A Smart Service Platform for Cost Efficient Cardiac Health Monitoring



Abstract
:1. Introduction
2. Background
2.1. Atrial Fibrillation
2.2. Sleep Disorders
2.3. Cardiovascular Disease
2.4. Diabetes
2.5. Research Gap
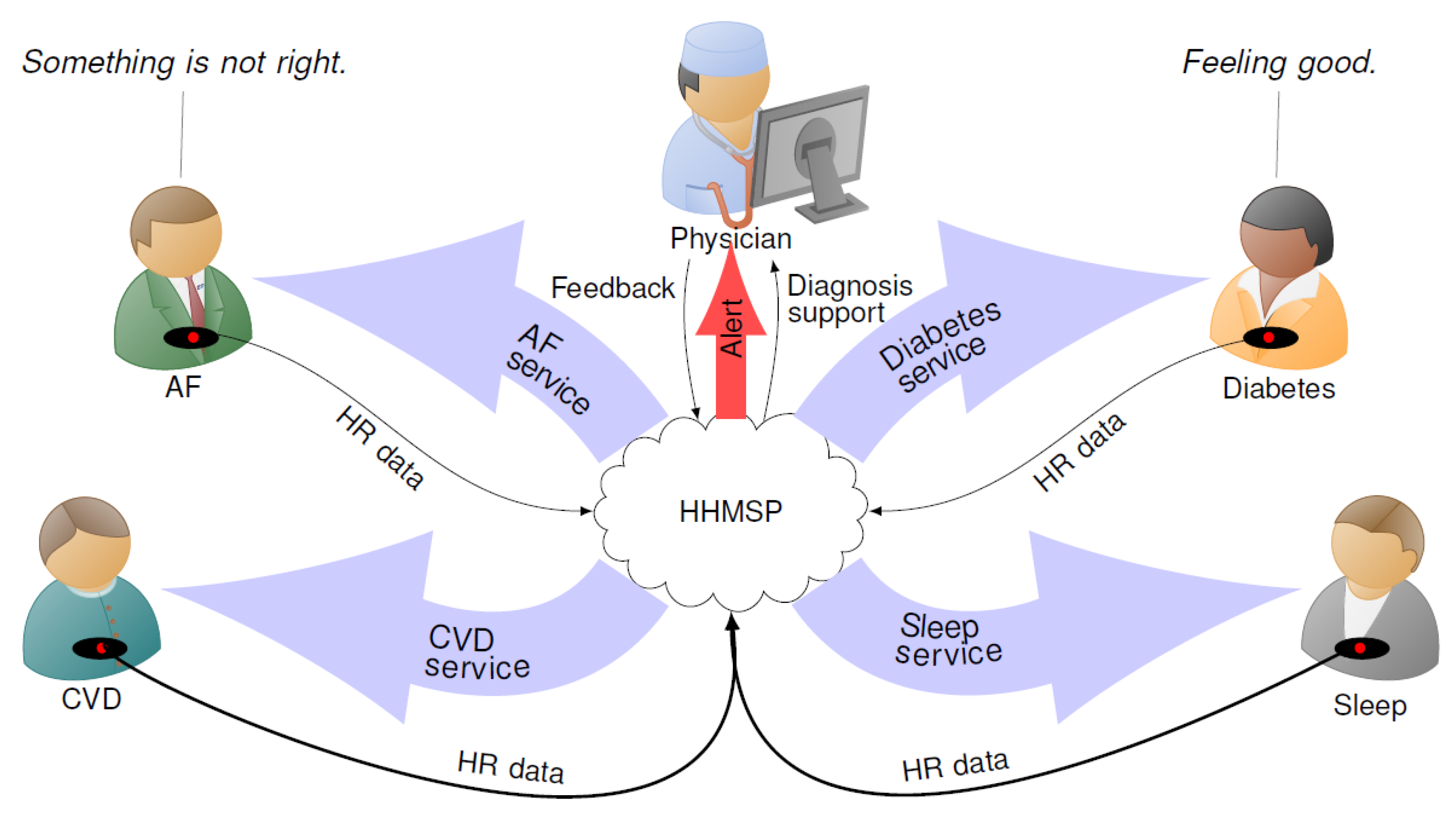
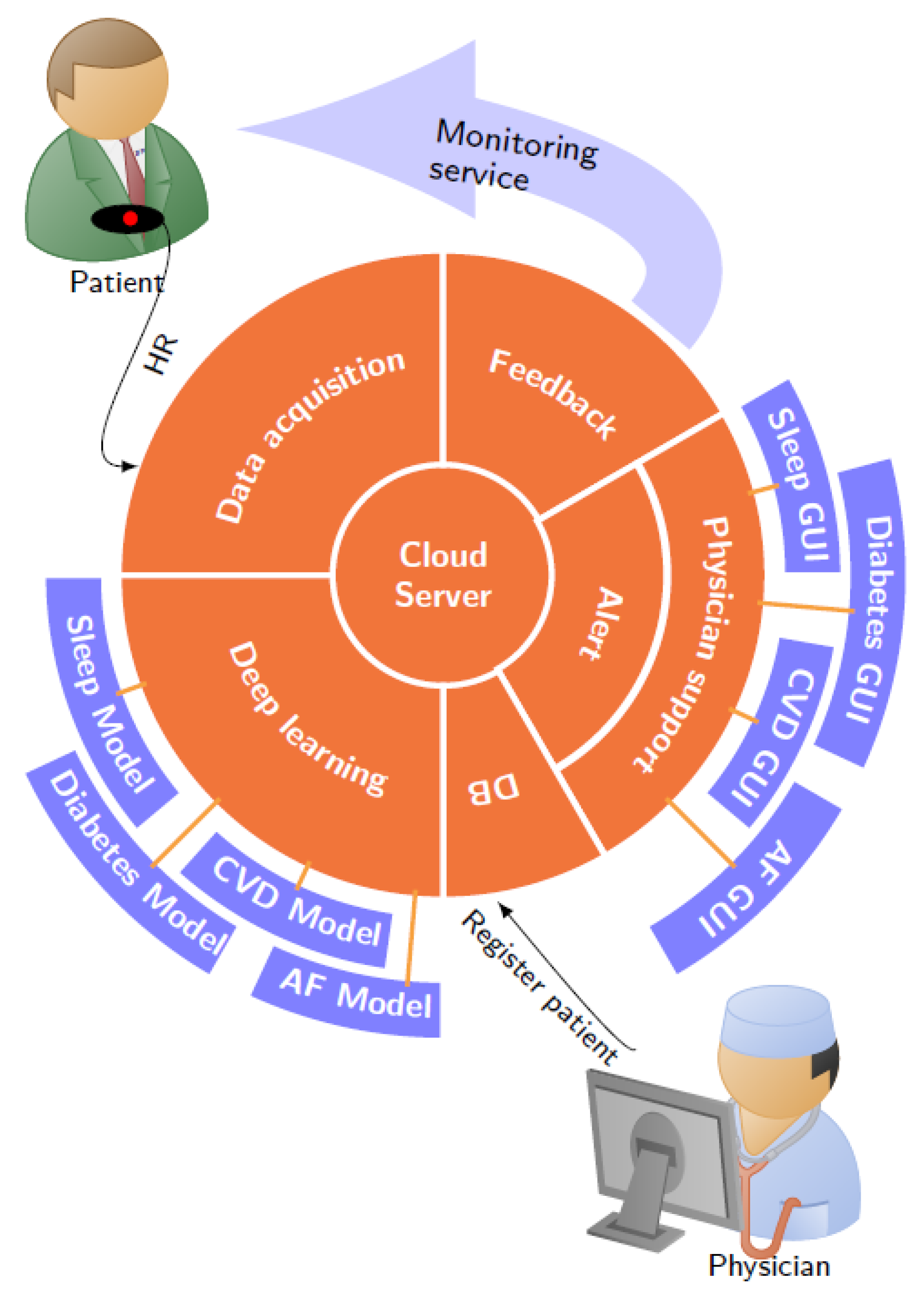
3. System Architecture
3.1. DB Module
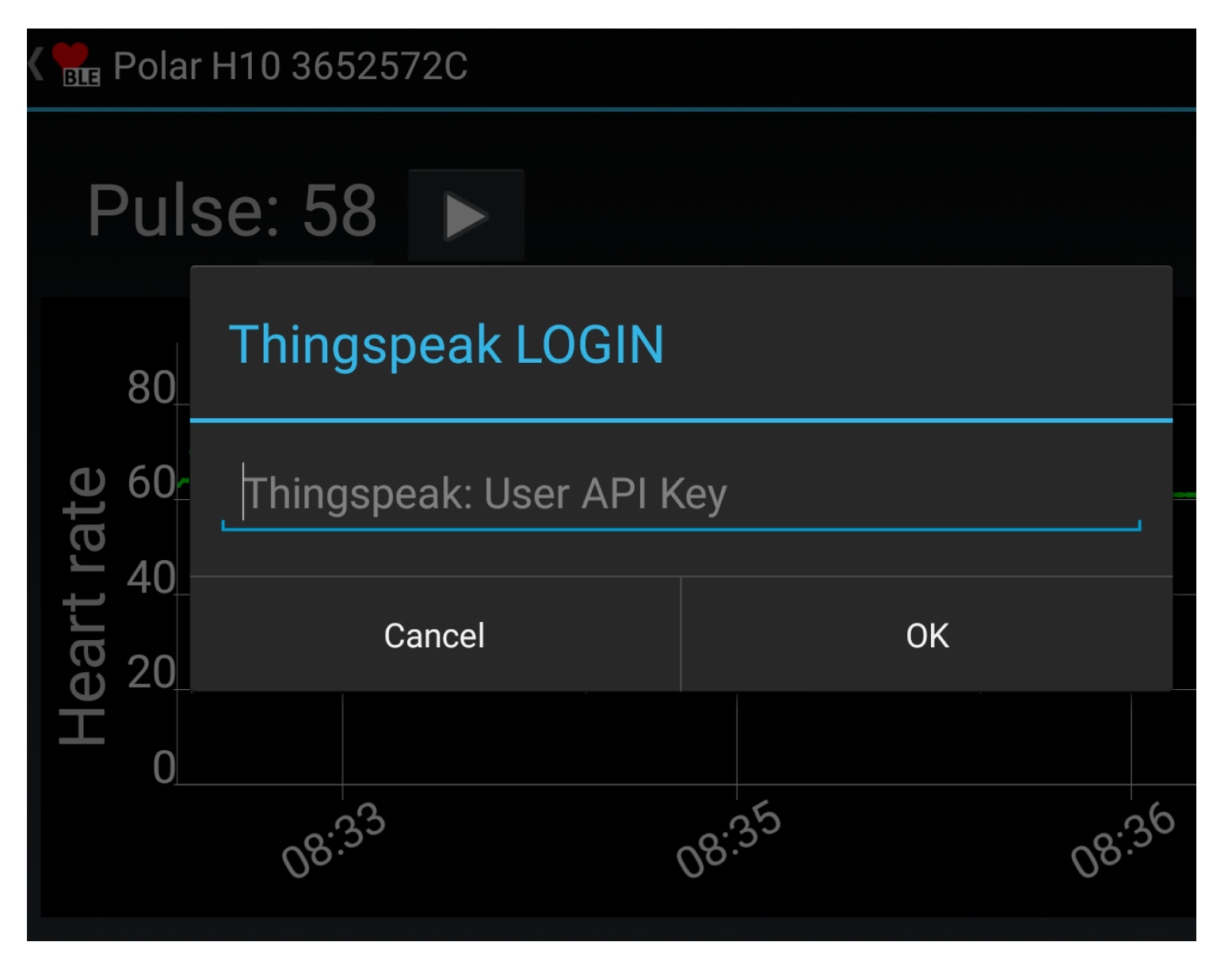
3.2. Data Acquisition Module
3.3. Cloud Server
3.4. Deep Learning Module
3.5. Alert Module
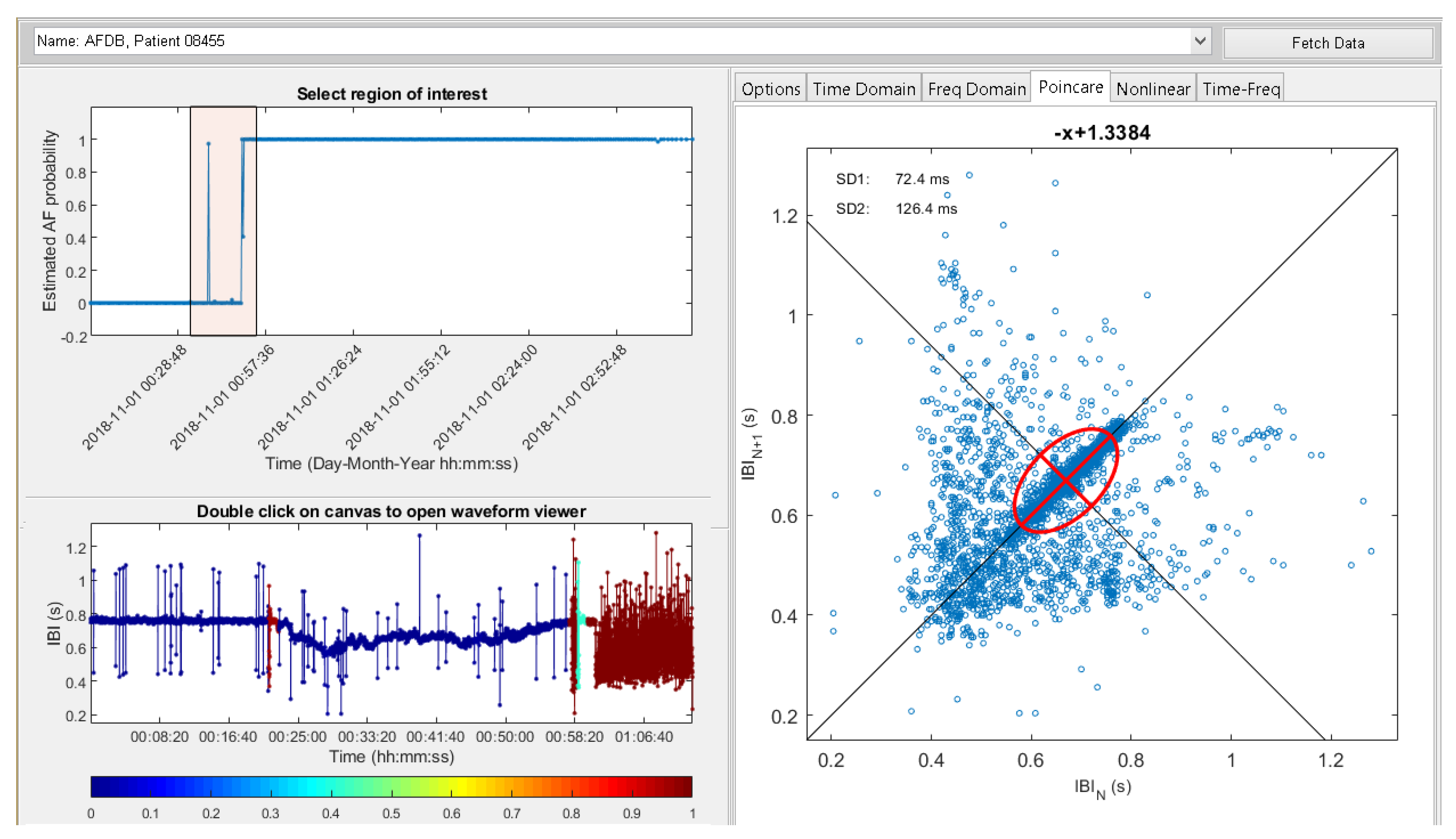
3.6. Physician Support Module
3.7. Feedback Module
3.8. Testing
4. Discussion
4.1. Limitations
4.2. Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Acc | Accuracy |
| AF | Atrial Fibrillation |
| ANS | Autonomic Nervous System |
| AI | Artificial Intelligence |
| CAD | Computer-Aided Diagnosis |
| CArD | Coronary Artery Disease |
| CHF | Congestive Heart Failure |
| CVD | Cardiovascular Disease |
| DB | Database |
| DL | Deep Learning |
| ECG | Electrocardiogram |
| EPR | Electronic Patient Record |
| GUI | Graphical User Interface |
| HHMSP | Heart Health Monitoring Service Platform |
| HIS | Hospital Information System |
| HR | Heart Rate |
| HRV | Heart Rate Variability |
| HRVAS | Heart Rate Variability Analysis Software |
| IoT | Internet of Things |
| K-NN | K-Nearest Neighbour |
| NREM | Non-Rapid Eye Movement |
| NSR | Normal Sinus Rhythm |
| REM | Rapid Eye Movement |
| SCD | Sudden Cardiac Death |
| Sen | Sensitivity |
| Spe | Specificity |
| SVM | Support Vector Machine |
| WHO | World Health Organization |
References
- Chao, T.F.; Lip, G.Y.; Liu, C.J.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P. Relationship of aging and incident comorbidities to stroke risk in patients with atrial fibrillation. J. Am. Coll. Cardiol. 2018, 71, 122–132. [Google Scholar] [CrossRef]
- Pekkarinen, S.; Ulkuniemi, P. Modularity in developing business services by platform approach. Int. J. Logist. Manag. 2008, 84–103. [Google Scholar] [CrossRef]
- Lei, N.; Moon, S.K. A decision support system for market segment driven product design. In Proceedings of the DS 75-9: 19th International Conference on Engineering Design (ICED13), Design for Harmonies, Vol. 9: Design Methods and Tools, Seoul, Korea, 19–22 August 2013; pp. 177–186. [Google Scholar]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Faust, O.; Yi, L.M.; Hua, L.M. Heart rate variability analysis for different age and gender. J. Med Imaging Health Inform. 2013, 3, 395–400. [Google Scholar] [CrossRef]
- Faust, O.; Ciaccio, E.J.; Acharya, U.R. A Review of Atrial Fibrillation Detection Methods as a Service. Int. J. Environ. Res. Public Health 2020, 17, 3093. [Google Scholar] [CrossRef]
- Steinberg, J.S. Atrial fibrillation: An emerging epidemic? Heart 2004, 90, 239–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajpai, A.; Savelieva, I.; Camm, A. Epidemiology and economic burden of atrial fibrillation. US Cardiol. 2007, 4, 14–17. [Google Scholar]
- Hagiwara, Y.; Fujita, H.; Oh, S.L.; Tan, J.H.; San Tan, R.; Ciaccio, E.J.; Acharya, U.R. Computer-aided diagnosis of atrial fibrillation based on ECG signals: A review. Inf. Sci. 2018, 467, 99–114. [Google Scholar] [CrossRef]
- Faust, O.; Hagiwara, Y.; Hong, T.J.; Lih, O.S.; Acharya, U.R. Deep learning for healthcare applications based on physiological signals: A review. Comput. Methods Programs Biomed. 2018, 161, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a New Research Resource for Complex Physiologic Signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, O.; Kareem, M.; Shenfield, A.; Ali, A.; Acharya, U.R. Validating the robustness of an internet of things based atrial fibrillation detection system. Pattern Recognit. Lett. 2020, 133, 55–61. [Google Scholar] [CrossRef]
- Ivanovic, M.D.; Atanasoski, V.; Shvilkin, A.; Hadzievski, L.; Maluckov, A. Deep Learning Approach for Highly Specific Atrial Fibrillation and Flutter Detection based on RR Intervals. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1780–1783. [Google Scholar] [CrossRef]
- Andersen, R.S.; Peimankar, A.; Puthusserypady, S. A deep learning approach for real-time detection of atrial fibrillation. Expert Syst. Appl. 2019, 115, 465–473. [Google Scholar] [CrossRef]
- Faust, O.; Shenfield, A.; Kareem, M.; San, T.R.; Fujita, H.; Acharya, U.R. Automated detection of atrial fibrillation using long short-term memory network with RR interval signals. Comput. Biol. Med. 2018, 102, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henzel, N.; Wróbel, J.; Horoba, K. Atrial fibrillation episodes detection based on classification of heart rate derived features. In Proceedings of the Mixed Design of Integrated Circuits and Systems, 2017 MIXDES-24th International Conference, Bydgoszcz, Poland, 22–24 June 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 571–576. [Google Scholar] [CrossRef]
- Cui, X.; Chang, E.; Yang, W.H.; Jiang, B.; Yang, A.; Peng, C.K. Automated detection of paroxysmal atrial fibrillation using an information based similarity approach. Entropy 2017, 19, 677. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Ammour, N.; Alajlan, N.; Aboalsamh, H. Rhythm based heartbeat duration normalization for atrial fibrillation detection. Comput. Biol. Med. 2016, 72, 160–169. [Google Scholar] [CrossRef]
- Faust, O.; Acharya, U.R.; Ng, E.; Fujita, H. A review of ECG based diagnosis support systems for obstructive sleep apnea. J. Mech. Med. Biol. 2016, 16, 1640004. [Google Scholar] [CrossRef]
- Faust, O.; Razaghi, H.; Barika, R.; Ciaccio, E.J.; Acharya, U.R. A review of automated sleep stage scoring based on physiological signals for the new millennia. Comput. Methods Programs Biomed. 2019, 176, 81–91. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Griffith, K.A.; Nieto, F.J.; O’connor, G.T.; Walsleben, J.A.; Redline, S. The association of sleep-disordered breathing and sleep symptoms with quality of life in the Sleep Heart Health Study. Sleep 2001, 24, 96–105. [Google Scholar] [CrossRef] [Green Version]
- Willemen, T.; Van Deun, D.; Verhaert, V.; Vandekerckhove, M.; Exadaktylos, V.; Verbraecken, J.; Van Huffel, S.; Haex, B.; Vander Sloten, J. An evaluation of cardiorespiratory and movement features with respect to sleep-stage classification. IEEE J. Biomed. Health Informatics 2013, 18, 661–669. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Smirne, S. Prevalence and consequences of insomnia disorders in the general population of Italy. Sleep Med. 2002, 3, 115–120. [Google Scholar] [CrossRef]
- Wickwire, E.M.; Shaya, F.T.; Scharf, S.M. Health economics of insomnia treatments: The return on investment for a good night’s sleep. Sleep Med. Rev. 2016, 30, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Ozminkowski, R.J.; Wang, S.; Walsh, J.K. The direct and indirect costs of untreated insomnia in adults in the United States. Sleep 2007, 30, 263–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viswabhargav, C.S.; Tripathy, R.; Acharya, U.R. Automated detection of sleep apnea using sparse residual entropy features with various dictionaries extracted from heart rate and EDR signals. Comput. Biol. Med. 2019, 108, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Chua, E.C.P.; Faust, O.; Lim, T.C.; Lim, L.F.B. Automated detection of sleep apnea from electrocardiogram signals using nonlinear parameters. Physiol. Meas. 2011, 32, 287. [Google Scholar] [CrossRef]
- Tripathy, R.; Gajbhiye, P.; Acharya, U.R. Automated sleep apnea detection from cardio-pulmonary signal using bivariate fast and adaptive EMD coupled with cross time-frequency analysis. Comput. Biol. Med. 2020, 103769. [Google Scholar] [CrossRef]
- Trinder, J.; Kleiman, J.; Carrington, M.; Smith, S.; Breen, S.; Tan, N.; Kim, Y. Autonomic activity during human sleep as a function of time and sleep stage. J. Sleep Res. 2001, 10, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Penzel, T.; Kantelhardt, J.W.; Grote, L.; Peter, J.H.; Bunde, A. Comparison of detrended fluctuation analysis and spectral analysis for heart rate variability in sleep and sleep apnea. IEEE Trans. Biomed. Eng. 2003, 50, 1143–1151. [Google Scholar] [CrossRef] [Green Version]
- Yajima, Y.; Koyama, T.; Kobayashi, M.; Ichikawa, T.; Hoshino, S.; Abe, H. Continuous Positive Airway Pressure Therapy Improves Heterogeneity of RR intervals in a Patient with Obstructive Sleep Apnea Syndrome. Intern. Med. 2019, 58, 1279–1282. [Google Scholar] [CrossRef] [Green Version]
- Tripathy, R.; Acharya, U.R. Use of features from RR-time series and EEG signals for automated classification of sleep stages in deep neural network framework. Biocybern. Biomed. Eng. 2018, 38, 890–902. [Google Scholar] [CrossRef]
- Yoon, H.; Hwang, S.H.; Choi, J.W.; Lee, Y.J.; Jeong, D.U.; Park, K.S. REM sleep estimation based on autonomic dynamics using R–R intervals. Physiol. Meas. 2017, 38, 631. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Teng, J.; Qi, X.; Wei, S.; Liu, C. Comparison between heart rate variability and pulse rate variability during different sleep stages for sleep apnea patients. Technol. Health Care 2017, 25, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network 1000: Bruxelles, Belgium, 2017. [Google Scholar]
- Sood, S.; Kumar, M.; Pachori, R.B.; Acharya, U.R. Application of empirical mode decomposition- based features for analysis of normal and cad heart rate signals. J. Mech. Med. Biol. 2016, 16, 1640002. [Google Scholar] [CrossRef]
- Mikael, L.d.R.; Paiva, A.M.G.d.; Gomes, M.M.; Sousa, A.L.L.; Jardim, P.C.B.V.; Vitorino, P.V.d.O.; Euzébio, M.B.; Sousa, W.d.M.; Barroso, W.K.S. Vascular aging and arterial stiffness. Arq. Bras. Cardiol. 2017, 109, 253–258. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Wilson, P.W.; Kannel, W.B. Beyond established and novel risk factors: Lifestyle risk factors for cardiovascular disease. Circulation 2008, 117, 3031–3038. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A. Psychological Factors in Cardiovascular Disorders; Academic Press: London, UK, 1981. [Google Scholar]
- Patidar, S.; Pachori, R.B.; Acharya, U.R. Automated diagnosis of coronary artery disease using tunable-Q wavelet transform applied on heart rate signals. Knowl. Based Syst. 2015, 82, 1–10. [Google Scholar] [CrossRef]
- Giri, D.; Acharya, U.R.; Martis, R.J.; Sree, S.V.; Lim, T.C.; VI, T.A.; Suri, J.S. Automated diagnosis of coronary artery disease affected patients using LDA, PCA, ICA and discrete wavelet transform. Knowl. Based Syst. 2013, 37, 274–282. [Google Scholar] [CrossRef]
- Lih, O.S.; Jahmunah, V.; San, T.R.; Ciaccio, E.J.; Yamakawa, T.; Tanabe, M.; Kobayashi, M.; Faust, O.; Acharya, U.R. Comprehensive electrocardiographic diagnosis based on deep learning. Artif. Intell. Med. 2020, 103, 101789. [Google Scholar] [CrossRef]
- Shi, M.; Zhan, C.; He, H.; Jin, Y.; Wu, R.; Sun, Y.; Shen, B. Renyi distribution entropy analysis of short-term heart rate variability signals and its application in coronary artery disease detection. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, D.; Shenoy, A.R.; Prakash, V. Alteration of heart rate variability in patients with coronary artery disease. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 820–823. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.S.; Saini, B.S.; Sunkaria, R.K. Detection of coronary artery disease by reduced features and extreme learning machine. Clujul Med 2018, 91, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yıldız, B.S.; Özkan, E.; Esin, F.; Özkan, H.; Alihanoğlu, Y.İ.; Kılıç, İ.D.; Evrengül, H.; Kaftan, H.A. Evaluation of heart rate variability in patients with coronary artery ectasia and coronary artery disease. Turk Kardiyol Dern Ars 2016, 44, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Pachori, R.B.; Acharya, U.R. An efficient automated technique for CAD diagnosis using flexible analytic wavelet transform and entropy features extracted from HRV signals. Expert Syst. Appl. 2016, 63, 165–172. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global public health burden of heart failure. Card. Fail. Rev. 2017, 3, 7. [Google Scholar] [CrossRef]
- Binder, T.; Frey, B.; Porenta, G.; Heinz, G.; Wutte, M.; Kreiner, G.; Gössinger, H.; Schmidinger, H.; Packer, R.; Weber, H. Prognostic value of heart rate variability in patients awaiting cardiac transplantation. Pacing Clin. Electrophysiol. 1992, 15, 2215–2220. [Google Scholar] [CrossRef]
- Hsu, C.F.; Lin, P.Y.; Chao, H.H.; Hsu, L.; Chi, S. Average Entropy: Measurement of disorder for cardiac RR interval signals. Phys. Stat. Mech. Appl. 2019, 529, 121533. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, L.; Cai, Z.; Liu, F.; Li, Y.; Wei, S.; Li, J.; Murray, A. Effect of Ectopic Beats on Heart Rate Variability Indices in Heart Failure Patients. World Congress on Medical Physics and Biomedical Engineering 2018; Springer: Berlin/Heidelberg, Germany, 2019; pp. 361–365. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Zhou, W.; Liu, N.; Xing, Y.; Zhou, X. CHF Detection with LSTM Neural Network. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 514–517. [Google Scholar] [CrossRef]
- Yoon, K.H.; Nam, Y.; Thap, T.; Jeong, C.; Kim, N.H.; Ko, J.S.; Noh, S.E.; Lee, J. Automatic detection of congestive heart failure and atrial fibrillation with short RR interval time series. J. Electr. Eng. Technol. 2017, 12, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Gao, R. Multiscale entropy analysis of the differential RR interval time series signal and its application in detecting congestive heart failure. Entropy 2017, 19, 251. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Liu, G.; Su, S.; Jiang, Q.; Nguyen, H. A CHF detection method based on deep learning with RR intervals. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 3369–3372. [Google Scholar] [CrossRef]
- Kannel, W.B.; Schatzkin, A. Sudden death: Lessons from subsets in population studies. J. Am. Coll. Cardiol. 1985, 5, 141B–149B. [Google Scholar] [CrossRef] [Green Version]
- Bommer, C.; Sagalova, V.; Heesemann, E.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Davies, J.; Vollmer, S. Global economic burden of diabetes in adults: Projections from 2015 to 2030. Diabetes Care 2018, 41, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dall, T. Undiagnosed diabetes has high economic burden in USA. Pharmacoeconomics Outcomes News 2019, 826, 20–32. [Google Scholar]
- Zhou, X.; Pang, Z.; Gao, W.; Wang, S.; Zhang, L.; Ning, F.; Qiao, Q. Performance of an A1C and fasting capillary blood glucose test for screening newly diagnosed diabetes and pre-diabetes defined by an oral glucose tolerance test in Qingdao, China. Diabetes Care 2010, 33, 545–550. [Google Scholar] [CrossRef] [Green Version]
- Pachori, R.B.; Avinash, P.; Shashank, K.; Sharma, R.; Acharya, U.R. Application of empirical mode decomposition for analysis of normal and diabetic RR-interval signals. Expert Syst. Appl. 2015, 42, 4567–4581. [Google Scholar] [CrossRef]
- Faust, O.; Acharya, U.R.; Molinari, F.; Chattopadhyay, S.; Tamura, T. Linear and non-linear analysis of cardiac health in diabetic subjects. Biomed. Signal Process. Control. 2012, 7, 295–302. [Google Scholar] [CrossRef]
- Acharya, U.R.; Vidya, K.S.; Ghista, D.N.; Lim, W.J.E.; Molinari, F.; Sankaranarayanan, M. Computer-aided diagnosis of diabetic subjects by heart rate variability signals using discrete wavelet transform method. Knowl. Based Syst. 2015, 81, 56–64. [Google Scholar] [CrossRef]
- Acharya, U.R.; Faust, O.; Sree, S.V.; Ghista, D.N.; Dua, S.; Joseph, P.; Ahamed, V.T.; Janarthanan, N.; Tamura, T. An integrated diabetic index using heart rate variability signal features for diagnosis of diabetes. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 222–234. [Google Scholar] [CrossRef]
- Swapna, G.; Rajendra Acharya, U.; VinithaSree, S.; Suri, J.S. Automated detection of diabetes using higher order spectral features extracted from heart rate signals. Intell. Data Anal. 2013, 17, 309–326. [Google Scholar] [CrossRef]
- Yildirim, O.; Talo, M.; Ay, B.; Baloglu, U.B.; Aydin, G.; Acharya, U.R. Automated detection of diabetic subject using pre-trained 2D-CNN models with frequency spectrum images extracted from heart rate signals. Comput. Biol. Med. 2019, 113, 103387. [Google Scholar] [CrossRef]
- Xiao, M.X.; Wei, H.C.; Xu, Y.J.; Wu, H.T.; Sun, C.K. Combination of RR interval and crest time in assessing complexity using multiscale cross-approximate entropy in normal and diabetic subjects. Entropy 2018, 20, 497. [Google Scholar] [CrossRef] [Green Version]
- Swapna, G.; Vinayakumar, R.; Soman, K. Diabetes detection using deep learning algorithms. ICT Express 2018, 4, 243–246. [Google Scholar] [CrossRef]
- Swapna, G.; Kp, S.; Vinayakumar, R. Automated detection of diabetes using CNN and CNN-LSTM network and heart rate signals. Procedia Comput. Sci. 2018, 132, 1253–1262. [Google Scholar] [CrossRef]
- Wilson, L.C.; Peebles, K.C.; Hoye, N.A.; Manning, P.; Sheat, C.; Williams, M.J.; Wilkins, G.T.; Wilson, G.A.; Baldi, J.C. Resting heart rate variability and exercise capacity in Type 1 diabetes. Physiol. Rep. 2017, 5, e13248. [Google Scholar] [CrossRef] [PubMed]
- Faust, O.; Ciaccio, E.J.; Majid, A.; Acharya, U.R. Improving the safety of atrial fibrillation monitoring systems through human verification. Saf. Sci. 2019, 118, 881–886. [Google Scholar] [CrossRef]
- Acharya, U.R.; Faust, O.; Sree, V.; Swapna, G.; Martis, R.J.; Kadri, N.A.; Suri, J.S. Linear and nonlinear analysis of normal and CAD-affected heart rate signals. Comput. Methods Programs Biomed. 2014, 113, 55–68. [Google Scholar] [CrossRef]
- Moody, G. A new method for detecting atrial fibrillation using RR intervals. Comput. Cardiol. 1983, 10, 227–230. [Google Scholar]
- Kamath, G.S.; Cotiga, D.; Koneru, J.N.; Arshad, A.; Pierce, W.; Aziz, E.F.; Mandava, A.; Mittal, S.; Steinberg, J.S. The utility of 12-lead Holter monitoring in patients with permanent atrial fibrillation for the identification of nonresponders after cardiac resynchronization therapy. J. Am. Coll. Cardiol. 2009, 53, 1050–1055. [Google Scholar] [CrossRef] [Green Version]
- Faust, O.; Acharya, R.; Krishnan, S.; Min, L.C. Analysis of cardiac signals using spatial filling index and time-frequency domain. Biomed. Eng. Online 2004, 3, 30. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Data and Method | Performance | ||
|---|---|---|---|---|
| Acc/% | Sen/% | Spe/% | ||
| Faust et al. 2020 [12] | Physionet Long Term AF Database. DL with hold out validation | 94 | - | - |
| Ivanovic et al. 2019 [13] | Private data set. DL | 89.67 | 94.20 | - |
| Andersen et al. 2019 [14] | Physionet: MIT-BIH AF Database, MIT-BIH Arrhythmia Database, and MIT-BIH NSR Database DL | - | 98.98 | 96.95 |
| Faust et al. 2018 [15] | MIT-BIH Atrial Fibrillation Database. DL | 98.51 | 98.32 | 98.67 |
| Henzel et al. 2017 [16] | MIT-BIH Atrial Fibrillation Database. Linear measures & Threshold | 93 | 90 | 95 |
| Cui et al. 2017 [17] | MIT-BIH Atrial Fibrillation Database Ensemble model & Threshold | 97.78 | 97.04 | 97.96 |
| Islam et al. 2016 [18] | MIT-BIH AF database and MIT-BIH Arrhythmia database. Entropy & Threshold | 96.38 | 96.39 | 96.38 |
| Author | Data and Method | Performance | ||
|---|---|---|---|---|
| Acc/% | Sen/% | Spe/% | ||
| Yajima et al. 2019 [32] | One case: 52-year-old man. Statistical features and statistical analysis | - | - | - |
| 1-5 Tripathy et al. 2018 [33] | Fourteen subjects (six female and eight male). Recurrence quantification analysis and dispersion & DL | 95.71% | - | - |
| 1-5 Yoon et al. 2017 [34] | Twenty-one healthy subjects (male: 12, female: 9) and 30 subjects (male: 25, female: 5) with obstructive sleep apnea (OSA). Statistical parameters, Spectral power, variability measurements. Threshold decision | 87.54% | - | - |
| 1-5 Liu et al. 2017 [35] | Seventy-five sleep apnea patients. Time domain statistical parameters, Spectral power, nonlinear measurements evaluated with statistical methods | - | - | - |
| Author | Data and Method | Performance | ||
|---|---|---|---|---|
| Acc/% | Sen/% | Spe/% | ||
| Lih et al. 2020 [44] | Physionet data, no further specifications. DL | 98.5% | 99.30% | 97.89% |
| Shi et al. 2019 [45] | Fantasia and St. Petersburg Institute of Cardiological Technics 12-lead Arrhythmia databases. Wavelet and entropy & K-Nearest Neighbour (K-NN) | 97.5 | 100 | 95 |
| Venkatesh et al. 2018 [46] | Privaate data set. Statistical analysis | - | - | - |
| Singh et al. 2018 [47] | NSR Physionet and St. Petersburg Institute of Cardiological Technics database. Generalized discriminant analysis & extreme learning machine | 100 | - | - |
| Yıldız et al. 2016 [48] | Private data set. Statistical analysis | - | - | - |
| Kumar et al. 2016 [49] | Private data set. FAWT and entropy & LS-Support Vector Machine (SVM) | 100 | - | - |
| Author | Data and Method | Performance | ||
|---|---|---|---|---|
| Acc/% | Sen/% | Spe/% | ||
| Hsuet al. 2019 [52] | BIDMC Congestive Heart Failure Database, MIT-BIH Normal Sinus Rhythm Database, and Long Term AF Database. Average entropy & Threshold | 90 | - | - |
| Liu et al. 2019 [53] | Physionet CHF database. Statistical measures & analysis | - | - | - |
| Wanget et al. 2018 [54] | Physionet CHF database. DL | 85.13 | - | - |
| Yoon et al. 2017 [55] | MIT-BIH Atrial fibrillation, MIT-BIH Normal Sinus Rhythm, BIDMC Congestive Heart Failure, and Congestive Heart Failure RRI databases. CHF & AF detection with statistical methods and threshold decision making | 91.08 | 88.09 | 94.06 |
| Liu and Gao 2017 [56] | Physionet NSR and CHF databases. Multiscale Entropy Analysis & SVM | 85.6 | - | - |
| Chenet et al. 2017 [57] | Physionet CHF and NSR databases. DL | 72.41 | - | - |
| Author | Data and Method | Performance | ||
|---|---|---|---|---|
| Acc/% | Sen/% | Spe/% | ||
| Yildirim et al. 2019 [67] | Private data set. DL | 97.62% | 100% | - |
| Xiao et al. 2018 [68] | Private data set. Multiscale Cross-Approximate Entropy & Statistical analysis | - | - | - |
| Swapna et al. 2018 [69] | Private data set. DL | 95.7 | - | - |
| Swapna et al. 2018 [70] | Private data set. DL | 90.9 | - | - |
| Wilsonet et al. 2017 [71] | Private data set. Linear analysis methods & statistical evaluation | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faust, O.; Lei, N.; Chew, E.; Ciaccio, E.J.; Acharya, U.R. A Smart Service Platform for Cost Efficient Cardiac Health Monitoring. Int. J. Environ. Res. Public Health 2020, 17, 6313. https://doi.org/10.3390/ijerph17176313
Faust O, Lei N, Chew E, Ciaccio EJ, Acharya UR. A Smart Service Platform for Cost Efficient Cardiac Health Monitoring. International Journal of Environmental Research and Public Health. 2020; 17(17):6313. https://doi.org/10.3390/ijerph17176313
Chicago/Turabian StyleFaust, Oliver, Ningrong Lei, Eng Chew, Edward J. Ciaccio, and U Rajendra Acharya. 2020. "A Smart Service Platform for Cost Efficient Cardiac Health Monitoring" International Journal of Environmental Research and Public Health 17, no. 17: 6313. https://doi.org/10.3390/ijerph17176313