. Meas. 2003, 11, 97–117. [Google Scholar] [CrossRef]
- Paloma-Castro, O.; Romero-Sánchez, J.M.; Paramio-Cuevas, J.C.; PastorMontero, S.M.; Sánchez-Dalda, M.C.; Rozadillas-Sanmiquel, E.; MorenoCorral, L.J. Development and psychometric evaluation of questionnaire based on the Nursing Outcomes Classification to determine the knowledge of parents on breast-feeding: Research Protocol. Int. J. Nurs. Knowl. 2015. [Google Scholar] [CrossRef] [PubMed]
- Health and Social General Department of Andalusian Government. Validation of a Nursing Resources Allocation Model, Adjusted by Levels of Dependence in Care of Hospitalized Patients Evaluated with Initiate, for the Improvement of Staff Outcomes and Reduction of Adverse Events, in the Andalusian Public Health System: Multi-Center Study Nursing_Iniciare_Patient (NIP 3.0) Study Protocol; Health and Social General Department of Andalusian Government: Seville, Spain, 2016.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patients | Clinical Nurses | ||
|---|---|---|---|---|
| Sample 1 | Sample 2 | Sample 3 | Sample | |
| n = 1901 | n = 821 | n = 883 | n = 157 | |
| n (%) or Mean (SD) | n (%) or Mean (SD) | n (%) or Mean (SD) | n (%) or Mean (SD) | |
| Age | 64.7 (17.0) | 64.5 (17.0) | 64.5 (16.9) | |
| Gender | ||||
| Male | 1022 (53.8) | 471 (57.4) | 489 (55.4) | |
| Female | 879 (46.2) | 350 (42.6) | 394 (44.6) | |
| Unit | ||||
| Medical | 1191 (62.7) | 497 (60.5) | 536 (60.7) | |
| Surgical | 710 (37.3) | 324 (39.5) | 347 (39.3) | |
| Functional and cognitive status | ||||
| Barthel Index | 54.3 (35.7) | 58.5 (36.8) | 55.9 (35.9) | |
| Pfeiffer | 1.1 (0.3) | 1.1 (0.3) | 1.1 (0.3) | |
| Hospital | ||||
| Primary | 845 (44.4) | 404 (49.2) | 412 (46.6) | 68 (43.3) |
| Specialties | 622 (32.7) | 306 (37.3) | 309 (34.9) | 65 (41.4) |
| Tertiary | 434 (22.8) | 111 (13.5) | 162 (18.3) | 24 (15.3) |
| No. | Factor | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| 1 | 160007 Provides rationale for adopting a health behaviour | 0.880 | |||||||
| 2 | 182402 Description of specific disease process | 0.874 | |||||||
| 3 | 160601 Claims decision-making responsibility | 0.873 | |||||||
| 4 | 182408 Description of treatment regimen | 0.870 | |||||||
| 5 | 182308 Behaviors to promote health | 0.858 | |||||||
| 6 | 160001 Asks health-related questions | 0.852 | |||||||
| 7 | 170202 Requested involvement in health decisions | 0.823 | |||||||
| 8 | 130501 Sets realistic goals | 0.816 | |||||||
| 9 | 130208 Adapts to life change | 0.794 | |||||||
| 10 | 170411 Perceived impact on future lifestyle | 0.777 | |||||||
| 11 | 130502 Maintains self-esteem | 0.774 | |||||||
| 12 | 170404 Concern regarding illness or injury | 0.768 | |||||||
| 13 | 190201 Acknowledges risk factors | 0.731 | |||||||
| 14 | 170401 Perceived threat to health | 0.713 | |||||||
| 15 | 040302 Respiratory rhythm | 0.883 | |||||||
| 16 | 041004 Respiratory rate | 0.871 | |||||||
| 17 | 040309 Accessory muscle use | 0.857 | |||||||
| 18 | 040310 Adventitious breath sounds | 0.844 | |||||||
| 19 | 040203 Dyspnea at rest | 0.829 | |||||||
| 20 | 040204 Dyspnea with mild exertion | 0.794 | |||||||
| 21 | 040206 Cyanosis | 0.750 | |||||||
| 22 | 030012 Positions self | 0.816 | |||||||
| 23 | 020814 Moves with ease | 0.814 | |||||||
| 24 | 020002 Walks with effective gait | 0.804 | |||||||
| 25 | 030002 Dressing | 0.802 | |||||||
| 26 | 030211 Removes clothes from upper body | 0.793 | |||||||
| 27 | 020802 Body positioning performance | 0.723 | |||||||
| 28 | 101406 Food Intake | 0.857 | |||||||
| 29 | 100801 Oral food intake | 0.837 | |||||||
| 30 | 101016 Food acceptance | 0.678 | |||||||
| 31 | 060107 24-h intake and output balance | 0.549 | |||||||
| 32 | 050301 Elimination pattern (urinary) | 0.728 | |||||||
| 33 | 050312 Urinary incontinence | 0.688 | |||||||
| 34 | 031001 Responds to full bladder in timely manner | 0.684 | |||||||
| 35 | 060211 Urine output | 0.640 | |||||||
| 36 | 050002 Maintains control of stool passage | 0.415 | |||||||
| 37 | 000404 Sleep quality | 0.842 | |||||||
| 38 | 000303 Rest quality | 0.819 | |||||||
| 39 | 000403 Sleep pattern | 0.814 | |||||||
| 40 | 110102 Sensation | 0.753 | |||||||
| 41 | 110111 Tissue perfusion | 0.722 | |||||||
| 42 | 110113 Skin integrity | 0.640 | |||||||
| 43 | 090703 Verbalizes a coherent message | 0.655 | |||||||
| 44 | 090014 Communication clear for age | 0.643 | |||||||
| 45 | 090003 Attentiveness | 0.608 | |||||||
| 46 | 090210 Accurate interpretation of messages received | 0.601 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porcel-Gálvez, A.M.; Barrientos-Trigo, S.; Fernández-García, E.; Allande-Cussó, R.; Quiñoz-Gallardo, M.D.; Morales-Asencio, J.M. Development and External Validity of a Short-Form Version of the INICIARE Scale to Classify Nursing Care Dependency Level in Acute Hospitals. Int. J. Environ. Res. Public Health 2020, 17, 8511. https://doi.org/10.3390/ijerph17228511
Porcel-Gálvez AM, Barrientos-Trigo S, Fernández-García E, Allande-Cussó R, Quiñoz-Gallardo MD, Morales-Asencio JM. Development and External Validity of a Short-Form Version of the INICIARE Scale to Classify Nursing Care Dependency Level in Acute Hospitals. International Journal of Environmental Research and Public Health. 2020; 17(22):8511. https://doi.org/10.3390/ijerph17228511
Chicago/Turabian StylePorcel-Gálvez, Ana María, Sergio Barrientos-Trigo, Elena Fernández-García, Regina Allande-Cussó, María Dolores Quiñoz-Gallardo, and José Miguel Morales-Asencio. 2020. "Development and External Validity of a Short-Form Version of the INICIARE Scale to Classify Nursing Care Dependency Level in Acute Hospitals" International Journal of Environmental Research and Public Health 17, no. 22: 8511. https://doi.org/10.3390/ijerph17228511