The Relationship between Leisure-Time Sedentary Behaviors and Metabolic Risks in Middle-Aged Chinese Women


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Anthropometric Measurements
2.3. Categories of LTSB
2.4. Definitions of Outcome Variables
2.4.1. Diabetes
2.4.2. Dyslipidemia
2.4.3. Hypertension
2.4.4. Overweight and Obesity
2.4.5. Metabolic Syndrome
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. The Relationship between LTSB and TC, TG, HDL-C, WC, and BMI
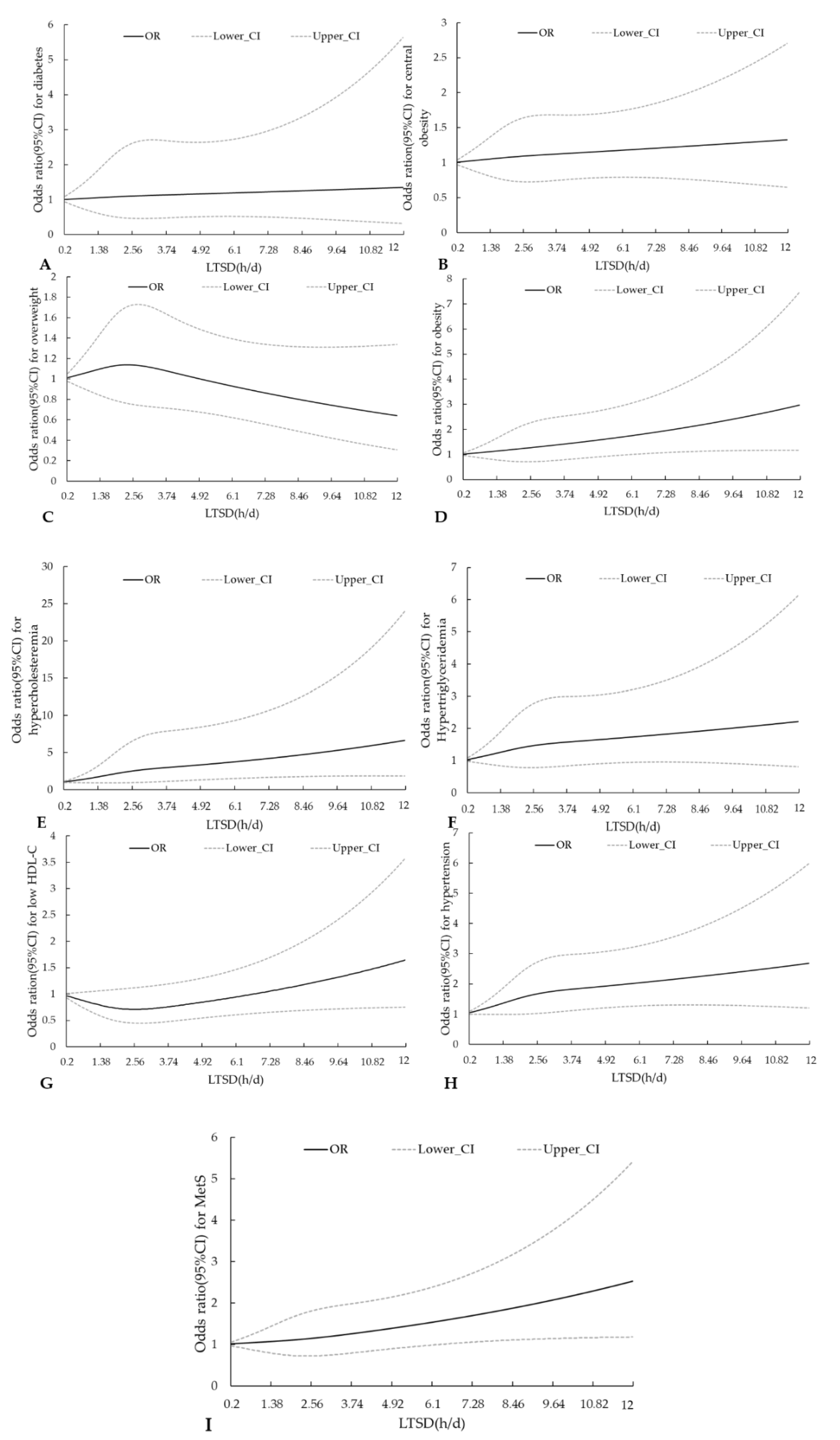
3.3. RCS Curves for LTSD and Metabolic Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 2 July 2020).
- WHO. Global Status Report on Noncommunicable Diseases 2014. Available online: https://www.who.int/nmh/publications/ncd-status-report-2014/en/ (accessed on 26 August 2020).
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Hassen Abate, K.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [Green Version]
- He, Y.N.; Zhao, W.H.; Zhao, L.Y.; Yu, D.M.; Zhang, J.; Yang, X.G.; Ding, G.Q. Prevalance of metabolic syndrome in Chinese adults in 2010–2012. Chin. J. Epidemiol. 2017, 38, 212–215. [Google Scholar] [CrossRef]
- Zhang, J.; Shi, X.M.; Liang, X.F. Economic costs of both overweight and obesity among Chinese urban and rural residents, in 2010. Chin. J. Epidemiol. 2013, 34, 598–600. [Google Scholar] [CrossRef]
- Liu, M.B.; Li, Y.C.; Liu, S.W.; Wang, W.; Zhou, M.G. Burden on blood-pressure-related diseases among the Chinese population, in 2010. Chin. J. Epidemiol. 2014, 680–683. [Google Scholar] [CrossRef]
- Chinese Diabetes Society, National Office for Primary Diabetes Care. National guidelines for the prevention and control of diabetes in primary care (2018). Chin. J. Intern. Med. 2018, 57, 885–893. [Google Scholar] [CrossRef]
- Joint Committee for Guideline Revision. 2016 Chinese guidelines for the management of dyslipidemia in adults. J. Geriatr. Cardiol. 2018, 15, 1–29. [Google Scholar] [CrossRef]
- Pate, R.R.; O’Neill, J.R.; Lobelo, F. The evolving definition of “sedentary”. Exerc. Sport Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef]
- Bennett, D.A.; Du, H.; Bragg, F.; Guo, Y.; Wright, N.; Yang, L.; Bian, Z.; Chen, Y.; Yu, C.; Wang, S.; et al. Physical activity, sedentary leisure-time and risk of incident type 2 diabetes: A prospective study of 512,000 Chinese adults. BMJ Open Diabetes Res. Care 2019, 7, e000835. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B.; Li, T.Y.; Colditz, G.A.; Willett, W.C.; Manson, J.E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. Jama J. Am. Med. Assoc. 2003, 289, 1785–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, M.; Tremblay, M.S. Sedentary behaviour and obesity. Health Rep. 2008, 19, 19–30. [Google Scholar] [PubMed]
- Su, C.; Jia, X.F.; Wang, Z.H.; Wang, H.J.; Ouyang, Y.F.; Zhang, B. Longitudinal association of leisure time physical activity and sedentary behaviors with body weight among Chinese adults from China Health and Nutrition Survey 2004–2011. Eur J. Clin. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Man Sup, L.; Bumjung, P.; Il Gyu, K.; Songyong, S.; So Young, K.; Jin-Hwan, K.; Hyo Geun, C. Leisure sedentary time is differentially associated with hypertension, diabetes mellitus, and hyperlipidemia depending on occupation. BMC Public Health 2017. [Google Scholar] [CrossRef] [Green Version]
- Beunza, J.J.; Martínez-González, M.A.; Ebrahim, S.; Bes-Rastrollo, M.; Núñez, J.; Martínez, J.A.; Alonso, A. Sedentary behaviors and the risk of incident hypertension: The SUN Cohort. Am. J. Hypertens. 2007, 20, 1156–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisson, S.B.; Camhi, S.M.; Church, T.S.; Martin, C.K.; Tudor-Locke, C.; Bouchard, C.; Earnest, C.P.; Smith, S.R.; Newton, R.L., Jr.; Rankinen, T.; et al. Leisure time sedentary behavior, occupational/domestic physical activity, and metabolic syndrome in U.S. men and women. Metab. Syndr. Relat. Disord. 2009, 7, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Salmon, J.; Owen, N.; Armstrong, T.; Zimmet, P.Z.; Welborn, T.A.; Cameron, A.J.; Dwyer, T.; Jolley, D.; Shaw, J.E.; et al. Associations of TV viewing and physical activity with the metabolic syndrome in Australian adults. Diabetologia 2005, 48, 2254–2261. [Google Scholar] [CrossRef] [Green Version]
- Barton, M. Cholesterol and atherosclerosis: Modulation by oestrogen. Curr. Opin. Lipidol. 2013, 24, 214–220. [Google Scholar] [CrossRef]
- Poehlman, E.T. Retracted: Menopause, energy expenditure, and body composition. Acta Obstet. Gynecol. Scand. 2002, 81, 603–611. [Google Scholar] [CrossRef]
- WHO. Physical Activity and Women. Available online: https://www.who.int/dietphysicalactivity/factsheet_women/en/ (accessed on 9 July 2020).
- Zhao, L.; Ma, G.; Piao, J.; Zhang, J.; Yu, D.; He, Y.; Huo, J.; Hu, X.; Yang, Z.; Yang, X. Scheme of the 2010–2012 Chinese nutrition and health surveillance. Chin. J. Prev. Med. 2016, 50, 204–207. [Google Scholar] [CrossRef]
- Liu, L.; Wu, S.; Wang, J.; Wang, W.; Bao, Y.; Cai, J.; Chen, L.; Chen, W.; Chu, S.; Feng, Y.; et al. 2018 Chinese guidelines for the management of hypertension. Chin. J. Cardiol. 2019, 24, 24–56. [Google Scholar] [CrossRef]
- Chen, C.M.; Frank, C.L.; Department of Disease Control Ministry of Health, PR China. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci. 2004, 17, 1–36. [Google Scholar] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and management of the metabolic syndrome—An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Curr. Opin. Cardiol. 2006, 21, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauthier, J.; Wu, Q.V.; Gooley, T.A. Cubic splines to model relationships between continuous variables and outcomes: A guide for clinicians. Bone Marrow Transplant. 2020, 55, 675–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.J.; Wang, C.Y.; Fan, H.M.; Hu, B.; Yang, Y.Y.; Wang, L.H.; Xiao, M.Y.; Che, C.L.; Yuan, J.X. Relationship Between Shift Work Years and Hypertension in Male Steel Workers: Based on Restricted Cubic Spline Model. J. Environ. Occup. Med. 2016, 33, 839–844. [Google Scholar] [CrossRef]
- Fan, J.; Ding, C.; Gong, W.; Yuan, F.; Zhang, Y.; Feng, G.; Song, C.; Liu, A. Association of Sleep Duration and Overweight/Obesity among Children in China. Int J. Environ. Res. Public Health 2020, 17, 1962. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.J.; Su, J.; Yu, H.; Luo, P.F.; Qin, Y.; Pan, E.C.; Gao, Y.; Zhang, N.; Zhou, J.Y.; Yu, X.J.; et al. Association between sedentary behavior and mortality in patients with type 2 diabetes: A dose-response relationship analysis. Chin. J. Endocrinol. Metab. 2019, 35, 296–301. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Salmon, J.; Owen, N.; Armstrong, T.; Zimmet, P.Z.; Welborn, T.A.; Cameron, A.J.; Dwyer, T.; Jolley, D.; Shaw, J.E. Physical activity and television viewing in relation to risk of undiagnosed abnormal glucose metabolism in adults. Diabetes Care 2004, 27, 2603–2609. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Hamburg, N.M.; McMackin, C.J.; Huang, A.L.; Shenouda, S.M.; Widlansky, M.E.; Schulz, E.; Gokce, N.; Ruderman, N.B.; Keaney, J.F., Jr.; Vita, J.A. Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2650–2656. [Google Scholar] [CrossRef] [Green Version]
- Bey, L.; Hamilton, M.T. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: A molecular reason to maintain daily low-intensity activity. J. Physiol 2003, 551, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, L.A.; Bagwell, M. Television viewing and obesity in adult females. Am. J. Public Health 1991, 81, 908–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Low-Level LTSB (<2.0 h/day) | Middle-Level LTSB (2.0–3.0 h/day) | High-Level LTSB (≥3.0 h/day) | p |
|---|---|---|---|---|
| Total | 463 (17.5%) | 962 (36.4%) | 1218 (46.1%) | |
| Residence (%) | ||||
| Urban | 47.5 | 45.5 | 57.2 | <0.0001 |
| Rural | 52.5 | 54.5 | 42.8 | |
| Education (%) | ||||
| Primary school and low | 46.4 | 37.9 | 30.9 | <0.0001 |
| Middle school | 33.7 | 36.5 | 37.7 | |
| High school and above | 19.9 | 25.6 | 31.4 | |
| Family income | ||||
| Low income | 50.8 | 46.9 | 44.6 | 0.184 |
| Middle income | 36.5 | 36.0 | 39.2 | |
| High income | 8.0 | 10.8 | 10.8 | |
| Unknown | 4.8 | 6.3 | 5.5 | |
| BMI (kg/m²) | 24.3 ± 13.3 | 24.6 ± 3.3 | 24.6 ± 3.6 | 0.097 |
| WC (cm) | 81.3 ± 9.0 | 81.5 ± 8.9 | 81.3 ± 9.3 | 0.203 |
| Leisure exercise (%) | 13.8 | 13.6 | 15.3 | 0.509 |
| Drinking (%) | 19.2 | 17.3 | 17.2 | 0.583 |
| Energy intake (kcal) | 1912.8 ± 737.6 | 1936.2 ± 743.2 | 1908.7 ± 818.8 | 0.485 |
| Fat energy ratio (%) | 26.6 ± 13.3 | 27.2 ± 12.8 | 27.7 ± 12.8 | 0.000 |
| TC (mmol/L) | 4.66 ± 0.93 | 4.72 ± 0.93 | 4.83 ± 0.96 | 0.007 |
| TG (mmol/L) | 1.38 ± 0.91 | 1.43 ± 0.99 | 1.49 ± 1.07 | 0.031 |
| HDL-C (mmol/L) | 1.21 ± 0.34 | 1.22 ± 0.32 | 1.22 ± 0.33 | 0.264 |
| Hypercholesteremia (%) | 4.3 | 5.2 | 8.2 | 0.002 |
| Hypertriglyceridemia (%) | 11.0 | 12.6 | 13.1 | 0.528 |
| Low HDL-C level (%) | 29.2 | 25.0 | 25.9 | 0.230 |
| Diabetes (%) | 5.2 | 6.8 | 5.9 | 0.477 |
| Hypertension (%) | 20.7 | 25.9 | 25.9 | 0.068 |
| BMI status | <0.0001 | |||
| Underweight | 2.2 | 2.4 | 2.4 | |
| Normal | 46.2 | 40.8 | 43.3 | |
| Overweight | 37.4 | 42.6 | 38.1 | |
| Obesity | 14.3 | 14.2 | 16.3 | |
| Central Obesity (%) | 55.3 | 55.9 | 55.7 | 0.975 |
| Metabolic syndrome (%) | 25.7 | 27.4 | 28.2 | 0.601 |
| Variables | Simple Linear Regression | Multiple Linear Regression 1 | ||
|---|---|---|---|---|
| β1 | p1 | β2 | p2 | |
| TC | 0.04 | 0.004 | 0.03 | 0.019 |
| TG | 0.03 | 0.030 | 0.04 | 0.015 |
| HDL-C | 0.00 | 0.534 | 0.00 | 0.336 |
| WC | 0.15 | 0.253 | 0.23 | 0.076 |
| BMI | 0.08 | 0.112 | 0.10 | 0.055 |
| LTSD | OR | 95% CI | p for Trend |
|---|---|---|---|
| 1.3 | 1.06 | (0.79–1.42) | 0.0276 |
| 2.3 | 1.12 | (0.72–1.75) | |
| 3.3 | 1.21 | (0.76–1.93) | |
| 4.3 | 1.32 | (0.85–2.06) | |
| 5.3 | 1.44 | (0.93–2.22) | |
| 6.3 | 1.56 | (1.00–2.44) | |
| 7.3 | 1.70 | (1.06–2.72) | |
| 8.3 | 1.85 | (1.10–3.10) | |
| 9.3 | 2.01 | (1.13–3.58) | |
| 10.3 | 2.19 | (1.15–4.16) | |
| 11.3 | 2.39 | (1.17–4.87) |
| LTSD | OR | 95% CI | p for Trend |
|---|---|---|---|
| 1.0 | 1.10 | (0.83–1.47) | 0.0369 |
| 2.0 | 1.21 | (0.72–2.05) | |
| 3.0 | 1.33 | (0.73–2.42) | |
| 4.0 | 1.46 | (0.82–2.58) | |
| 5.0 | 1.59 | (0.91–2.76) | |
| 6.0 | 1.75 | (1.00–3.04) | |
| 7.0 | 1.90 | (1.07–3.39) | |
| 8.0 | 2.08 | (1.11–3.88) | |
| 9.0 | 2.27 | (1.15–4.51) | |
| 10.0 | 2.49 | (1.17–5.31) | |
| 11.0 | 2.72 | (1.17–6.31) |
| LTSD | OR | 95% CI | p for Trend |
|---|---|---|---|
| 2.0 | 1.54 | (1.00–2.38) | 0.0062 |
| 3.0 | 1.75 | (1.06–2.89) | |
| 4.0 | 1.85 | (1.14–2.99) | |
| 5.0 | 1.94 | (1.22–3.08) | |
| 6.0 | 2.03 | (1.27–3.24) | |
| 7.0 | 2.13 | (1.30–3.48) | |
| 8.0 | 2.23 | (1.31–3.80) | |
| 9.0 | 2.34 | (1.30–4.21) | |
| 10.0 | 2.45 | (1.28–4.71) | |
| 11.0 | 2.57 | (1.24–5.31) |
| LTSD | OR | 95% CI | p for Trend |
|---|---|---|---|
| 1.7 | 2.02 | (0.94–4.34) | 0.0033 |
| 2.7 | 2.64 | (1.00–6.96) | |
| 3.7 | 3.00 | (1.14–7.88) | |
| 4.7 | 3.31 | (1.31–8.32) | |
| 5.7 | 3.64 | (1.47–8.99) | |
| 6.7 | 4.01 | (1.62–9.97) | |
| 7.7 | 4.42 | (1.73–11.33) | |
| 8.7 | 4.87 | (1.80–13.17) | |
| 9.7 | 5.37 | (1.85–15.60) | |
| 10.7 | 5.92 | (1.87–18.77) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, J.; Ding, C.; Gong, W.; Yuan, F.; Ma, Y.; Feng, G.; Song, C.; Liu, A. The Relationship between Leisure-Time Sedentary Behaviors and Metabolic Risks in Middle-Aged Chinese Women. Int. J. Environ. Res. Public Health 2020, 17, 7171. https://doi.org/10.3390/ijerph17197171
Fan J, Ding C, Gong W, Yuan F, Ma Y, Feng G, Song C, Liu A. The Relationship between Leisure-Time Sedentary Behaviors and Metabolic Risks in Middle-Aged Chinese Women. International Journal of Environmental Research and Public Health. 2020; 17(19):7171. https://doi.org/10.3390/ijerph17197171
Chicago/Turabian StyleFan, Jing, Caicui Ding, Weiyan Gong, Fan Yuan, Yanning Ma, Ganyu Feng, Chao Song, and Ailing Liu. 2020. "The Relationship between Leisure-Time Sedentary Behaviors and Metabolic Risks in Middle-Aged Chinese Women" International Journal of Environmental Research and Public Health 17, no. 19: 7171. https://doi.org/10.3390/ijerph17197171