Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?—A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
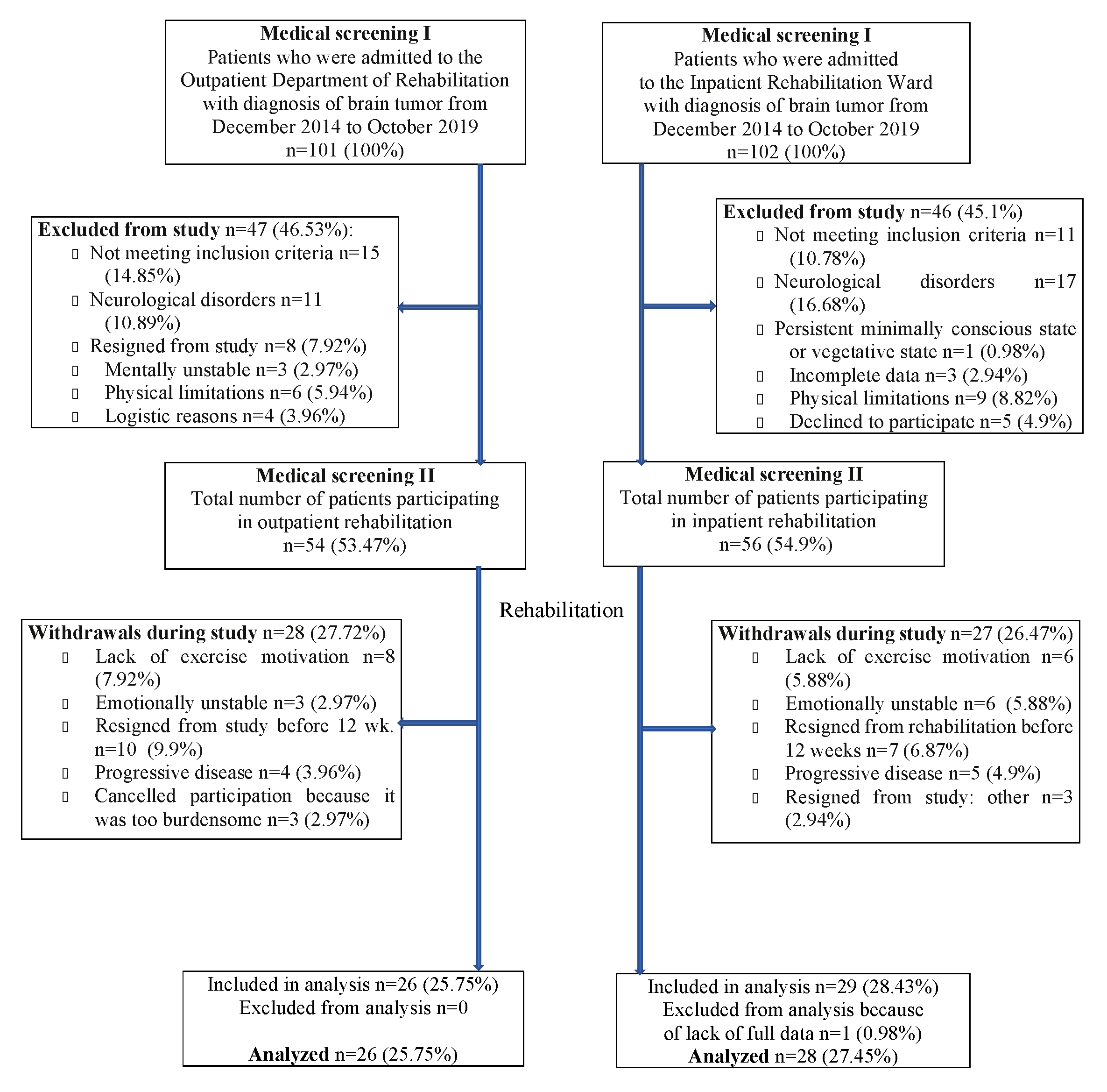
2.2. Participants and Setting
2.2.1. Inpatient Group
2.2.2. Outpatient Group
2.3. Rehabilitation Program
2.3.1. Inpatient Rehabilitation Program
2.3.2. Outpatient Rehabilitation Program
2.4. Measurement
2.4.1. Functional Assessment
Functional Independence Measure
Barthel Index
Berg Balance Scale
2.4.2. Cognitive Function Assessment
2.4.3. Patient Reported Outcome—Functional Assessment of Cancer Therapy
The Functional Assessment of Cancer Therapy for Brain Tumors Scale (FACT-Br)
The Functional Assessment of Cancer Therapy—Cognitive Scale (FACT-Cog)
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. General Assessment at Admission to Rehabilitation Program
3.3. Analysis of Physical Functioning Results in BT Inpatients and Outpatients
3.4. Effect of Rehabilitation Treatment on Cognitive Functioning in BT Inpatients and Outpatients
3.5. Results of Rehabilitation Treatment in Patient-Reported Function Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE III | Addenbrooke’s Cognitive Examination III |
| ADL | Activities of Daily Living |
| BBS | Berg Balance Scale |
| BDNF | Brain-Derived Neurotrophic Factor |
| BI | Barthel Index |
| BT | Brain Tumor |
| CNS | Central Nervous System |
| FACT | Functional Assessment of Cancer Therapy |
| FACT-Br | Functional Assessment of Cancer Therapy for Brain Tumors Scale |
| FACT-Cog | Functional Assessment of Cancer Therapy–Cognitive Scale |
| FIM | Functional Independence Measure |
| HRmax | Maximum Heart Rate |
| ICF | International Classification of Functioning, Disability and Health |
| MMSE | Mini-Mental State Examination |
| MoCA | Montreal Cognitive Assessment |
| NYHA | New York Heart Association |
| PNF | Proprioceptive Neuromuscular Facilitation |
| QoL | Quality of Life |
| VEGF | Vascular Endothelial Growth Factor |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leece, R.; Xu, J.; Ostrom, Q.T.; Chen, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. Global incidence of malignant brain and other central nervous system tumors by histology, 2003–2007. Neuro Oncol. 2017, 19, 1553–1564. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, P.K.; et al. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, K.W.; Yoo, H.; Kong, H.J.; Won, Y.J.; Park, S.; Lee, S.H. Population-based survival data for brain tumors in Korea. J. Neurooncol. 2012, 109, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.B.; Morishita, S.; Yadav, R. Changing paradigms in the rehabilitation of inpatients with brain tumors. Curr. Phys. Med. Rehabil. Rep. 2018, 6, 115–120. [Google Scholar] [CrossRef]
- Kim, W.J.; Novotna, K.; Amatya, B.; Khan, F. Clinical practice guidelines for the management of brain tumours: A rehabilitation perspective. J. Rehabil. Med. 2019, 51, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Day, J.; Gillespie, D.C.; Rooney, A.G.; Bulbeck, H.J.; Zienius, K.; Boele, F.; Grant, R. Neurocognitive Deficits and Neurocognitive Rehabilitation in Adult Brain Tumors. Curr. Treat. Options Neurol. 2016, 18, 22. [Google Scholar] [CrossRef]
- Baker, P.D.; Bambrough, J.; Fox, J.R.E.; Kyle, S.D. Health-related quality of life and psychological functioning in patients with primary malignant brain tumors: A systematic review of clinical, demographic and mental health factors. Neurooncol. Pract. 2016, 3, 211–221. [Google Scholar] [CrossRef]
- Alfano, C.M.; Kent, E.E.; Padgett, L.S.; Grimes, M.; de Moor, J.S. Making cancer rehabilitation services work for cancer patients: Recommendations for research and practice to improve employment outcomes. PM R. 2017, 9, S398–S406. [Google Scholar] [CrossRef]
- Jones, L.W.; Guill, B.; Keir, S.T.; Carter, K.; Friedman, H.S.; Bigner, D.D.; Reardon, D.A. Exercise interest and preferences among patients diagnosed with primary brain cancer. Support. Care Cancer. 2007, 15, 47–55. [Google Scholar] [CrossRef]
- Capozzi, L.C.; Boldt, K.R.; Easaw, J.; Bultz, B.; Culos-Reed, S.N. Evaluating a 12-week exercise program for brain cancer patients. Psychooncology 2016, 25, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Søgaard, K.; Minet, L.R.; Jarden, J.O. A 12-week interdisciplinary rehabilitation trial in patients with gliomas—A feasibility study. Disabil. Rehabil. 2018, 40, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Amatya, B.; Ng, L.; Drummond, K.; Galea, M. Multidisciplinary rehabilitation after primary brain tumour treatment. Cochrane Database Syst. Rev. 2015, 2015, CD009509. [Google Scholar] [CrossRef] [PubMed]
- Pace, A.; Villani, V.; Parisi, C.; di Felice, S.; Lamaro, M.; Falcicchio, C.; Bonucci, A.; Pugliese, P.; di Napoli, A.; Di Lallo, D.; et al. Rehabilitation pathways in adult brain tumor patients in the first 12 months of disease. A retrospective analysis of services utilization in 719 patients. Support Care Cancer. 2016, 24, 4801–4806. [Google Scholar] [CrossRef] [PubMed]
- Maritz, R.; Tennant, A.; Fellinghauer, C.; Stucki, G.; Prodinger, B. The Functional Independence Measure 18-item version can be reported as a unidimensional interval-scaled metric: Internal construct validity revisited. J. Rehabil. Med. 2019, 51, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutta, D.; Vanere, P.; Gupta, T.; Munshi, A.; Jalali, R. Factors influencing activities of daily living using FIM-FAM scoring system before starting adjuvant treatment in patients with brain tumors: Results from a prospective study. J. Neurooncol. 2009, 94, 103–110. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief. 2020, 30, 105419. [Google Scholar] [CrossRef]
- Liljehult, M.M.; Buus, L.; Liljehult, J.; Rasmussen, B.K. Walking ability in patients with glioblastoma: Prognostic value of the Berg Balance Scale and the 10 meter walk test. J. Neurooncol. 2017, 135, 335–342. [Google Scholar] [CrossRef]
- Downs, S.; Marquez, J.; Chiarelli, P. The berg balance scale has high intra-and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Geler-Kulcu, D.; Gulsen, G.; Buyukbaba, E.; Ozkan, D. Functional recovery of patients with brain tumor or acute stroke after rehabilitation: A comparative study. J. Clin. Neurosci. 2009, 16, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Matías-Guiu, J.A.; Fernández-Bobadilla, R.; Cortés-Martínez, A. Addenbrooke’s cognitive examination III: A neuropsychological test useful to screen and obtain a cognitive profile. Neurologia 2018, 33, 140. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, J.A.; Cortés-Martínez, A.; Valles-Salgado, M.; Rognoni, T.; Fernández-Matarrubia, M.; Moreno-Ramos, T.; Matías-Guiu, J. Addenbrooke’s cognitive examination III: Diagnostic utility for mild cognitive impairment and dementia and correlation with standardized neuropsychological test. Int. Psychogeriatr. 2017, 29, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Burrell, J.R.; Piguet, O. Lifting the veil: How to use clinical neuropsychology to assess dementia. J. Neurol. Neurosurg. Psychiatry. 2015, 86, 1216–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Lin, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J.; et al. The functional assessment of cancer therapy scale: Development and validation of the general measure. J. Clin. Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef]
- Weitzner, M.A.; Meyers, C.A.; Gelke, C.K.; Byrne, K.S.; Cella, D.F.; Levin, V.A. The functional assessment of cancer therapy (FACT) scale. Development of a brain subscale and revalidation of the general version (FACT-G) in patients with primary brain tumors. Cancer 1995, 75, 1151–1161. [Google Scholar] [CrossRef]
- Gazzotti, M.R.; Malheiros, S.M.; Batan Alith, M.; Nascimento, O.; Lopes Santoro, I.; Jardim, J.R.; Vidotto, M. Quality of life and physical limitations in primary brain tumor patients. Qual. Life Res. 2011, 20, 1639–1643. [Google Scholar] [CrossRef]
- Wagner, L.I.; Sweet, J.; Butt, Z.; Lai, J.S.; Cella, D. Measuring patient self-reported cognitive function: Development of the functional assessment of cancer therapy-Cognitive function instrument. J. Support Oncol. 2009, 7, 32–39. [Google Scholar]
- Dyk, K.V.; Crespi, C.M.; Petersen, L.; Ganz, P.A. Identifying cancer-related cognitive impairment using the FACT-Cog perceived cognitive impairment. JNCI Cancer Spectr. 2019, 4, pkz099. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.R-project.org/ (accessed on 5 July 2019).
- World Health Organization (WHO). International Classification of Functioning; Disability and Health, ICF.: Geneva, Switzerland, 2001. Available online: http://www.who.int/classifications/icf/en (accessed on 26 May 2015).
- Bartolo, M.; Zucchella, C.; Pace, A.; Lanzetta, G.; Vecchione, C.; Bartolo, M.; Grillea, G.; Serrao, M.; Tassorelli, C.; Sandrini, G.; et al. Early rehabilitation after surgery improves functional outcome in inpatients with brain tumours. J. Neurooncol. 2012, 107, 537–544. [Google Scholar] [CrossRef]
- Fu, J.B.; Parsons, H.A.; Shin, K.Y.; Guo, Y.; Konzen, B.S.; Yadav, R.R.; Smith, D.W. Comparison of functional outcomes in low- and high-grade astrocytoma rehabilitation inpatients. Am. J. Phys. Med. Rehabil. 2010, 89, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.; Treger, I.; Ring, H. Rehabilitation outcomes in patients with brain tumors and acute stroke: Comparative study of inpatient rehabilitation. Am. J. Phys. Med. Rehabil 2006, 85, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Pedersen, C.B.; Jarden, J.O.; Beier, D.; Minet, L.R.; Søgaard, K. Effectiveness of physical therapy-and occupational therapy-based rehabilitation in people who have glioma and are undergoing active anticancer treatment: Single-blind, randomized controlled trial. Phys. Ther. 2020, 100, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, S.; Abo, M.; Okamoto, T.; Kakuda, W.; Miyamura, K.; Kimura, I. Responsiveness of the functioning and disability parts of the international classification of functioning, disability, and health core sets in postacute stroke patients. Int. J. Rehabil. Res. 2017, 40, 246–253. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B. Use of the international classification of functioning, disability and health (ICF) to describe patient-reported disability in primary brain tumour in an Australian community cohort. J. Rehabil. Med. 2013, 45, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Nebiker, L.; Lichtenstein, E.; Minghetti, A.; Zahner, L.; Gerber, M.; Faude, O.; Donath, L. Moderating effects of exercise duration and intensity in neuromuscular vs. endurance exercise interventions for the treatment of depression: A meta-analytical review. Front. Psychiatry. 2018, 9, 305. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Brand, S.; Cordes, J.; Malchow, B.; Gerber, M.; et al. EPA Guidance on physical activity as a treatment for severe mental illness: A meta-review of the evidence and position statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur. Psychiatry. 2018, 54, 124–144. [Google Scholar] [CrossRef] [Green Version]
- Giovagnoli, A.R. Investigation of cognitive impairments in people with brain tumors. J. Neurooncol. 2012, 108, 277–283. [Google Scholar] [CrossRef]
- Wefel, J.S.; Noll, K.R.; Scheurer, M.E. Neurocognitive functioning and genetic variation in patients with primary brain tumours. Lancet Oncol. 2016, 17, e97–e108. [Google Scholar] [CrossRef] [Green Version]
- Tymowski, M.; Kaspera, W.; Metta-Pieszka, J.; Zarudzki, Ł.; Ładziński, P. Neuropsychological assessment of patients undergoing surgery due to low-grade glioma involving the supplementary motor area. Clin. Neurol. Neurosurg. 2018, 175, 1–8. [Google Scholar] [CrossRef]
- Brown, P.D.; Buckner, J.C.; O’Fallon, J.R.; Iturria, N.L.; Brown, C.A.; O’Neill, B.P.; Scheithauer, B.W.; Dinapoli, R.P.; Arusell, R.M.; Curran, W.J.; et al. Effects of radiotherapy on cognitive function in patients with low-grade glioma measured by the Folstein mini-mental state examination. J. Clin. Oncol. 2003, 21, 2519–2524. [Google Scholar] [CrossRef] [PubMed]
- Bruno, D.; Schurmann Vignaga, S. Addenbrooke’s cognitive examination III in the diagnosis of dementia: A critical review. Neuropsychiatr. Dis. Treat. 2019, 15, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Granata, C.; Jamnick, N.A.; Bishop, D.J. Principles of exercise prescription, and how they influence exercise-induced changes of transcription factors and other regulators of mitochondrial biogenesis. Sports Med. 2018, 48, 1541–1559. [Google Scholar] [CrossRef] [PubMed]
- Zamani Sani, S.H.; Fathirezaie, Z.; Brand, S.; Puhse, U.; Holsboer-Trachsler, E.; Gerber, M.; Telepasand, S. Physical activity and self-esteem: Testing direct and indirect relationships associated with psychological and physical mechanisms. Neuropsychiatr. Dis. Treat. 2016, 12, 2617–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knapen, J.; van de Vliet, P.; van Coppenolle, H.; David, A.; Peuskens, J.; Pieters, G.; Knapen, K. Comparison of changes in physical self-concept, global self-esteem, depression and anxiety following two different psychomotor therapy programs in nonpsychotic psychiatric inpatients. Psychother. Psychosom. 2005, 74, 353–361. [Google Scholar] [CrossRef] [PubMed]
- McCarty, S.; Eickmeyer, S.M.; Kocherginsky, M.; Keeshin, S.; Shahpar, S.; Semik, P.; Wong, A.W.K. Health-related quality of life and cancer-related symptoms during interdisciplinary outpatient rehabilitation for malignant brain tumor. Am. J. Phys. Med. Rehabil. 2017, 96, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Bates, A.; Gonzalez-Viana, E.; Cruickshank, G.; Roques, T. Guideline committee. Primary and metastatic brain tumours in adults: Summary of NICE guidance. BMJ 2018, 362, k2924. [Google Scholar] [CrossRef]
- Shahpar, S.; Wong, A.W.K.; Keeshin, S.; Eickmeyer, S.M.; Semik, P.; Kocherginsky, M.; McCarty, S. Functional outcomes of an interdisciplinary outpatient rehabilitation program for patients with malignant brain tumors. PM R. 2018, 10, 926–933. [Google Scholar] [CrossRef]
- Kluetz, P.G.; Slagle, A.; Papadopoulos, E.J.; Lee Johnson, L.; Donoghue, M.; Kwiatkowski, V.E.; Chen, W.H.; Sridhara, R.; Farell, A.T.; Keegan, P.; et al. Focusing on core patient-reported outcomes in cancer clinical trials: Symptomatic adverse events, physical function, and disease-related symptoms. Clin. Cancer Res. 2016, 22, 1553–1558. [Google Scholar] [CrossRef] [Green Version]
- Ownsworth, T.; Hawkes, A.; Steginga, S.; Walker, D.; Shum, D. A biopsychosocial perspective on adjustment and quality of life following brain tumor: A systematic evaluation of the literature. Disabil. Rehabil. 2009, 31, 1038–1055. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Inpatient (n = 28) | Outpatient (n = 26) | Both Groups (n = 54) | p-Value | |
|---|---|---|---|---|---|
| Age | Mean ± SD | 54.39 ±13.66 | 47.08 ± 7.77 | 50.87 ± 11.71 | 0.02 |
| Median | 55 | 47 | 49 | p | |
| QR | 43.25–65.25 | 43.25–53 | 43.25–58.25 | ||
| Sex | Female | 14 (50.00%) | 11 (42.31%) | 25 (46.30%) | 0.769 |
| Male | 14 (50.00%) | 15 (57.69%) | 29 (53.70%) | chi 2 | |
| WHO grades of selected CNS tumors according to the 2016 CNS WHO [3] | Diffuse astrocytic and oligodendroglial tumors | 0.716 F | |||
| diffuse astrocytoma II | 3 (10.71%) | 2 (7.69%) | 5 (9.26%) | ||
| oligodendrogliglioma IDH-mutant II | 1 (3.57%) | 0 (0.00%) | 1 (1.85%) | ||
| anaplastic astrocytoma, IDH-mutant III | 2 (7.14%) | 0 (0.00%) | 2 (3.70%) | ||
| glioblastoma, IDH-wildtype IV | 3 (10.71%) | 6 (23.08%) | 9 (16.67%) | ||
| diffuse midline glioma, H3K27M-mutant IV | 1 (3.57%) | 3 (11.54%) | 4 (7.41%) | ||
| Other astrocytic tumors | |||||
| pilocytic astrocytoma I | 0 (0.00%) | 1 (3.85%) | 1 (1.85%) | ||
| subependymal giant cell astrocytoma I | 4 (14.29%) | 2 (7.69%) | 6 (11.11%) | ||
| Ependymal tumors | |||||
| subependynoma I | 1 (3.57%) | 1 (3.85%) | 2 (3.70%) | ||
| ependynoma I/II | 0 (0.00%) | 1 (3.85%) | 1 (1,85%) | ||
| anaplastic ependynoma III | 1 (3.57%) | 0 (0.00%) | 1 (1.85%) | ||
| Meningiomas | |||||
| meningioma I | 7 (25.00%) | 7 (26.92%) | 14 (25.93%) | ||
| atypical meningioma II | 5 (17.86%) | 3 (11.54%) | 8 (14.81%) | ||
| Side of paresis | Left | 14 (50.00%) | 15 (57.69%) | 29 (53.70%) | 0.763 |
| Right | 11 (39.29%) | 10 (38.46%) | 21 (38.89%) | F | |
| Both sides | 3 (10.71%) | 1 (3.85%) | 4 (7.41%) | ||
| Radiotherapy | No | 16 (57.14%) | 13 (50.00%) | 29 (53.70%) | 0.8 |
| Yes | 12 (42.86%) | 13 (50.00%) | 25 (46.30%) | chi 2 | |
| Chemotherapy | No | 24 (85.71%) | 17 (65.38%) | 41 (75.93%) | 0.153 |
| Yes | 4 (14.29%) | 9 (34.62%) | 13 (24.07%) | chi 2 | |
| Parameters | Inpatient (n = 28) Median; QR | Outpatient (n = 26) Median; QR | p-Value |
|---|---|---|---|
| BI | 9; 5.75–13 | 16; 14–16.75 | <0.001 |
| BBS | 29; 13.5–38 | 34.5; 30–42 | 0.007 |
| FIM total | 77; 49.25–89.75 | 91; 84–100.75 | 0.001 |
| FIM self-care | 26; 17–30.5 | 31; 27.25–35 | 0.005 |
| FIM sphincter control | 10; 6.75–12.5 | 12; 10.25–14 | 0.019 * |
| FIM transfers/stability | 13; 6–16 | 14; 12–16 | 0.012 * |
| FIM locomotion | 4.5; 0–10 | 10; 8–12 | 0.002 * |
| FIM communication | 10; 6.75–12 | 10; 10–12 | 0.159 * |
| FIM social cognition | 15; 8–17 | 15; 10–16.75 | 0.727 * |
| ACE III global | 74.5; 53–80 | 77.5; 70.25–80.75 | 0.212 * |
| ACE III attention and orientation | 14; 9.75–17 | 16; 14–17.75 | 0.085 * |
| ACE III memory | 17.5; 10–22 | 19; 15–22 | 0.361 * |
| ACE III language fluency | 9; 4.75–10 | 10; 7.25–11.75 | 0.255 * |
| ACE III language functioning | 20.5; 12.25–24.25 | 21.5; 19.25–24.75 | 0.313 * |
| ACE III visual-spatial functions | 9; 7.75–13.25 | 11; 9–14 | 0.043 |
| MMSE | 22; 19–28.75 | 23; 20–29.5 | 0.144 * |
| Parameters | Rehabilitation Treatment | N | Baseline Mean ± SD | After 12 Weeks Mean ± SD | p-Value |
|---|---|---|---|---|---|
| BI score | IP | 28 | 9.07 ± 4.35 | 14.46 ± 4.76 | <0.001 |
| OP | 26 | 15.27 ± 2.13 | 17.73 ± 1.76 | <0.001 | |
| BBS score | IP | 28 | 25.96 ± 14.52 | 40.18 ± 12.52 | <0.001 |
| OP | 26 | 35.08 ± 8.05 | 43.42 ± 7.69 | <0.001 * | |
| FIM Total score | IP | 28 | 71.29 ± 29.94 | 95.89 ± 29.14 | <0.001 |
| OP | 26 | 93.23 ± 13.15 | 107.35 ± 10.84 | <0.001 | |
| FIM self-care subscale | IP | 28 | 24.57 ± 9.96 | 31.93 ± 9.67 | <0.001 |
| OP | 26 | 31 ± 5.07 | 36.12 ± 4.57 | <0.001 | |
| FIM sphincter control subscale | IP | 28 | 9.29 ± 4.42 | 11.39 ± 4.32 | 0.005 * |
| OP | 26 | 12.12 ± 3.19 | 14.35 ± 3.1 | <0.001 | |
| FIM transfers subscale | IP | 28 | 11.36 ± 6.02 | 15.75 ± 4.76 | <0.001 |
| OP | 26 | 14.69 ± 2.62 | 17.38 ± 2.65 | <0.001 * | |
| FIM locomotion subscale | IP | 28 | 5.36 ± 5.04 | 10.18 ± 4.04 | <0.001 |
| OP | 26 | 9.69 ± 2.72 | 11.85 ± 1.93 | <0.001 * | |
| FIM communication subscale | IP | 28 | 9.29 ± 4.17 | 11.29 ± 3.95 | 0.006 * |
| OP | 26 | 11.27 ± 2.54 | 12.62 ± 2.06 | <0.001 * | |
| FIM social cognition subscale | IP | 28 | 12.71 ± 5.67 | 17.25 ± 5.15 | <0.001 * |
| OP | 26 | 13.77 ± 3.98 | 14.5 ± 3.36 | 0.18 |
| Parameters | Rehabilitation Program | N | Baseline Mean ± SD | After 12 Weeks Mean ± SD | p-Value |
|---|---|---|---|---|---|
| ACE III global | IP | 28 | 65.5 ± 23.77 | 76.79 ± 23.78 | <0.001 |
| OP | 26 | 75.58 ± 11.99 | 82.19 ± 11.23 | <0.001 | |
| ACE III attention and orientation | IP | 28 | 12.89 ± 4.75 | 15.07 ± 4.66 | 0.001 |
| OP | 26 | 15.35 ± 2.91 | 16.88 ± 2.7 | 0.001 | |
| ACE III memory | IP | 28 | 15.75 ± 6.9 | 18.93 ± 7.13 | 0.001 |
| OP | 26 | 17.96 ± 4.85 | 19.42 ± 4.75 | 0.002 | |
| ACE III language fluency | IP | 28 | 8 ± 3.69 | 9.79 ± 4.21 | 0.002 * |
| OP | 26 | 9.19 ± 3.07 | 11.12 ± 2.7 | <0.001 * | |
| ACE III language functioning | IP | 28 | 17.57 ± 8.35 | 20.14 ± 7.22 | 0.001 |
| OP | 26 | 21.23 ± 3.66 | 21.92 ± 3.85 | 0.059 * | |
| ACE III visual-spatial functions | IP | 28 | 9.21 ± 4.61 | 11.43 ± 4.73 | <0.001 |
| OP | 26 | 11.5 ± 3.35 | 12.69 ± 3.02 | 0.006 * |
| Scores | Rehabilitation Program | N | Baseline Mean ± SD | After 12 Weeks Mean ± SD | p-Value |
|---|---|---|---|---|---|
| FACT-Brain Total | IP | 28 | 89.93 ± 6.31 | 113.82 ± 6.13 | <0.001 |
| OP | 26 | 99.31 ± 5.92 | 129.31 ± 5.18 | <0.001 | |
| FACT-General Total | IP | 28 | 45.07 ± 4.74 | 56.64 ± 4.68 | <0.001 |
| OP | 26 | 54.23 ± 3.25 | 66.27 ± 4.07 | <0.001 | |
| FACT–Physical Well-Being | IP | 28 | 11.5 ± 3.37 | 18.43 ± 2.59 | <0.001 |
| OP | 26 | 14.5 ± 2.28 | 21.35 ± 2.33 | <0.001 | |
| FACT–Social/Family Well-Being | IP | 28 | 12.21 ± 1.91 | 10.18 ± 1.83 | <0.001 |
| OP | 26 | 14.58 ± 1.68 | 12.85 ± 1.91 | 0.003 | |
| FACT- Emotional Well-Being | IP | 28 | 9.93 ± 2.23 | 14.82 ± 1.56 | <0.001 |
| OP | 26 | 11.19 ± 2.19 | 14.46 ± 1.56 | <0.001 | |
| FACT–Functional Well-Being | IP | 28 | 11.43 ± 2.15 | 13.21 ± 2.22 | 0.001 |
| OP | 26 | 13.96 ± 2.11 | 17.62 ± 2.04 | <0.001 | |
| FACT–Brain Cancer | IP | 28 | 44.86 ± 3.03 | 57.18 ± 3.45 | <0.001 |
| OP | 26 | 45.08 ± 4.15 | 63.04 ± 4.3 | <0.001 | |
| FACT-Cognitive Total | IP | 28 | 48.61 ± 5.57 | 82.57 ± 7.08 | <0.001 |
| OP | 26 | 64.23 ± 2.42 | 89 ± 4.09 | <0.001 | |
| FACT-Perceived Cognitive Impairments | IP | 28 | 27.32 ± 5.58 | 45.07 ± 5.54 | <0.001 |
| OP | 26 | 34.92 ± 3.08 | 53.73 ± 3.4 | <0.001 * | |
| FACT-Impact of Perceived Cognitive Impairments on QoL | IP | 28 | 3.86 ± 0.89 | 9.21 ± 1.6 | <0.001 |
| OP | 26 | 5.19 ± 0.94 | 8.5 ± 1.33 | <0.001 * | |
| FACT-Comments from Others | IP | 28 | 6.29 ± 1.96 | 9.93 ± 1.7 | <0.001 * |
| OP | 26 | 7.19 ± 1.67 | 9.27 ± 1.69 | <0.001 | |
| FACT-Perceived Cognitive Abilities | IP | 28 | 11.14 ± 1.74 | 18.36 ± 2.66 | <0.001 |
| OP | 26 | 16.92 ± 2.23 | 17.5 ± 1.86 | 0.248 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hojan, K.; Gerreth, K. Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?—A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6488. https://doi.org/10.3390/ijerph17186488
Hojan K, Gerreth K. Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?—A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial. International Journal of Environmental Research and Public Health. 2020; 17(18):6488. https://doi.org/10.3390/ijerph17186488
Chicago/Turabian StyleHojan, Katarzyna, and Karolina Gerreth. 2020. "Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?—A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial" International Journal of Environmental Research and Public Health 17, no. 18: 6488. https://doi.org/10.3390/ijerph17186488