The Age Distribution among Children Seeking Medical Treatment for Precocious Puberty in Taiwan


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Estimation of Prevalence
2.3. Estimation of Incidence
2.4. Statistical Analysis
2.5. Ethical Committee Approval
3. Results
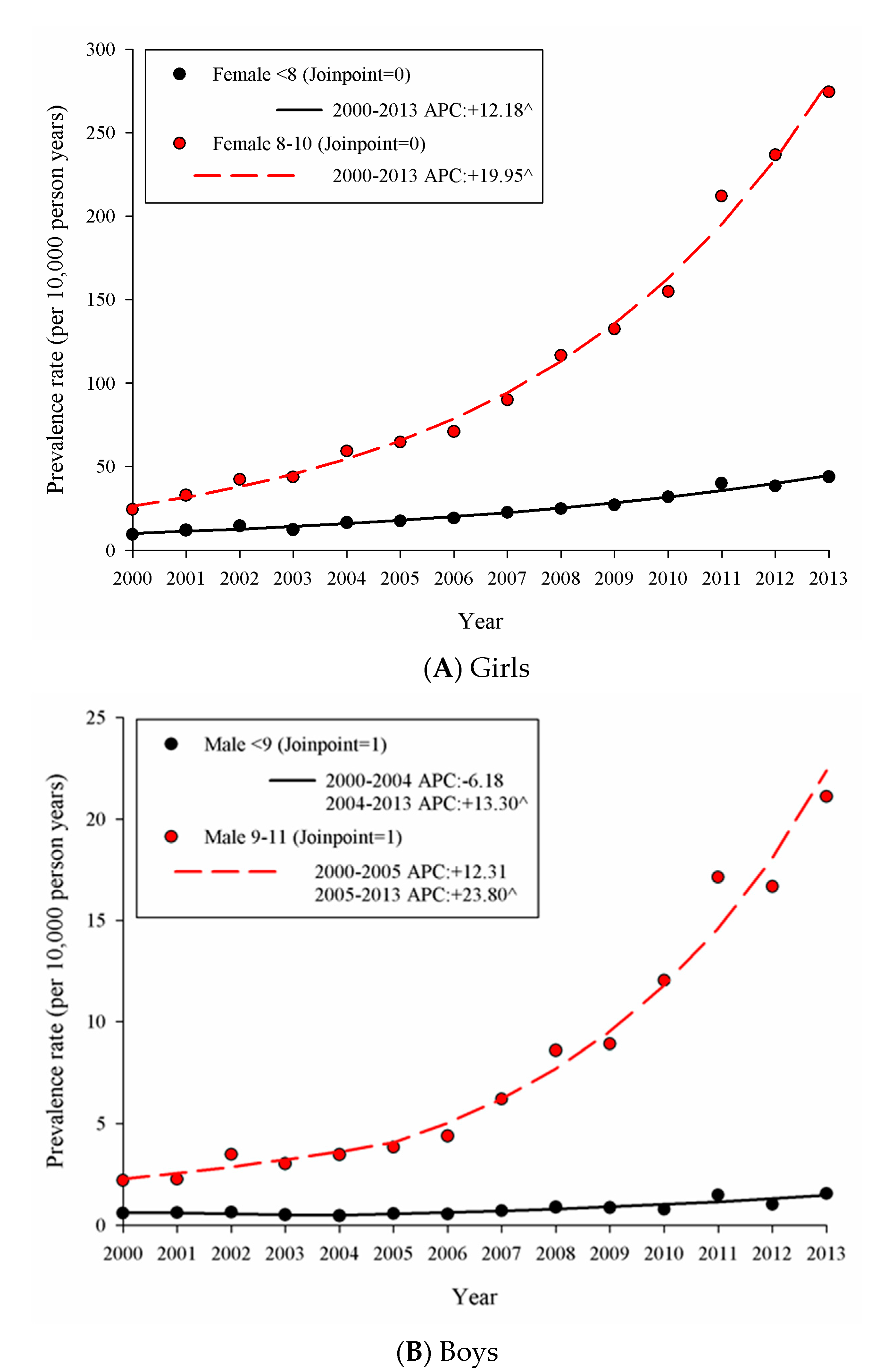
3.1. Prevalence of Precocious Puberty in Taiwan from 2000 to 2013
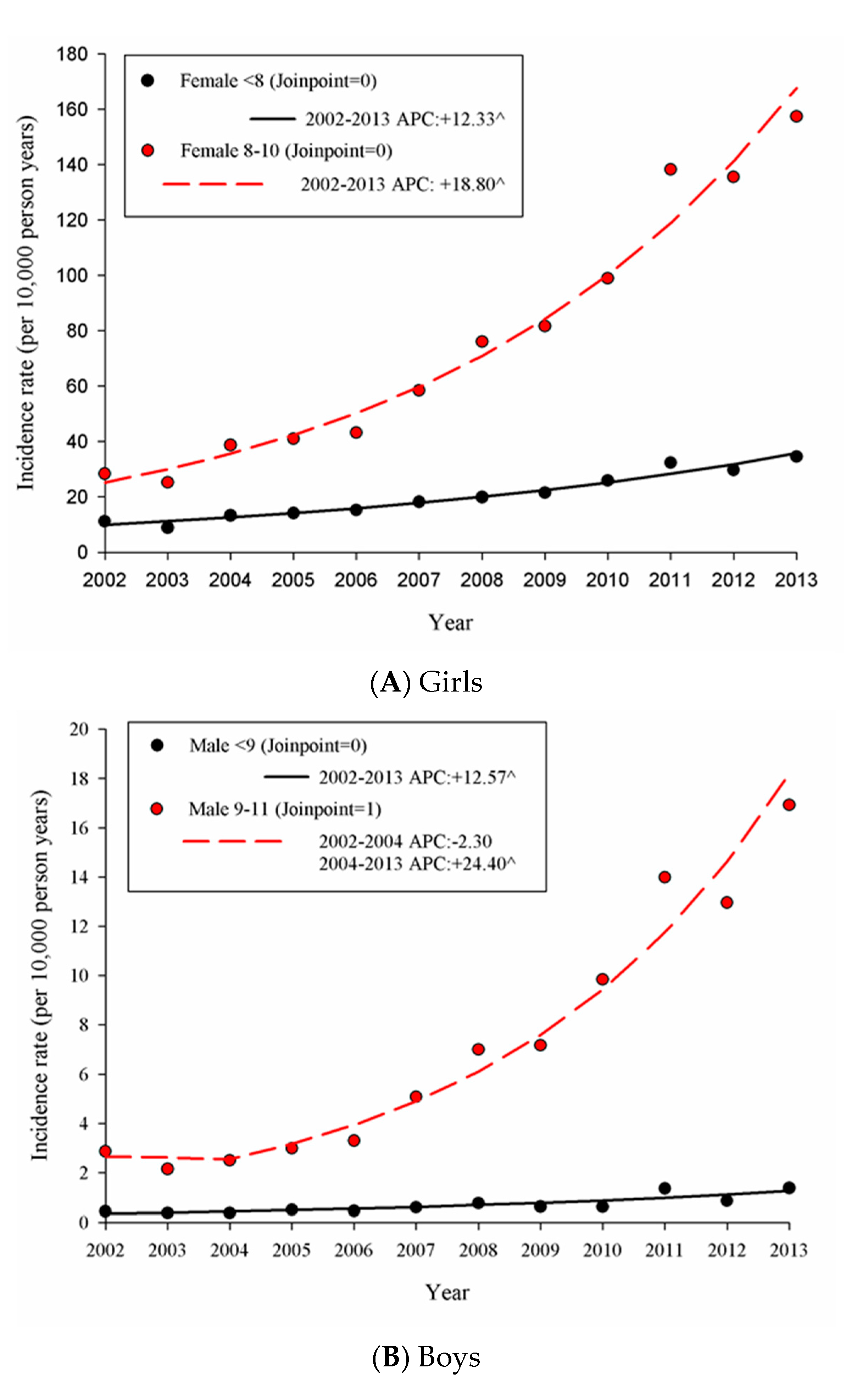
3.2. Incidence of Precocious Puberty in Taiwan from 2002 to 2013
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Styne, D.M.; Grumbach, M.M. Physiology and disorders of puberty. In Williams Textbook of Endocrinology, 13th ed.; Melmed, S., Polonsky, K.S., Larsen, P.R., Kronenberg, H., Williams, R.H., Eds.; Elsevier: Philadelphia, PA, USA, 2016; pp. 1074–1218. [Google Scholar]
- Klein, D.A.; Emerick, J.E.; Sylvester, J.E.; Vogt, K.S. Disorders of Puberty: An Approach to Diagnosis and Management. Am. Fam. Physician 2017, 96, 590–599. [Google Scholar] [PubMed]
- Carel, J.C.; Leger, J. Precocious puberty. N. Engl. J. Med. 2008, 358, 2366–2377. [Google Scholar] [CrossRef]
- Holland-Hall, C.; Burstein, G.R. Adolescent development. In Nelson Textbook of Pediatrics, 20th ed.; Kliegman, R., Stanton, B.F., St. Geme, J.W., Eds.; Elsevier: Philadelphia, PA, USA, 2016; pp. 926–936. [Google Scholar]
- Lucaccioni, L.; Trevisani, V.; Marrozzini, L.; Bertoncelli, N.; Predieri, B.; Lugli, L.; Berardi, A.; Iughetti, L. Endocrine-Disrupting Chemicals and Their Effects during Female Puberty: A Review of Current Evidence. Int. J. Mol. Sci. 2020, 21, 2078. [Google Scholar] [CrossRef] [Green Version]
- Cesario, S.K.; Hughes, L.A. Precocious puberty: A comprehensive review of literature. J. Obstet. Gynecol. Neonatal. Nurs. 2007, 36, 263–274. [Google Scholar] [CrossRef]
- Pan, W.H.; Wu, H.J.; Yeh, C.J.; Chuang, S.Y.; Chang, H.Y.; Yeh, N.H.; Hsieh, Y.T. Diet and health trends in Taiwan: Comparison of two nutrition and health surveys from 1993–1996 and 2005–2008. Asia. Pac. J. Clin. Nutr. 2011, 20, 238–250. [Google Scholar]
- Chu, N.F. Prevalence of obesity in Taiwan. Obes. Rev. 2005, 6, 271–274. [Google Scholar] [CrossRef]
- Chu, N.F. Prevalence and trends of obesity among school children in Taiwan—The Taipei Children Heart Study. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Ho, M.S. Resisting Naphtha Crackers. A historical survey of environmental politics in Taiwan. China Perspect. 2014, 2014, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.C.; Chen, C.Y.; Guo, Y.L.; Lee, C.C. Phthalate Exposure and Associated Health Effects in Taiwanese. Formosa. J. Med. 2010, 14, 169–180. [Google Scholar]
- Wams, T.J. Diethylhexyl phthalate as an environmental contaminant—A review. Sci. Total Environ. 1987, 66, 1–16. [Google Scholar] [CrossRef]
- Yang, F.; Wang, M.; Wang, Z.Y. Sorption behavior of 17 phthalic acid esters on three soils: Effects of pH and dissolved organic matter, sorption coefficient measurement and QSPR study. Chemosphere 2013, 93, 82–89. [Google Scholar] [CrossRef]
- Sun, K.; Jin, J.; Keiluweit, M.; Kleber, M.; Wang, Z.Y.; Pan, Z.Z.; Xing, B. Polar and aliphatic domains regulate sorption of phthalic acid esters (PAEs) to biochars. Bioresour. Technol. 2012, 118, 120–127. [Google Scholar] [CrossRef]
- Huang, P.C.; Tien, C.J.; Sun, Y.M.; Hsieh, C.Y.; Lee, C.C. Occurrence of Phthalates in Sediment and Biota: Relationship to Aquatic Factors, and the Biota-Sediment Accumulation Factor. Chemosphere 2008, 73, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Iughetti, L.; Lucaccioni, L.; Street, M.E.; Bernasconi, S. Clinical expression of endocrine disruptors in children. Curr. Opin. Pediatr. 2020, 32, 554–559. [Google Scholar] [CrossRef]
- Zeng, H.H.; Zhang, H.X.; Wu, X.; Gu, H.X.; Zhang, L.Z.; Liu, Y.Y.; Zhao, X.F.; Li, J.H. Pollution levels and health risk assessment of particulate phthalic acid esters in arid urban areas. Atmos. Pollut. Res. 2017, 8, 188–195. [Google Scholar] [CrossRef]
- Roth, C.L.; Di Vall, S. Consequences of early life programing by genetic and environmental influences: A synthesis regarding pubertal Timing. Endocr. Dev. 2016, 29, 134–152. [Google Scholar]
- Lee, J.E.; Jung, H.W.; Lee, Y.J.; Lee, Y.A. Early-life exposure to endocrine-disrupting chemicals and pubertal development in girls. Ann. Pediatr. Endocrinol. Metab. 2019, 24, 78–91. [Google Scholar] [CrossRef] [Green Version]
- Poursafa, P.; Ataei, E.; Kelishadi, R. A systematic review on the effects of environmental exposure to some organohalogens and phthalates on early puberty. J. Res. Med. Sci. 2015, 20, 613–618. [Google Scholar]
- Lin, L.C.; Wang, S.L.; Chang, Y.C.; Huang, P.C.; Cheng, J.T.; Su, P.H.; Liao, P.C. Associations between maternal phthalate exposure and cord sex hormones in human infants. Chemosphere 2011, 83, 1192–1199. [Google Scholar] [CrossRef]
- Su, P.H.; Chang, C.K.; Lin, C.Y.; Chen, H.Y.; Liao, P.C.; Hsiung, C.A.; Chiang, H.C.; Wang, S.L. Prenatal exposure to phthalate ester and pubertal development in a birth cohort in central Taiwan: A 12-year follow-up study. Environ. Res. 2015, 136, 324–330. [Google Scholar] [CrossRef]
- Editorial Team. The Biggest Plasticizer-Contaminated Food Episode in Human History. Column A1. Apple Daily, 28 May 2011. [Google Scholar]
- Li, J.H.; Ko, Y.C. Plasticizer incident and its health effects in Taiwan. Kaohsiung J. Med Sci. 2012, 28, S17–S21. [Google Scholar] [CrossRef]
- Yen, T.H.; Lin-Tan, D.T.; Lin, J.L. Food safety involving ingestion of foods and beverages prepared with phthalate-plasticizer-containing clouding agents. J. Formos. Med. Assoc. 2011, 110, 671–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Moal, J.; Rigou, A.; Le Tertre, A.; De Crouy-Channel, P.; Léger, J.; Carel, J.C. Marked geographic patterns in the incidence of idiopathic central precocious puberty: A nationwide study in France. Eur. J. Endocrinol. 2018, 178, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Huh, K.; Won, S.; Lee, K.W.; Park, M.J. A Significant Increase in the Incidence of Central Precocious Puberty among Korean Girls from 2004 to 2010. PLoS ONE 2015, 10, e0141844. [Google Scholar] [CrossRef] [Green Version]
- Soriano-Guillén, L.; Corripio, R.; Labarta, J.I.; Cañete, R.; Castro-Feijóo, L.; Espino, R.; Argente, J. Central precocious puberty in children living in Spain: Incidence, prevalence, and influence of adoption and immigration. J. Clin. Endocrinol. Metab. 2010, 95, 4305–4313. [Google Scholar] [CrossRef] [Green Version]
- Teilmann, G.; Pedersen, C.B.; Jensen, T.K.; Skakkebæk, N.E.; Juul, A. Prevalence and incidence of precocious pubertal development in Denmark: An epidemiologic study based on national registries. Pediatrics 2015, 116, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Huang, Y.T.; Tsai, Y.W.; Huang, S.M.; Kuo, K.N.; McKee, M.; Nolte, E. The impact of universal National Health Insurance on population health: The experience of Taiwan. BMC Health Serv. Res. 2010, 10, 225. [Google Scholar] [CrossRef] [Green Version]
- Kaplowitz, P.; Clifford, B. Evaluation and referral of children with signs of early puberty. Pediatrics 2016, 137, e20153732. [Google Scholar] [CrossRef] [Green Version]
- Mul, D.; Hughes, I.A. The use of GnRH agonists in precocious puberty. Eur. J. Endocrinol. 2008, 159, S3–S8. [Google Scholar] [CrossRef]
- Latronico, A.C.; Brito, V.N.; Carel, J.C. Causes, diagnosis, and treatment of central precocious puberty. Lancet. Diabetes Endocrinol. 2016, 4, 265–274. [Google Scholar] [CrossRef]
- Kuo, C.F.; Grainge, M.J.; See, L.C.; Yu, K.H.; Luo, S.F.; Zhang, W.; Doherty, M. Epidemiology and management of gout in Taiwan: A nationwide population study. Arthritis Res. Ther. 2015, 17, 13. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute, Division of Cancer Control and Population Sciences. Join-Point Trend Analysis Software. Regression Program, Version 4.6.0.0. April 2018. Available online: https://surveillance.cancer.gov/join-point/ (accessed on 12 December 2019).
- Langman, C.B.; Alon, U.; Ingelfinger, J.; Englund, M.; Saland, J.M.; Somers, M.J.G.; Stapleton, F.B.; Orta Sibú, N.; Cochat, P.; Wong, W.; et al. A position statement on kidney disease from powdered infant formula-based melamine exposure in Chinese infants. Pediatr. Nephrol. 2009, 24, 1263–1266. [Google Scholar] [CrossRef]
- Cheng, C.L.; Kao, Y.H.Y.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef]
- National Health Insurance Administration, Ministry of Health and Welfare. 2010 Version_Chinese ICD-10-CM/PSC. Available online: https://www.nhi.gov.tw/Content_List.aspx?n=EBBF30B22FF4E869&topn=23C660CAACAA159D (accessed on 19 August 2020).
- Iughetti, L.; Lucaccioni, L. Precocious pubertal development: A challenge for pediatric endocrinologists. Expert Rev. Endocrinol. Metab. 2015, 10, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.C.; Crockett, L.; Richards, M.; Boxer, A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J. Youth Adolesc. 1988, 17, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, A.R.; Wohlfahrt-Veje, C.; de Renzy-Martin, K.T.; Hagen, C.P.; Tinggaard, J.; Mouritsen, A.; Mieritz, M.G.; Main, K.M. Validity of self-assessment of pubertal maturation. Pediatrics 2015, 135, 86–98. [Google Scholar] [CrossRef] [Green Version]
- Hergenroeder, A.C.; Hill, R.B.; Wong, W.W.; Sangi-Haghpeykar, H.; Taylor, W. Validity of self-assessment of pubertal maturation in African American and European American adolescents. J. Adolesc. Health 1999, 24, 201–205. [Google Scholar] [CrossRef]
- Carel, J.C.; Eugster, E.A.; Rogol, A.; Ghizzoni, L.; Palmert, M.R. Consensus statement on the use of gonado-tropin-releasing hormone analogs in children. Pediatrics 2009, 123, e752–e762. [Google Scholar] [CrossRef]
- Pasquino, A.M.; Pucarelli, I.; Passeri, F.; Segni, M.; Mancini, M.A.; Municchi, G. Progression of premature thelarche to central precocious puberty. J. Pediatr. 1995, 126, 11–14. [Google Scholar] [CrossRef]
- Bereket, A. A Critical Appraisal of the Effect of Gonadotropin-Releasing Hormon Analog Treatment on Adult Height of Girls with Central Precocious Puberty. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 33–48. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, P.-H.; Huang, J.-Y.; Li, C.-S.; Chang, H.-P. The Age Distribution among Children Seeking Medical Treatment for Precocious Puberty in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 6765. https://doi.org/10.3390/ijerph17186765
Su P-H, Huang J-Y, Li C-S, Chang H-P. The Age Distribution among Children Seeking Medical Treatment for Precocious Puberty in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(18):6765. https://doi.org/10.3390/ijerph17186765
Chicago/Turabian StyleSu, Pen-Hua, Jing-Yang Huang, Cho-Shun Li, and Hua-Pin Chang. 2020. "The Age Distribution among Children Seeking Medical Treatment for Precocious Puberty in Taiwan" International Journal of Environmental Research and Public Health 17, no. 18: 6765. https://doi.org/10.3390/ijerph17186765