Production of Vegetables and Artichokes Is Associated with Lower Cardiovascular Mortality: An Ecological Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harper, S.; Lynch, J.; Smith, G.D. Social determinants and the decline of cardiovascular diseases: Understanding the links. Annu. Rev. Public Health 2011, 32, 39–69. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Obermeyer, Z.; Tzoulaki, I.; Mayosi, B.M.; Elliott, P.; Leon, D.A. Contributions of risk factors and medical care to cardiovascular mortality trends. Nat. Rev. Cardiol. 2015, 12, 508–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Hyeon, J.; Lee, S.A.; Kwon, S.O.; Lee, H.; Keum, N.; Lee, J.K.; Park, S.M. Role of total, red, processed, and white meat consumption in stroke incidence and mortality: A systematic review and meta-analysis of prospective cohort studies. J. Am. Heart Assoc. 2017, 6, e005983. [Google Scholar] [CrossRef] [PubMed]
- Meier, T.; Gräfe, K.; Senn, F.; Sur, P.; Stangl, G.I.; Dawczynski, C.; März, W.; Kleber, M.E.; Lorkowski, S. Cardiovascular mortality attributable to dietary risk factors in 51 countries in the WHO European Region from 1990 to 2016: A systematic analysis of the Global Burden of Disease Study. Eur. J. Epidemiol. 2019, 34, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Grau, M.; Elosua, R.; Cabrera de León, A.; Guembe, M.J.; Baena-Díez, J.M.; Vega Alonso, T.; Javier Félix, F.; Zorrilla, B.; Rigo, F.; Lapetra, J.; et al. Factores de riesgo cardiovascular en España en la primera década del siglo xxi: Análisis agrupado con datos individuales de 11 estudios de base poblacional, estudio DARIOS. Rev. Esp. Cardiol. 2011, 64, 295–304. [Google Scholar] [CrossRef]
- Roth, G.A.; Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Naghavi, M.; Mokdad, A.H.; Murray, C.J.L. Trends and patterns of geographic variation in cardiovascular mortality among US counties, 1980–2014. JAMA 2017, 317, 1976–1992. [Google Scholar] [CrossRef]
- Mena, C.; Sepúlveda, C.; Fuentes, E.; Ormazábal, Y.; Palomo, I. Spatial analysis for the epidemiological study of cardiovascular diseases: A systematic literature search. Geospat. Health 2018, 13, 587. [Google Scholar] [CrossRef] [Green Version]
- Rajabi, M.; Mansourian, A.; Pilesjö, P.; Åström, D.O.; Cederin, K.; Sundquist, K. Exploring spatial patterns of cardiovascular disease in Sweden between 2000 and 2010. Scand. J. Public Health 2018, 46, 647–658. [Google Scholar] [CrossRef]
- Ferrandiz, J.; Abellan, J.J.; Gomez-Rubio, V.; Lopez-Quilez, A.; Sanmartin, P.; Abellan, C.; Martinez-Beneito, M.A.; Melchor, I.; Vanaclocha, H.; Zurriaga, O.; et al. Spatial analysis of the relationship between mortality from cardiovascular and cerebrovascular disease and drinking water hardness. Environ. Health Perspect. 2004, 112, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Maheswaran, R.; Haining, R.P.; Brindley, P.; Law, J.; Pearson, T.; Fryers, P.R.; Wise, S.; Campbell, M.J. Outdoor air pollution and stroke in Sheffield, United Kingdom: A small-area level geographical study. Stroke 2005, 36, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Barroso, D.; Prieto-Flores, M.E.; Mellado San Gabino, A.; Moreno Jiménez, A. Análisis espacial de la mortalidad por enfermedades cardiovasculares en la ciudad de Madrid, España. Rev. Esp. Salud Publica 2015, 89, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wróblewska, W. Territorial variation in mortality from causes amenable to medical care in Poland. Ann. Agric. Environ. Med. 2017, 24, 489–495. [Google Scholar] [CrossRef] [PubMed]
- AGEPI: Analisis Geográfico Epidemiológico. Programa de Mortalidad de la Comunidad Valenciana. Valencia Conselleria de Sanitat 2005. Available online: http://www.agepi.es (accessed on 11 July 2017).
- Lopez-Quilez, A.; Verdejo, F.; Zurriaga, O.; Botella, P.; Vanaclocha, H.; Martinez-Beneito, M.A.; Amador, A. AGEPI (Analisis Geografico Epidemiologico): Una herramienta para cartografia de enfermedades. Logroño: XXIV Reunión de la Sociedad Española de Epidemiología 2006. Gac. Sanit. 2006, 20, 78. [Google Scholar]
- Martinez-Beneito, M.A.; Lopez-Quiles, A.; Amador-Iscla, A.; Melchor-Alos, I.; Botella-Rocamora, P.; Abellan-Andres, C.; Abellan-Andres, J.J.; Verdejo-Mañez, F.; Zurriaga-Lloréns, O.; Vanaclocha-Lina, H.; et al. Altas de mortalidad de la Comunidad Valenciana. 1991–2000. Valencia Generaliata Valenciana. Coselleria de Sanitat. 2005. Available online: http://san.gva.es/publicaciones/documentos/V.5093-2005.pdf (accessed on 8 September 2020).
- Corpas-Burgos, F.; Vergara-Hernandez, Botella-Rocamora, P.; Perez-Panades, J.; Perpiñan-Faubel, H.; Martinez-Beneito, M.A. Atlas nacional de mortalidad de España (ANDEES). FISABIO-Generalidad Valenciana 2020. Available online: http://fisabio.san.gva.es/desigualdades-en-salud. (accessed on 8 September 2020).
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Conrad, Z.; Thomson, J.; Jahns, L. Prospective analysis of vegetable amount and variety on the risk of all-cause and cause-specific mortality among US adults, 1999–2011. Nutrients 2018, 10, 1377. [Google Scholar] [CrossRef] [Green Version]
- Tang, G.Y.; Meng, X.; Li, Y.; Zhao, C.N.; Liu, Q.; Li, H.B. Effects of vegetables on cardiovascular diseases and related mechanisms. Nutrients 2017, 9, 857. [Google Scholar] [CrossRef] [Green Version]
- Pandino, G.; Lombardo, S.; Mauromicale, G. Mineral profile in globe artichoke as affected by genotype, head part and environment. J. Sci. Food Agric. 2011, 91, 302–308. [Google Scholar] [CrossRef]
- Rondanelli, M.; Giacosa, A.; Morazzoni, P.; Guido, D.; Grassi, M.; Morandi, G.; Bologna, C.; Riva, A.; Allegrini, P.; Perna, S. MediterrAsian diet products that could raise HDL-cholesterol: A systematic review. Biomed. Res. Int. 2016, 2016, 2025687. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Sanidad, Consumo y Bienestar Social. Madrid 2008. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/Estadisticas.htm/ (accessed on 20 August 2020).
- World Health Organization. The International Classification of Diseases (ICD) 9th and 10th Edition; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Argos. Banco de Datos Municipales. Valencia: Generalitat Valenciana. Available online: www.argos.gva.es (accessed on 22 January 2020).
- Generalitat Valenciana: Portal Estadístico. Banco de Datos de Series. Municipios y Comarcas. Banco de Datos Territorial. Available online: http://www.pegv.gva.es/es/bdt (accessed on 21 January 2020).
- Instituto Nacional de Estadística. Censos de Población y Viviendas 2001–2011. Madrid: Instituto Nacional de Estadistica. Available online: www.ine.es (accessed on 8 January 2020).
- Clayton, D.; Kaldor, J. Empirical Bayes estimates of age-standarized relative risks for use in disease mapping. Biometrics 1987, 43, 671–681. [Google Scholar] [CrossRef]
- Mollié, A. Bayesian mapping of Hodgkin’s disease in France. In Spacial Epidemiology: Methods and Applications; Elliot, P., Wakefield, J., Best, N., Briggs, D., Eds.; Oxford University Press: New York, NY, USA, 2001; pp. 267–285. [Google Scholar]
- Textor, J.; Van der Zander, B.; Gilthorpe, M.K.; Liskiewicz, M.; Ellison, G.T.H. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef] [Green Version]
- Moran, P.A.P. The interpretation of statistical maps. J. R. Stat. Soc. Ser. B 1948, 10, 243–251. [Google Scholar] [CrossRef]
- Francula-Zaninovic, S.; Nola, I.A. Management of measurable variable cardiovascular disease’ risk factors. Curr. Cardiol. Rev. 2018, 14, 153–163. [Google Scholar] [CrossRef]
- Orozco-Beltran, D.; Gil-Guillen, V.F.; Redon, J.; Martin-Moreno, J.M.; Pallares-Carratala, V.; Navarro-Perez, J.; Valls-Roca, F.; Sanchis-Domenech, C.; Fernandez-Gimenez, A.; Perez-Navarro, A.; et al. Lipid profile, cardiovascular disease and mortality in a Mediterranean high-risk population: The ESCARVAL-RISK study. PLoS ONE 2017, 12, e0186196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelman, Y.; Van Rijn, B.B.; Ten Haaf, M.E.; Boersma, E.; Peters, S.A. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis 2015, 241, 211–218. [Google Scholar] [CrossRef]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Al-Kindi, S.G.; Brook, R.D. Air pollution and cardiovascular disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2054–2070. [Google Scholar] [CrossRef]
- Martínez-García, M.; Salinas-Ortega, M.; Estrada-Arriaga, I.; Hernández-Lemus, E.; García-Herrera, R.; Vallejo, M. A systematic approach to analyze the social determinants of cardiovascular disease. PLoS ONE 2018, 13, e0190960. [Google Scholar] [CrossRef] [Green Version]
- Pallares-Carratala, V.; Piñón-Selles, F.; Diago-Torrent, J.L.; en nombre de los investigadores del estudio Burriana. Diabetes mellitus y otros factores de riesgo cardiovascular mayores en una población del Mediterraneo español. Estudio Burriana. Endocrinol. Nutr. 2006, 53, 158–167. [Google Scholar] [CrossRef]
- Crouse, D.L.; Balram, A.; Hystad, P.; Pinault, L.; Van den Bosch, M.; Chen, H.; Rainham, D.; Thomson, E.M.; Close, C.H.; Van Donkelaar, A.; et al. Associations between living near water and risk of mortality among urban Canadians. Environ. Health Perspect. 2018, 126, 077008. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Gascon, M.; Martinez, D.; Ponjoan, A.; Blanch, J.; Garcia-Gil, M.D.M.; Ramos, R.; Foraster, M.; Mueller, N.; Espinosa, A.; et al. Air pollution, noise, blue space, and green space and premature mortality in Barcelona: A mega cohort. Int. J. Environ. Res. Public Health 2018, 15, 2405. [Google Scholar] [CrossRef] [Green Version]
- Leurs, L.J.; Schouten, L.J.; Mons, M.N.; Goldbohm, R.A.; Van den Brandt, P.A. Relationship between tap water hardness, magnesium, and calcium concentration and mortality due to ischemic heart disease or stroke in The Netherlands. Environ. Health Perspect. 2010, 118, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, P. Potential health impacts of hard water. Int. J. Prev. Med. 2013, 4, 866–875. [Google Scholar]
- Fioranelli, M.; Bottaccioli, A.G.; Bottaccioli, F.; Bianchi, M.; Rovesti, M.; Roccia, M.G. Stress and inflammation in coronary artery disease: A review psychoneuroendocrineimmunology-based. Front. Immunol. 2018, 9, 2031. [Google Scholar] [CrossRef]
- Sekhotha, M.M.; Monyeki, K.D.; Sibuyi, M.E. Exposure to agrochemicals and cardiovascular disease: A review. Int. J. Environ. Res. Public Health 2016, 13, 229. [Google Scholar] [CrossRef] [Green Version]
- Comité d’Agricultura Ecológica de la Comunitat Valenciana. Estadisticas. Hectareas de Producción. Available online: https://www.caecv.com/ (accessed on 21 August 2020).
- Portal Estadístico de la Generalitat Valenciana. Superficies de Cultivo de Hortalizas de Regadío Por Municipio 2002–2011. Available online: http://www.pegv.gva.es/es/bdt (accessed on 21 August 2020).
- Cardona, D.; Cerezo Mdel, P.; Parra, H.; Quintero, L.; Muñoz, L.; Cifuentes, O.L.; Vélez, S.C. Desigualdades en la mortalidad por enfermedades cardiovasculares en los municipios del Eje Cafetero, 2009–2011. Biomedica 2015, 35, 379–394. [Google Scholar] [CrossRef] [PubMed]
- Karp, D.N.; Wolff, C.S.; Wiebe, D.J.; Branas, C.C.; Carr, B.G.; Mullen, M.T. Reassessing the stroke belt: Using small area spatial statistics to identify clusters of high stroke mortality in the United States. Stroke 2016, 47, 1939–1942. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M.; Fedorko, E.; Halverson, J. Pollution sources and mortality rates across rural-urban areas in the United States. J. Rural Health 2010, 26, 383–391. [Google Scholar] [CrossRef]
- Ghebremeskel, K.; Crawford, M.A. Nutrition and health in relation to food production and processing. Nutr. Health 1994, 9, 237–253. [Google Scholar] [CrossRef]
- Bhupathiraju, S.N.; Wedick, N.M.; Pan, A.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Besson, H.; Paccaud, F.; Marques-Vidal, P. Ecologic correlations of selected food groups with disease incidence and mortality in Switzerland. J. Epidemiol. 2013, 23, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Dietary patterns and the risk of CVD and all-cause mortality in older British men. Br. J. Nutr 2016, 116, 1246–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, H.C.; Nicholls, A. Primary prevention of CVD: Diet. BMJ Clin. Evid. 2014, 2014, 0219. [Google Scholar] [PubMed]
- Misirli, G.; Benetou, V.; Lagiou, P.; Bamia, C.; Trichopoulos, D.; Trichopoulou, A. Relation of the traditional Mediterranean diet to cerebrovascular disease in a Mediterranean population. Am. J. Epidemiol. 2012, 176, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Gillman, M.W.; Cupples, L.A.; Gagnon, D.; Posner, B.M.; Ellison, R.C.; Castelli, W.P.; Wolf, P.A. Protective effect of fruits and vegetables on development of stroke in men. JAMA 1995, 273, 1113–1117. [Google Scholar] [CrossRef] [PubMed]
- Mori, N.; Shimazu, T.; Charvat, H.; Mutoh, M.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Inoue, M.; Goto, A.; Takachi, R.; et al. Cruciferous vegetable intake and mortality in middle-aged adults: A prospective cohort study. Clin. Nutr. 2019, 38, 631–643. [Google Scholar] [CrossRef]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef] [Green Version]
- Banach, M.; Patti, A.M.; Giglio, R.V.; Cicero, A.F.G.; Atanasov, A.G.; Bajraktari, G.; Bruckert, E.; Descamps, O.; Djuric, D.M.; Ezhov, M.; et al. The role of nutraceuticals in statin intolerant patients. J. Am. Coll Cardiol. 2018, 72, 96–118. [Google Scholar] [CrossRef]
- Ben Salem, M.; Affes, H.; Ksouda, K.; Dhouibi, R.; Sahnoun, Z.; Hammami, S.; Zeghal, K.M. Pharmacological studies of artichoke leaf extract and their health benefits. Plant. Foods Hum. Nutr. 2015, 70, 441–453. [Google Scholar] [CrossRef]
- Ben Salem, M.; Affes, H.; Dhouibi, R.; Charfi, S.; Turki, M.; Hammami, S.; Ayedi, F.; Sahnoun, Z.; Zeghal, K.M.; Ksouda, K. Effect of artichoke (Cynara scolymus) on cardiac markers, lipid profile and antioxidants levels in tissue of HFD-induced obesity. Arch. Physiol. Biochem. 2019, 1–7. [Google Scholar] [CrossRef]
- Rondanelli, M.; Monteferrario, F.; Perna, S.; Faliva, M.A.; Opizzi, A. Health-promoting properties of artichoke in preventing cardiovascular disease by its lipidic and glycemic-reducing action. Monaldi Arch. Chest Dis. 2013, 80, 17–26. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Bove, M.; Giovannini, M.; Veronesi, M.; Borghi, C. Short-Term effects of dry extracts of artichokeand berberis in hypercholesterolemic patients without cardiovascular disease. Am. J. Cardiol. 2019, 123, 588–591. [Google Scholar] [CrossRef]
- Pittler, M.H.; Thompson, C.O.; Ernst, E. Artichoke leaf extract for treating hypercholesterolaemia. Cochrane Database Syst. Rev. 2002, 3, CD003335. [Google Scholar]
- Wider, B.; Pittler, M.H.; Thompson-Coon, J.; Ernst, E. Artichoke leaf extract for treating hypercholesterolaemia. Cochrane Database Syst. Rev. 2009, 4, CD003335. [Google Scholar]
- Wider, B.; Pittler, M.H.; Thompson-Coon, J.; Ernst, E. Artichoke leaf extract for treating hypercholesterolaemia. Cochrane Database Syst. Rev. 2013, 3, CD003335. [Google Scholar]
- Santos, H.O.; Bueno, A.A.; Mota, J.F. The effect of artichoke on lipid profile: A review of possible mechanisms of action. Pharmacol. Res. 2018, 137, 170–178. [Google Scholar] [CrossRef]
- Roghani-Dehkordi, F.; Kamkhah, A.F. Artichoke leaf juice contains antihypertensive effect in patients with mild hypertension. J. Diet. Suppl. 2009, 6, 328–341. [Google Scholar] [CrossRef]
- Khan, M.Y.; Kumar, V. Mechanism & inhibition kinetics of bioassay-guided fractions of Indian medicinal plants and foods as ACE inhibitors. J. Tradit. Complement Med. 2018, 9, 73–84. [Google Scholar]
- Ardalani, H.; Jandaghi, P.; Meraji, A.; Hassanpour Moghadam, M. The Effect of Cynara scolymus on blood pressure and BMI in hypertensive patients: A randomized, double-blind, placebo-controlled, clinical trial. Complement Med. Res. 2019, 27, 40–46. [Google Scholar] [CrossRef]
- Castellino, G.; Nikolic, D.; Magán-Fernández, A.; Malfa, G.A.; Chianetta, R.; Patti, A.M.; Amato, A.; Montalto, G.; Toth, P.P.; Banach, M.; et al. Altilix® supplement containing chlorogenic acid and luteolin improved hepatic and cardiometabolic parameters in subjects with metabolic syndrome: A 6 month randomized, double-blind, placebo-controlled study. Nutrients 2019, 25, 2580. [Google Scholar] [CrossRef] [Green Version]
- Bjørklund, G.; Dadar, M.; Martins, N.; Chirumbolo, S.; Goh, B.H.; Smetanina, K.; Lysiuk, R. Brief challenges on medicinal plants: An eye-opening look at ageing-related disorders. Basic. Clin. Pharmacol. Toxicol. 2018, 122, 539–558. [Google Scholar] [CrossRef] [Green Version]
- D’Antuono, I.; Carola, A.; Sena, L.M.; Linsalata, V.; Cardinali, A.; Logrieco, A.F.; Colucci, M.G.; Apone, F. Artichoke polyphenols produce skin anti-Age effects by improving endothelial cell integrity and functionality. Molecules 2018, 23, 2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahebkar, A.; Pirro, M.; Banach, M.; Mikhailidis, D.P.; Atkin, S.L.; Cicero, A.F.G. Lipid-lowering activity of artichoke extracts: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 58, 2549–2556. [Google Scholar] [CrossRef] [PubMed]
- Waltenberger, B.; Mocan, A.; Šmejkal, K.; Heiss, E.H.; Atanasov, A.G. Natural products to counteract the epidemic of cardiovascular and metabolic disorders. Version 2. Molecules 2016, 21, 807. [Google Scholar] [CrossRef] [PubMed]
- Xia, N.; Pautz, A.; Wollscheid, U.; Reifenberg, G.; Förstermann, U.; Li, H. Artichoke, cynarin and cyanidin downregulate the expression of inducible nitric oxide synthase in human coronary smooth muscle cells. Molecules 2014, 19, 3654–3668. [Google Scholar] [CrossRef] [Green Version]
- Ayuntamiento de Benicarló. La Carxofa de Benicarlò. Available online: https://www.ajuntamentdebenicarlo.org/car/pcar-carxofa.php?g_idioma=v (accessed on 20 August 2020).
- Maura, J. Coordinador. In Els Millors Pinxos i Tapes de la Carxofa de Benicarló; Onada Editions: Benicarló, Spain, 2015. [Google Scholar]
- Soler, C.; Fernandez, F. Estructura de la Propiedad de Tierras en España; Fundación Mundubat Revista Soberania Alimentaria Biodiversidad Culturas: Bilbao, Spain, 2015. [Google Scholar]
- Thompson, R. Gardening for health: A regular dose of gardening. Clin. Med. 2018, 18, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Kathiresan, S.; Srivastava, D. Genetics of human cardiovascular disease. Cell 2012, 148, 1242–1257. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
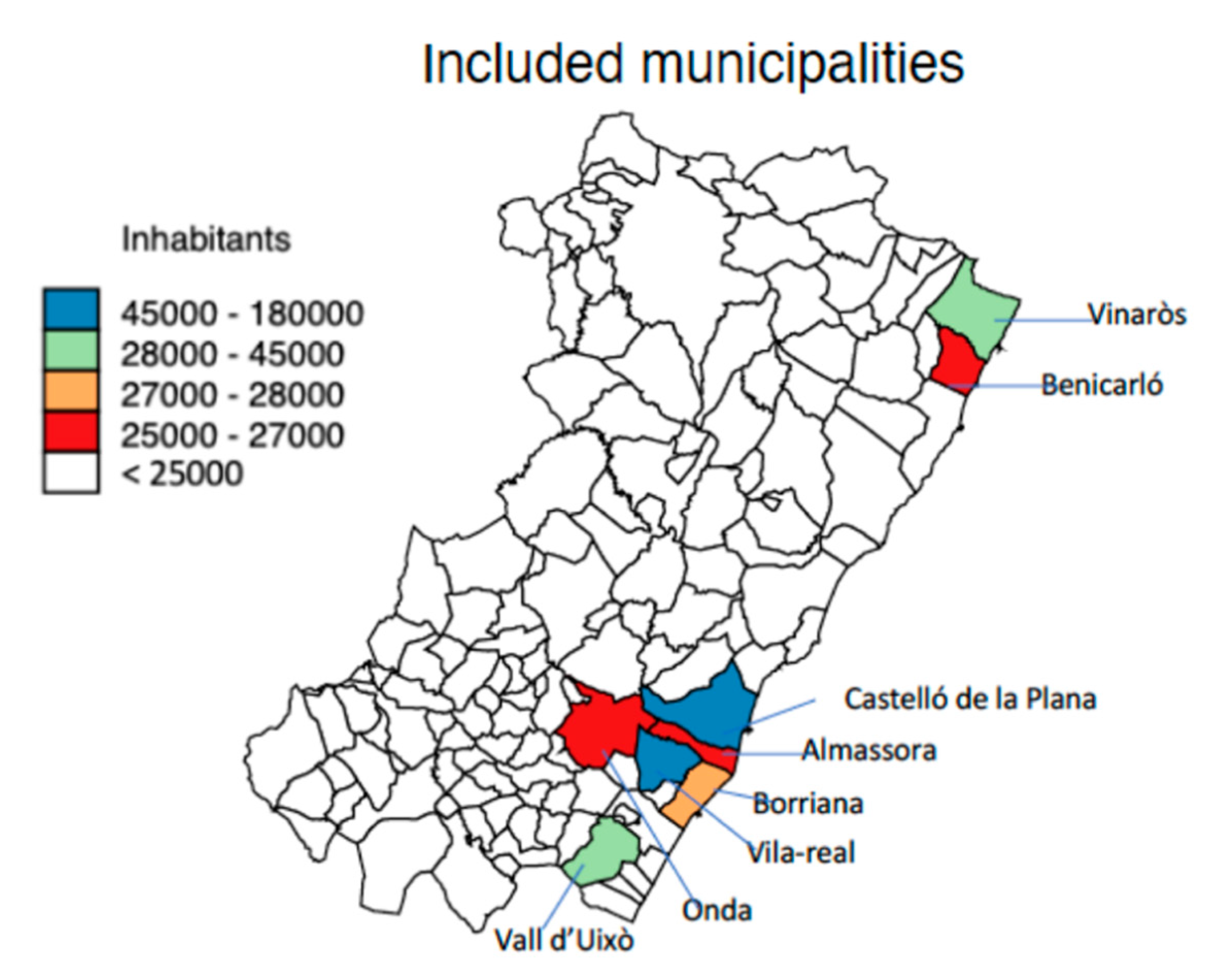
| Variables | Almassora | Benicarló | Borriana | Castelló | Onda | Vall d’Uixó | Vila- Real | Vinaròs |
|---|---|---|---|---|---|---|---|---|
| Socio-economic indicators | ||||||||
| Health departments | 2 | 1 | 3 | 2 | 3 | 3 | 3 | 1 |
| Population 1 | 17,384 | 21,015 | 27,385 | 150,444 | 20,021 | 29,638 | 42,961 | 22,960 |
| Population aged 65 years and above % | 14.2 | 17.8 | 17.1 | 17.8 | 15.7 | 19.1 | 15.8 | 18.1 |
| Foreign-born % | 14.8 | 21.2 | 15.9 | 15.9 | 12.5 | 7.1 | 11.8 | 17.8 |
| Household income in euros | 14,064 | 13,824 | 14,077 | 15,519 | 13,815 | 13,754 | 14,436 | 14,198 |
| Unemployment % | 18.1 | 15.3 | 16.8 | 17.9 | 21.2 | 18.67 | 19.6 | 15.3 |
| Illiteracy % | 32.1 | 22.6 | 22.4 | 20.4 | 23.3 | 24.0 | 24.4 | 22.9 |
| Occupation % | ||||||||
| Agriculture % | 3.2 | 8.8 | 10.0 | 2.7 | 5.9 | 8.6 | 4.8 | 8.7 |
| Industrial % | 22.1 | 18.7 | 22.7 | 17.2 | 33.1 | 20.5 | 26.6 | 16.7 |
| Construction % | 11.8 | 10.1 | 7.8 | 6.6 | 8.7 | 9.3 | 8.6 | 8.2 |
| Services % | 62.9 | 62.4 | 59.5 | 73.5 | 52.3 | 61.7 | 60.0 | 66.4 |
| Agriculture production Ha 2 | ||||||||
| Agriculture 2 | 104.3 | 181.0 | 130.7 | 46.0 | 404.0 | 189.1 | 88.8 | 335.9 |
| Herbaceous 2 | 8.7 | 58.9 | 4.7 | 7.5 | 14.6 | 4.3 | 4.7 | 37.0 |
| Woody plants 2 | 90.0 | 105.8 | 122.9 | 29.2 | 242.2 | 77.9 | 80.2 | 281.5 |
| Pastures 2 | 5.8 | 15.8 | 3.1 | 8.1 | 69.9 | 106.0 | 3.9 | 16.3 |
| Forest species 2 | 0.15 | 1.2 | 0.01 | 1.21 | 89.4 | 0.02 | 0.0 | 1.04 |
| Vegetables 3 | 1.1 | 64.0 | 0.9 | 0.2 | 0.2 | 0.3 | 0.0 | 10.3 |
| Artichoke 3 | 0.5 | 27.4 | 0.2 | 0.1 | 0.0 | 0.03 | 0.0 | 2.8 |
| Citrus 3 | 94.4 | 52.3 | 111.7 | 21.7 | 182.7 | 70.9 | 76.2 | 204.6 |
| Environmental indicators | ||||||||
| Water hardness in French degrees 4 | 35.8° | 35.5° | 45.8° | 49.5° | 48.9° | 28.9° | 45.0° | 30.4° |
| Coastal distance in km | 5.0 | 0.10 | 5.7 | 5.0 | 10.6 | 20.0 | 8.4 | 0.10 |
| PM10 mg/m3 5 | 36.58 | 16.03 | 27.38 | 29.08 | 21.93 | 19.0 6 | 31.64 | 16.03 |
| NO2 mg/m3 5 | 22.7 | 6.25 | 16.22 | 21.49 | 9.0 | 6.5 6 | 19.20 | 6.25 |
| Variables | (a) | (b) | (c) | (d) | (e) | (f) | (g) | (h) | (i) | (j) | (k) | (l) | (m) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population aged 65 years and above % (a) | 1.0 | ||||||||||||
| Household income in euros (b) | −0.06 | 1.0 | |||||||||||
| Foreign-born % (c) | 0.16 | 0.38 | 1.0 | ||||||||||
| Illiteracy % (d) | −0.41 | −0.33 | −0.71 | 1.0 | |||||||||
| Agriculture Production 1 (e) | 0.22 | −0.69 | −0.17 | 0.10 | 1.0 | ||||||||
| Vegetables 1 (f) | 0.22 | 0.33 | 0.52 | 0.10 | 0.40 | 1.0 | |||||||
| Artichoke 1 (g) | 0.25 | 0.04 | 0.75 | −0.29 | 0.05 | 0.91 | 1.0 | ||||||
| Citrus 1 (h) | −0.25 | −0.12 | −0.22 | 0.24 | 0.62 | 0.21 | −0.01 | 1.0 | |||||
| Unemployment % (i) | −0.44 | −0.57 | −0.83 | −0.57 | 0.05 | −0.43 | −0.92 | 0.01 | 1.0 | ||||
| Coastal distance in km (j) | −0.11 | −0.42 | −0.88 | 0.36 | 0.14 | −0.66 | 0.87 | 0.02 | 0.84 | 1.0 | |||
| PM10 mg/m3/(k) | −0.70 | 0.40 | −0.31 | 0.37 | −0.72 | −0.56 | −0.41 | −0.14 | 0.49 | 0.25 | 1.0 | ||
| NO2 mg/m3 (l) | −0.64 | 0.42 | −0.19 | 0.23 | −0.74 | −0.54 | −0.35 | −0.22 | 0.42 | 0.19 | 0.98 | 1.0 | |
| Water hardness 2 (m) | −0.54 | 0.45 | 0.19 | −0.40 | 0.40 | −0.57 | −0.41 | −0.10 | 0.29 | 0.11 | 0.51 | 0.59 | 1.0 |
| Municipality | All-Cause Mortality | Cardiovascular Disease (CVD) | Cerebrovascular Disease (CED) | Ischaemic Heart Disease (IHD) | CED + IHD | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | Males | Females | Males | Females | |
| Almassora | 101.2 | 103.8 | 99.2 | 115.5 | 98.2 | 98.5 | 110.2 | 101.1 | 103.8 | 99.1 |
| Benicarló | 104.7 | 111.8 | 94.9 | 97.7 | 75.5 | 71.4 | 94.1 | 82.1 | 83.3 | 73.9 |
| Borriana | 95.4 | 101.0 | 120.6 | 116.3 | 137.0 | 141.6 | 113.4 | 97.6 | 126.5 | 129.3 |
| Castelló | 98.1 | 107.1 | 106.4 | 106.5 | 100.6 | 98.9 | 108.1 | 117.9 | 104.1 | 104.3 |
| Onda | 115.2 | 109.1 | 111.3 | 120.2 | 119.3 | 133.1 | 107.2 | 87.0 | 104.1 | 120.1 |
| Vall d’Uixó | 108.2 | 111.7 | 105.0 | 116.1 | 103.8 | 106.4 | 107.2 | 88.2 | 114.0 | 101.0 |
| Vila-real | 104.1 | 106.2 | 113.7 | 121.0 | 128.3 | 138.4 | 101.3 | 96.2 | 115.9 | 126.4 |
| Vinaròs | 100.7 | 103.0 | 100.6 | 102.0 | 85.4 | 101.7 | 109.0 | 90.9 | 96.3 | 98.5 |
| Municipality | All-Cause Mortality | Cardiovascular Disease (CVD) | Cerebrovascular Disease (CED) | Ischaemic Heart Disease (IHD) | CED + IHD | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | Males | Females | Males | Females | |
| Almassora | 952.2 | 866.2 | 287.7 | 382.5 | 80.8 | 109.8 | 80.2 | 46.4 | 161.1 | 156.1 |
| Benicarló | 891.9 | 812.0 | 274.8 | 335.5 | 60.7 | 78.5 | 68.0 | 36.2 | 128.7 | 114.7 |
| Borriana | 1082.9 | 894.8 | 350.8 | 399.0 | 114.7 | 159.2 | 82.5 | 44.8 | 197.2 | 203.4 |
| Castelló | 976.5 | 834.2 | 378.3 | 365.8 | 83.5 | 110.9 | 78.5 | 53.2 | 162.0 | 164.1 |
| Onda | 977.7 | 929.0 | 323.0 | 414.4 | 99.2 | 151.5 | 77.6 | 38.5 | 176.7 | 190.0 |
| Vall d’Uixó | 948.0 | 885.3 | 303.7 | 399.0 | 85.6 | 118.6 | 71.2 | 39.3 | 159.9 | 157.7 |
| Vila-real | 1027.0 | 925.3 | 331.2 | 414.1 | 106.9 | 155.7 | 73.2 | 43.8 | 180.1 | 198.8 |
| Vinaròs | 996.4 | 853.6 | 292.4 | 350.2 | 69.5 | 113.7 | 79.5 | 41.0 | 148.9 | 154.6 |
| SMRs | Moran’s I Index | Z | p-Value |
|---|---|---|---|
| All-cause mortality | −0.013 | 0.620 | 0.268 |
| Cardiovascular (CVD) mortality | 0.110 | 2.015 | 0.022 |
| Cerebrovascular (CED) mortality | 0.073 | 1.596 | 0.055 |
| Ischaemic heart disease (IHD) mortality | −0.008 | 0.741 | 0.229 |
| CED + IHD mortality | 0.110 | 2.052 | 0.020 |
| AMRs | |||
| All-cause mortality | 0.006 | 0.699 | 0.242 |
| Cardiovascular (CVD) mortality | 0.046 | 1.292 | 0.098 |
| Cerebrovascular (CED) mortality | 0.073 | 1.199 | 0.115 |
| Ischaemic heart disease (IHD) mortality | 0.006 | 0.817 | 0.207 |
| CED + IHD mortality | 0.113 | 2.083 | 0.019 |
| Factors | SMRs | AMR | ||||
|---|---|---|---|---|---|---|
| RC 1(95% CI 2) | p-Value | ICC 3 (95% CI) | RC 1 (95% CI 2) | p-Value | ICC 3 (95% IC) | |
| All-cause mortality | ||||||
| Agriculture 4 | −0.01 (−0.04 to 0.43) | 0.726 | 0.24(0.01 to 0.92) 5 | −0.04 (−0.27 to 0.20) | 0.761 | 0.25 (0.00–0.91) |
| Vegetables 4 | −0.19 (−0.31 to −0.07) | 0.003 | NC 6 | −1.76 (−2.88 to −0.63) | 0.002 | NC 6 |
| Artichokes 4 | −0.42 (−0.62 to −0.11) | 0.003 | NC 6 | −3.92 (−6.41 to −1.42) | 0.002 | NC 6 |
| Citrus 4 | 0.03 (−0.01 to 0.07) | 0.196 | 0.16 (0.00 to 0.97) 5 | 0.25 (−0.11 to 0.61) | 0.178 | 0.15 (0.00 to 0.97) |
| Cardiovascular disease (CVD) mortality | ||||||
| Agriculture 4 | −0.02 (−0.05 to 0.01) | 0.169 | 0.23 (0.01 to 0.92) | −0.05 (−0.17 to 0.06) | 0.376 | NC 6 |
| Vegetables 4 | −0.20 (−0.36 to −0.03) | 0.017 | 0.07(0.00 to 0.99) | −0.58 (−1.33 to 0.16) | 0.126 | NC 6 |
| Artichokes 4 | −0.42 (−0.79 to −0.04) | 0.028 | 0.10 (0.00 to 0.99) | −1.20 (−2.88 to 0.48) | 0.161 | NC 6 |
| Citrus 4 | 0.02 (−0.01 to 0.06) | 0.137 | 0.88 (0.50 to 0.98) | −0.02 (−0.22 to 0.18) | 0.862 | NC 6 |
| Cerebrovascular disease (CED) mortality | ||||||
| Agriculture 4 | −0.05 (−0.14 to 0.04) | 0.309 | 0.82 (0.54 to 0.96) | −0.04 (−0.14 to 0.05) | 0.372 | 0.62 (0.21 to 0.90) |
| Vegetables 4 | −0.68 (−1.16 to −0.19) | 0.006 | 0.72 (0.33 to 0.93) | −0.71 (−1.18 to −0.24) | 0.003 | 0.39 (0.05 to 0.88) |
| Artichokes 4 | −1.47 (−2.57 to −0.36) | 0.000 | 0.73 (0.35 to 0.93) | −1.54 (−2.16 to −0.47) | 0.005 | 0.41 (0.06 to 0.88) |
| Citrus 4 | 0.04 (−0.13 to 0.21) | 0.623 | 0.84 (0.54 to 0.96) 5 | 0.05 (−0.12 to 0.22) | 0.544 | 0.64 (0.23 to 0.99) |
| Ischaemic heart disease (IHD) mortality | ||||||
| Agriculture 4 | 0.01 (−0.05 to 0.07) | 0.771 | NC 6 | 0.01 (−0.02 to 0.03) | 0.651 | 0.19 (0.0 to 0.95) |
| Vegetables 4 | −0.36 (−0.76 to 0.03) | 0.067 | NC 6 | −0.21 (−0.31 to −0.12) | 0.000 | NC 6 |
| Artichokes 4 | −0.78 (−1.65 to 0.10) | 0.083 | NC 6 | −0.46 (−0.68 to −0.25) | 0.000 | NC 6 |
| Citrus 4 | 0.30 (−0.07 to 0.14) | 0.548 | NC 6 | 0.03 (−0.01 to 0.06) | 0.104 | 0.06 (0.00 to 0.99) |
| Cerebrovascular disease (CED) and ischaemic heart disease (IHD) mortality | ||||||
| Agriculture 4 | −0.02 (−0.10 to 0.05) | 0.509 | 0.80 (0.47 to 0.95) 5 | −0.04 (0.15 to 0.08) | 0.528 | 0.80 (0.45 to 0.95) 5 |
| Vegetables 4 | −0.57 (−0.89 to −0.26) | 0.000 | 0.59 (0.18 to 0.90) | −0.92 (−1.41 to −0.42) | 0.000 | 0.56(0.16 to 0.90) |
| Artichokes 4 | −1.24 (−1.97 to −0.52) | 0.001 | 0.61 (0.20 to 0.91) | −2.00 (−3.14 to −0.86) | 0.001 | 0.58 (0.17 to 0.90) |
| Citrus 4 | 0.05 (−0.07 to 0.17) | 0.434 | 0.80 (0.47 to 0.95) 5 | 0.08 (−0.12 to 0.28) | 0.421 | 0.79 (0.44 to 0.95) 5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnedo-Pena, A.; Puig-Barberà, J.; Bellido-Blasco, J.; Romeu-Garcia, M.; Pac-Sa, M.R.; Guillen-Grima, F. Production of Vegetables and Artichokes Is Associated with Lower Cardiovascular Mortality: An Ecological Study. Int. J. Environ. Res. Public Health 2020, 17, 6583. https://doi.org/10.3390/ijerph17186583
Arnedo-Pena A, Puig-Barberà J, Bellido-Blasco J, Romeu-Garcia M, Pac-Sa MR, Guillen-Grima F. Production of Vegetables and Artichokes Is Associated with Lower Cardiovascular Mortality: An Ecological Study. International Journal of Environmental Research and Public Health. 2020; 17(18):6583. https://doi.org/10.3390/ijerph17186583
Chicago/Turabian StyleArnedo-Pena, Alberto, Joan Puig-Barberà, Juan Bellido-Blasco, MªAngeles Romeu-Garcia, Mª Rosario Pac-Sa, and Francisco Guillen-Grima. 2020. "Production of Vegetables and Artichokes Is Associated with Lower Cardiovascular Mortality: An Ecological Study" International Journal of Environmental Research and Public Health 17, no. 18: 6583. https://doi.org/10.3390/ijerph17186583