The Analysis of the Frequency of Leukoplakia in Reference of Tobacco Smoking among Northern Polish Population

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Methods
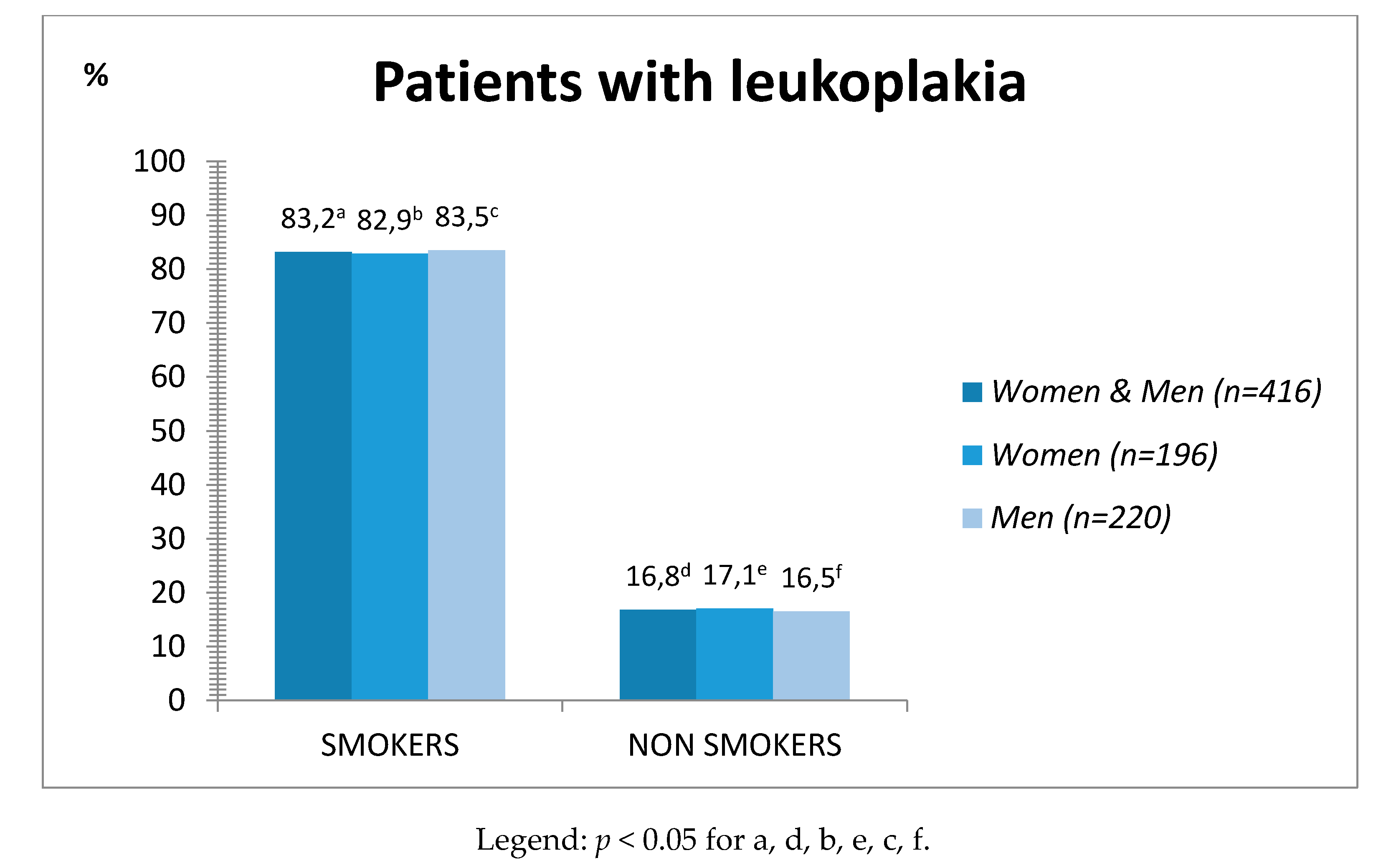
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Carrard, V.; Haas, A.N.; Rados, P.V.; Filho, M.; Oppermann, R.; Albandar, J.M.; Susin, C. Prevalence and risk indicators of oral mucosal lesions in an urban population from South Brazil. Oral Dis. 2011, 17, 171–179. [Google Scholar] [CrossRef]
- Vallejo, M.J.G.-P.; Diaz-Canel, A.I.M.; Garcia-Martin, J.M.; García, M.G. Risk factors for oral soft tissue lesions in an adult Spanish population. Community Dent. Oral Epidemiol. 2002, 30, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Pentenero, M.; Broccoletti, R.; Carbone, M.; Conrotto, D.; Gandolfo, S. The prevalence of oral mucosal lesions in adults from the Turin area. Oral Dis. 2008, 14, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Petkowicz, B.; Skiba, M.; Tomaszewski, T.; Wysokińska-Miszczuk, J. Leukoplakia in Clinical and Epidemiological Aspect—Analysis of Cases. Dent. Med. Probl. 2004, 41, 635–641. [Google Scholar]
- Scully, C. Oral and Maxillofacial Medicine the Basis of Diagnosis and Treatment, 3rd ed.; Elsevier: London, UK, 2013; pp. 186–191. [Google Scholar]
- Warnakulasuriya, S.; Johnson, N.W.; Van Der Waal, I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J. Oral Pathol. Med. 2007, 36, 575–580. [Google Scholar] [CrossRef]
- Petti, S. Pooled estimate of world leukoplakia prevalence: A systematic review. Oral Oncol. 2003, 39, 770–780. [Google Scholar] [CrossRef]
- Harris, C.K.; Warnakulasuriya, S.; Cooper, D.J.; Peters, T.J.; Gelbier, S. Prevalence of oral mucosal lesions in alcohol misusers in south London. J. Oral Pathol. Med. 2004, 33, 253–259. [Google Scholar] [CrossRef]
- Ker, A.R.; Sirois, D.A.; Epstein, J.B. Clinical evaluation of chemiluminescent lighting—An adjunct for oral mucosal examinations. J. Clin. Dent. 2006, 17, 59–63. [Google Scholar]
- Kovac-Kovacic, M.; Skaleric, U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. J. Oral Pathol. Med. 2000, 29, 331–335. [Google Scholar] [CrossRef]
- O’Sullivan, E.M. Prevalence of oral mucosal abnormalities in addiction treatment centrereidents in Southern Ireland. Oral Oncol. 2011, 47, 395–399. [Google Scholar] [CrossRef]
- Rooban, T.; Rao, A.; Joshua, E.; Ranganathan, K. The prevalence of oral mucosal lesions in alcohol misusers in Chennai, south India. Indian J. Dent. Res. 2009, 20, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Taiwo, J.O.; Kolude, B.; Akinmoladun, V. Oral mucosal lesions and temporomandibular joint impairment of eldery people in the South East Local Government Area of Ibadan. Gerodontology 2009, 26, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Dietrich, T.; Bornstein, M.M.; Peidró, E.C.; Preshaw, P.M.; Walter, C.; Wennström, J.L.; Bergström, J. Oral health risks of tobacco use and effects of cessation. Int. Dent. J. 2010, 60, 7–30. [Google Scholar] [PubMed]
- Górska, R. Epidemiologic studies of oral mucosa changes occurring in children, adolescents, and adults 13–24 years of age in Warsaw. Przegl. Epidemiol. 1997, 51, 339–347. [Google Scholar]
- Konopka, T.; Mendak, M. Prevalence of Oral Mucosal Diseases in Patients of Specialistic Clinic in Wroclaw in the Years 1992–2003. Dent. Med. Probl. 2004, 41, 717–725. [Google Scholar]
- Radwan-Oczko, M.; Kozłowski, Z.; Kazanowska, M. Pathological changes of the oral mucosa in patients attending outpatient Clinic of Periodontology and Oral Pathology—The analysis of years 2006–2009. J. Stomatol. 2011, 64, 186–199. [Google Scholar]
- Axell, T. Occurrence of leukoplakia and some other oral white lesions among 20,333 adult Swedish people. Community Dent. Oral Epidemiol. 1987, 15, 46–51. [Google Scholar] [CrossRef]
- Bánóczy, J.; Rigo, O. Prevalence study of oral precancerous lesions within a complex screening system in Hungary. Community Dent. Oral Epidemiol. 1991, 19, 265–267. [Google Scholar] [CrossRef]
- Jáhn, M.; Schmidt, J.; Fejérdy, L.; Tollas, O.L.; Fejérdy, P.; Madléna, M. The prevalence of oral mucosal lesions in Hungary. Fogorv. Szle. 2007, 100, 59–63. [Google Scholar]
- Reichart, P.A. Oral mucosal lesions in a representative cross-sectional study of aging Germans. Community Dent. Oral Epidemiol. 2000, 28, 390–398. [Google Scholar] [CrossRef]
- Reichart, P.A.; Kohn, H. Prevalence of oral leukoplakia in 1000 Berliners. Oral Dis. 1996, 2, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Reichart, P.A.; Philipsen, H.P. Color Atlasof Dental Medicine. Oral Pathology; ThiemeVerlag: New York, NY, USA, 2000; pp. 73–78. [Google Scholar]
- Silverman, S.; Bhargava, K.; Mani, N.J.; Smith, L.W.; Malaowalla, A.M. Malignant transformation and natural history of oral leukoplakia in 57,518 industrial workers of Gujarat, India. Cancer 1976, 38, 1790–1795. [Google Scholar] [CrossRef]
- Górska, R.; Dembowska, E.; Pietruska, M.; Dymalski, P.; Konopka, T. Frequency of the incidence of periodontal diseases and oral mucosa diseases in the individuals aged 35–44 and 65–74 years in the selected Polish cities. J. Stomatol. 2014, 67, 57–59. [Google Scholar]
- von Arx, T.; Koch, S.; Hardt, N. Lesions of the mouth mucosa. An anamnestic and clinical study of 100 consecutive patients with mucosal lesions. Schweiz Mon. Zahnmed. 2002, 112, 326–329. [Google Scholar]
- Wang, T.; Wang, L.; Yang, H.; Lu, H.; Zhang, J.; Li, N.; Guo, C. Development and Validation of Nomogram for Prediction of Malignant Transformation in Oral Leukoplakia: A Large-Scale Cohort Study. J. Oral Pathol. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Jayasooriya, P.R.; Dayaratne, K.; Dissanayake, U.B.; Warnakulasuriya, S. Malignant transformation of oral leukoplakia: A follow-up study. Clin. Oral Investig. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rubert, A.; Bagán, L.; Bagán, J.V. Oral leukoplakia, a clinical-histopathological study in 412 patients. J. Clin. Exp. Dent. 2020, 12, 540–546. [Google Scholar] [CrossRef]
- Matulić, N.; Bago, I.; Sušić, M.; Gjorgievska, E.; KotaracKnežević, A.; Gabrić, D. Comparison of Er:YAG and Er,Cr:YSGG Laser in the Treatment of Oral Leukoplakia Lesions Refractory to the Local Retinoid Therapy. PhotobiomodulationPhotomed. Laser Surg. 2019, 37, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Mello, F.W.; Miguel, A.F.P.; Dutra-Horstmann, K.L.; Porporatti, A.L.; Warnakulasuriya, S.; Guerra, E.N.S.; Rivero, E.R.C. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 633–640. [Google Scholar] [CrossRef]
- Pinto, A.C.; Caramês, J.; Francisco, H.; Chen, A.; Azul, A.M.; Marques, D. Malignant transformation rate of oral leukoplakia—Systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020. [Google Scholar] [CrossRef]
- Chandroth, S.V.; Venugopal, H.K.V.; Puthenveetil, S.; Jayaram, A.; Mathews, J.; Suresh, N.; Al Kheraif, A.A.; Ramakrishnaiah, R.; Divakar, D.D.; Asawa, K.; et al. Prevalence of oral mucosal lesions among fishermen of Kutch coast, Gujarat, India. Int. Marit Health 2014, 65, 192–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K.; Udaltsova, N.; Engels, E.A.; Katzel, J.A.; Yanik, E.L.; Katki, H.A.; Lingen, M.W.; Silverberg, M.J. Oral leukoplakia and risk of progression to oral cancer: A population-based cohort study. J. Natl. Cancer Inst. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouns, E.; Baart, J.; Karagozoglu, K.H.; Aartman, I.; Bloemena, E.; van der Waal, I. Malignant transformation of oral leukoplakia in a well-de- fined cohort of 144 patients. Oral Dis. 2014, 20, e19–e24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (in Years) | Patients with Leukoplakia | ||||
|---|---|---|---|---|---|
| Total Number of Patients | Smokers | Non-Smokers | |||
| N (%) | n | % | N | % | |
| Women and men | |||||
| 21–40 | 73 (17.6) | 63 a | 86.3 | 10 b | 13.7 |
| 41–60 | 194 (46.6) | 165 c | 85.1 | 29 d | 14.9 |
| >60 | 149 (35.8) | 123 e | 82.6 | 26 f | 17.4 |
| Total | 416 | 363 g | 83.2 | 53 h | 16.8 |
| Women | |||||
| 21–40 | 38 (9.1) | 33 i | 86.8 | 5 j | 13.2 |
| 41–60 | 96 (23.1) | 80 k | 83.3 | 16 l | 19.7 |
| >60 | 62 (14.9) | 50 m | 83.8 | 12 n | 16.2 |
| Total | 196 (47.1) | 160 o | 82.9 | 36 p | 17.1 |
| Men | |||||
| 21–40 | 35 (8.4) | 30 r | 85.7 | 5 s | 14.3 |
| 41–60 | 98 (23.6) | 85 t | 86.2 | 13 u | 17.8 |
| >60 | 87 (20.9) | 73 w | 83.9 | 14 y | 16.1 |
| Total | 220 (52.9) | 188 x | 83.5 | 32 z | 16.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusiak, A.; Maj, A.; Cichońska, D.; Kochańska, B.; Cydejko, A.; Świetlik, D. The Analysis of the Frequency of Leukoplakia in Reference of Tobacco Smoking among Northern Polish Population. Int. J. Environ. Res. Public Health 2020, 17, 6919. https://doi.org/10.3390/ijerph17186919
Kusiak A, Maj A, Cichońska D, Kochańska B, Cydejko A, Świetlik D. The Analysis of the Frequency of Leukoplakia in Reference of Tobacco Smoking among Northern Polish Population. International Journal of Environmental Research and Public Health. 2020; 17(18):6919. https://doi.org/10.3390/ijerph17186919
Chicago/Turabian StyleKusiak, Aida, Adrian Maj, Dominika Cichońska, Barbara Kochańska, Aleksandra Cydejko, and Dariusz Świetlik. 2020. "The Analysis of the Frequency of Leukoplakia in Reference of Tobacco Smoking among Northern Polish Population" International Journal of Environmental Research and Public Health 17, no. 18: 6919. https://doi.org/10.3390/ijerph17186919