An Overview of the World Current and Future Assessment of Novel COVID-19 Trajectory, Impact, and Potential Preventive Strategies at Healthcare Settings

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
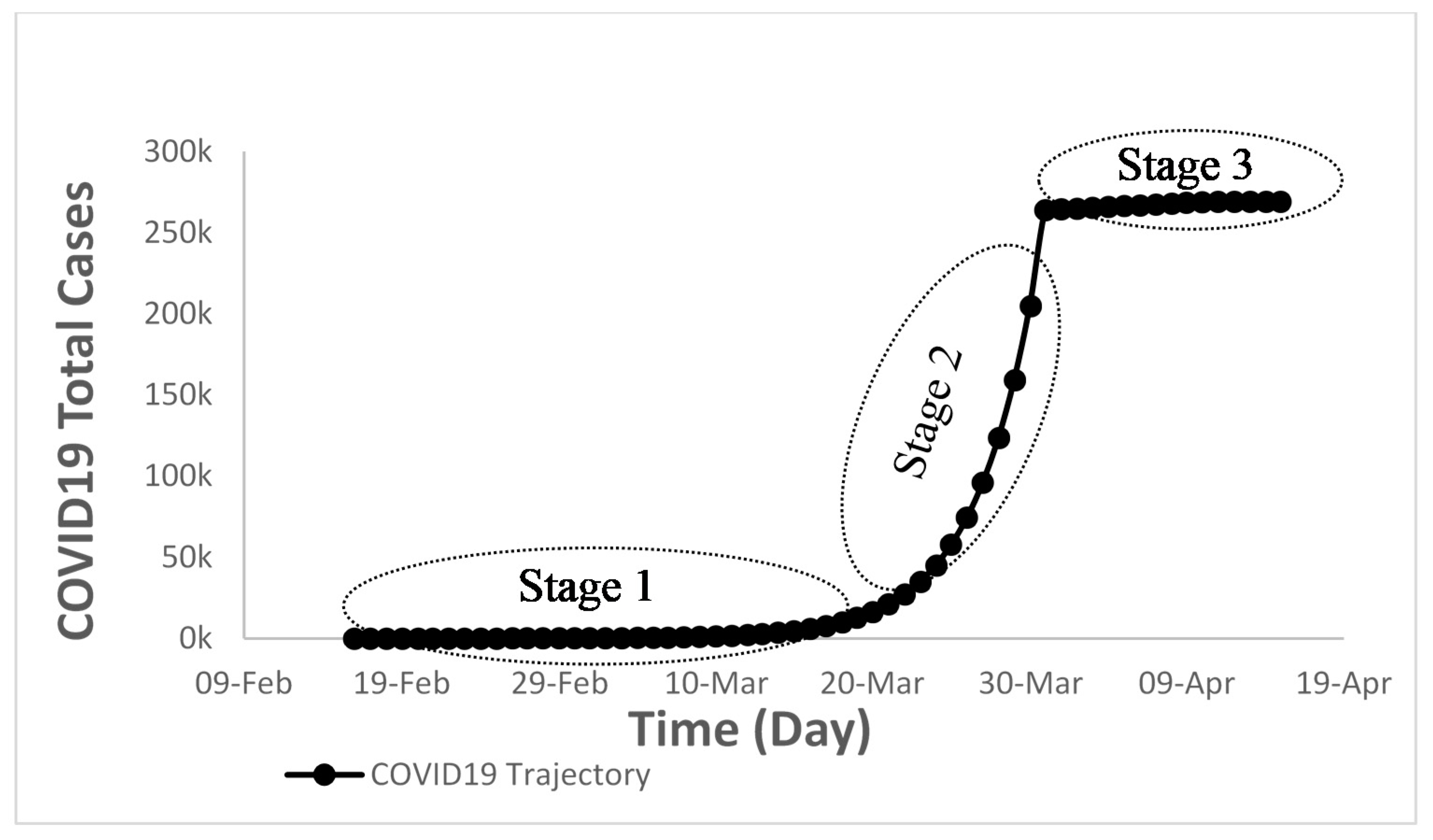
3.1. Actual Data of New Cases
3.2. Reported Deaths
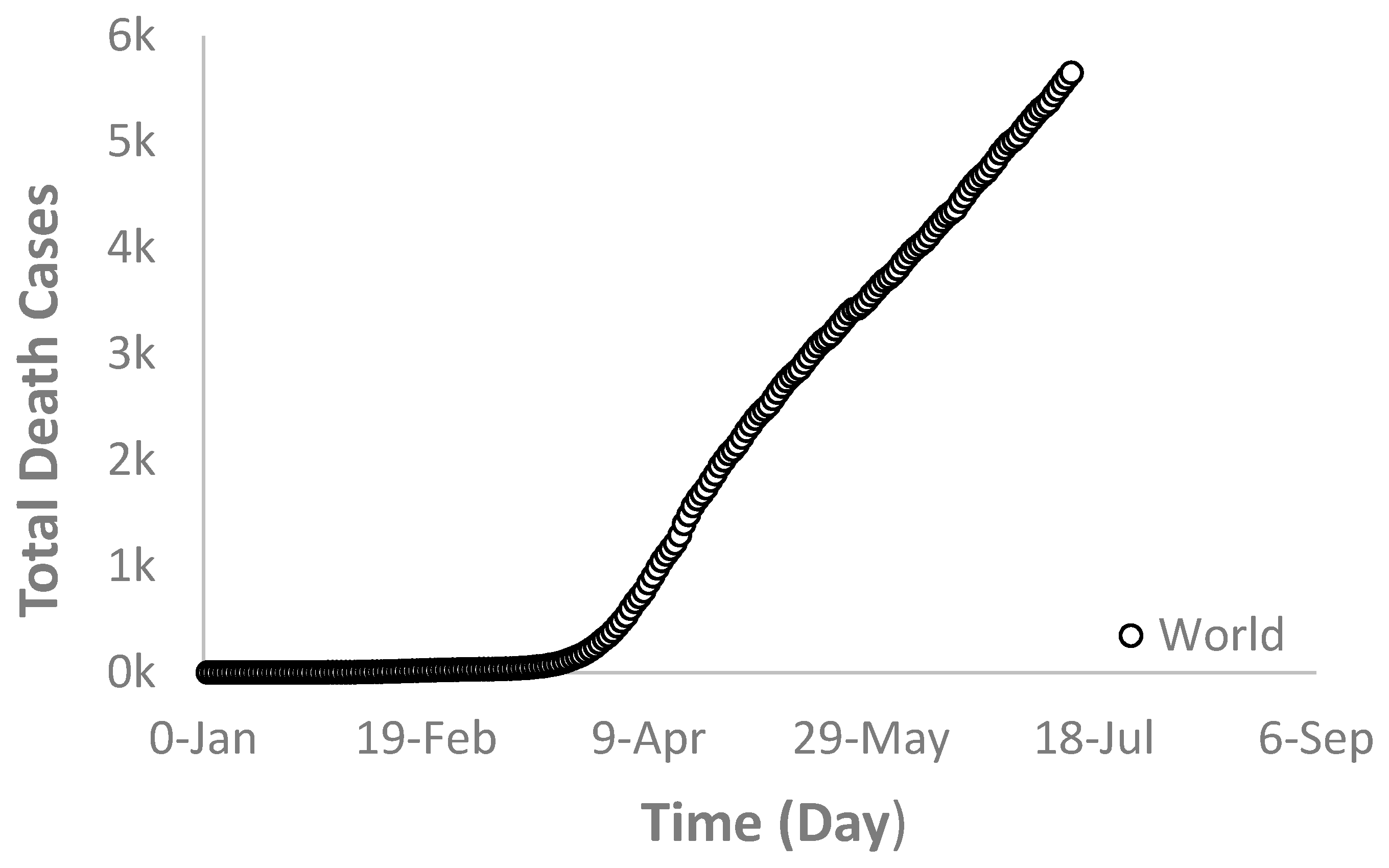
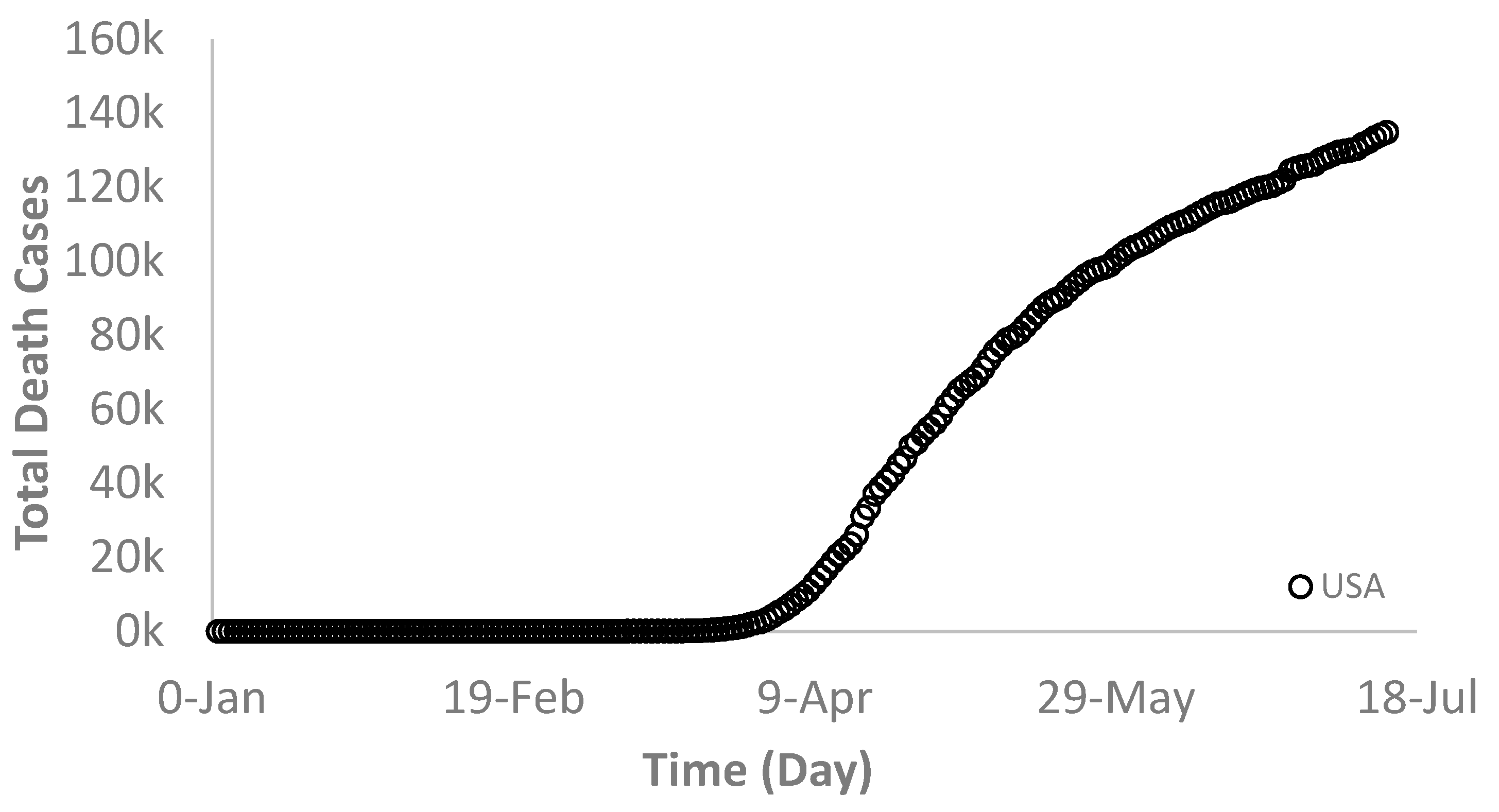
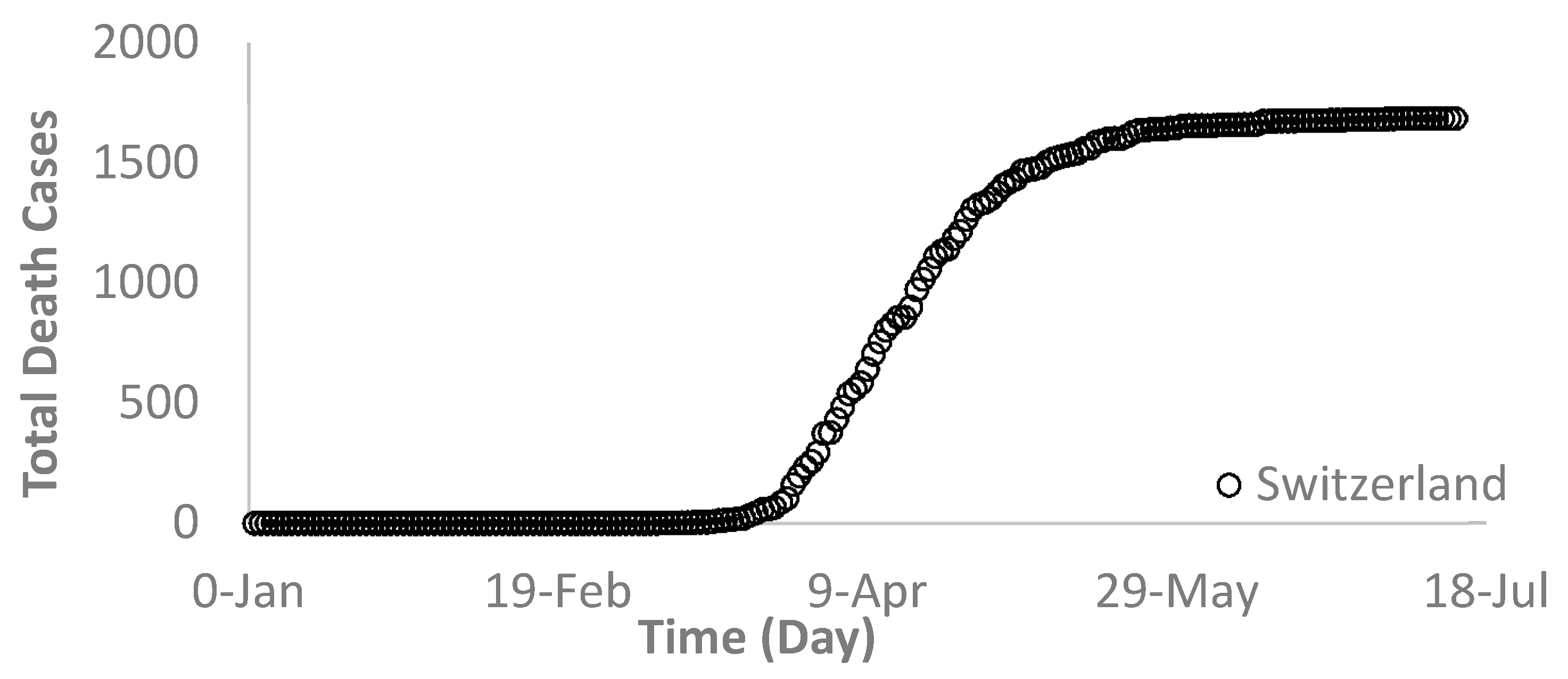
3.2.1. Total Deaths
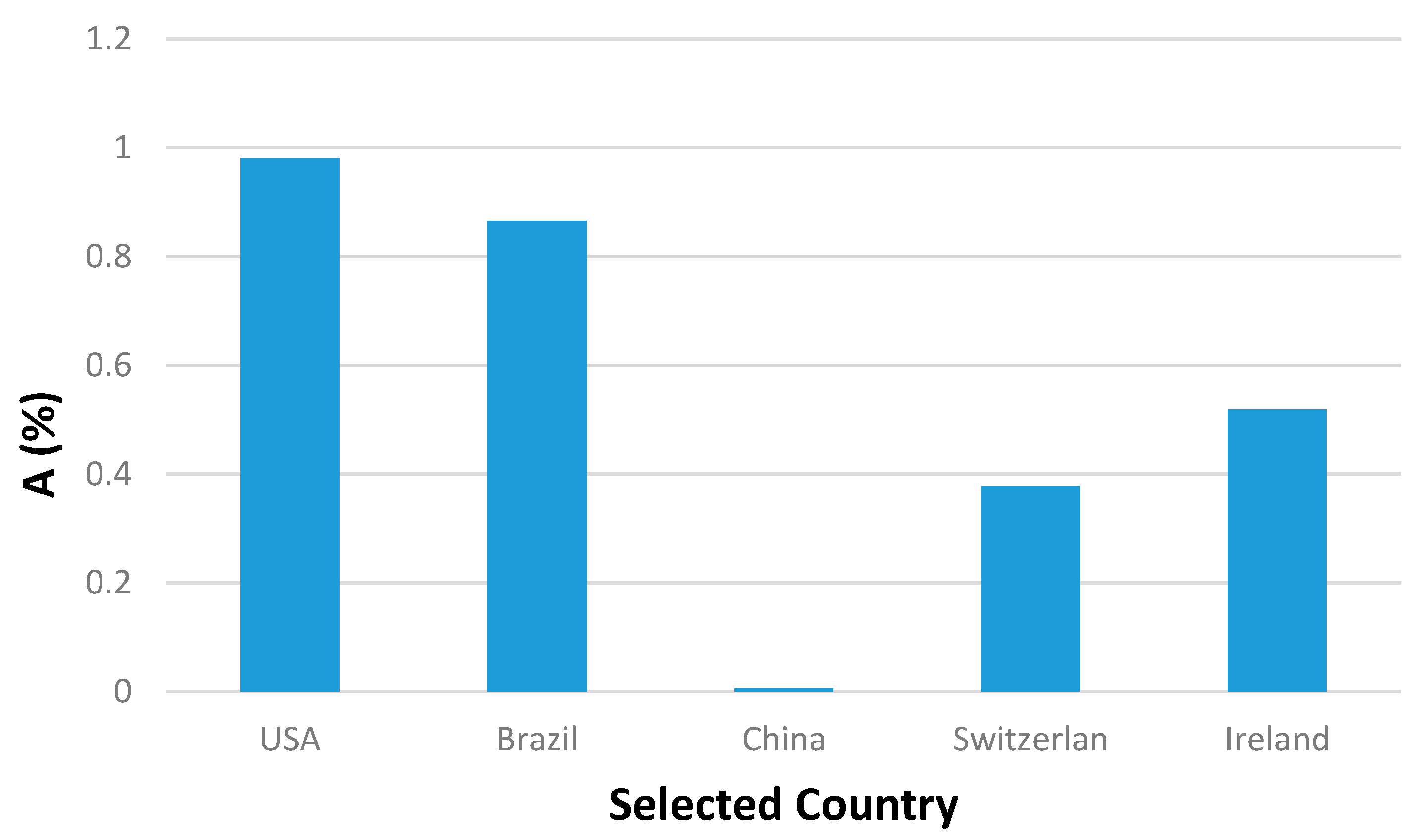
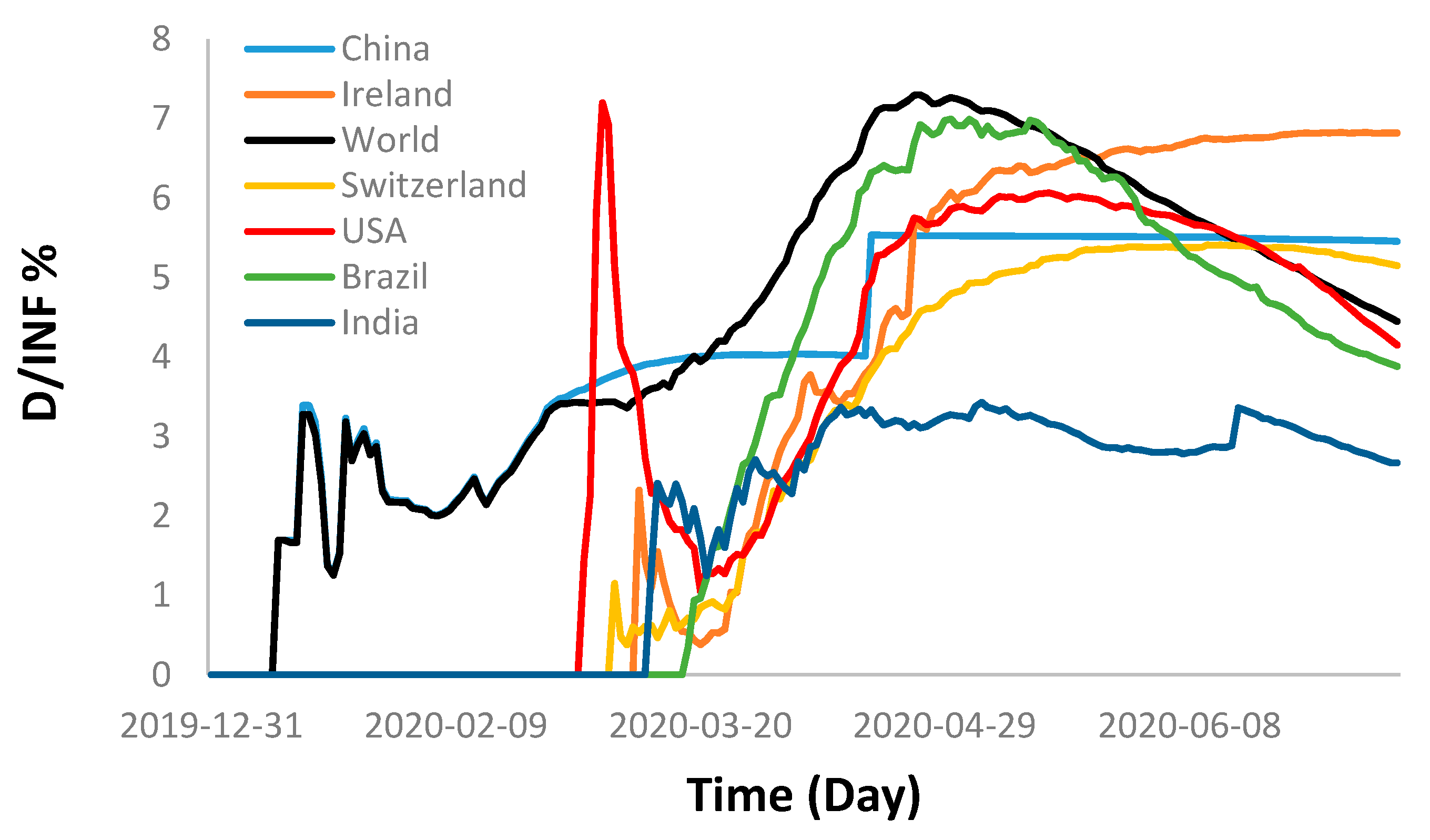
3.2.2. Death Percentage
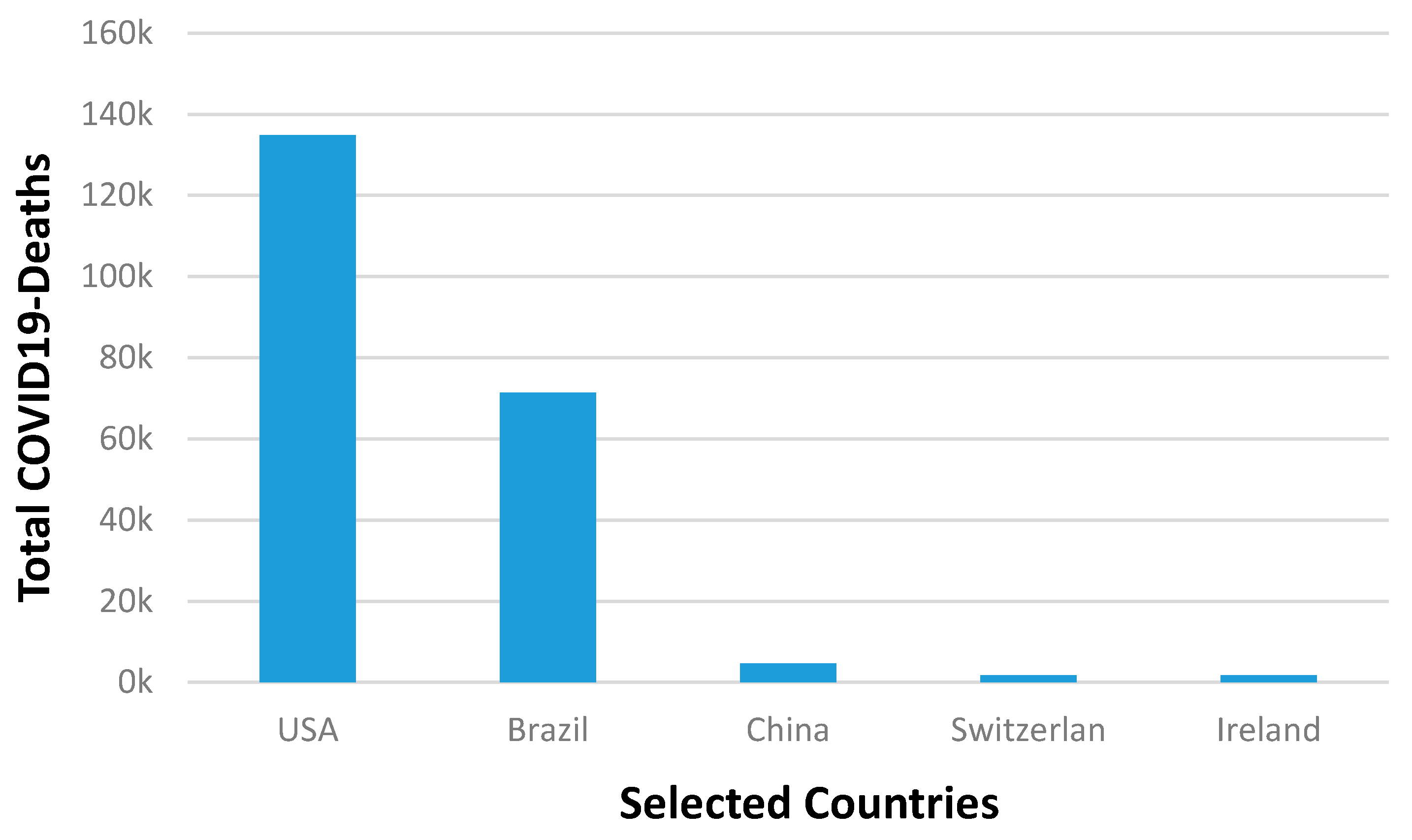
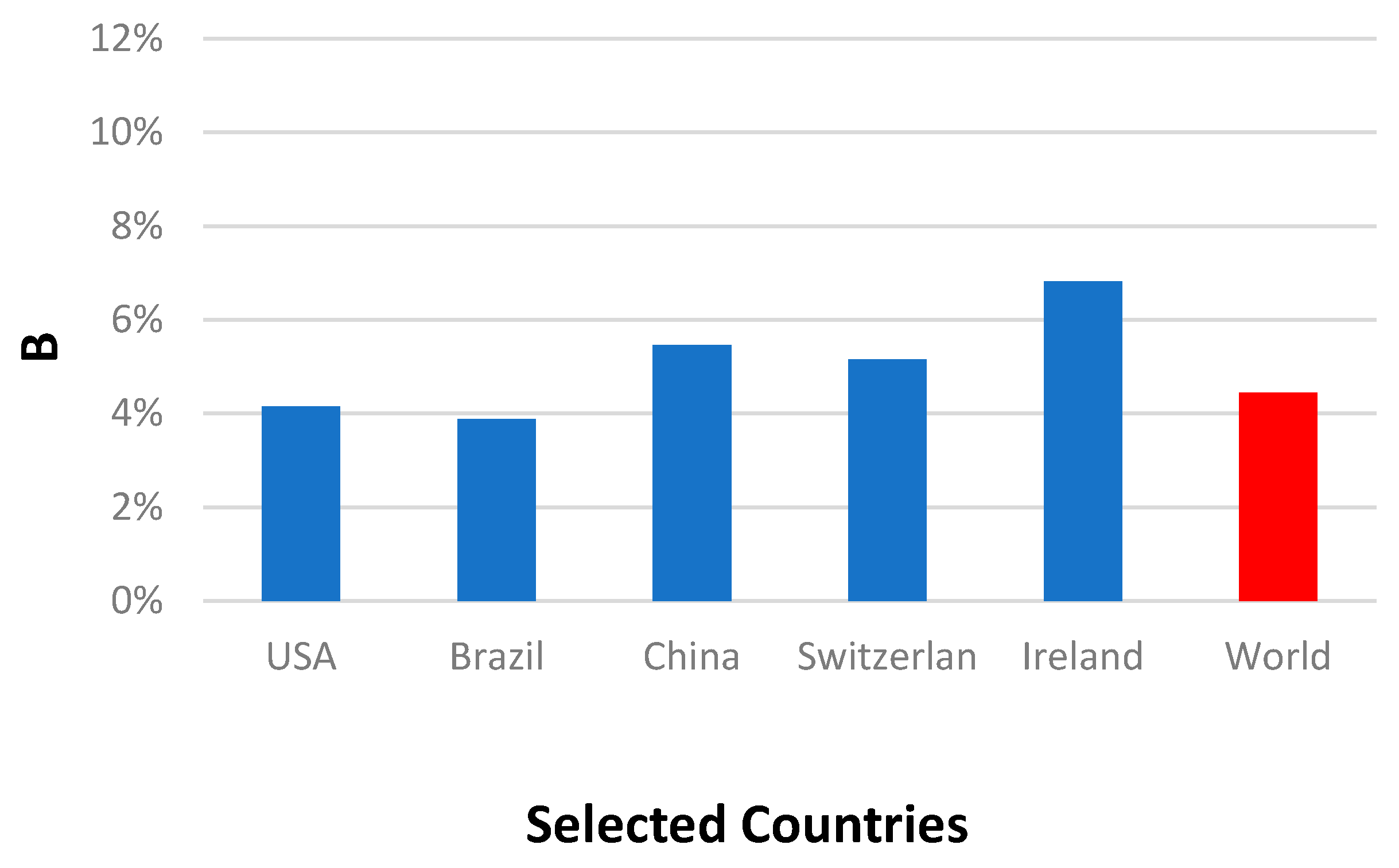
3.2.3. Novel COVID-19 Death Percentages Comparison
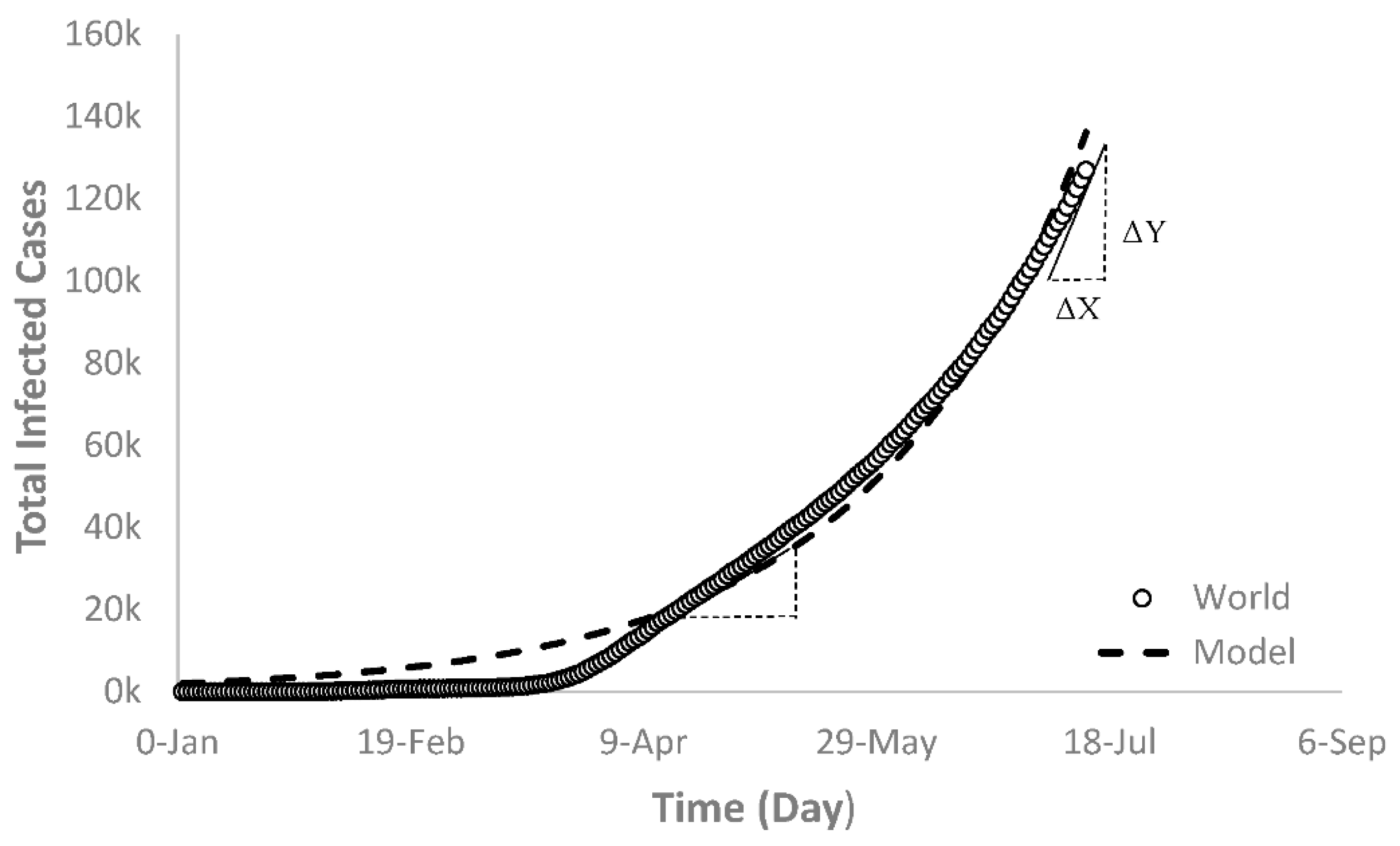
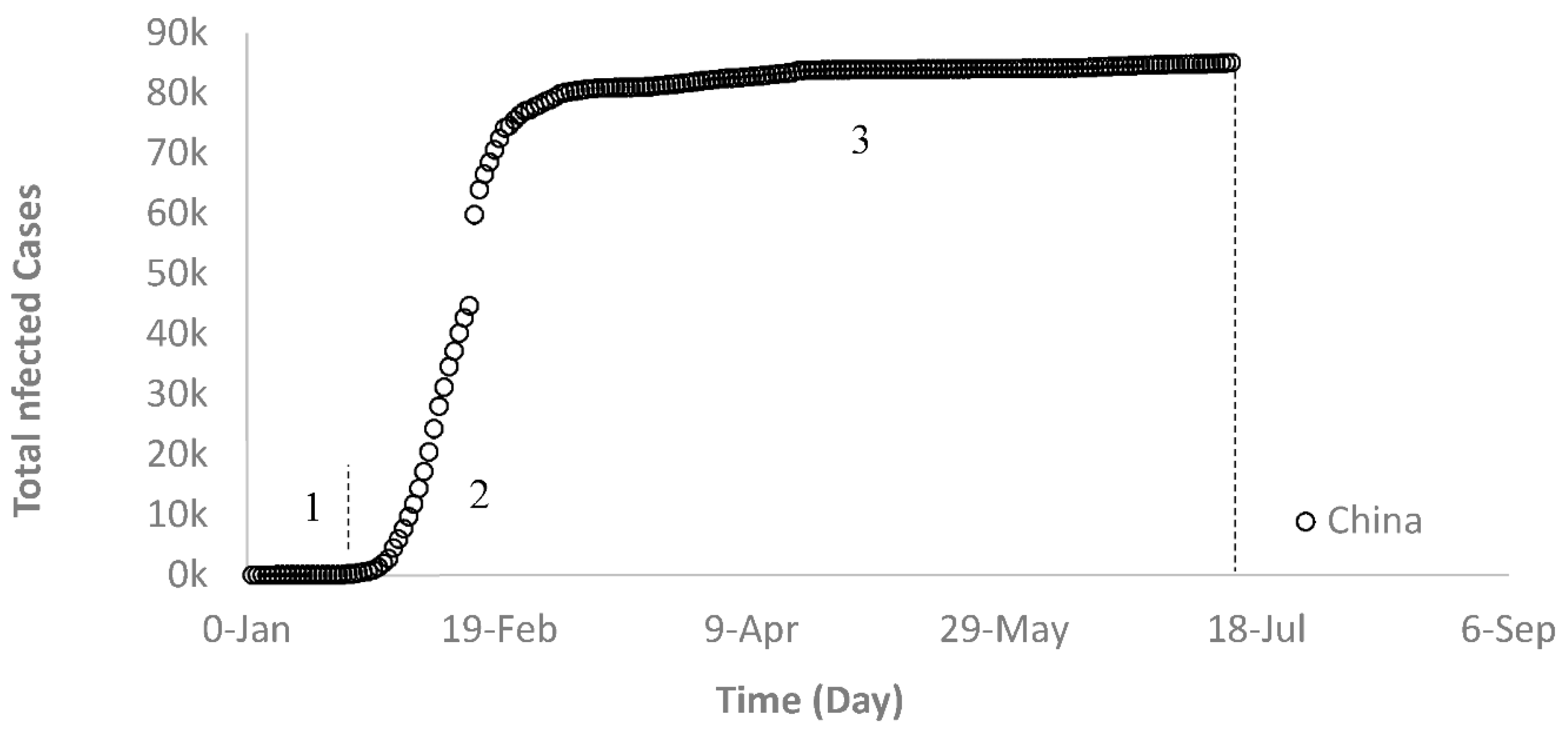
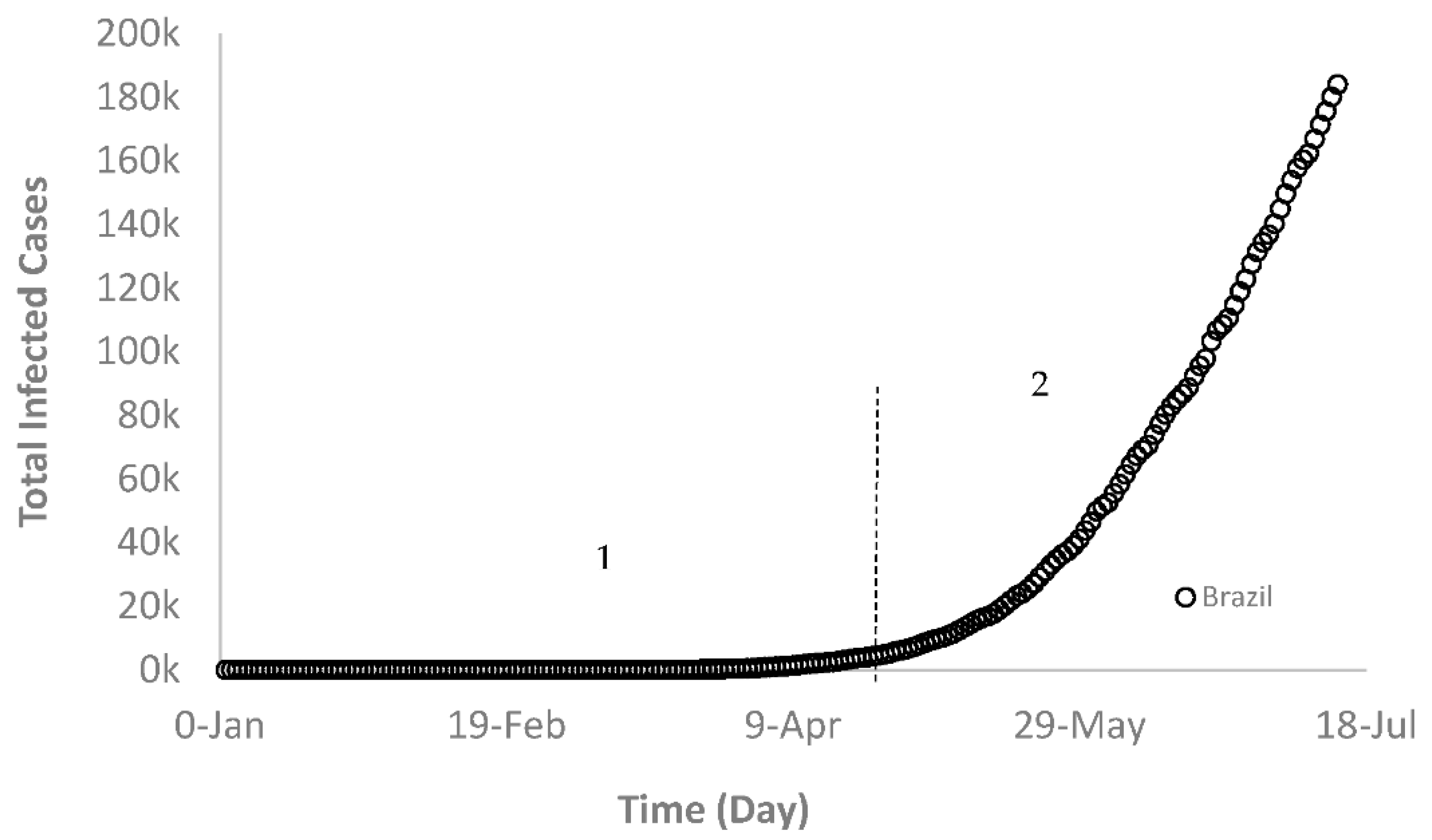
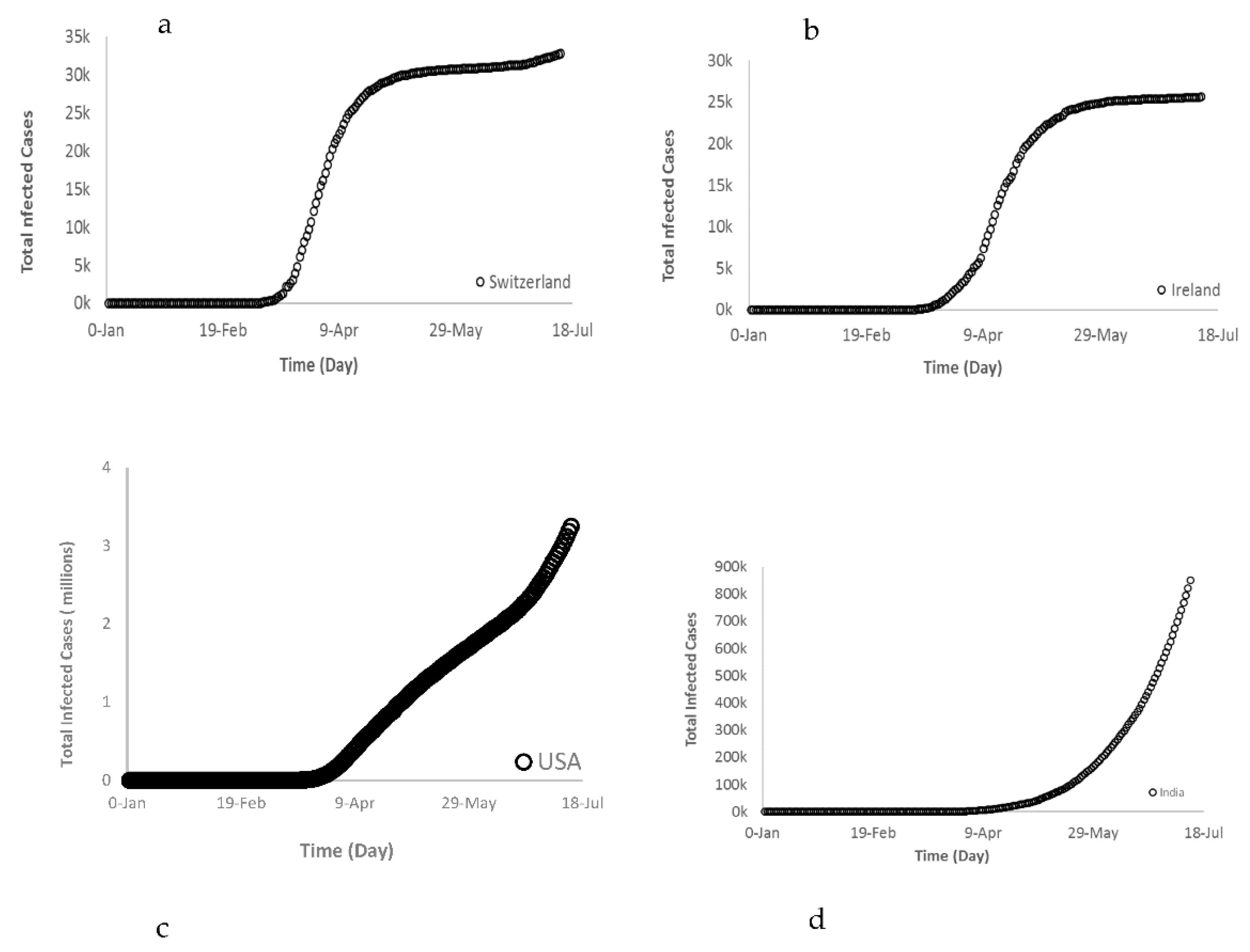
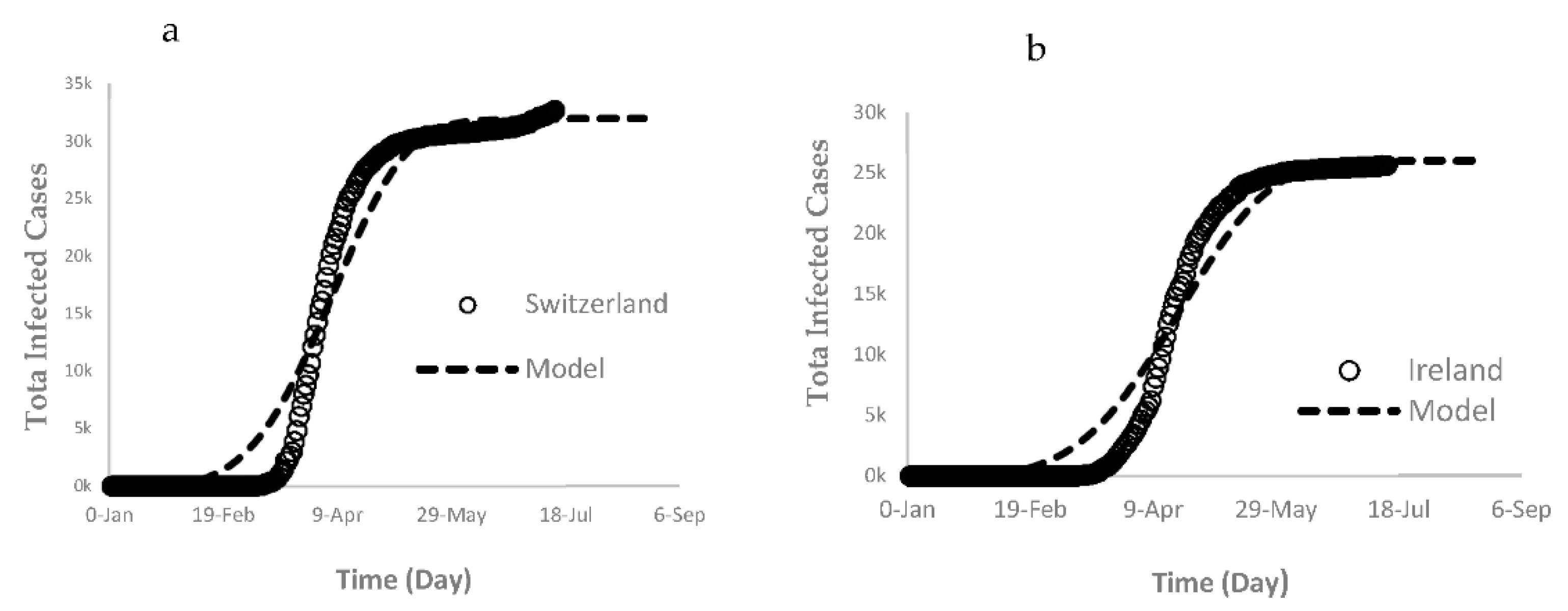
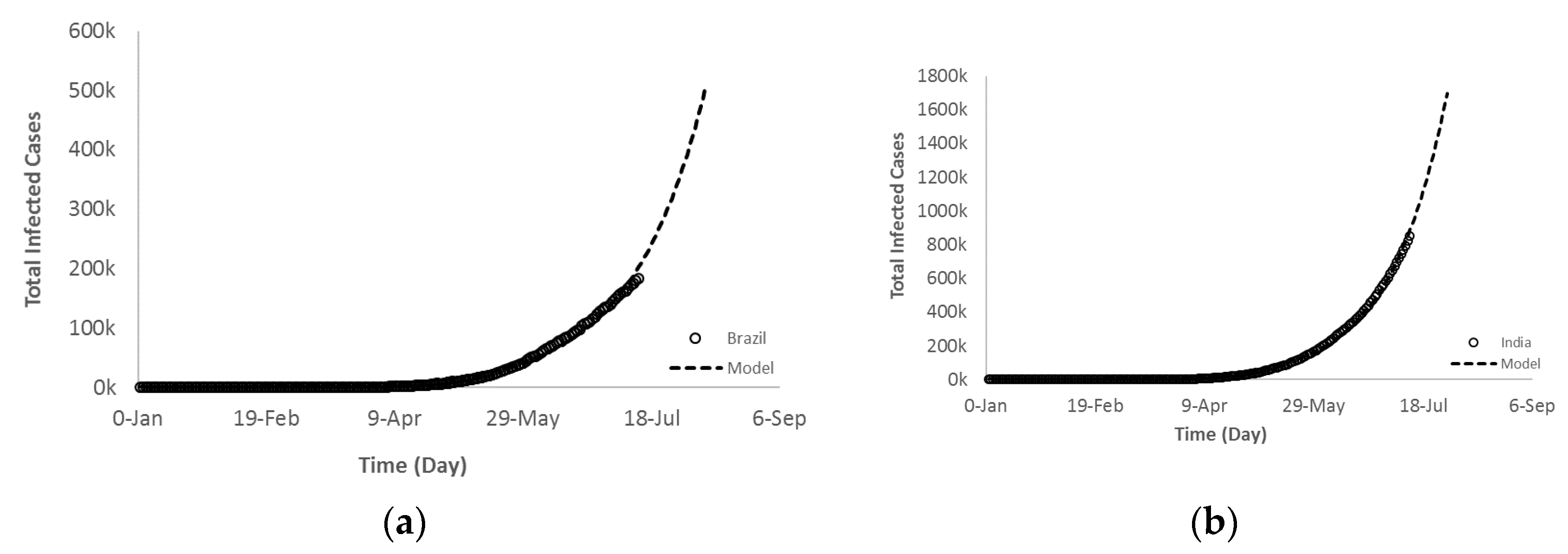
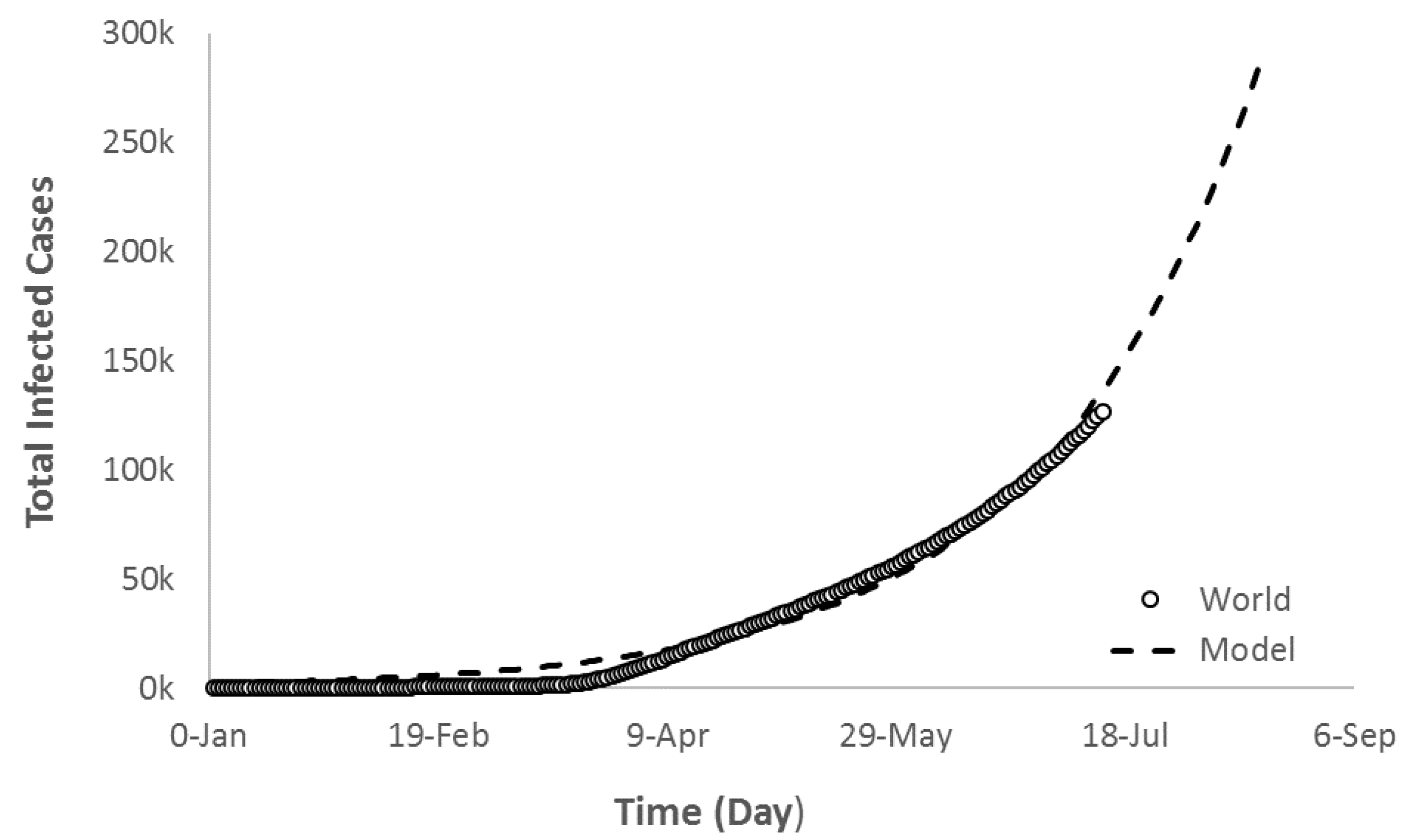
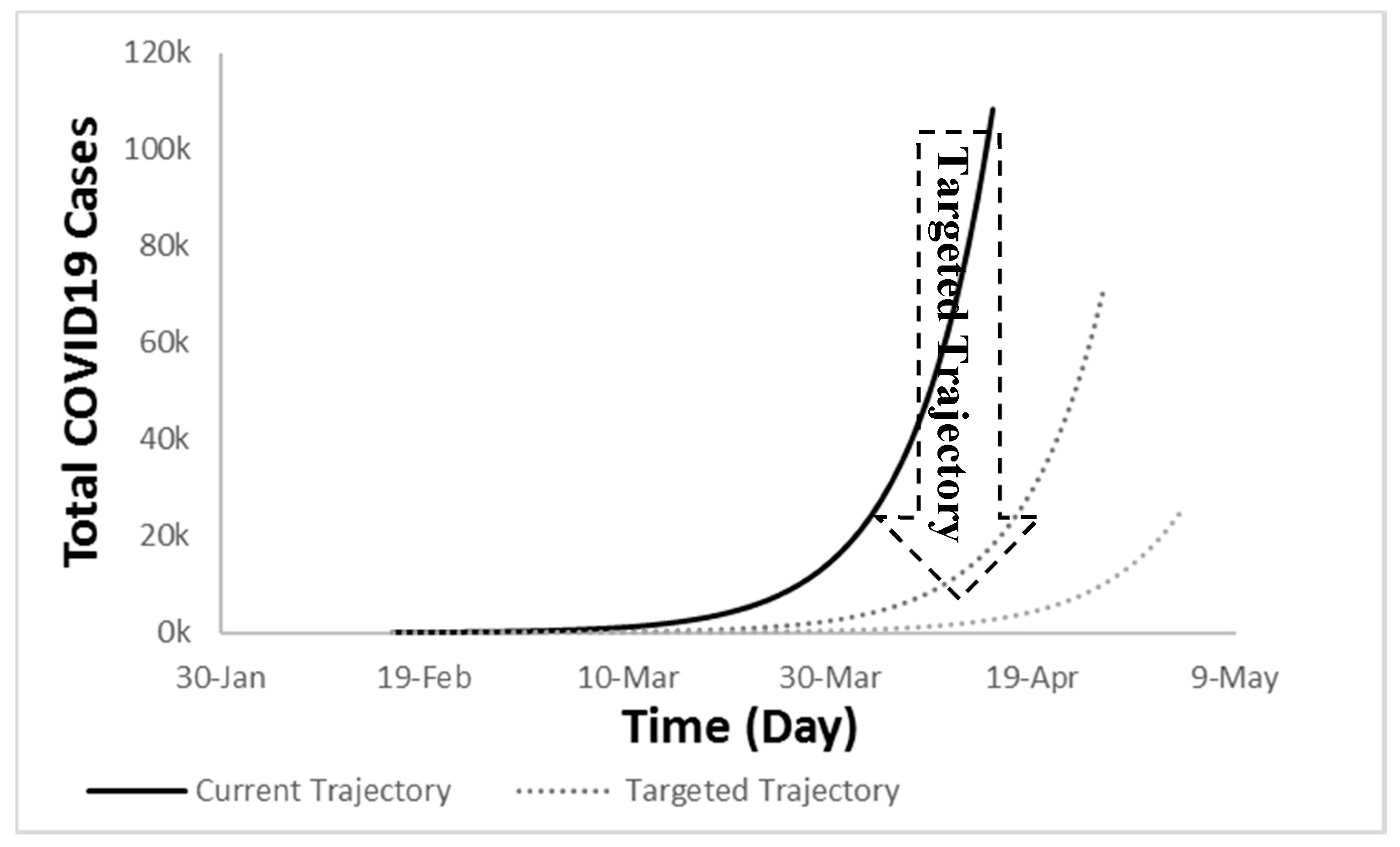
3.3. COVID-19 Future Regression-Based Trajectory
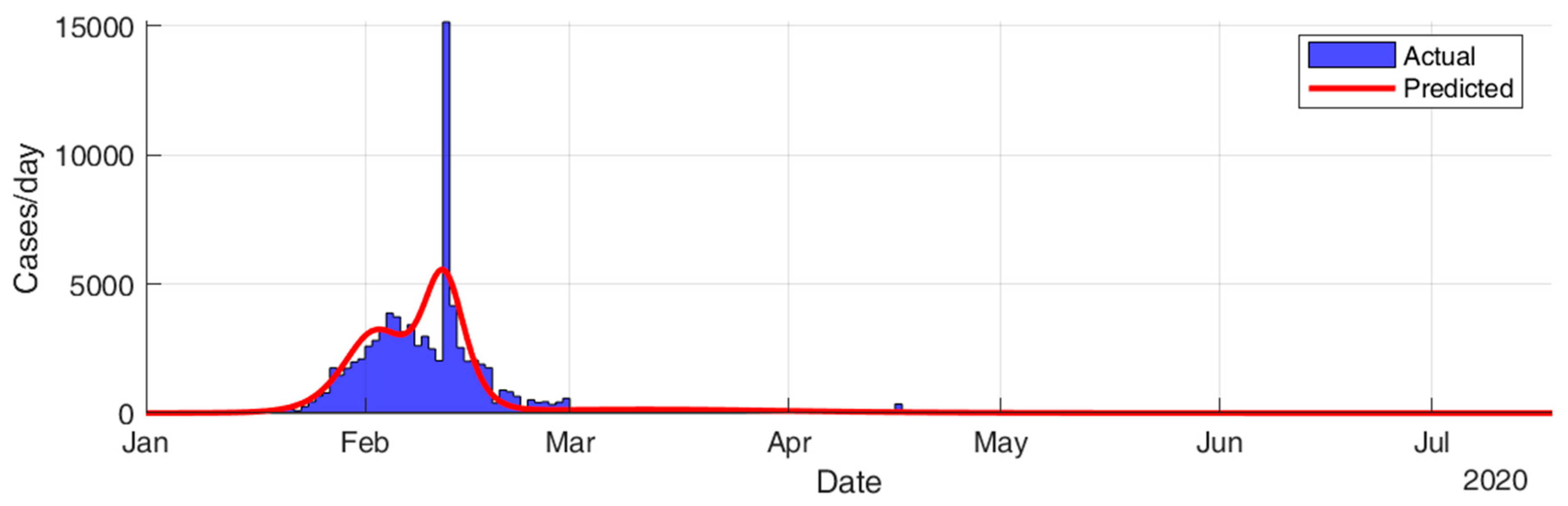
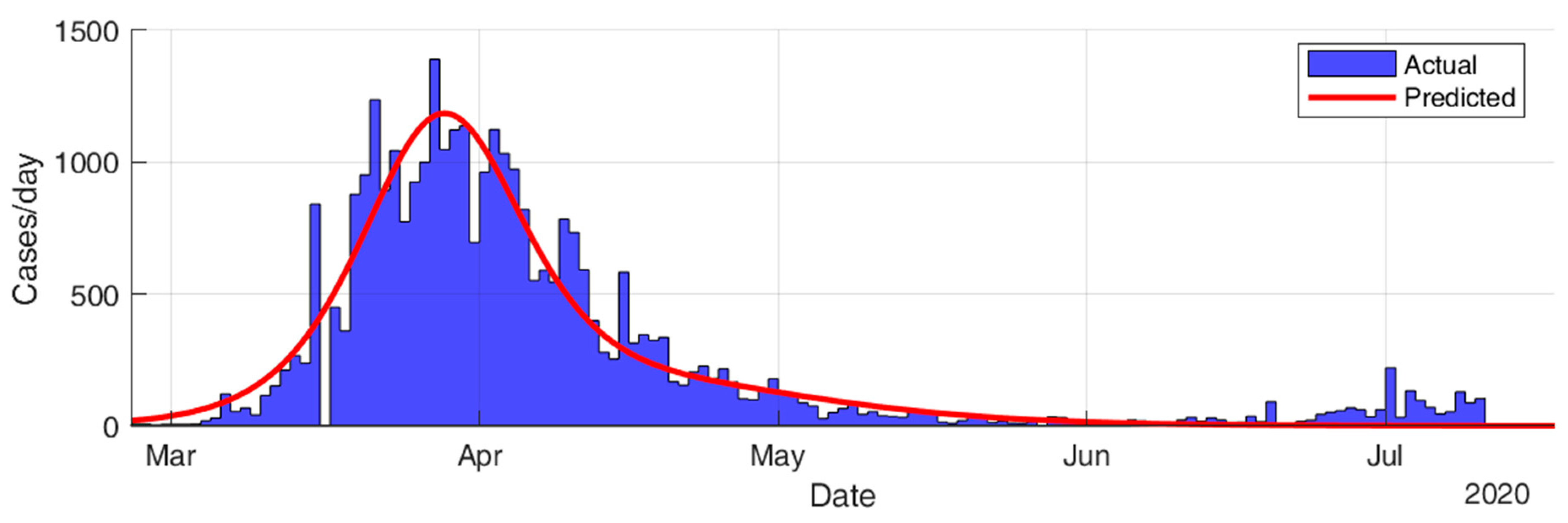
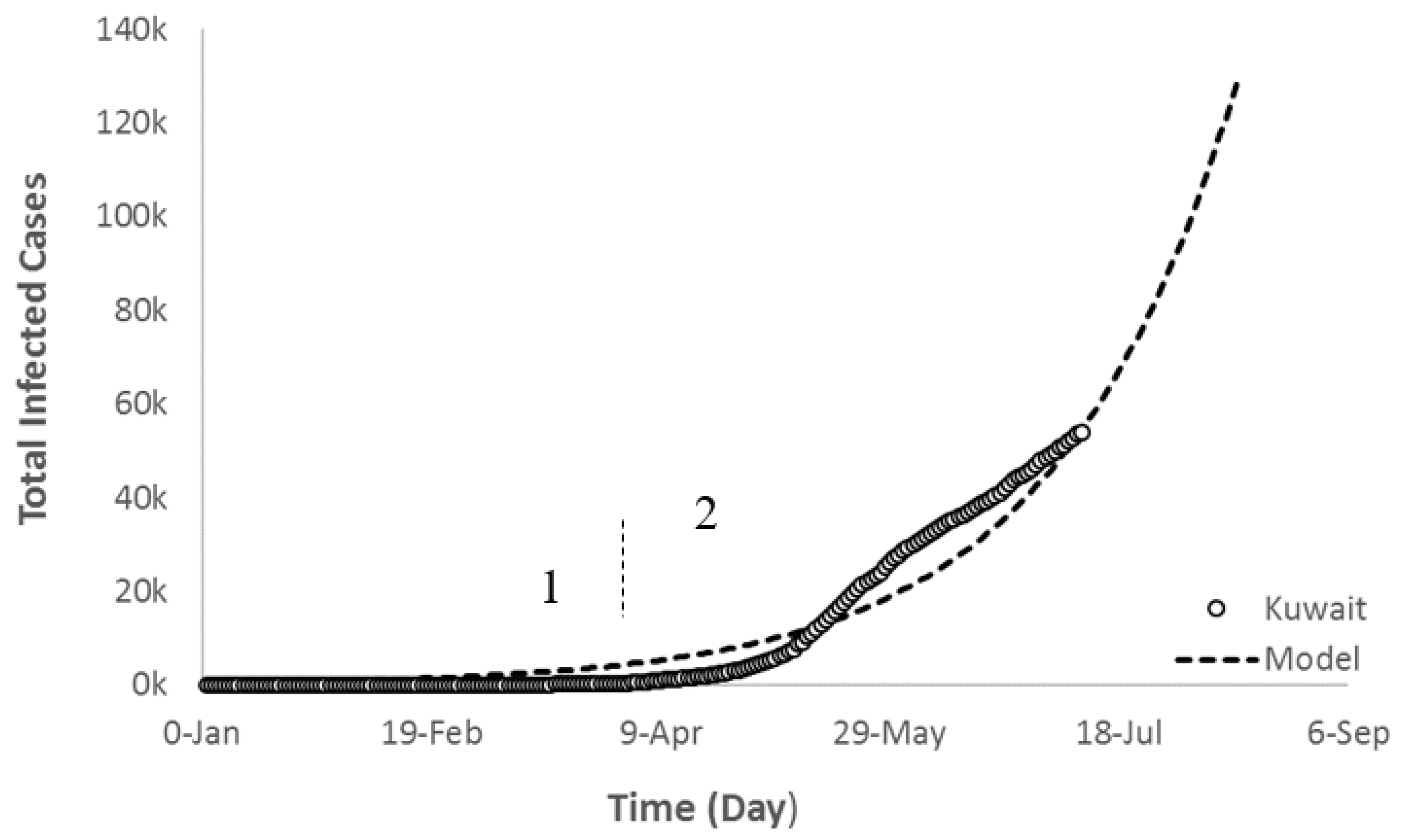
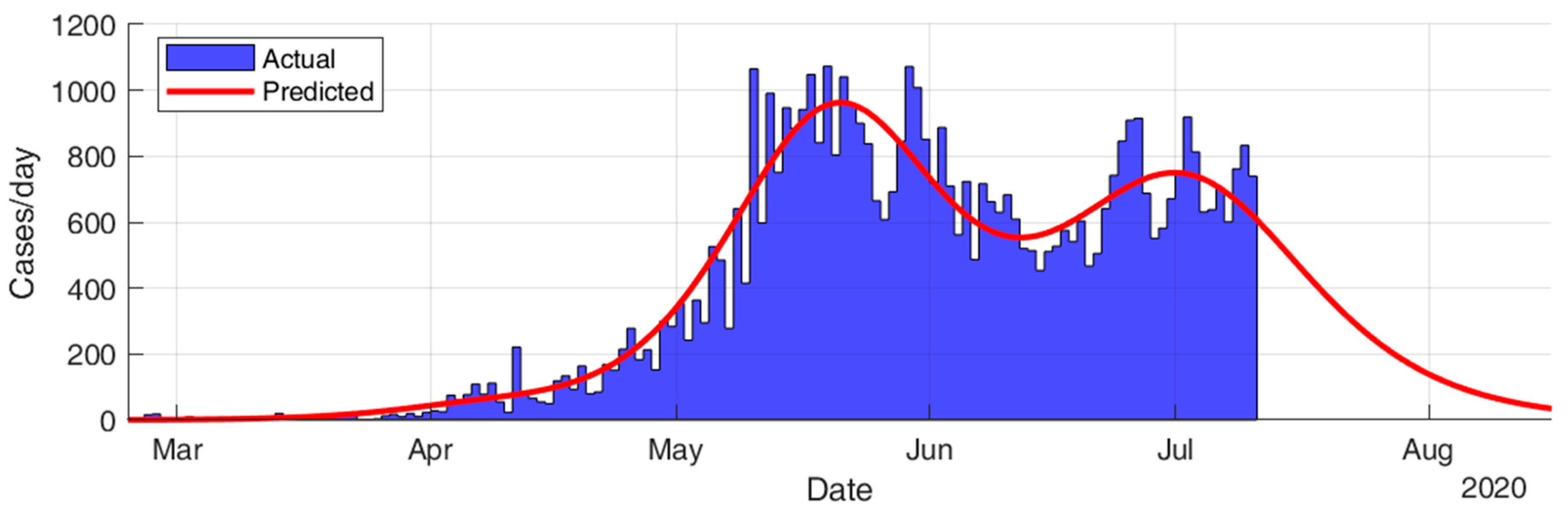
3.4. COVID-19 Future SIR-Based Trajectory
3.5. Local COVID-19 Study
4. Potential Prevention/Containment Strategies
4.1. Development of Biodegradable Antiviral Masks
4.2. Antiviral Nano-Coatings of Surfaces
5. Conclusions and Recommendations
Author Contributions
Funding
Conflicts of Interest
References
- Zappa, A.; Amendola, A.; Romanò, L.; Zanetti, A. Emerging and re-emerging viruses in the era of globalization. Blood Transfus. 2009, 7, 167–171. [Google Scholar] [PubMed]
- Visualizing the History of Pandemics, Visual Capitalist. Available online: https://www.visualcapitalist.com/history-of-pandemics-deadliest/ (accessed on 30 March 2020).
- Edwards, P.; Hannover, R.E. Epidemics: Past, Present and Future—What are the Risks? 2017. Available online: https://www.hannover-rueck.de/1085858/recent-medical-news-epidemics-2017.pdf (accessed on 30 March 2020).
- Rappuoli, R. From Pasteur to genomics: Progress and challenges in infectious diseases. Nat. Med. 2004, 10, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Benfield, E.; Treat, J. As Ebola Death Toll Rises, Remembering History’s Worst Epidemics. National Geographic. Available online: https://www.nationalgeographic.com/news/2014/10/141025-ebola-epidemic-perspective-history-pandemic/ (accessed on 30 March 2020).
- COVID-19. Coronavirus Outbreak. World Meters. 2020. Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 7 March 2020).
- Kiran, T.N.R.; Latha, A.V.S.M.; Sureshkumar, J.N.; Reddy, E.S. Novel Coronavirus. Res. J. Pharmacol. Pharmacodyn. 2020, 12, 64. [Google Scholar] [CrossRef]
- Madigan, M.T.; Martino, J.M.; Bender, K.S.; Buckley, D.H. Brock Biology of Microorganisms-Microbiology, 14th ed.; David, A., Ed.; Pearson: London, UK, 2006. [Google Scholar]
- Fehr, A.R.; Perlman, S. Coronaviruses: An Overview of Their Replication and Pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar]
- Li, F. Structure, Function, and Evolution of Coronavirus Spike Proteins. Annu. Rev. Virol. 2016, 3, 237–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholls, J.M.; Poon, L.L.M.; Lee, K.C.; Ng, W.F.; Lai, S.T.; Leung, C.Y.; Chu, C.; Hui, P.K.; Mak, K.L.; Lim, W.; et al. Lung pathology of fatal severe acute respiratory syndrome. Lancet 2003, 361, 1773–1778. [Google Scholar] [CrossRef] [Green Version]
- Woo, P.C.Y.; Lau, S.K.P.; Chu, C.; Chan, K.-H.; Tsoi, H.-W.; Huang, Y.; Wong, B.H.L.; Poon, R.W.S.; Cai, J.J.; Luk, W.-K.; et al. Characterization and Complete Genome Sequence of a Novel Coronavirus, Coronavirus HKU1, from Patients with Pneumonia. J. Virol. 2005, 79, 884–895. [Google Scholar] [CrossRef] [Green Version]
- Parry, J. WHO investigates China’s fall in SARS cases. BMJ Br. Med. J. 2003, 326, 1285. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Napoli, R.D. Features, Evaluation and Treatment Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Zhang, N.; Li, Y. Transmission of Influenza A in a Student Office Based on Realistic Person-to-Person Contact and Surface Touch Behaviour. Int. J. Environ. Res. Public Health 2018, 15, 1699. [Google Scholar] [CrossRef] [Green Version]
- Corona Virus Diseases 2019 (COVID 19) Situation Report 60. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200320-sitrep-60-covid-19.pdf?sfvrsn=d2bb4f1f_2 (accessed on 20 March 2020).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y. Early transmission dynamics in Wuhan, China, of novel corona virus infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Lin, Q.; Ran, J.; Musa, S.S.; Yang, G.; Wang, W.; Lou, Y.; Gao, D.; Yang, L.; He, D.; et al. Preliminary estimation of the basic reproduction number of novelcoronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int. J. Infect. Dis. 2020, 92, 214–217. [Google Scholar] [CrossRef] [Green Version]
- Iwata, K.; Miyakoshi, C. A Simulation on Potential Secondary Spread of Novel Coronavirus in an Exported Country Using a Stochastic Epidemic SEIR Model. J. Clin. Med. 2020, 9, 944. [Google Scholar] [CrossRef] [Green Version]
- Kuniya, T. Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020. J. Clin. Med. 2020, 9, 789. [Google Scholar] [CrossRef] [Green Version]
- Al-Qaness, M.A.; Ewees, A.A.; Fan, H.; Elaziz, M.A. Optimization Method for Forecasting Confirmed Cases of COVID-19 in China. J. Clin. Med. 2020, 9, 674. [Google Scholar] [CrossRef] [Green Version]
- Roosa, K.; Lee, Y.; Luo, R.; Kirpich, A.; Rothenberg, R.; Hyman, J.M.; Yan, P.; Chowell, G. Short-term Forecasts of the COVID-19 Epidemic in Guangdong and Zhejiang, China: February 13–23, 2020. J. Clin. Med. 2020, 9, 596. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.-M.; Akhmetzhanov, A.R.; Hayashi, K.; Linton, N.M.; Yang, Y.; Yuan, B.; Kobayashi, T.; Kinoshita, R.; Nishiura, H. Real-Time Estimation of the Risk of Death from Novel Coronavirus (COVID-19) Infection: Inference Using Exported Cases. J. Clin. Med. 2020, 9, 523. [Google Scholar] [CrossRef] [Green Version]
- Hethcote, H.W. The Mathematics of Infectious Diseases. SIAM Rev. 2000, 42, 599–653. [Google Scholar] [CrossRef] [Green Version]
- Batista, M. fitVirusXX. MATLAB Central File Exchange. Available online: https://www.mathworks.com/matlabcentral/fileexchange/76956-fitvirusxx (accessed on 24 September 2020).
- Batista, M. Estimation of the Final Size of the Coronavirus Epidemic by the SIR Model. Available online: https://www.researchgate.net/publication/339311383 (accessed on 20 February 2020).
- Current World Population, World Meters. Available online: https://www.worldometers.info/world-population/ (accessed on 25 March 2020).
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.; Xu, H.; Rebaza, A.; Sharma, L.; Cruz, C.S.D. Protecting health-care workers from subclinical coronavirus infection. Lancet Respir. Med. 2020, 8, e13. [Google Scholar] [CrossRef] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Tuladhar, E.; Hazeleger, W.C.; Koopmans, M.; Zwietering, M.H.; Beumer, R.R.; Duizer, E. Residual Viral and Bacterial Contamination of Surfaces after Cleaning and Disinfection. Appl. Environ. Microbiol. 2012, 78, 7769–7775. [Google Scholar] [CrossRef] [Green Version]

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| What | When | Where | Deaths |
|---|---|---|---|
| Black Death | 1347–1351 | Europe | 50,000,000 |
| HIV | 1980 | Global | 39,000,000 |
| Spanish Flu | 1918–1920 | Global | 20,000,000 |
| Asian Flu | 1957–1961 | Global | 2,000,000 |
| Seventh cholera pandemic | 1961 | Global | 570,000 |
| Swine Flu | 2009 | Global | 284,000 |
| Ebola | 2014 | West Africa | 4877 |
| Measles | 2011 | Congo | 4555 |
| SARS | 2002–2003 | Global | 774 |
| Group A: Controlled | Croup B: Uncontrolled | ||||
|---|---|---|---|---|---|
| Country | Total Infected | Total Deaths | Country | Total Infected | Total Deaths |
| China | 85,071 | 4641 | USA | 3,247,684 | 134,814 |
| Switzerland | 32,713 | 1685 | Brazil | 1,839,850 | 71,469 |
| Ireland | 25,611 | 1746 | India | 849,553 | 22,674 |
| Coefficient | M | k | n | r2 | |
|---|---|---|---|---|---|
| Country | |||||
| Switzerland | 31,962.5 | 5.0 × 10−9 | 4.1 | 0.99 | |
| Ireland | 26,000 | 3.7 × 10−9 | 4.1 | 0.97 | |
| Country | F | R | r2 |
|---|---|---|---|
| Brazil | 316 | 29 | 0.99 |
| India | 247 | 26 | 0.997 |
| USA | 1300 | 78 | 0.97 |
| Group | Country | Expected Number Of Cases | Expected 97% End of Pandemic | Expected 99% End of Pandemic |
|---|---|---|---|---|
| A | China | 84,294 | 21-March-20 | 9-April-20 |
| Switzerland | 31,376 | 11-May-20 | 25-May-20 | |
| Ireland | 25,486 | 25-May-20 | 7-June-20 | |
| B | USA | 4,007,934 | 6-August-20 | 18-August-20 |
| Brazil | 2,339,875 | 3-August-20 | 14-August-20 | |
| India | 1,305,506 | 10-August-20 | 22-August-20 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Anzi, B.S.; Alenizi, M.; Al Dallal, J.; Abookleesh, F.L.; Ullah, A. An Overview of the World Current and Future Assessment of Novel COVID-19 Trajectory, Impact, and Potential Preventive Strategies at Healthcare Settings. Int. J. Environ. Res. Public Health 2020, 17, 7016. https://doi.org/10.3390/ijerph17197016
Al-Anzi BS, Alenizi M, Al Dallal J, Abookleesh FL, Ullah A. An Overview of the World Current and Future Assessment of Novel COVID-19 Trajectory, Impact, and Potential Preventive Strategies at Healthcare Settings. International Journal of Environmental Research and Public Health. 2020; 17(19):7016. https://doi.org/10.3390/ijerph17197016
Chicago/Turabian StyleAl-Anzi, Bader S., Mohammad Alenizi, Jehad Al Dallal, Frage Lhadi Abookleesh, and Aman Ullah. 2020. "An Overview of the World Current and Future Assessment of Novel COVID-19 Trajectory, Impact, and Potential Preventive Strategies at Healthcare Settings" International Journal of Environmental Research and Public Health 17, no. 19: 7016. https://doi.org/10.3390/ijerph17197016