Designing a Participatory Total Worker Health® Organizational Intervention for Commercial Construction Subcontractors to Improve Worker Safety, Health, and Well-Being: The “ARM for Subs” Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Theory-Based Models Used to Guide Intervention Design
2.2. Formative Research Conducted to Inform Intervention Design
2.3. Designing the Intervention
Vetting and Refining the Intervention Design with Key Stakeholders and Construction Workers
2.4. Piloting the Intervention
3. Results
3.1. Key Findings from our Formative Research
3.2. Drafting the ARM for Subs Intervention
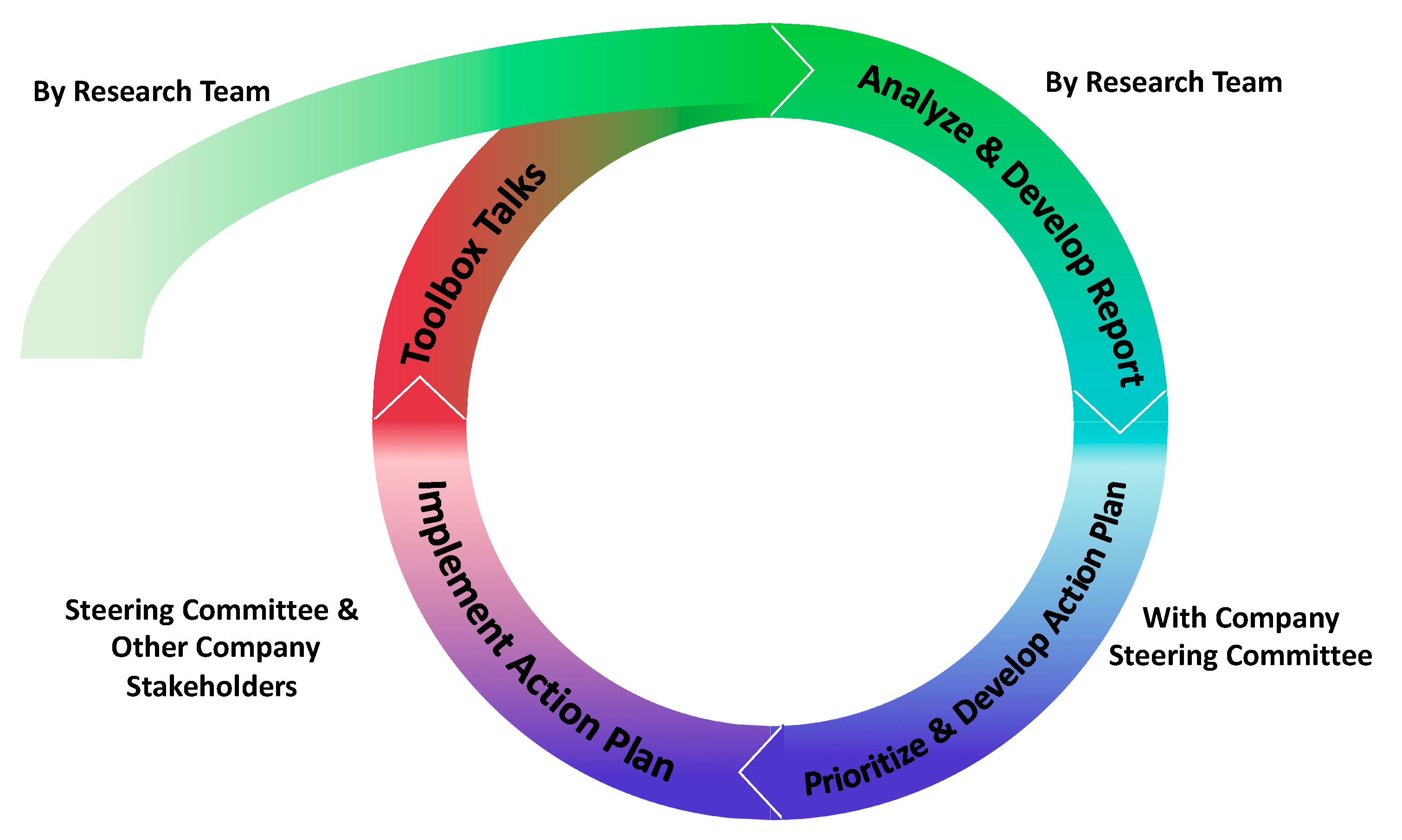
3.2.1. The Continuous Improvement Cycle with the Specific Intervention Components
3.2.2. Cycle 2 and Sustainability of the Program
3.3. The Pilot
3.3.1. Company and Worker Sample
3.3.2. Pilot Cycle 1
- Health effects caused by lack of clean and dedicated areas for meal breaks: This was selected as a short-term “quick win” for the Program that could be easily remedied with a low-cost solution. The plan was quickly agreed upon and implemented shortly thereafter. The operations manager was responsible for purchasing a portable table and chairs to create a clean meal area that could be moved from site-to-site. This was implemented within a week;
- Toxic effects caused by exposure to unknown chemicals in the air and ground during excavation: This was selected as the most important topic area by both workers and managers due to its long-term health consequences and the stress that it was causing workers. Potential solutions were more complex and required changes across multiple systems and organizational levels at the worksite, such as engaging the site’s general contractor. During the planning, the committee realized that the contract between a subcontractor and the general contractor contains information regarding policies for air and soil sampling, and how and what is communicated by the general contractor to the subcontractor. Providing detailed information raised liability considerations from their insurance company—i.e., what are the implications if a certain contaminant is not known at the time and hence not communicated to workers? As a result, two alternate solutions were pursued. One “quick-win” to reduce the uncertainty of exposure was to provide facilities for workers to change out contaminated clothes before leaving the site. Again, the operations manager was responsible for implementing this solution. Another longer-term solution was to update the company’s policy in their safety handbook to allow workers to stop work when a worker identifies a potential hazard from the ground or in the air and to notify the operations manager to escalate and resolve the issue. The specific updated page from the handbook was then printed and placed in employees’ pay-checks so that all workers were told the new policy.
3.3.3. Pilot Cycle 2
3.3.4. Sustainability of the Program at the Pilot Company
3.4. Lessons Learned from the Pilot
- Timing: Our anticipated timeline needed to be extended to 12 weeks as each cycle took approximately three months, instead of the intended 6–8 weeks. This was mainly due to the logistics of setting up meetings and toolbox talks as well the iterative process necessary for action planning for more complex topics. This was also complicated by distributed crew locations, inclement weather, and project timing. Of the three priority topics, one was a quick win, while the other two were more complicated and required more time to go through the iterative steps of brainstorming and determining the feasibility of potential solutions;
- Implementation support: We learned that balancing the amount of information we gave the steering committee at any time was important—too much upfront and they felt overwhelmed, but not enough and they felt lost in the process. A delivery method and format for resources (e.g., in-person training as well as written materials) were needed. Thus, we created FAQs and tip-sheets in simple language for how to complete each of the steps and key intervention activities. Supporting materials needed to be straightforward, easy to follow and brief due to the dynamic and fast nature of construction.
- Tailoring to fit the company: A benefit of the intervention was that it was able to be flexible to the companies’ needs and was able to be adapted to fit within the current systems. All companies have their own characteristics and systems in place. An intervention such as this one should consider using an existing committee to serve as the steering committee to streamline meeting times and locations; and identify other mechanisms for conducting needs assessments that could be easily implemented by companies themselves, e.g., worker quarterly surveys distributed with their pay-checks. We also realized that companies may need to modify our resources to according to their own needs and preferences;
- Capacity building: The company needed a minimum level of training and technical assistance to be able to complete the ARM for Subs program. Companies have limited time during the day to participate in the intervention activities in addition to their usual workload. If you provide too much training, it takes too much time and they also feel overwhelmed; too little, and they do not feel well informed and potentially lose trust in the process. During key informant interviews, steering committee members stated that they benefitted from a research-led cycle followed by a researcher-coached cycle, prior to taking over the ARM for the Subs program themselves.
- The universality of building communication processes within the company: One of the benefits reported was that the company “learned more about their own company”—both the areas that were working well, and areas that could be improved. They also learned that communication was integral to ensuring leadership commitment to the program and worker buy-in. TTs were moved to earlier in the intervention cycle so that they were delivered in the week after the report was generated, rather than at the end of the intervention cycle. The company reported that workers provided them with constructive information that could benefit the company by enhancing workers safety and health systems, and also quality and productivity outcomes.
- Adaptability and sustainability: Exploring structures that already existed and could be tapped into by the steering committee, allowed the company to see that the approach used in this program could be easily integrated and potentially sustained. The cyclical design of the intervention allowed us to demonstrate to the company the processes in the first cycle, with the second cycle allowing the company to adapt and ‘own’ the process, which helped to demonstrate the sustainability of the program over the long-term.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tamers, S.L.; Chosewood, L.C.; Childress, A.; Hudson, H.; Nigam, J.; Chang, C.C. Total Worker Health(R) 2014–2018: The Novel Approach to Worker Safety, Health, and Well-Being Evolves. Int. J. Environ. Res. Public Health 2019, 16, 321. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, G.; McLellan, D.L.; Sabbath, E.L.; Dennerlein, J.T.; Nagler, E.M.; Hurtado, D.A.; Pronk, N.P.; Wagner, G.R. Integrating worksite health protection and health promotion: A conceptual model for intervention and research. Prev. Med. 2016, 91, 188–196. [Google Scholar] [CrossRef] [Green Version]
- Umer, W.; Antwi-Afari, M.F.; Li, H.; Szeto, G.P.Y.; Wong, A.Y.L. The prevalence of musculoskeletal symptoms in the construction industry: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2018, 91, 125–144. [Google Scholar] [CrossRef]
- Pronk, N.P.; McLellan, D.L.; McGrail, M.P.; Olson, S.M.; McKinney, Z.J.; Katz, J.N.; Wagner, G.R.; Sorensen, G. Measurement Tools for Integrated Worker Health Protection and Promotion: Lessons Learned From the SafeWell Project. J. Occup. Environ. Med. 2016, 58, 651–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, G.; Barbeau, E.M. Integrating occupational health, safety and worksite health promotion: Opportunities for research and practice. Med. Lav 2006, 97, 240–257. [Google Scholar]
- U.S. Bureau of Labor Statistics. Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work, 2013–2014; U.S. Department of Labor: Washington, DC, USA; p. 31. Available online: https://www.bls.gov/opub/ted/2015/nonfatal-occupational-injuries-and-illnesses-requiring-days-away-from-work-in-2014.htm. (accessed on 1 July 2019).
- Viester, L.; Verhagen, E.; Bongers, P.M.; van der Beek, A.J. Effectiveness of a Worksite Intervention for Male Construction Workers on Dietary and Physical Activity Behaviors, Body Mass Index, and Health Outcomes: Results of a Randomized Controlled Trial. Am. J. Health Promot 2018, 32, 795–805. [Google Scholar] [CrossRef] [Green Version]
- Dietz, A.; Ramroth, H.; Urban, T.; Ahrens, W.; Becher, H. Exposure to cement dust, related occupational groups and laryngeal cancer risk: Results of a population based case-control study. Int. J. Cancer 2004, 108, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, N.; Wada, O. Silicosis and smoking strongly increase lung cancer risk in silica-exposed workers. J. Ind. Health 2004, 42, 303–314. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.N. Relation between exposure to asbestos and smoking jointly and the risk of lung cancer. Occup. Environ. Med. 2001, 58, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.M.; Lipari, R.N. Substance Use and Substance Use Disorder by Industry. In The CBHSQ Report: Short Report; Substance Abuse and Mental Health Services Administration (US): Rockville, MD, USA, 2015. [Google Scholar]
- Borsting Jacobsen, H.; Caban-Martinez, A.; Onyebeke, L.C.; Sorensen, G.; Dennerlein, J.T.; Endresen Reme, S. Construction Workers Struggle With a High Prevalence of Mental Distress, and This Is Associated With Their Pain and Injuries. J. Occup. Environ. Med. 2013, 55, 1197–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntosh, W.L.; Spies, E.; Stone, D.M.; Lokey, C.N.; Trudeau, A.T.; Bartholow, B. Suicide Rates by Occupational Group—17 States, 2012. Morb. Mortal. Wkly. Rep. (MMWR) 2016, 65, 641–645. [Google Scholar] [CrossRef] [PubMed]
- U.S. Bureau of Labor Statistics. Summary Table 1-Incidence Rates-Detailed Industry Level; U.S. Department of Labor: Washington, DC, USA, 2018.
- Amick, B.C.; Habeck, R.V.; Hunt, A.; Fossel, A.H.; Chapin, A.; Keller, R.B.; Katz, J.N. Measuring the impact of organizational behaviors on work disability prevention and management. J. Occup. Rehabil. 2000, 10, 21–38. [Google Scholar] [CrossRef]
- National Research Council (NRC) and Institute of Medicine (U.S.) Panel of Musculoskeletal Disorders and Workplace. Musculoskeletal Disorders and the Workplaces: Low Back and Upper Extremities; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Eyllon, M.; Vallas, S.P.; Dennerlein, J.T.; Garverich, S.; Weinstein, D.; Owens, K.; Lincoln, A.K. Mental Health Stigma and Wellbeing Among Commercial Construction Workers: A Mixed Methods Study. J. Occup. Environ. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- McLellan, D.; Moore, W.; Nagler, E.; Sorensen, G. Implementing an Integrated Approach Weaving Worker Health, Safety, and Well-Being into the Fabric of Your Organization; Harvard Center for Work, Health and Wellbeing: Cambridge, MA, USA, 2017; p. 141. [Google Scholar]
- Kitt, M.; Howard, J. The face of occupational safety and health: 2020 and beyond. Public Health Rep. 2013, 128, 138–139. [Google Scholar] [CrossRef] [Green Version]
- Weil, D. The Fissured Workplace Why Work Became so Bad for so Many and What Can Be Done to Improve it; Harvard University Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Weil, D. The Contemporary Industrial Relations System in Construction: Analysis, Observations and Speculations. Labor Hist. 2005, 46, 447–471. [Google Scholar] [CrossRef]
- Valluru, C.T.; Dekker, S.; Rae, A. How and why do subcontractors experience different safety on high-risk work sites? Cogn. Tech. Work 2017, 19, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Sparer, E.H.; Murphy, L.A.; Taylor, K.M.; Dennerlein, J.T. Correlation between safety climate and contractor safety assessment programs in construction. Am. J. Ind. Med. 2013, 56, 1463–1472. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.H.; Tessler, J.; Murphy, L.A.; Chang, C.C.; Dennerlein, J.T. The Gap Between Tools and Best Practice: An Analysis of Safety Prequalification Surveys in the Construction Industry. New Solut. 2019, 28, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Sparer, E.H.; Herrick, R.F.; Dennerlein, J.T. Development of a safety communication and recognition program for construction. New Solut. 2015, 25, 42–58. [Google Scholar] [CrossRef] [Green Version]
- Manjourides, J.; Dennerlein, J.T. Testing the associations between leading and lagging indicators in a contractor safety pre-qualification database. Am. J. Ind Med. 2019, 62, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.E.; Grant, M.P.; Rodgers, J.; Manjourides, J.; Okechukwu, C.A.; Dennerlein, J.T. A Cluster Randomized Controlled Trial of a Total Worker Health® Intervention on Commercial Construction Sites. Int. J. Environ. Res. Public Health 2018, 15, 2354. [Google Scholar] [CrossRef] [Green Version]
- Dennerlein, J.T.; Weinstein, D.; Huynh, W.; Tessler, J.; Bigger, L.; Murphy, L.A.; Manjourides, J. Associations between a safety prequalification survey and worker safety experiences on commercial construction sites. Am. J. Ind. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Eng, E.; Schulz, A.J.; Parker, E.A. Methods in Community-Based Participatory Research for Health, 2nd ed.; John Wiley & Sons: San Francisco, CA, USA, 2012. [Google Scholar]
- Bartholomew Eldridge, L.K.; Markham, C.M.; Ruiter, R.A.C.; Fernandez, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs An. Intervention Mapping Approach, 4th ed.; John Wiley and Sons, Inc.: San Francsico, CA, USA, 2016. [Google Scholar]
- Sparer, E.H.; Sheldon, A.; Dennerlein, J.T. B-SAFE: Bulding Safety for Everyone. Available online: http://www.northeastern.edu/b-safe/ (accessed on 11 November 2015).
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef] [Green Version]
- Sparer, E.H.; Catalano, P.J.; Herrick, R.F.; Dennerlein, J.T. Improving safety climate through a communication and recognition program for construction: A mixed methods study. Scand. J. Work Environ. Health 2016, 42, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Small Business Administration Office Of Advocacy. Small Business Profile United States. 2018. Available online: https://www.sba.gov/sites/default/files/advocacy/2018-Small-Business-Profiles-US.pdf (accessed on 26 June 2020).
- U.S. Bureau of Labor Statistics. Establishments with Fewer than 50 Workers Employed 60 Percent of Construction Workers in March 2016. Available online: https://www.bls.gov/opub/ted/2017/establishments-with-fewer-than-50-workers-employed-60-percent-of-construction-workers-in-march-2016.htm (accessed on 26 June 2020).
- Nielsen, K.; Miraglia, M. What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Work Stress 2017, 70, 40–62. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.E.; Nielsen, K.; Nagler, E.M.; Revette, A.C.; Madden, J.R.; Sorensen, G. Ensuring organization-intervention fit for a participatory organizational intervention to improve food service workers’ health and wellbeing: Workplace Organizational Health Study. J. Occup. Environ. Med. 2020, 62, e33–e45. [Google Scholar] [CrossRef] [PubMed]
- Abildgaard, J.S.; Hasson, H.; von Thiele Schwarz, U.; Løvseth, L.T.; Ala-Laurinaho, A.; Nielsen, K. Forms of participation: The development and application of a conceptual model of participation in work environment interventions. Econ. Ind. Democr. 2018. [Google Scholar] [CrossRef] [Green Version]
- Minkler, M.; Blackwell, A.G.; Thompson, M.; Tamir, H. Community-based participatory research: Implications for public health funding. Am. J. Public Health 2003, 93, 1210–1213. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R. The importance of employee participation and perceptions of changes in procedures in a teamworking intervention. Work Stress 2012, 26, 91–111. [Google Scholar] [CrossRef] [Green Version]
- Abildgaard, J.S.; Nielsen, K. The interplay of sensemaking and material artefacts during interventions: A case study. Nord. J. Work. Life Stud. 2019, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Holte, K.A.; Kjestveit, K.; Lipscomb, H.J. Company size and differences in injury prevalence among apprentices in building and construction in Norway. Saf. Sci. 2015, 71, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Masi, D.; Cagno, E. Barriers to OHS interventions in small and medium-sized enterprises. Saf. Sci. 2015, 71, 226–241. [Google Scholar] [CrossRef]
- Micheli, G.J.L.; Cagno, E.; Calabrese, A. The Transition from Occupational Safety and Health (OSH) Interventions to OSH Outcomes: An Empirical Analysis of Mechanisms and Contextual Factors within Small and Medium-Sized Enterprises. Int. J. Environ. Res. Public Health 2018, 15, 1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ipsen, C.; Gish, L.; Poulsen, S. Organizational-level interventions in small and medium-sized enterprises: Enabling and inhibiting factors in the PoWRS program. Saf. Sci. 2015, 71, 264–274. [Google Scholar] [CrossRef] [Green Version]
- Hasle, P.; Limborg, H.J.; Kallehave, T.; Klitgaard, C.; Andersen, T.R. The working environment in small firms: Responses from owner-managers. Int. Small Bus. J. 2012, 30, 622–639. [Google Scholar] [CrossRef]
- Masi, D.; Cagno, E.; Micheli, G.J.L. Developing, implementing and evaluations OSH interventions in SMEs: A pilot, exploratory study. Int. J. Occup. Saf. Ergon. 2014, 20, 385–405. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Challenges Faced by Subcontractors | Assets That Could Contribute to Successful Intervention Implementation |
|---|---|
|
|
| Intervention Components | Description of Activities | Anticipated Timing | Adapatation Made during Pilot | Future Recommendations Based on Pilot |
|---|---|---|---|---|
| Needs Assessment (NA) to determine workers’ experiences | ITTs over 3 days facilitated by research team | Week 1 | ITTs were conducted over 2 weeks due to multiple sites. Some sites had 2 ITTs on same day | Allowed flexibility in ITTs timing to meet company’s needs |
| Provided resources for company to complete their own NA | ||||
| Develop Steering Committee (SC) | Workers and managers invited to participate in an intervention SC | Week 1 | SC composition and location changed to work with existing structures | Adapted SC so company can use existing committee if one is present |
| Report generated by Research Team | Using NA data, a report is generated using a systematic iterative process | Week 2 | No adaptations were made to the report. However, an we added a meeting to review the report with company leadership prior to the first SC meeting. | Add review of the report by company leadership prior to first SC meeting |
| Prioritization of intervention topics by SC | Training on prioritization and action planning process | Week 3 | Company selected more than one topic area per cycle as some topics were quick wins and some required longer. | Company can select more than one topic area per cycle. |
| Review report | Developed FAQs and tip sheets to support in-person training | |||
| Prioritize intervention focus area | ||||
| Action planning and implementation of strategies | Steering committee meetings to develop action plans | Weeks 4–8 | Action planning took approx. three months to complete a cycle | Increased time for each cycle |
| Implement action plans between meetings | ||||
| Toolbox Talks (TT) with workers | Toolbox talks on NA topics | Week 8 | No adaptations made | Moved TTs earlier in the intervention cycle |
| Toolbox talk to communicate action plans | Developed new TTs based on company’s priority NA topics | Developed new TTs based on company’s NA topics | ||
| Sustainability of the program | Continuing the cycles | After the program | Company adapted activities to fit with existing systems and structures | Developed FAQs/tipsheets for companies on how to complete activities themselves |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peters, S.E.; Trieu, H.D.; Manjourides, J.; Katz, J.N.; Dennerlein, J.T. Designing a Participatory Total Worker Health® Organizational Intervention for Commercial Construction Subcontractors to Improve Worker Safety, Health, and Well-Being: The “ARM for Subs” Trial. Int. J. Environ. Res. Public Health 2020, 17, 5093. https://doi.org/10.3390/ijerph17145093
Peters SE, Trieu HD, Manjourides J, Katz JN, Dennerlein JT. Designing a Participatory Total Worker Health® Organizational Intervention for Commercial Construction Subcontractors to Improve Worker Safety, Health, and Well-Being: The “ARM for Subs” Trial. International Journal of Environmental Research and Public Health. 2020; 17(14):5093. https://doi.org/10.3390/ijerph17145093
Chicago/Turabian StylePeters, Susan E., Hao D. Trieu, Justin Manjourides, Jeffrey N. Katz, and Jack T. Dennerlein. 2020. "Designing a Participatory Total Worker Health® Organizational Intervention for Commercial Construction Subcontractors to Improve Worker Safety, Health, and Well-Being: The “ARM for Subs” Trial" International Journal of Environmental Research and Public Health 17, no. 14: 5093. https://doi.org/10.3390/ijerph17145093