Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial



Abstract
:1. Introduction
2. Materials and Methods
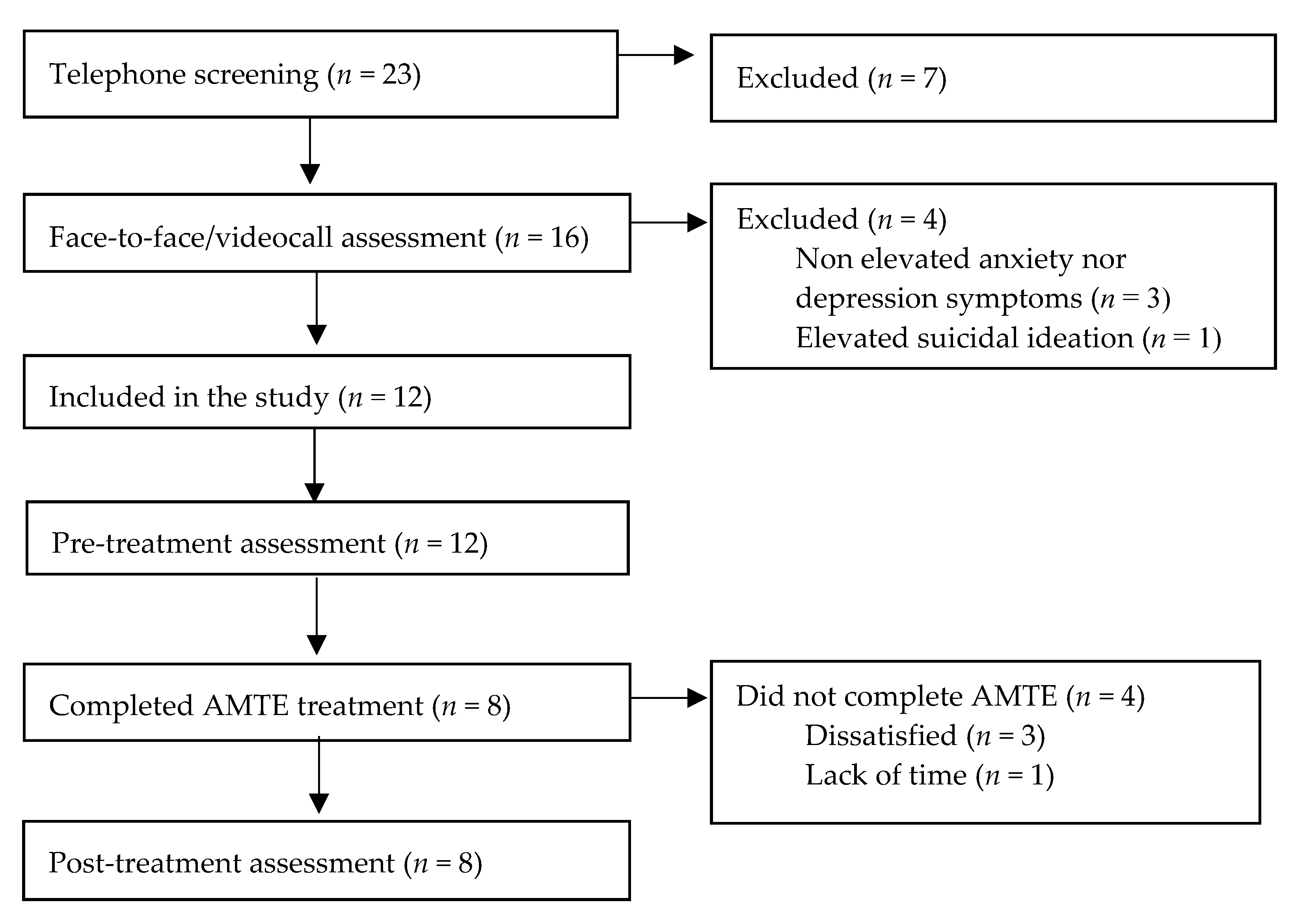
2.1. Participants
2.2. Procedure and Design
2.3. Intervention
2.4. Instruments
2.5. Statistical Analysis
3. Results
3.1. Intervention Effects
3.2. Feasibility and Acceptability
3.2.1. Adolescent Report
3.2.2. Parents Report
4. Discussion
5. Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatry. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef]
- Ahlen, J.; Lenhard, F.; Ghaderi, A. Universal prevention for anxiety and depressive symptoms in children: A meta-analysis of randomized and cluster-randomized trials. J. Prim. Prev. 2015, 36, 387–403. [Google Scholar] [CrossRef]
- Balázs, J.; Miklósi, M.; Keresztény, Á.; Hoven, C.W.; Carli, V.; Wasserman, C.; Apter, A.; Bobes, J.; Brunner, R.; Cosman, D. Adolescent subthreshold-depression and anxiety: Psychopathology, functional impairment and increased suicide risk. J. Child. Psychol. Psychiatry 2013, 54, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Weersing, V.R.; Gonzalez, A.; Campo, J.V.; Lucas, A.N. Brief behavioral therapy for pediatric anxiety and depression: Piloting an integrated treatment approach. Cogn. Behav. Pract. 2008, 15, 126–139. [Google Scholar] [CrossRef]
- Ehrenreich-May, J.; Bilek, E.L.; Queen, A.H.; Hernandez Rodriguez, J. A unified protocol for the group treatment of childhood anxiety and depression. Rev. Psicopatol. Psicol. Clin. 2012, 17, 219–236. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Valiente, R.M. Psicopatología de la ansiedad y trastornos de ansiedad: Hacia un enfoque transdiagnóstico [Psychopathology of anxiety and the anxiety disorders: Towards a transdignostic perspective]. In Manual de Psicopatología, 3rd ed.; Belloch, A., Sandín, B., Ramos, F., Eds.; McGraw-Hill: Madrid, Spain, 2020; Volume 2, pp. 3–34. [Google Scholar]
- Sandín, B.; Chorot, P.; Valiente, R.M. Transdiagnóstico: Nueva frontera en psicología clínica [Transdiagnostic: A new frontier in clinical psychology]. Rev. Psicopatol. Psicol. Clin. 2012, 17, 185–203. [Google Scholar] [CrossRef] [Green Version]
- Andersen, P.; Toner, P.; Bland, M.; McMillan, D. Effectiveness of transdiagnostic cognitive behaviour therapy for anxiety and depression in adults: A systematic review and meta-analysis. Behav. Cogn. Psychother. 2016, 44, 673–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Escalera, J.; Chorot, P.; Valiente, R.M.; Reales, J.M.; Sandín, B. Efficacy of transdiagnostic cognitive-behavioral therapy for anxiety and depression in adults, children and adolescents: A meta-analysis. Rev. Psicopatol. Psicol. Clin. 2016, 21, 147–175. [Google Scholar] [CrossRef] [Green Version]
- Sakiris, N.; Berle, D. A systematic review and meta-analysis of the unified protocol as a transdiagnostic emotion regulation based intervention. Clin. Psychol. Rev. 2019, 72, 1–13. [Google Scholar] [CrossRef]
- Ehrenreich-May, J.; Kennedy, S.M.; Sherman, J.A.; Bilek, L.B.; Buzzella, B.A.; Bennett, S.M.; Barlow, D.H. Unified Protocols for Transdiagnostic Treatment of Emotional Disorders in Children and Adolescents; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Ehrenreich, J.T.; Goldstein, C.R.; Wright, L.R.; Barlow, D.H. Development of a unified protocol for the treatment of emotional disorders in youth. Child. Fam. Behav. Ther. 2009, 31, 20–37. [Google Scholar] [CrossRef]
- Ehrenreich-May, J.; Rosenfield, D.; Queen, A.H.; Kennedy, S.M.; Remmes, C.S.; Barlow, D.H. An initial waitlist-controlled trial of the unified protocol for the treatment of emotional disorders in adolescents. J. Anxiety Disord. 2017, 46, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Osma, J. Aplicaciones del Protocolo Unificado Para el Tratamiento Transdiagnóstico de la Disregulación Emocional; Alianza Editorial: Madrid, Spain, 2019. [Google Scholar]
- Trosper, S.E.; Buzzella, B.A.; Bennett, S.M.; Ehrenreich, J.T. Emotion regulation in youth with emotional disorders: Implications for a unified treatment approach. Clin. Child. Fam. Psychol. Rev. 2009, 12, 234–254. [Google Scholar] [CrossRef] [PubMed]
- García-Escalera, J.; Valiente, R.M.; Sandín, B.; Ehrenreich-May, J.; Prieto, A.; Chorot, P. The unified protocol for transdiagnostic treatment of emotional disorders in adolescents (UP-A) adapted as a school-based anxiety and depression prevention program: An initial cluster randomized wait-list-controlled trial. Behav. Ther. 2020, 51, 461–473. [Google Scholar] [CrossRef] [PubMed]
- García-Escalera, J.; Chorot, P.; Sandín, B.; Ehrenreich-May, J.; Prieto, A.; Valiente, R.M. An open trial applying the unified protocol for transdiagnostic treatment of emotional disorders in adolescents (UP-A) adapted as a school-based prevention program. Child. Youth Care Forum 2019, 48, 29–53. [Google Scholar] [CrossRef]
- Titov, N.; Dear, B.F.; Johnston, L.; Terides, M. Transdiagnostic internet treatment for anxiety and depression. Rev. Psicopatol. Psicol. Clin. 2012, 17, 237–260. [Google Scholar] [CrossRef]
- Andersson, G.; Titov, N. Advantages and limitations of internet-based interventions for common mental disorders. World Psychiatry 2014, 13, 4–11. [Google Scholar] [CrossRef]
- Carlbring, P.; Andersson, G.; Cuijpers, P.; Riper, H.; Hedman-Lagerlöf, E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn. Behav. Ther. 2018, 47, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Etzelmueller, A.; Vis, C.; Karyotaki, E.; Baumeister, H.; Titov, N.; Berking, M.; Cuijpers, P.; Riper, H.; Ebert, D.D. Effects of internet-based cognitive behavioral therapy in routine care for adults in treatment for depression and anxiety: Systematic review and meta-analysis. JMIR 2020, 22, 1–27. [Google Scholar] [CrossRef]
- Vigerland, S.; Lenhard, F.; Bonnert, M.; Lalouni, M.; Hedman, E.; Ahlen, J.; Olén, O.; Serlachius, E.; Ljótsson, B. Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 50, 1–10. [Google Scholar] [CrossRef]
- Barlow, D.H.; Farchione, T.J.; Sauer-Zavala, S.; Latin, H.M.; Ellard, K.K.; Bullis, J.R.; Bentley, K.H.; Boettcher, H.T.; Cassiello-Robbins, C. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Gonzalez-Robles, A.; Garcia-Palacios, A.; Baños, R.; Riera, A.; Llorca, G.; Traver, F.; Haro, G.; Palop, V.; Lera, G.; Romeu, J.E.; et al. Effectiveness of a transdiagnostic internet-based protocol for the treatment of emotional disorders versus treatment as usual in specialized care: Study protocol for a randomized controlled trial. Trials 2015, 16, 488–493. [Google Scholar] [CrossRef] [Green Version]
- Păsărelu, C.R.; Andersson, G.; Bergman Nordgren, L.; Dobrean, A. Internet-delivered transdiagnostic and tailored cognitive behavioral therapy for anxiety and depression: A systematic review and meta-analysis of randomized controlled trials. Cogn. Behav. Ther. 2017, 46, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Pineda, D.; Espinosa, V.; Magaz, A.M.; Chorot, P. Protocolo unificado para el tratamiento transdiagnóstico de los trastornos emocionales en adolescentes a través de internet (iUP-A): Aplicación web y protocolo de un ensayo controlado aleatorizado [Internet-delivered unified protocol for transdiagnostic treatment of emotional disorders in adolescents (iUP-A): Web application and study protocol for a randomized controlled trial]. Rev. Psicopatol. Psicol. Clin. 2019, 24, 197–215. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Colón-Soto, M.; Díaz, V.; Soto, O.; Santana, C. Mini International Neuropsychiatric Interview Para Niños y Adolescentes (MINI-KID) Versión en Español; Medical Outcome Symptoms: Tampa, FL, USA, 2005. [Google Scholar]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N. TREND Group Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Ehrenreich-May, J.; Queen, A.H.; Bilek, E.L.; Remmes, C.S.; Kristen, K.M. The Unified Protocols for the Treatment of Emotional Disorders in Children and Adolescents. In Transdiagnostic Treatments for Children and Adolescents: Principles and Practice; Ehrenreich-May, J., Chu, B.C., Eds.; Guilford Press: New York, NY, USA, 2014; pp. 267–292. [Google Scholar]
- Sandín, B.; Chorot, P.; Valiente, R.M. TCC de los Trastornos de Ansiedad: Innovaciones en Niños y Adolescentes [CBT for Anxiety Disorders: Innovations for Children and Adolescents]; Klinik: Madrid, Spain, 2016. [Google Scholar]
- Sandín, B.; Chorot, P.; Valiente, R.M.; Chorpita, B.F. Development of a 30-item version of the Revised Child Anxiety and Depression Scale. Rev. Psicopatol. Psicol. Clin. 2010, 15, 165–178. [Google Scholar] [CrossRef] [Green Version]
- Sandín, B. Escalas PANAS de afecto positivo y negativo para niños y adolescentes (PANASN) [The PANAS scales of positive and negative affect for children and adolescents (PANASN)]. Rev. Psicopatol. Psicol. Clin. 2003, 8, 173–182. [Google Scholar] [CrossRef] [Green Version]
- Silverman, W.K.; Fleisig, W.; Rabian, B.; Peterson, R.A. Childhood anxiety sensitivity index. J. Clin. Child. Adolesc. Psychol. 1991, 20, 162–168. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Santed, M.A.; Valiente, R.M. Análisis factorial confirmatorio del Índice de Sensibilidad a la Ansiedad para Niños [A confirmatory factor analysis of the Childhood Anxiety Sensitivity Index]. Psicothema 2002, 14, 333–339. [Google Scholar]
- Kennedy, S.M.; Ehrenreich-May, J. Assessment of emotional avoidance in adolescents: Psychometric properties of a new multidimensional measure. J. Psychopathol. Behav. Assess. 2016, 39, 279–290. [Google Scholar] [CrossRef]
- García-Escalera, J.; Chorot, P.; Valiente, R.; Sandín, B.; Tonarely, N.; Ehrenreich-May, J. Spanish Version of the Emotional Avoidance Strategy Inventory for Adolescents (EASI-A); Universidad Nacional de Educación a Distancia: Madrid, Spain, 2016; Unpublished. [Google Scholar]
- Sandín, B.; Chorot, P.; Valiente, R.M. Cuestionario PSWQ para Niños y Adolescentes (PSWQN-11) [Questionnaire PSWQ for Children and Adolescents (PSWQ-11)]; Universidad Nacional de Educación a Distancia: Madrid, Spain, 2010; Unpublished. [Google Scholar]
- La Greca, A.M.; Stone, W.L. Social anxiety scale for children-revised: Factor structure and concurrent validity. J. Clin. Child. Psychol. 1993, 22, 17–27. [Google Scholar] [CrossRef]
- Sandín, B. Ansiedad, Miedos y Fobias en Niños y Adolescentes [Anxiety, Fears and Phobias in Children and Adolescents]; Dykinson: Madrid, Spain, 1997. [Google Scholar]
- Houck, P.R.; Spiegel, D.A.; Shear, M.K.; Rucci, P. Reliability of the self-report version of the panic disorder severity scale. Depress. Anxiety 2002, 15, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Sandín, B. Panic Disorder Severity Scale–Self Report (PDSS-SR) (Spanish version). In Trastorno de Pánico; Sandín, B., Ed.; UNED: Madrid, Spain, 2010. [Google Scholar]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the mini international neuropsychiatric interview for children and adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Valiente, R.M.; Sandín, B.; Chorot, P. Miedos comunes en niños y adolescentes: Relación con la sensibilidad a la ansiedad, el rasgo de ansiedad, la afectividad negativa y la depresión [Common fears in children and adolescents: Their relationship to anxiety sensitivity, trait anxiety, negative affectivity, and depression]. Rev. Psicopatol. Psicol. Clin. 2002, 7, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Sandín, B.; Chorot, P.; Valiente, R.M.; Lostao, L. Validación española del cuestionario de preocupación PSWQ: Estructura factorial y propiedades psicométricas [Spanish validation of the PSWQ: Factor structure and psychometric properties]. Rev. Psicopatol. Psicol. Clin. 2009, 14, 107–122. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Arribas, C.; Chorot, P.; Valiente, R.M.; Sandín, B. Evaluación de factores cognitivos positivos y negativos relacionadas con el trastorno de pánico: Validación del CATP [Assessment of positive and negative cognitive factors related to panic disorder: Validation of the CATP]. Rev. Psicopatol. Psicol. Clin. 2015, 20, 85–100. [Google Scholar] [CrossRef] [Green Version]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Chorot, P. Feasibility and Acceptability Questionnaire (FAQ); Universidad Nacional de Educación a Distancia: Madrid, Spain, 2020; Unpublished. [Google Scholar]
- Rapee, R.M.; Wignall, A.; Sheffield, J.; Kowalenko, N.; Davis, A.; McLoone, J.; Spence, S.H. Adolescents’ reactions to universal and indicated prevention programs for depression: Perceived stigma and consumer satisfaction. Prevent. Sci. 2006, 7, 167–177. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- De la Torre-Luque, A.; Fiol-Veny, A.; Essau, C.A.; Balle, M.; Bornas, X. Effects of a transdiagnostic cognitive behaviour therapy-based programme on the natural course of anxiety symptoms in adolescence. J. Affect. Disord. 2020, 264, 474–482. [Google Scholar] [CrossRef]
- Fernández-Martínez, I.; Orgilés, M.; Morales, A.; Espada, J.P.; Essau, C.A. One-Year follow-up effects of a cognitive behavior therapy-based transdiagnostic program for emotional problems in young children: A school-based cluster-randomized controlled trial. J. Affect. Disord. 2020, 262, 258–266. [Google Scholar] [CrossRef]
- Calear, A.L.; Batterham, P.J.; Poyser, C.T.; Mackinnon, A.J.; Griffiths, K.M.; Christensen, H. Cluster randomised controlled trial of the e-couch Anxiety and Worry program in schools. J. Affect. Disord. 2016, 196, 210–217. [Google Scholar] [CrossRef] [PubMed]
- González-Robles, A.; Díaz-García, A.; García-Palacios, A.; Roca, P.; Ramos-Quiroga, J.A.; Botella, C. Effectiveness of a Transdiagnostic Guided Internet-Delivered Protocol for Emotional Disorders Versus Treatment as Usual in Specialized Care: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Ellard, K.K.; Bernstein, E.E.; Hearing, C.; Baek, J.H.; Sylvia, L.G.; Nierenberg, A.A.; Barlow, D.H.; Deckersbach, T. Transdiagnostic treatment of bipolar disorder and comorbid anxiety using the Unified Protocol for Emotional Disorders: A pilot feasibility and acceptability trial. J. Affect. Disord. 2017, 219, 209–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilek, E.L.; Ehrenreich-May, J. An open trial investigation of a transdiagnostic group treatment for children with anxiety and depressive symptoms. Behav. Ther. 2012, 43, 887–897. [Google Scholar] [CrossRef]
- Stallard, P.; Richardson, T.; Velleman, S.; Attwood, M. Computerized CBT (Think, Feel, Do) for depression and anxiety in children and adolescents: Outcomes and feedback from a pilot randomized controlled trial. Behav. Cogn. Psychother. 2011, 39, 273. [Google Scholar] [CrossRef] [Green Version]
- Tillfors, M.; Andersson, G.; Ekselius, L.; Furmark, T.; Lewenhaupt, S.; Karlsson, A.; Carlbring, P. A randomized trial of internet-delivered treatment for social anxiety disorder in high school students. Cogn. Behav. Ther. 2011, 40, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Carlbring, P.; Gunnarsdóttir, M.; Hedensjö, L.; Andersson, G.; Ekselius, L.; Furmark, T. Treatment of social phobia: Randomised trial of internet-delivered cognitive-behavioural therapy with telephone support. Br. J. Psychiatry 2007, 190, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Andersson, G.; Paxling, B.; Wiwe, M.; Vernmark, K.; Felix, C.B.; Lundborg, L.; Furmark, T.; Cuijpers, P.; Carlbring, P. Therapeutic alliance in guided internet-delivered cognitive behavioural treatment of depression, generalized anxiety disorder and social anxiety disorder. Behav. Res. Ther. 2012, 50, 544–550. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Principal Diagnosis/Symptoms | Comorbid Diagnoses/Symptoms |
|---|---|
| Social phobia | Depressive symptoms |
| Bulimia | Major depressive disorder |
| Anxiety and depressive symptoms | --- |
| Social phobia | --- |
| Major depressive disorder | Generalized anxiety disorder |
| Panic disorder with agoraphobia | Obsessive-compulsive disorder |
| Anxiety symptoms | --- |
| Hypomanic episode–current and past | Separation anxiety disorder; Obsessive-compulsive disorder; Oppositional defiant disorder |
| Depressive symptoms | --- |
| Panic disorder without agoraphobia | --- |
| Major depressive disorder | Posttraumatic stress disorder |
| Posttraumatic stress disorder | Agoraphobia; Social phobia; Obsessive-compulsive disorder; Transient TIC Disorder |
| Module Title | Main Contents |
|---|---|
| [M1] Building motivation | Obtain three top problems, severity ratings, and a goal for each problem. Discover what motivates the adolescent to change. |
| [M2] Getting to know your emotions | Psychoeducation about emotions and their function. Understand the three parts of emotional experiences. Learn about emotional behaviors and the cycle of avoidance. |
| [M3] Enjoy positive activities | Psychoeducation about opposite action and behavioral experiments. Come up with a list of enjoyed activities. Engage the adolescent in behavioral experiments (behavioral activation) for sadness. |
| [M4] Awareness of your emotional experiences | Introduce the rationale for present-moment awareness and non-judgmental awareness. Practice body scanning. Practice awareness skills when exposed to non-emotional and emotional triggers. |
| [M5] Learn to be flexible in your thinking | Learn about the concept of “thinking traps” (i.e., cognitive distortions), automatic thoughts, and alternative thoughts. Learn detective thinking and problem-solving skills. |
| [M6] Cope with your body sensations | Psychoeducation about body sensations, their relationship with intense emotions, and their harmlessness. Conduct exposures to body sensations to learn to tolerate uncomfortable physical feelings. |
| [M7] Cope with emotional situations | Review the cycle of avoidance and introduce situational emotion exposures. Create an Emotional Behaviors Form to identify relevant exposures. Assign exposures for home learning. |
| [M8] Maintain your gains | Review skills that have been most useful for each adolescent and make an individualized relapse prevention plan. |
| Measures | Pre-Treatment n = 12 | Post-Treatment n = 8 | Completer Sample Analyses n = 8 | Intention-to-Treat Analyses b n = 12 | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Z a | d | d | |
| CDN | 19.17 | 11.50 | 15.25 | 8.92 | 1.47 | 1.14 | 0.66 |
| EAN | 14.50 | 8.58 | 10.88 | 5.82 | 2.38 ** | 2.36 | 1.43 |
| RCADS-30 | |||||||
| Total | 32.58 | 18.43 | 24.25 | 9.68 | 2.38 ** | 4.14 | 2.58 |
| MDD | 6.42 | 4.08 | 4.88 | 3.23 | 2.05 * | 0.96 | 0.58 |
| PD | 4.83 | 5.11 | 1.75 | 1.98 | 1.99 * | 2.54 | 1.75 |
| Soc.P | 8.58 | 4.40 | 8.25 | 3.49 | 1.06 | 0.88 | 0.52 |
| SAD | 1.25 | 1.54 | 0.88 | 1.13 | 1.84 + | 0.74 | 0.52 |
| GAD | 7.33 | 3.80 | 5.88 | 2.10 | 2.21 * | 2.27 | 1.25 |
| OCD | 4.17 | 4.59 | 2.63 | 1.85 | 1.10 | 1.32 | 0.93 |
| Measures | Pre-Treatment n = 12 | Post-Treatment n = 8 | Completer Sample Analyses n = 8 | Intention-to-Treat Analyses b n = 12 | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Z a | d | d | |
| PANASN-NA | 21.08 | 2.91 | 20.75 | 2.66 | 0.50 | 0.53 | 0.35 |
| PANASN-PA | 20.50 | 3.80 | 23.38 | 4.27 | 1.47 + | −1.13 | −0.73 |
| CASI | 31.92 | 8.52 | 29.00 | 4.66 | 2.22 * | 2.87 | 1.74 |
| EASI-A | 37.25 | 16.24 | 32.13 | 12.91 | 1.82 * | 2.97 | 1.19 |
| PDSS-SR | 10.58 | 8.03 | 2.75 | 3.49 | 2.52 ** | 4.82 | 2.59 |
| PSWQ-N | 32.92 | 12.92 | 27.25 | 5.42 | 2.39 ** | 3.40 | 2.30 |
| SASC-R | 37.67 | 10.82 | 40.88 | 5.79 | 0.42 | 0.67 | 0.37 |
| Experience with the Online Platform (Range: 0–10) | M | SD |
| How easy has it been for you to use the AMTE online platform? | 9.00 | 1.20 |
| How easy has it been for you to understand what the videos and Dr. AMTE were telling you? | 8.50 | 1.77 |
| How useful has it been for you what Dr. AMTE and the different videos were teaching you? | 9.38 | 0.92 |
| How easy has it been for you to include the AMTE program in your daily routine? | 8.50 | 1.60 |
| To what degree have you been able to do the exercises and home learning assignments without technical or computer problems? | 7.25 | 1.58 |
| To what extent have you applied what you have learned with AMTE to your real life? | 8.50 | 0.93 |
| Satisfaction with the Program (Range: 0–10) | M | SD |
| How much did you learn in this program? | 8.75 | 1.58 |
| How effective was this program in helping you cope with your problems? | 8.86 | 1.07 |
| How much did you enjoy doing this program? | 8.50 | 1.20 |
| To what extent would you recommend the program to other adolescents? | 9.38 | 0.74 |
| What was your ability to cope with emotions before the program? | 4.13 | 1.64 |
| What was your ability to cope with emotions after the program? | 8.25 | 1.39 |
| Ability to cope with emotions after the program minus ability before | 4.13 | 1.96 |
| Therapeutic Alliance (Range: 0–10) | M | SD |
| How much has your therapist helped you deal with your top problems? | 8.88 | 1.46 |
| How appreciated by your therapist have you felt? | 9.50 | 0.76 |
| To what extent have you felt that you and your therapist respected each other? | 9.88 | 0.35 |
| To what extent have you agreed with your therapist on what things were important for you to work to overcome? | 9.50 | 1.07 |
| To what extent have you felt that your therapist cared about you? | 9.38 | 0.92 |
| How correct do you think the way you and your therapist have worked to solve your problems has been? | 9.38 | 0.92 |
| Experience of the Adolescent with the Online Platform (Range: 0–10) | M | SD |
| How easy has it been for your son/daughter to use the AMTE online platform? | 8.50 | 1.31 |
| How easy has it been for your child to understand what the videos and Dr. AMTE were telling them? | 9.25 | 1.04 |
| How useful has it been for your child what Dr. AMTE and the different videos were teaching them? | 8.88 | 1.36 |
| How easy has it been for your child to include the AMTE program in their daily routine? | 8.63 | 1.41 |
| To what degree has your child been able to do the exercises and home learning assignments without technical or computer problems? | 8.63 | 1.06 |
| To what extent has your child applied what he/she has learned with AMTE to their real life? | 8.38 | 1.60 |
| Experience with the Parent’s Section of the Online Platform | n (%) [yes] | |
| Have you ever logged in to the parent’s section of the AMTE platform? | 7 (87.50%) | |
| To what extent has the parent’s section of the platform helped you to help your son/daughter during treatment? (range: 0–10) | 7.29 | 2.81 |
| Satisfaction with the Program (Range: 0–10) | M | SD |
| How much has your child learned in this program? | 9.14 | 0.69 |
| How effective was this program in helping your child cope with their problems? | 9.14 | 1.07 |
| How much has your child enjoyed doing this program? | 8.00 | 2.27 |
| To what extent would you recommend the program to other adolescents? | 9.75 | 0.71 |
| What was the ability of your child to cope with emotions before the program? | 4.63 | 2.00 |
| What was the ability of your child to cope with their emotions after the program? | 8.00 | 1.51 |
| Ability to cope with emotions after the program minus ability before | 3.38 | 1.51 |
| Therapeutic Alliance (Range: 0–10) | M | SD |
| How much has the therapist helped your child deal with their top problems? | 9.38 | 0.92 |
| How appreciated by the therapist has your child felt? | 9.88 | 0.35 |
| To what extent have you felt that you and the therapist respected each other? | 9.88 | 0.35 |
| To what extent have you agreed with the therapist on what things were important for your son/daughter to work to overcome? | 9.75 | 0.46 |
| To what extent have you felt that the therapist cared about your child? | 9.88 | 0.35 |
| How correct do you think the AMTE’s approach to solving your child problems has been? | 9.75 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandín, B.; García-Escalera, J.; Valiente, R.M.; Espinosa, V.; Chorot, P. Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial. Int. J. Environ. Res. Public Health 2020, 17, 8306. https://doi.org/10.3390/ijerph17228306
Sandín B, García-Escalera J, Valiente RM, Espinosa V, Chorot P. Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial. International Journal of Environmental Research and Public Health. 2020; 17(22):8306. https://doi.org/10.3390/ijerph17228306
Chicago/Turabian StyleSandín, Bonifacio, Julia García-Escalera, Rosa M. Valiente, Victoria Espinosa, and Paloma Chorot. 2020. "Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial" International Journal of Environmental Research and Public Health 17, no. 22: 8306. https://doi.org/10.3390/ijerph17228306