Effects of Virtual Reality on Cardiac Rehabilitation Programs for Ischemic Heart Disease: A Randomized Pilot Clinical Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
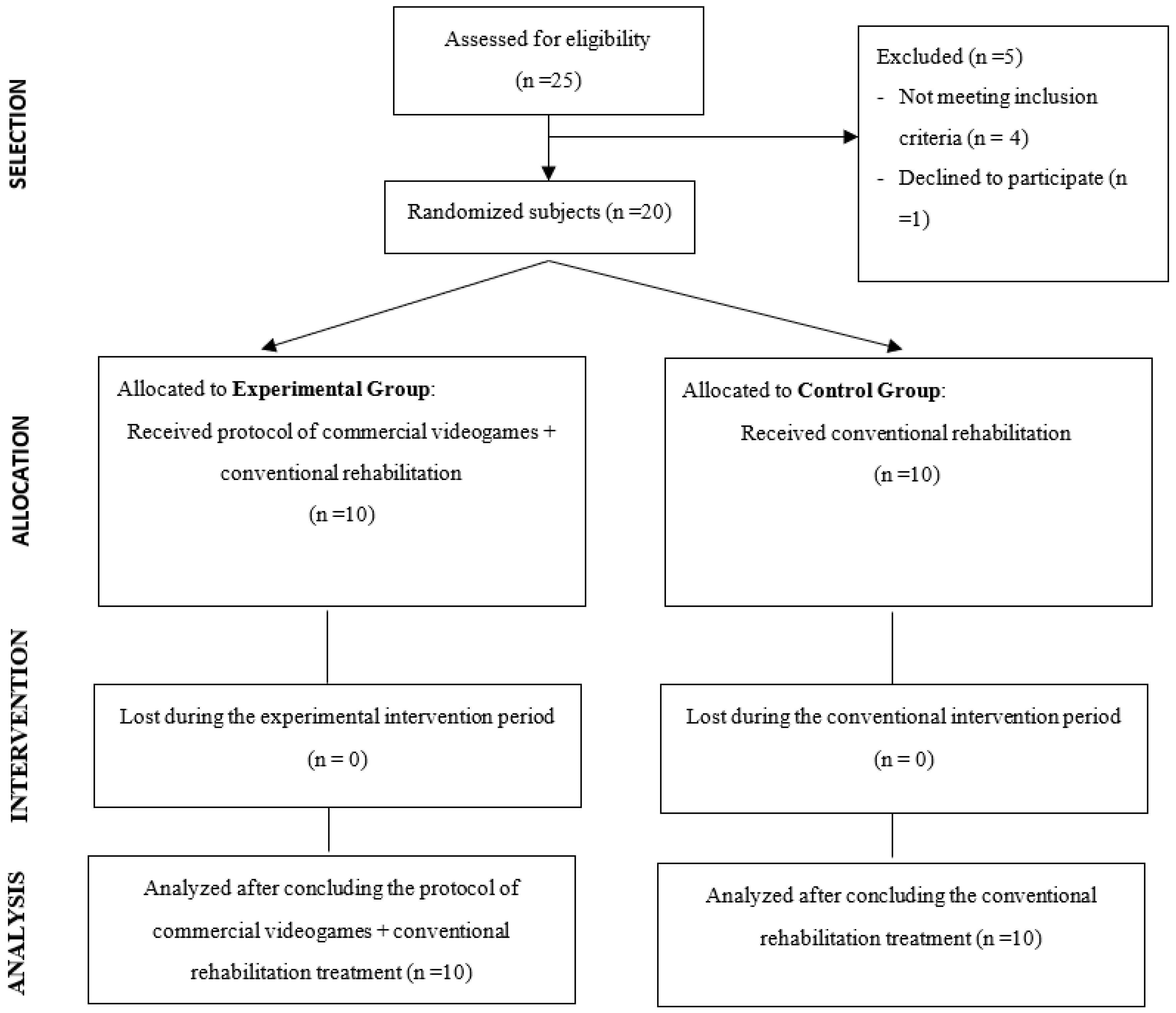
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Outcome Measures
- Ergometry. In the present study, a treadmill (Bruce protocol) was used as an ergometric test, in three-minute stages. At each stage, both the speed and slope of the treadmill increased, causing an increase in workload. Exceeding 85% maximum HR (220-Patient age) as submaximal HR (>85%) was used as a theoretical guide. The Bruce protocol has a maximum duration of 21 min, with a recovery phase of 8–10 min, until the parameters evaluated are normalized, with the first two minutes being especially important. The ergometry ended with the following assumptions: reaching 85% of the maximum HR in the presence of physical exhaustion, appearance of symptoms, perception of a certain effort on the Börg Scale or altered electrical activity in the electro-cardiogram [28]. The final HR of the ergometry, the time in minutes of the ergometry and the % complete of the ergometry (considering as conclusive >85% estimated HR) were recorded as variables.
- Metabolic Equivalents (METS). The equivalence table was used for the transformation formula from Watts to METS, in order to estimate the VO2max (1 MET equals 3.5 mL/kg/min), proposed by the Spanish Society of Cardiology [29].
- Functional Independence Measure. This is the most accepted functional evaluation measure in the field of rehabilitation. It values six functional areas: self-care, toileting, transfers, locomotion, communication and awareness of the outside world. The first four include 13 items and comprise motor function. The areas related to communication and awareness with the outside world comprise five items and refer to the cognitive sphere. The total score can vary between 7 (total dependence) and 126 (total independence) [30,31].
- 6-min walk test (6MWT). To carry out this test, a closed and marked corridor with a length equal to 30 m was available. It was carried out by going around this section, delimited by indicators on the ground. These signs were placed at a distance of 29 m from each other, leaving 0.5 m at each end for the patient to rotate. Following the international recommendations, the patient walked in the company of the examiner, carrying a portable pulse oximeter that recorded both HR and O2 saturation (% O2) every minute. Before starting this, the patient was reminded of the idea of traveling as far as possible in 6 min, being able to change the rhythm or stop if needed. The distance traveled in meters was recorded [32]. The final HR at 6MWT, the recovery HR at two minutes, the average HR, the maximum distance traveled in meters, the total number of laps, as well as the maximum HR were recorded as outcome measures.
- Short Form Health Survey-36 Questionnaire (SF-36). The SF-36 is an assessment instrument used by a larger number of authors in the assessment of health-related quality of life in patients with heart disease. It is made up of 35 scoring items, divided into 8 dimensions: Physical Function, Physical Role, Emotional Role, Social Function, Mental Health, General Health, Body Pain and Vitality. It also contains an additional item that is not part of any dimension and which measures the declared evolution of health [33,34].
- Beck-II Depression Inventory. This questionnaire was used to detect and assess the severity of depression in the sample. It is based on a self-administered questionnaire with 21 items that are answered on a four-point Likert-type scale (from 0 to 3), except for items 16 (changes in sleep pattern) and 18 (changes in appetite) which contain seven categories. The minimum and maximum scores on the test are 0 (no depression) and 63 (severe depression) [35].
- Degree of satisfaction with the treatment. The Client Satisfaction Questionnaire was used to assess satisfaction with the health service provided to both groups. This is a self-administered questionnaire, consisting of eight questions that assess the level of satisfaction in relation to the care and quality of the service received, as well as the degree of compliance with the patient’s expectations prior to the intervention. The responses are coded from 1–4, with the total score of the questionnaire being 32 points, where higher values indicate greater satisfaction with the treatment received [36].
- Additionally, the EG completed a specific questionnaire regarding treatment with VR technology and video games, designed and used by the research group based on previous research in the field of rehabilitation using technologies. The questionnaire is made up of 18 items that assess the degree of satisfaction in the following dimensions: technical quality of the equipment (four items), ease of use of video games (five items), compliance with the program and applicability (seven items) and degree of satisfaction or complacency (two items). The responses are established based on a Likert-type scale of 1–5 points, with alternative directionality of the responses to avoid stereotyped responses. Regarding the interpretation of the results, the maximum possible score is 90 points [14,15,16].
- Adherence. The percentage of attendance to both treatment modalities was registered, as well as the presence of adverse effects (such as nausea, vomiting, headache, dizziness, muscle aches or general pain) in both groups.
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Data
3.2. Intra-Group and Inter-Group Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferreira-González, I. Epidemiología de la enfermedad coronaria. Revista Española de Cardiología 2014, 67, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; De Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C. Executive summary: Heart disease and stroke statistics—2010 update: A report from the American Heart Association. Circulation 2010, 121, 948–954. [Google Scholar] [PubMed]
- Lloyd-Jones, D.M.; Larson, M.G.; Beiser, A.; Levy, D. Lifetime risk of developing coronary heart disease. Lancet 1999, 353, 89–92. [Google Scholar] [CrossRef]
- Nichols, M.; Townsend, N.; Luengo-Fernandez, R.; Leal, J.; Gray, A.; Scarborough, P.; Rayner, M. European Cardiovascular Disease Statistics 2012; European Heart Network, Brussels and European Society of Cardiology: Sophia Antipolis, France, 2012. [Google Scholar]
- Marrugat, J.; Elosua, R.; Martí, H.; Martí-Soler, H. Epidemiología de la cardiopatía isquémica en España: Estimación del número de casos y de las tendencias entre 1997 y 2005. Rev. Española Cardiol. 2002, 55, 337–346. [Google Scholar] [CrossRef]
- Olmedo-Llanes, J. Factores Relacionados Con La Mortalidad a Largo Plazo de Una Cohorte de Pacientes Que Sobreviven 28 Días Tras un IAM. Ph.D. Thesis, Facultad de Medicina, Universidad Autónoma de Madrid, Madrid, Spain, 2017. [Google Scholar]
- World Health Organization. Technical Report Series 270. Rehabilitation of Patients with Cardiovascular Diseases. Ginebra: Report of WHO Expert Committee; WHO: Geneva, Switzerland, 1964. [Google Scholar]
- Maroto, J.M.; Prados, C. Rehabilitación cardíaca. Historia. Indicaciones. Protocolos. In Rehabilitación Cardiovascular; Maroto, J.M., de Pablo, C., Eds.; Médica Panamericana: Madrid, Spain, 2011. [Google Scholar]
- Martín, J.C.; Vivas, T.M.; Pinedo, M.R.; Esteso, J.J. Rehabilitación cardíaca en el síndrome coronario agudo. Rehabilitación 2006, 40, 318–332. [Google Scholar] [CrossRef]
- Tirado, J.E.; Lozano, A.L.; Saborido, A.A.; Carmona, J.V.; Praena-Fernández, J.M.; De Vargas, C.E.R. Impacto de la adherencia a las recomendaciones de hábitos de vida cardiosaludables en la capacidad funcional a largo plazo en pacientes que han completado un programa de rehabilitación cardíaca. Rehabilitación 2017, 51, 22–29. [Google Scholar] [CrossRef]
- García-Bravo, S.; Cuesta-Gomez, A.; Campuzano-Ruiz, R.; López-Navas, M.J.; Domínguez-Paniagua, J.; Araújo-Narváez, A.; Barreñada-Copete, E.; García-Bravo, C.; Flórez-García, M.T.; Botas-Rodríguez, J.; et al. Virtual reality and video games in cardiac rehabilitation programs. A systematic review. Disabil. Rehabil. 2019, 30, 1–10. [Google Scholar] [CrossRef]
- Manetta, C.; Blade, R.A. Glossary of Virtual Reality Terminology. Int. J. Virtual Real. Multimed. Publ. Prof. 1995, 1, 35–39. [Google Scholar] [CrossRef]
- Ortiz-Gutiérrez, R.M.; Bermejo, A.; Cano-de la Cuerda, R. Realidad virtual en neurorrehabilitación. In Nuevas Tecnologías en Neurorrehabilitación. Aplicaciones Diagnósticas y Terapéuticas; Cano-de la Cuerda, R., Ed.; Panamericana: Madrid, Spain, 2018. [Google Scholar]
- Ortiz-Gutiérrez, R.; Del Río, F.G.; De La Cuerda, R.C.; Alguacil-Diego, I.M.; González, R.A.; Page, J.C.M. A telerehabilitation program by virtual reality-video games improves balance and postural control in multiple sclerosis patients. Neurorehabilitation 2013, 33, 545–554. [Google Scholar] [CrossRef]
- Luna-Oliva, L.; Ortiz-Gutiérrez, R.; La Cuerda, R.C.-D.; Piédrola, R.M.; Alguacil-Diego, I.M.; Sánchez-Camarero, C.; Culebras, M.D.C.M. Kinect Xbox 360 as a therapeutic modality for children with cerebral palsy in a school environment: A preliminary study. Neurorehabilitation 2013, 33, 513–521. [Google Scholar] [CrossRef]
- Ortiz-Gutiérrez, R.; Cano-De-La-Cuerda, R.; Galán-Del-Río, F.; Alguacil-Diego, I.M.; Palacios-Ceña, D.; Miangolarra-Page, J.C. A Telerehabilitation Program Improves Postural Control in Multiple Sclerosis Patients: A Spanish Preliminary Study. Int. J. Environ. Res. Public Health 2013, 10, 5697–5710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira, Á.; Gabriel, J.; Melo, C.; Machado, J. Kinect system in home-based cardiovascular rehabilitation. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 231, 40–47. [Google Scholar] [CrossRef]
- Vieira, Á.; Melo, C.; Machado, J.; Gabriel, J. Virtual reality exercise on a home-based phase III cardiac rehabilitation program, effect on executive function, quality of life and depression, anxiety and stress: A randomized controlled trial. Disabil. Rehabil. Assist. Technol. 2017, 13, 112–123. [Google Scholar] [CrossRef]
- Cacau, L.P.D.A.; Oliveira, G.U.; Maynard, L.G.; Filho, A.A.D.A.; Júnior, W.M.D.S.; Neto, M.L.C.; Antoniolli, Â.R.; Santana-Filho, V.J. The use of the virtual reality as intervention tool in the postoperative of cardiac surgery. Braz. J. Cardiovasc. Surg. 2013, 28, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Ruivo, J.M.; Karim, K.; O’Shea, R.; Oliveira, R.C.; Keary, L.; O’Brien, C.; Gormley, J.P. In-class active videogame supplementation and adherence to cardiac rehabilitation: A pilot randomized controlled study. Eur. J. Prev. Cardiol. 2015, 22, S90. [Google Scholar]
- Klompstra, L.; Jaarsma, T.; Stromberg, A. Exergaming to increase the exercise capacity and daily physical activity in heart failure patients: A pilot study. BMC Geriatr. 2014, 14, 119. [Google Scholar] [CrossRef] [Green Version]
- Blanc, P.; Freyssin, C.; Rivière, F.; Mourot, L.; Benaich, P.; Boussuges, A.; Maunier, S. 264 Effect of the Wii sport boxing video game on the heart rate in cardiac rehabilitation patients. Arch. Cardiovasc. Dis. Suppl. 2011, 3, 87. [Google Scholar] [CrossRef] [Green Version]
- Vieira, A.S.D.S.; De Melo, M.C.D.A.; Noites, S.P.A.R.S.; Machado, J.P.; Gabriel, M.M.J. The effect of virtual reality on a home-based cardiac rehabilitation program on body composition, lipid profile and eating patterns: A randomized controlled trial. Eur. J. Integr. Med. 2017, 9, 69–78. [Google Scholar] [CrossRef]
- Jaarsma, T.; Klompstra, L.; Ben Gal, T.; Boyne, J.; Vellone, E.; Bäck, M.; Dickstein, K.; Fridlund, B.; Hoes, A.; Piepoli, M.F.; et al. Increasing exercise capacity and quality of life of patients with heart failure through Wii gaming: The rationale, design and methodology of the HF-Wii study; A multicentre randomized controlled trial. Eur. J. Heart Fail. 2015, 17, 743–748. [Google Scholar] [CrossRef]
- Ruivo, J.M.A.D.S.; Karim, K.; O’shea, R.; Oliveira, R.C.S.; Keary, L.; O’brien, C.; Gormley, J.P. In-class Active Video Game Supplementation and Adherence to Cardiac Rehabilitation. J. Cardiopulm. Rehabilit. Prev. 2017, 37, 274–278. [Google Scholar] [CrossRef]
- Serber, E.R.; Ciccolo, J.; Palmer, K.; Cobb, V.; Tilkemeier, P.L.; Bock, B.C. The feasibility of exercise videogames for cardiovascular risk reduction among adults: A pilot for “Wii heart fitness”. J. Sports Med. Phys. Fit. 2015, 56, 319–327. [Google Scholar]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.M.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muela-de Lara, A. Pruebas de esfuerzo. In Rehabilitación Cardiaca; Maroto-Montero, J.M., De Pablo-Zarazosa, C., Artigao-Ramírez, R., Morales-Durán, M.D., Eds.; Hurope SL: Barcelona, Spain, 1999; pp. 127–156. [Google Scholar]
- Arós, F.; Boraita, A.; Alegría, E.; Alonso, Á.M.; Bardají, A.; Lamiel, R.; Luengo, E.; Rabadán, M.; Alijarde, M.; Aznar, J.; et al. Guías de práctica clínica de la Sociedad Española de Cardiología en pruebas de esfuerzo. Rev. Española Cardiol. 2000, 53, 1063–1094. [Google Scholar] [CrossRef]
- Baldry Currents, J.A.; Coats, T.J. The timing of disability mesurements following injury. Injury 2000, 31, 93–98. [Google Scholar] [CrossRef]
- Currens, J.A.B. Evaluation of disability and handicap following injury. Injury 2000, 31, 99–106. [Google Scholar] [CrossRef]
- Sociedad Española de neumología y cirugía torácica. Manual SEPAR de Procedimientos. Módulo 4. Procedimientos de evaluación de la Función Pulmonar II; Publicaciones Permayer: Madrid, España, 2004. [Google Scholar]
- Ware, J.; Snow, K.; Kosinski, M.; Gandek, B. SF-36 Health Survey: Manual and Interpretation Guide; The Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Steer, R.A.; Ball, R.; Ranieri, W.F.; Beck, A.T. Dimensions of the Beck depression inventory-II in clinically depressed outpatients. J. Clin. Psychol. 1999, 55, 117–128. [Google Scholar] [CrossRef]
- Roberts, R.E.; Atrkisson, C.C.; Mendias, R.M. Assessing the Client Satisfaction Questionnaire in English and Spanish. Hisp. J. Behav. Sci. 1984, 6, 385–396. [Google Scholar] [CrossRef]
- De Pablo-Zarzosa, C.; Maroto-Montero, J.M.; Arribas, J.M. Prevención y rehabilitación de la enfermedad cardiovascular: Papel de la asistencia primaria. Rev. Española Cardiol. Supl. 2011, 11, 23–29. [Google Scholar] [CrossRef]
- Palanca-Sánchez, I.; Castro-Beiras, A.; Macaya-Miguel, C.; Elola-Somoza, J.; Bernal-Sobrino, J.L.; Paniagua-Caparrós, J.L. Unidades asistenciales del área del corazón: Estándares y recomendaciones; Ministerio de Sanidad, Política Social e Igualdad: Madrid, Spain, 2011.
- Bond, S.; Laddu, D.R.; Ozemek, C.; Lavie, C.J.; Arena, R. Exergaming and Virtual Reality for Health: Implications for Cardiac Rehabilitation. Curr. Probl. Cardiol. 2019, 12, 100472. [Google Scholar] [CrossRef]
- Ruivo, J.A. Exergames and Cardiac Rehabilitation. J. Cardiopulm. Rehabil. Prev. 2014, 34, 2–20. [Google Scholar] [CrossRef] [PubMed]
- Da Cruz, M.M.A.; Ricci-Vitor, A.L.; Borges, G.L.B.; Da Silva, P.F.; Ribeiro, F.; Vanderlei, L.C.M. Acute Hemodynamic Effects of Virtual Reality–Based Therapy in Patients of Cardiovascular Rehabilitation: A Cluster Randomized Crossover Trial. Arch. Phys. Med. Rehabil. 2020, 101, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Chaddha, A.; Jackson, E.A.; Richardson, C.R.; Franklin, B.A. Technology to Help Promote Physical Activity. Am. J. Cardiol. 2017, 119, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Bosch, P.R.; Poloni, J.; Thornton, A.; Lynskey, J.V. The Heart Rate Response to Nintendo Wii Boxing in Young Adults. Cardiopulm. Phys. Ther. J. 2012, 23, 13–18. [Google Scholar] [CrossRef]
- Fung, V.; So, K.; Park, E.; Ho, A.; Shaffer, J.; Chan, E.; Gomez, M. The Utility of a Video Game System in Rehabilitation of Burn and Nonburn Patients: A Survey among Occupational Therapy and Physiotherapy Practitioners. J. Burn. Care Res. 2010, 31, 768–775. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1 and 2 weeks | 120″ relative rest |
| Slalom of extensions (4:00′) | |
| 180″ relative rest | |
| Squats to the moon (1:30′) | |
| 180″ relative rest | |
| Slalom of extensions (4:00′) | |
| 150″ relative rest | |
| 3 and 4 weeks | Slalom of extensions (4:00′) |
| 150″ relative rest | |
| Squats to the moon (1:30′) | |
| 120″ relative rest | |
| Acrobatic Race (1:30′) | |
| 150″ relative rest | |
| Slalom of extensions (4:00′) | |
| 120″ relative rest | |
| 5 and 6 weeks | Slalom of extensions (4:00′) |
| 90″ relative rest | |
| Squats to the moon (1:30′) | |
| 90″ relative rest | |
| Snowstorm (4:00′) | |
| 120″ relative rest | |
| Slalom extensions (4:00′) | |
| 60″ relative rest | |
| 7 and 8 weeks | Slalom of extensions (4:00′) |
| 60″ relative rest | |
| Fight stomp (4:00′) | |
| 60″ relative rest | |
| Acrobatic Race (1:30′) | |
| 60″ relative rest | |
| Squats to the moon (1:30′) | |
| 60″ relative rest | |
| Slalom of extensions (4:00′) | |
| 60″ relative rest |
| Variable | Experimental Group | |||
|---|---|---|---|---|
| Pre | Post | Intra-Group Analysis p Value | Cohen’s d | |
| Median (Interquartile Range) | ||||
| Final HR ergometry | 138.00 (35.00) | 155.00 (42.00) | 0.028 * | 0.714 |
| Ergometry minutes | 9.00 (2.66) | 11.11 (2.98) | 0.049 * | 0.664 |
| % ergometry | 82.00 (14.00) | 92.00 (18.50) | 0.021 * | 0.746 |
| METS | 10.00 (3.00) | 13.30 (4.00) | 0.050 * | 0.714 |
| FIM | 126.00 (0) | 126.00 (0) | 1.000 | 0 |
| Final 6MWT FC | 89.00 (17.50) | 92.00 (29.50) | 0.028 * | 0.495 |
| 6MWT FC recovery | 72.00 (17.00) | 66.00 (24.50) | 1.000 | 0.013 |
| 6MWT FC average | 89.00 (20.50) | 88.00 (27.50) | 0.125 | 0.391 |
| 6MWT distance | 457.80 (132.00) | 513.00 (117.00) | 0.005 * | 0.837 |
| 6MWT number of laps | 7.63 (2.20) | 8.55 (1.95) | 0.005 * | 0.837 |
| 6MWT maximum FC | 174.00 (8.00) | 174.00 (8.00) | 0.157 | 0.048 |
| SF-36. Physical Function | 90.00 (17.50) | 100.00 (15.00) | 0.104 | 0.596 |
| SF3-6. Physical role | 100.00 (62.50) | 100.00 (50.00) | 0.157 | 0.205 |
| SF-36. Body ache | 72.00 (17.00) | 84.00 (54.00) | 0.498 | 0.035 |
| SF-36. General health | 72.00 (20.00) | 77.00 (21.50) | 0.049 * | 0.498 |
| SF-36. Vitality | 65.00 (32.50) | 80.00 (37.50) | 0.011 * | 0.618 |
| SF-36. Social function | 63.00 (50.50) | 100.00 (18.75) | 0.010 * | 0.841 |
| SF-36. Emotional role | 67.00 (83.50) | 100.00 (66.70) | 0.680 | 0.371 |
| SF-36. Mental health | 56.00 (44.00) | 84.00 (46.00) | 0.196 | 0.413 |
| SF-36. Declared evolution of health | 4.00 (2.00) | 3.00 (3.00) | 0.024 * | 0.721 |
| Beck-II Depression Inventory | 12 (27.00) | 11.00 (30.00) | 0.012 * | 2.158 |
| Variable | Control Group | |||
|---|---|---|---|---|
| Pre | Post | Intra-Group Analysis p Value | Cohen’s d | |
| Median (Interquartile Range) | ||||
| Final HR ergometry | 143.00 (12.75) | 144.00 (11.75) | 0.813 | 0.163 |
| Ergometry minutes | 9.46 (2.89) | 9.83 (3.11) | 0.017 * | 0.607 |
| % ergometry | 86.00 (7.00) | 86.50 (5.00) | 0.858 | 0.043 |
| METS | 11.50 (3.00) | 12.65 (3.23) | 0.008 * | 0.574 |
| FIM | 126.00 (0) | 126.00 (0) | 1.000 | 0 |
| Final 6MWT FC | 92.00 (15.50) | 96.00 (13.50) | 0.059 | 0.772 |
| 6MWT FC recovery | 67.00 (15.50) | 71.00 (16.75) | 0.241 | 0.508 |
| 6MWT FC average | 89.00 (14.25) | 91.50 (12.00) | 0.078 | 0.778 |
| 6MWT distance | 462,30 (65.40) | 557,40 (70.35) | 0.005 * | 0.757 |
| 6MWT number of laps | 7.70 (1.09) | 9.29 (1.17) | 0.005 * | 0.316 |
| 6MWT maximum FC | 167,50 (16.25) | 167.00 (17.00) | 0.180 | 0.438 |
| SF-36. Physical Function | 85.00 (22.50) | 95.00 (5.00) | 0.026 * | 0.787 |
| SF3-6. Physical role | 100.00 (100.00) | 100.00 (25.00) | 0.066 | 0.642 |
| SF-36. Body ache | 80.00 (28.00) | 100.00 (27.00) | 0.036 * | 0.640 |
| SF-36. General health | 62.00 (33.50) | 77.00 (40.00) | 0.259 | 0.477 |
| SF-36. Vitality | 70.00 (50.00) | 75.00 (27.50) | 0.106 | 0.661 |
| SF-36. Social function | 100.00 (43.50) | 100.00 (12.25) | 0.115 | 0.659 |
| SF-36. Emotional role | 100.00 (50.00) | 100.00 (50.00) | 1.000 | 0.033 |
| SF-36. Mental health | 72.00 (42.00) | 88.00 (18.00) | 0.075 | 0.680 |
| SF-36. Declared evolution of health | 3.00 (2.00) | 2.00 (1.50) | 0.132 | 0.675 |
| Beck-II Depression Inventory | 7.00 (8.00) | 3.00 (7.00) | 0.123 | 0.638 |
| Variable | Experimental Group | Control Group | Experimental Group vs. Control Group | |||||
|---|---|---|---|---|---|---|---|---|
| Median (Interquartile Range) | Mean Difference | Median (Interquartile Range) | Mean Difference | |||||
| Pre | Post | Pre | Post | Pre p Value | Post p Value | |||
| Final HR ergometry | 138.00 (35.00) | 155.00 (42.00) | 12.80 | 143.00 (12.75) | 144.00 (11.75) | −1.30 | 0.307 | 0.225 |
| Ergometry minutes | 9.00 (2.66) | 11.11 (2.98) | 1.73 | 9.46 (2.89) | 9.83 (3.11) | 0.99 | 0.880 | 0.364 |
| % ergometry | 82.00 (14.00) | 92.00 (18.50) | 7.30 | 86.00 (7.00) | 86.50 (5.00) | 1.30 | 0.288 | 0.570 |
| METS | 10.00 (3.00) | 13.30 (4.00) | 2.06 | 11.50 (3.00) | 12.65 (3.23) | 1.11 | 0.692 | 0.401 |
| FIM | 126.00 (0) | 126.00 (0) | 0.00 | 126.00 (0) | 126.00 (0) | 0.00 | 0.317 | 0.317 |
| Final 6MWT FC | 89.00 (17.50) | 92.00 (29.50) | 5.70 | 92.00 (15.50) | 96.00 (13.50) | 6.80 | 0.910 | 0.472 |
| 6MWT FC recovery | 72.00 (17.00) | 66.00 (24.50) | 0.40 | 67.00 (15.50) | 71.00 (16.75) | 3.70 | 0.405 | 0.667 |
| 6MWT FC average | 89.00 (20.50) | 88.00 (27.50) | 3.90 | 89.00 (14.25) | 91.50 (12.00) | 6.30 | 0.520 | 0.725 |
| 6MWT distance | 457.80 (132.00) | 513.00 (117.00) | 76.50 | 462.30 (65.40) | 557.40 (70.35) | 97.20 | 0.623 | 0.970 |
| 6MWT number of laps | 7.63 (2.20) | 8.55 (1.95) | 1.27 | 7.70 (1.09) | 9.29 (1.17) | 1.62 | 0.623 | 0.970 |
| 6MWT maximum FC | 174.00 (8.00) | 174.00 (8.00) | −0.20 | 167.50 (16.25) | 167.00 (17.00) | −0.30 | 0.289 | 0.307 |
| SF-36. Physical Function | 90.00 (17.50) | 100.00 (15.00) | 7.77 | 85.00 (22.50) | 95.00 (5.00) | 12.77 | 0.823 | 0.925 |
| SF3-6. Physical role | 100.00 (62.50) | 100.00 (50.00) | 5.55 | 100.00 (100.00) | 100.00 (25.00) | 22.22 | 0.844 | 0.576 |
| SF-36. Body ache | 72.00 (17.00) | 84.00 (54.00) | 2.44 | 80.00 (28.00) | 100.00 (27.00) | 18.33 | 0.964 | 0.227 |
| SF-36. General health | 72.00 (20.00) | 77.00 (21.50) | 8.66 | 62.00 (33.50) | 77.00 (40.00) | 7.55 | 0.755 | 0.658 |
| SF-36. Vitality | 65.00 (32.50) | 80.00 (37.50) | 11.11 | 70.00 (50.00) | 75.00 (27.50) | 12.77 | 0.790 | 0.374 |
| SF-36. Social function | 63.00 (50.50) | 100.00 (18.75) | 27.83 | 100.00 (43.50) | 100.00 (12.25) | 12.61 | 0.096 | 0.599 |
| SF-36. Emotional role | 67.00 (83.50) | 100.00 (66.70) | 11.06 | 100.00 (50.00) | 100.00 (50.00) | 0.00 | 0.288 | 0.693 |
| SF-36. Mental health | 56.00 (44.00) | 84.00 (46.00) | 6.66 | 72.00 (42.00) | 88.00 (18.00) | 11.11 | 0.155 | 0.105 |
| SF-36. Declared evolution of health | 4.00 (2.00) | 3.00 (3.00) | −1.00 | 3.00 (2.00) | 2.00 (1.50) | −0.66 | 0.135 | 0.455 |
| Beck-II Depression Inventory | 12 (27.00) | 11.00 (30.00) | 8.55 | 7.00 (8.00) | 3.00 (7.00) | 3.55 | 0.084 | 0.424 |
| CSQ-8 | 32.00 (0.25) | 32.00 (1.50) | 0.551 | |||||
| Variable | Experimental Group | Control Group |
|---|---|---|
| 1. Quality of service | 3.9 (0.31) | 3.8 (0.42) |
| 2. Type of service | 3.9 (0.31) | 3.70 (0.48) |
| 3. Needs covered | 4 (0) | 3.80 (0.63) |
| 4. Would you recommend to a friend | 4 (0) | 3.8 (0.42) |
| 5. Amount of aid | 4 (0) | 3.90 (0.31) |
| 6. Solve problems | 3.8 (.42) | 3.90 (0.31) |
| 7. General satisfaction | 4 (0) | 3.90 (0.31) |
| 8. Would you go back again | 4 (0) | 3.90 (0.31) |
| Total score | 31.60 (0.96) | 30.70 (2.86) |
| Variable | Experimental Group |
|---|---|
| 1. Accessibility | 4.80 (0.42) |
| 2. Ease of handling | 4.60 (0.69) |
| 3. Fun | 4.30 (0.82) |
| 4. Graphics and music | 4.20 (0.78) |
| 5. Duration of the program | 4.50 (0.70) |
| 6. Duration of the program | 4.30 (0.94) |
| 7. Understanding | 4.60 (0.69) |
| 8. Objective-result | 4.60 (0.51) |
| 9. Progression difficulty | 4.60 (0.51) |
| 10. Total number of sessions | 4.70 (0.67) |
| 11. Availability | 4.60 (0.69) |
| 12. Attention received | 4.90 (0.31) |
| 13. Clarity in explanations | 5.00 (0) |
| 14. Personalized attention | 4.90 (0.31) |
| 15. Possibility to objectify results | 4.50 (0.70) |
| 16. Possibility of transferring games to activities of daily life | 4.30 (0.82) |
| 17. Compliance with expectations | 4.40 (0.84) |
| 18. General satisfaction | 4.70 (0.48) |
| Total score | 82.50 (8.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Bravo, S.; Cano-de-la-Cuerda, R.; Domínguez-Paniagua, J.; Campuzano-Ruiz, R.; Barreñada-Copete, E.; López-Navas, M.J.; Araujo-Narváez, A.; García-Bravo, C.; Florez-Garcia, M.; Botas-Rodríguez, J.; et al. Effects of Virtual Reality on Cardiac Rehabilitation Programs for Ischemic Heart Disease: A Randomized Pilot Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 8472. https://doi.org/10.3390/ijerph17228472
García-Bravo S, Cano-de-la-Cuerda R, Domínguez-Paniagua J, Campuzano-Ruiz R, Barreñada-Copete E, López-Navas MJ, Araujo-Narváez A, García-Bravo C, Florez-Garcia M, Botas-Rodríguez J, et al. Effects of Virtual Reality on Cardiac Rehabilitation Programs for Ischemic Heart Disease: A Randomized Pilot Clinical Trial. International Journal of Environmental Research and Public Health. 2020; 17(22):8472. https://doi.org/10.3390/ijerph17228472
Chicago/Turabian StyleGarcía-Bravo, Sara, Roberto Cano-de-la-Cuerda, Joaquín Domínguez-Paniagua, Raquel Campuzano-Ruiz, Estrella Barreñada-Copete, María Jesús López-Navas, Aurora Araujo-Narváez, Cristina García-Bravo, Mariano Florez-Garcia, Javier Botas-Rodríguez, and et al. 2020. "Effects of Virtual Reality on Cardiac Rehabilitation Programs for Ischemic Heart Disease: A Randomized Pilot Clinical Trial" International Journal of Environmental Research and Public Health 17, no. 22: 8472. https://doi.org/10.3390/ijerph17228472