Clinical Relevance of Unexpected Findings of Post-Mortem Computed Tomography in Hospitalized Patients: An Observational Study


Abstract
:1. Introduction
1.1. Background
1.2. Purpose
2. Material and Methods
2.1. Setting and Design
2.2. Participants
2.3. Procedures
2.4. Identification and Classification of PMCT Findings
2.5. Methodological Analysis
3. Results
3.1. Patient Demographics
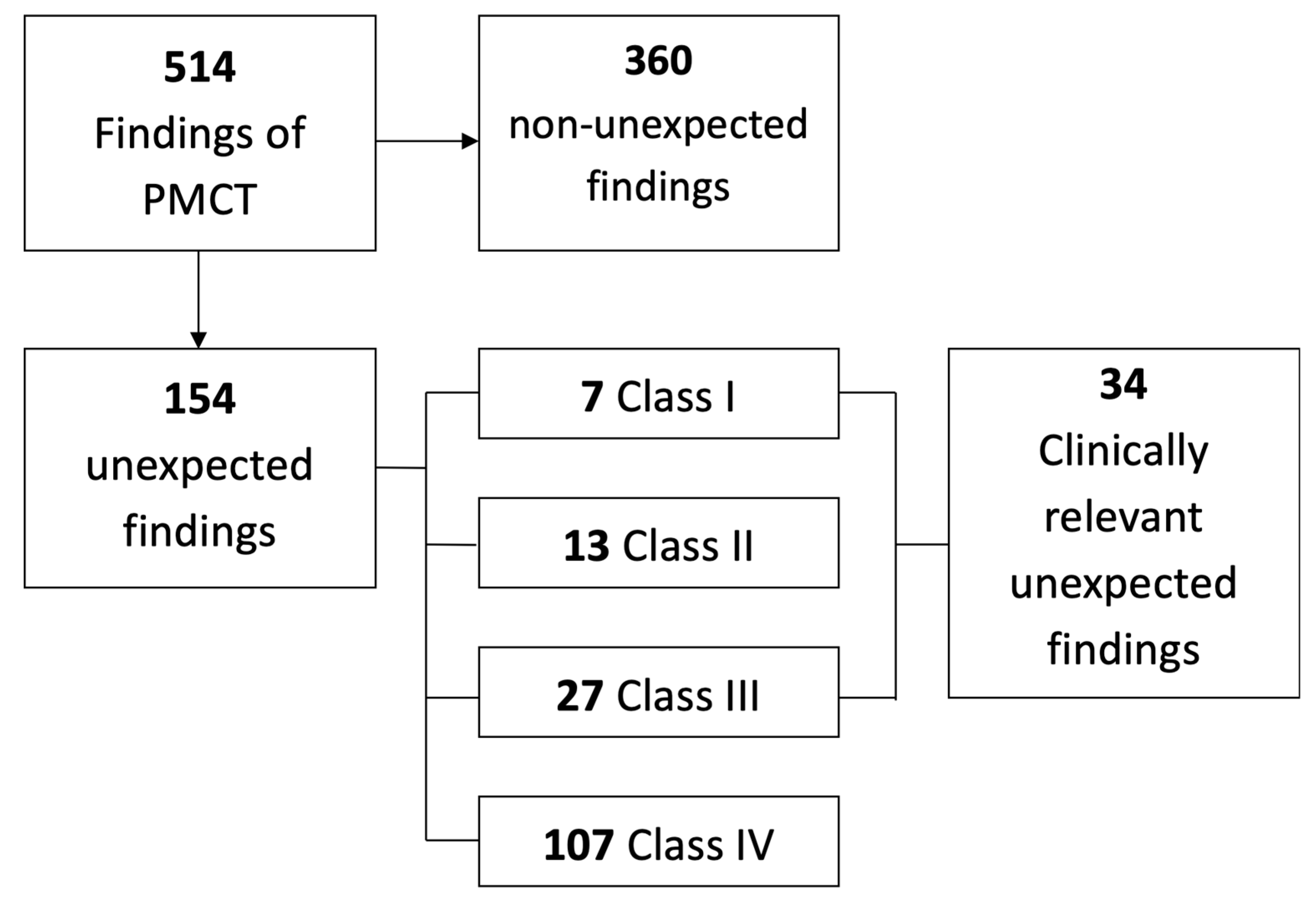
3.2. PMCT Findings
3.3. Relevant Unexpected PMCT Findings

{kind=link}
{kind=link}
{kind=link}
| Unexpected Findings (n = 154) | Clinically Relevant Unexpected Findings (n = 34) | Reported Clinically Relevant Findings | |
|---|---|---|---|
| Concordant with autopsy | 92 | 21 | Pancreatitis, pneumonia, excessive pleural fluid, pulmonary edema, gastro-intestinal bleeding, lung bleeding, lung mass, large hematoma (groin), pneumoporta (autopsy showed bowel ischemia), pneumothorax. |
| False-positive of PMCT (type I error) | 21 | 7 | No pathological substrate was found during autopsy in four of these findings (lung consolidation, lung edema, lung bleeding, pancreatitis). The other three findings were a lung consolidation, which turned out to be lung edema; a retroperitoneal bleeding that turned out to be a suppurative pyelonephritis; and pericardial fluid, where autopsy showed a thickened pericardium with adhesions. |
| False-negative of autopsy (type II error) | 38 | 3 | Hydropneumothorax, periprosthetic fracture, pneumatosis intestinalis. Two of these findings are illustrated in Figure 2. |
| PMCT findings in absence of brain autopsy | 3 | 3 | Cerebral mass, multiple cerebral metastases, and one case with post-procedural hypoxia. One of these cases is illustrated in Figure 3. |


4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blokker, B.M.; Wagensveld, I.M.; Weustink, A.C.; Oosterhuis, J.W.; Hunink, M.G. Non-invasive or minimally invasive autopsy compared to conventional autopsy of suspected natural deaths in adults: A systematic review. Eur. Radiol. 2016, 26, 1159–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busardo, F.P.; Frati, P.; Guglielmi, G.; Grilli, G.; Pinto, A.; Rotondo, A.; Panebianco, V.; Fineschi, V. Postmortem-computed tomography and postmortem-computed tomography-angiography: A focused update. La Radiol. Med. 2015, 120, 810–823. [Google Scholar] [CrossRef] [PubMed]
- Grabherr, S.; Heinemann, A.; Vogel, H.; Rutty, G.; Morgan, B.; Wozniak, K.; Dedouit, F.; Fischer, F.; Lochner, S.; Wittig, H.; et al. Postmortem CT angiography compared with autopsy: A forensic multicenter study. Radiology 2018, 288, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Rutty, G.N.; Morgan, B.; Robinson, C.; Raj, V.; Pakkal, M.; Amoroso, J.; Visser, T.; Saunders, S.; Biggs, M.; Hollingbury, F.; et al. Diagnostic accuracy of post-mortem CT with targeted coronary angiography versus autopsy for coroner-requested post-mortem investigations: A prospective, masked, comparison study. Lancet 2017, 390, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Morgan, B.; Adlam, D.; Robinson, C.; Pakkal, M.; Rutty, G.N. Adult post-mortem imaging in traumatic and cardiorespiratory death and its relation to clinical radiological imaging. Br. J. Radiol. 2014, 87, 20130662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blokker, B.M.; Weustink, A.C.; Wagensveld, I.M.; von der Thusen, J.H.; Pezzato, A.; Dammers, R.; Bakker, J.; Renken, N.S.; den Bakker, M.A.; van Kemenade, F.J.; et al. Conventional autopsy versus minimally invasive autopsy with postmortem MRI, CT, and CT-guided biopsy: Comparison of diagnostic performance. Radiology 2018, 289, 658–667. [Google Scholar] [CrossRef]
- Roberts, I.S.; Benamore, R.E.; Benbow, E.W.; Lee, S.H.; Harris, J.N.; Jackson, A.; Mallett, S.; Patankar, T.; Peebles, C.; Roobottom, C.; et al. Post-mortem imaging as an alternative to autopsy in the diagnosis of adult deaths: A validation study. Lancet 2012, 379, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Jackowski, C.; Schwendener, N.; Grabherr, S.; Persson, A. Post-mortem cardiac 3-T magnetic resonance imaging: Visualization of sudden cardiac death? J. Am. Coll. Cardiol. 2013, 62, 617–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutty, G.N.; Biggs, M.J.; Brough, A.; Robinson, C.; Mistry, R.; Amoroso, J.; Deshpande, A.; Morgan, B. Ventilated post-mortem computed tomography through the use of a definitive airway. Int. J. Leg. Med. 2015, 129, 325–334. [Google Scholar] [CrossRef]
- Westphal, S.E.; Apitzsch, J.; Penzkofer, T.; Mahnken, A.H.; Knuchel, R. Virtual CT autopsy in clinical pathology: Feasibility in clinical autopsies. Virchows Archiv. Int. J. Pathol. 2012, 461, 211–219. [Google Scholar] [CrossRef]
- Inai, K.; Noriki, S.; Kinoshita, K.; Sakai, T.; Kimura, H.; Nishijima, A.; Iwasaki, H.; Naiki, H. Postmortem CT is more accurate than clinical diagnosis for identifying the immediate cause of death in hospitalized patients: A prospective autopsy-based study. Virchows Arch. Int. J. Pathol. 2016, 469, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnemans, L.J.P.; Kubat, B.; Prokop, M.; Klein, W.M. Can virtual autopsy with postmortem CT improve clinical diagnosis of cause of death? A retrospective observational cohort study in a Dutch tertiary referral centre. BMJ Open 2018, 8, e018834. [Google Scholar] [CrossRef] [PubMed]
- La Russa, R.; Catalano, C.; Di Sanzo, M.; Scopetti, M.; Gatto, V.; Santurro, A.; Viola, R.V.; Panebianco, V.; Frati, P.; Fineschi, V. Postmortem computed tomography angiography (PMCTA) and traditional autopsy in cases of sudden cardiac death due to coronary artery disease: A systematic review and meta-analysis. La Radiol. Med. 2019, 124, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, C.; Doenz, F.; Vaucher, P.; Palmiere, C.; Dominguez, A.; Binaghi, S.; Mangin, P.; Grabherr, S. Postmortem computed tomography angiography vs. conventional autopsy: Advantages and inconveniences of each method. Int. J. Leg. Med. 2013, 127, 981–989. [Google Scholar] [CrossRef] [Green Version]
- Jalalzadeh, H.; Giannakopoulos, G.F.; Berger, F.H.; Fronczek, J.; van de Goot, F.R.W.; Reijnders, U.J.; Zuidema, W.P. Post-mortem imaging compared with autopsy in trauma victims—A systematic review. Forensic Sci. Int. 2015, 257, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Graziani, G.; Tal, S.; Adelman, A.; Kugel, C.; Bdolah-Abram, T.; Krispin, A. Usefulness of unenhanced post mortem computed tomography—Findings in postmortem non-contrast computed tomography of the head, neck and spine compared to traditional medicolegal autopsy. J. Forensic Leg. Med. 2018, 55, 105–111. [Google Scholar] [CrossRef]
- Kuijpers, C.C.; Fronczek, J.; van de Goot, F.R.; Niessen, H.W.; van Diest, P.J.; Jiwa, M. The value of autopsies in the era of high-tech medicine: Discrepant findings persist. J. Clin. Pathol. 2014, 67, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Rotman, S.; Zaugg, T.; Bart, P.A. The role of medical autopsies as a quality control of patients management in internal medicine units. Rev. Med Suisse 2016, 12, 2015–2019. [Google Scholar]
- Shojania, K.G.; Burton, E.C.; McDonald, K.M.; Goldman, L. Changes in rates of autopsy-detected diagnostic errors over time: A systematic review. JAMA 2003, 289, 2849–2856. [Google Scholar] [CrossRef]
- van den Tweel, J.G.; Wittekind, C. The medical autopsy as quality assurance tool in clinical medicine: Dreams and realities. Virchows Arch. Int. J. Pathol. 2016, 468, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Wichmann, D.; Obbelode, F.; Vogel, H.; Hoepker, W.W.; Nierhaus, A.; Braune, S.; Sauter, G.; Pueschel, K.; Kluge, S. Virtual autopsy as an alternative to traditional medical autopsy in the intensive care unit: A prospective cohort study. Ann. Intern. Med. 2012, 156, 123–130. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Goldman, L.; Sayson, R.; Robbins, S.; Cohn, L.H.; Bettmann, M.; Weisberg, M. The value of the autopsy in three medical eras. N. Engl. J. Med. 1983, 308, 1000–1005. [Google Scholar] [CrossRef] [PubMed]

| ICD Chapter | Definition of the ICD Chapter | Number of Findings n (%) | Number of Unexpected Findings in the Chapter n (%) |
|---|---|---|---|
| I | Infectious and parasitic diseases | 6 (0.6) | 4 (66.7) |
| II | Neoplasms | 53 (5.2) | 15 (28.3) |
| III | Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism | 1 (0.1) | 0 (0) |
| IV | Endocrine, nutritional, and metabolic diseases | 21 (2.1) | 16 (76.2) |
| VI | Diseases of the nervous system | 22 (2.2) | 4 (18.2) |
| VIII | Diseases of the ear and mastoid process | 2 (0.2) | 1 (50) |
| IX | Diseases of the circulatory system | 209 (20.5) | 42 (20.1) |
| X | Diseases of the respiratory system | 310 (30.4) | 76 (24.5) |
| XI | Diseases of the digestive system | 107 (10.5) | 36 (33.6) |
| XII | Diseases of the skin and subcutaneous tissue | 2 (0.2) | 0 (0) |
| XIII | Diseases of the musculoskeletal system and connective tissue | 33 (3.2) | 13 (39.4) |
| XIV | Diseases of the genitourinary system | 69 (6.8) | 22 (31.9) |
| XVII | Congenital malformations, deformations, and chromosomal abnormalities | 10 (1.0) | 3 (30) |
| XVIII | Symptoms, signs, and abnormal findings, not elsewhere classified | 153 (15.0) | 61 (39.9) |
| XIX | Injury, poisoning, and certain other consequences of external causes | 22 (2.2) | 9 (40.9) |
| Total | 1020 (100) | 302 (29.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mentink, M.G.; Latten, B.G.H.; Bakers, F.C.H.; Mihl, C.; Rennenberg, R.J.M.W.; Kubat, B.; Hofman, P.A.M. Clinical Relevance of Unexpected Findings of Post-Mortem Computed Tomography in Hospitalized Patients: An Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 7572. https://doi.org/10.3390/ijerph17207572
Mentink MG, Latten BGH, Bakers FCH, Mihl C, Rennenberg RJMW, Kubat B, Hofman PAM. Clinical Relevance of Unexpected Findings of Post-Mortem Computed Tomography in Hospitalized Patients: An Observational Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7572. https://doi.org/10.3390/ijerph17207572
Chicago/Turabian StyleMentink, Max G., Bartholomeus G. H. Latten, Frans C. H. Bakers, Casper Mihl, Roger J. M. W. Rennenberg, Bela Kubat, and Paul A. M. Hofman. 2020. "Clinical Relevance of Unexpected Findings of Post-Mortem Computed Tomography in Hospitalized Patients: An Observational Study" International Journal of Environmental Research and Public Health 17, no. 20: 7572. https://doi.org/10.3390/ijerph17207572