An Epidemiological Study on the Prevalence of the Clinical Features of SARS-CoV-2 Infection in Romanian People



Abstract
:1. Introduction
- (1)
- A patient with an acute respiratory infection, with sudden onset, having met at least one of three clinical criteria (cough, fever, shortness of breath/increased respiratory rate), without another aetiology that fully explains the clinical picture and with international travel history, within 14 days prior to symptom onset.
- (2)
- A patient with an acute respiratory infection, having been in close contact with a confirmed case of COVID-19 within 14 days prior to symptom onset.
- (3)
- A patient with pneumonia or severe acute respiratory infection (SARI), without another aetiology that fully explains the clinical picture.
2. Materials and Methods
2.1. Premises and Aim of the Study
2.2. Participants
2.3. Data Acquisition
2.4. Outcomes and Statistical Analysis
3. Results
3.1. Respondents
3.2. Sociodemographic Characteristics of Study Participants
3.3. Health Status Characteristics of Study Participants
3.4. Multiple Response Analysis
3.5. Reliability of the Survey Section for Clinical Features of SARS-CoV-2 Infection
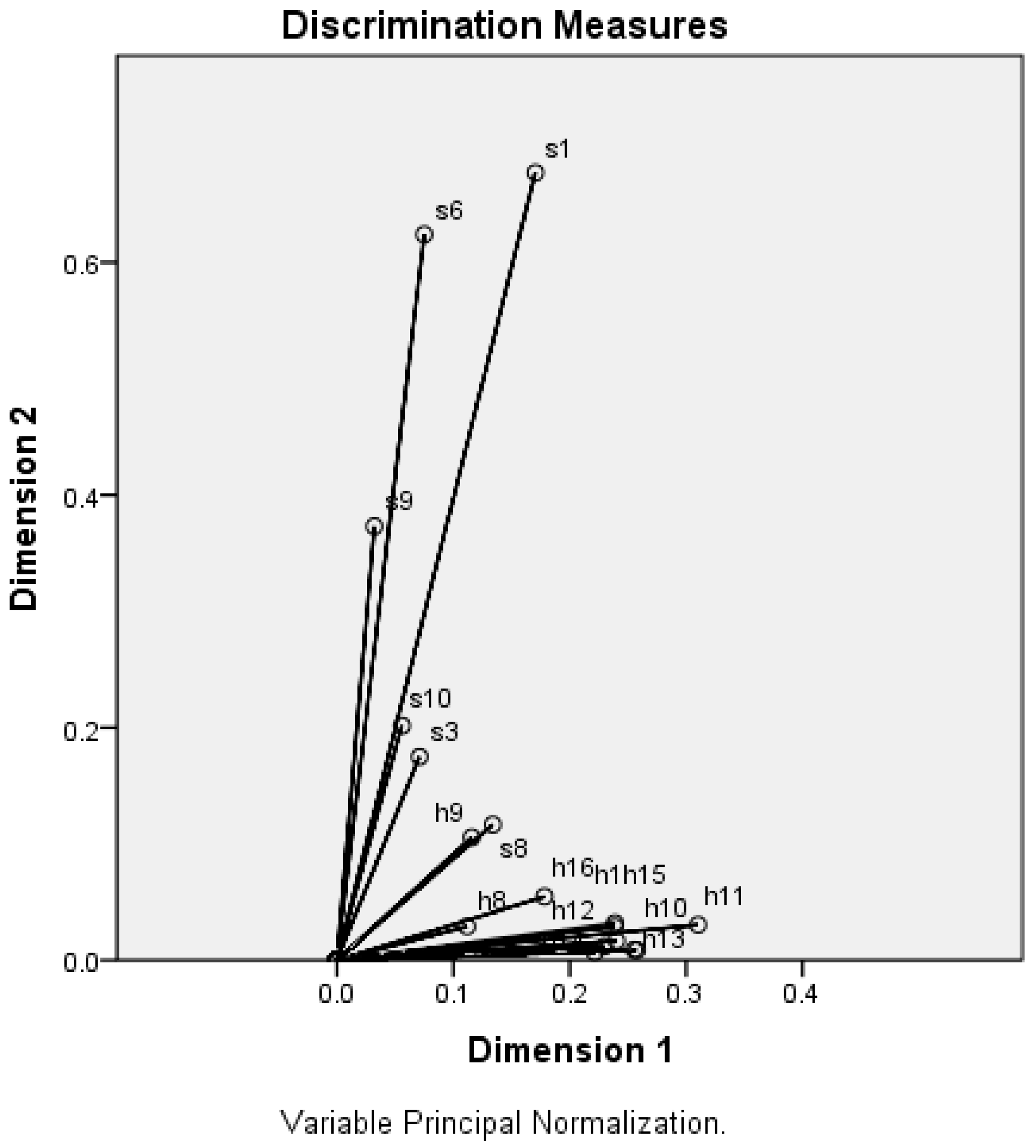
3.6. Categorical Principal Component Analysis (CATPCA) with Optimal Scaling
3.7. Two-Step Clustering Analysis
- (1)
- Cluster 1 (n = 491): participants mostly pupils/students (81.5%), young (mean age 22.77 years), with excellent or very good health (83.3%), self-insulated or confined at home (85.7%), who present in a very small proportion the analysed clinical features (between 0–1.2%).
- (2)
- Cluster 2 (n = 619): participants mostly employed (58.2%), mostly young adults (mean age 33.38 years), in very good or good health (79.6%), self-insulated or confined at home (68.8%), who present in a higher proportion the analysed clinical features (1.4–57.4%).
- (3)
- Cluster 3 (n = 720): participants mostly employed (83.6%), mostly adults (mean age 41.01 years), with excellent or very good health (65.3), heterogeneous in terms of social isolation, who present in very small proportion the analysed clinical features (0–2.2%).
3.8. Binomial Logistic Regression Analysis
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- European Centre for Disease Prevention and Control (ECDP). Rapid risk Assessment: Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK—Eighth Update; EU Publications: Solna, Sweden, 2020; Available online: https://www.ecdc.europa.eu/en/publications-data/rapid-risk-assessment-coronavirus-disease-2019-covid-19-pandemic-eighth-update (accessed on 9 April 2020).
- Purcell, L.N.; Charles, A.G. Invited Commentary on “World Health Organization declares global emergency: A review of the 2019 novel Coronavirus (COVID-19)”: Emergency or new reality? Int. J. Surg. 2020, 76, 111. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Public Health Romania (NIPHR). Rapid Analysis of Confirmed Cases with of Coronavirus Infection (COVID-19), Romania, 26 February–5 April 2020; NIPHR: Bucharest, Romania, 2020. Available online: https://www.cnscbt.ro/index.php/1643-analiza-cazuri-confirmate-pana-la-5-04-2020/file (accessed on 10 April 2020).
- Li, T. Diagnosis and clinical management of severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) infection: An operational recommendation of Peking Union Medical College Hospital (V2.0). Emerg. Microbes Infect. 2020, 9, 582–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Su, L.; Ma, X.; Yu, H.; Zhang, Z.; Bian, P.; Han, Y.; Sun, J.; Liu, Y.; Yang, C.; Geng, J.; et al. The different clinical characteristics of corona virus disease cases between children and their families in China—the character of children with COVID-19. Emerg. Microbes Infect. 2020, 9, 707–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: A cross-sectional study. Clin. Infect. Dis. 2020, ciaa330. [Google Scholar] [CrossRef] [Green Version]
- Day, M. Covid-19: Four fifths of cases are asymptomatic, China figures indicate. BMJ 2020, 369, m1375. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Public Health Romania (NIPHR). Document Prepared by National Center for Surveillance and Control of Communicable Diseases. Case Definitions for Acute Respiratory Syndrome with the New Coronavirus (COVID-19) Update 27.03.2020; NIPHR: Bucharest, Romania, 2020. Available online: http://www.cnscbt.ro/index.php/info-medical/1594-definitia-de-caz-covid-19-actualizare-27-03-2020/file (accessed on 10 April 2020).
- Kolifarhood, G.; Aghaali, M.; Mozafar Saadati, H.; Taherpour, N.; Rahimi, S.; Izadi, N. Epidemiological and Clinical Aspects of COVID-19: A Narrative Review. Arch. Acad. Emerg. Med. 2020, 8, e41. [Google Scholar]
- World Health Organization (WHO). Laboratory Testing Strategy Recommendations for COVID-19. Interim Guidance 22 March 2020; WHO: Geneva, Switzerland, 2020; Available online: https://www.cnscbt.ro/index.php/1590-who-covid-19-lab-testing-2020-1-eng/file (accessed on 10 April 2020).
- National Institute of Public Health Romania (NIPHR). Document Prepared by National Center for Surveillance and Control of Communicable Diseases. Test Algorithm for COVID-19, Hospitalization and Discharge, Update 10.04.2020; NIPHR: Bucharest, Romania, 2020. Available online: https://www.cnscbt.ro/index.php/info-medical/1649-algoritm-testare-internare-externare-10-04-2020/file (accessed on 12 April 2020).
- Pan, X.B. Application of personal-oriented digital technology in preventing transmission of COVID-19, China. Ir. J. Med. Sci. 2020, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Kamel Boulos, M.N.; Geraghty, E.M. Geographical tracking and mapping of coronavirus disease COVID-19/severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: How 21st century GIS technologies are supporting the global fight against outbreaks and epidemics. Int. J. Health Geogr. 2020, 19, 8. [Google Scholar] [CrossRef] [Green Version]
- Stoet, G. PsyToolkit—A software package for programming psychological experiments using Linux. Behav. Res. Methods 2010, 42, 1096–1104. [Google Scholar] [CrossRef]
- Stoet, G. PsyToolkit: A novel web-based method for running online questionnaires and reaction-time experiments. Teach. Psychol. 2017, 44, 24–31. [Google Scholar] [CrossRef]
- Taber, S.K. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Cronbach, L. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Linting, M.; Meulman, J.J.; Groenen, P.J.; van der Koojj, A.J. Nonlinear principal components analysis: Introduction and application. Psychol. Methods 2007, 12, 336–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattell, R.B. The scree test for the number of factors. Multivariate Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef] [PubMed]
- Zeijl, E. Young adolescent leisure. In A Cross-Cultural and Cross-Sectional Study of Dutch and German 10–15 Years-Olds; Opladen: Leske, Budrich, 2001; pp. 82–84. [Google Scholar]
- Van den Berge, M.J.C.; Free, R.H.; Arnold, R.; de Kleine, E.; Hofman, R.; van Dijk, J.M.C.; van Dijk, P. Cluster analysis to identify possible subgroups in tinnitus patients. Front. Neurol. 2017, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Public Health Romania (NIPHR). Situation of Coronavirus Infections (COVID 19) 8.04.2020; NIPHR: Bucharest, Romania, 2020. Available online: https://www.cnscbt.ro/index.php/situatia-la-nivel-global-actualizata-zilnic/1641-situatie-infectii-coronavirus-covid-19-8-04-2020/file (accessed on 14 April 2020).
- Meo, S.A.; Alhowikan, A.M.; Al-Khlaiwi, T.; Meo, I.M.; Halepoto, D.M.; Iqbal, M.; Usmani, A.M.; Hajjar, W.; Ahmed, N. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2012–2019. [Google Scholar] [CrossRef]
- Lupia, T.; Scabini, S.; Mornese Pinna, S.; Di Perri, G.; De Rosa, F.G.; Corcione, S. 2019 novel coronavirus (2019-nCoV) outbreak: A new challenge. J. Glob. Antimicrob. Resist. 2020, 21, 22–27. [Google Scholar] [CrossRef]
- Wu, X.; Cai, Y.; Huang, X.; Yu, X.; Zhao, L.; Wang, F.; Li, Q.; Gu, S.; Xu, T.; Li, Y.; et al. Co-infection with SARS-CoV-2 and Influenza A Virus in Patient with Pneumonia, China. Emerg. Infect. Dis. 2020, 26, 1324–1326. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Euro. Surveill. 2020, 25, 2000180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Ling, E.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; et al. COVID-19 Antibody Seroprevalence in Santa Clara County, California. medRxiv 2020. [Google Scholar] [CrossRef]
- Raoult, D.; Zumla, A.; Locatelli, F.; Ippolito, G.; Kroemer, G. Coronavirus infections: Epidemiological, clinical and immunological features and hypotheses. Cell Stress 2020, 4, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Al-Almaie, S.M. Ability of adult patients to predict absence or presence of fever in an emergency department triage clinic. J. Fam. Community Med. 1999, 6, 29–34. [Google Scholar]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.; Morwitzer, M.J.; Creager, H.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.; Schnaubelt, E.; Broadhurst, M.J.; et al. Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical Center. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Baggett, T.P.; Keyes, H.; Sporn, N.; Gaeta, J.M. Prevalence of SARS-CoV-2 infection in residents of a large komeless shelter in Boston. JAMA 2020. [Epub ahead of print]. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.B.; Roope, L.S.J.; Barnett, A.; Hunter, D.J.; Nolan, T.M.; Clarke, P.M. Group Testing for SARS-CoV-2: Forward to the Past? Pharmacoecon Open 2020, 4, 207–210. [Google Scholar] [CrossRef]
- Matheeussen, V.; Loens, K.; Lammens, C.; Vilken, T.; Koopmans, M.; Goossens, H.; Ieven, M. Preparedness of European diagnostic microbiology labs for detection of SARS-CoV-2, March 2020. J. Clin. Virol. 2020, 128, 104432. [Google Scholar] [CrossRef]
- Gasmi, A.; Noor, S.; Tippairote, T.; Dadar, M.; Menzel, A.; Bjørklund, G. Individual risk management strategy and potential therapeutic options for the COVID-19 pandemic. Clin. Immunol. 2020, 108409. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Chow, N.; Fleming-Dutra, K.; Gierke, R.; Hall, A.; Hughes, M.; Pilishvili, T.; Ritchey, M.; Roguski, K.; Skoff, T.; Ussery, E. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019—United States, February 12 March 28, 2020. Morb. Mortal Wkly Rep. (MMWR) 2020, 69, 382–386. [Google Scholar] [CrossRef]
- Deiana, G.; Azara, A.; Dettori, M.; Delogu, F.; Vargiu, G.; Gessa, I.; Stroscio, F.; Tidore, M.; Steri, G.; Castiglia, P. Deaths in SARS-Cov-2 Positive Patients in Italy: The Influence of Underlying Health Conditions on Lethality. Int. J. Environ. Res. Public Health 2020, 17, 4450. [Google Scholar] [CrossRef]
- Halpin, D.M.; Farber, R.; Sibila, O.; Badia, J.R.; Agusti, A. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir. Med. 2020, 8, 436–438. [Google Scholar] [CrossRef]
- Jefferson, T.; Del Mar, C.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; Rivetti, A. Physical interventions to interrupt or reduce the spread of respiratory viruses: Systematic review. BMJ 2009, 339, b3675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, M.; Gao, L.; Cheng, C.; Zhou, Q.; Uy, J.P.; Heiner, K.; Sun, C. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Song, R.; Han, B.; Song, M.; Wang, L.; Conlon, C.P.; Dong, T.; Tian, D.; Zhang, W.; Chen, Z.; Zhang, F.; et al. Clinical and epidemiological features of COVID-19 family clusters in Beijing, China. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cianetti, S.; Pagano, S.; Nardone, M.; Lombardo, G. Model for Taking Care of Patients with Early Childhood Caries during the SARS-Cov-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 3751. [Google Scholar] [CrossRef]
- Tostmann, A.; Bradley, J.; Bousema, T.; Yiek, W.K.; Holwerda, M.; Bleeker-Rovers, C.; ten Oever, J.; Meijer, C.; Rahamat-Langendoen, J.; Hopman, J.; et al. Strong associations and moderate predictive value of early symptoms for SARS-CoV-2 test positivity among healthcare workers, the Netherlands, March 2020. Eurosurveillance 2020, 25, 2000508. [Google Scholar] [CrossRef]


{kind=link}
| Item Code | Variable | Frequency (n) | Percent (%) |
|---|---|---|---|
| s1 | Age | ||
| 4–17 years | 49 | 2.7 | |
| 18–50 years | 1567 | 85.6 | |
| 51–64 years | 180 | 9.8 | |
| 65–90 years | 34 | 1.9 | |
| s2 | Sex | ||
| Male | 494 | 27 | |
| Female | 1336 | 73 | |
| s3 | Domicile (42 districts) | ||
| District 3 (Arges) | 1144 | 62.5 | |
| District 42 (Bucharest) | 152 | 8.3 | |
| Rest of districts | 534 | 29.2 | |
| s4 | Type of current residence | ||
| Urban | 1303 | 71.2 | |
| Rural | 527 | 28.8 | |
| s5 | Type of housing | ||
| Individual building | 966 | 52.8 | |
| Collective building | 864 | 47.2 | |
| s6 | Social status | ||
| Toddler/pre-schooler | 3 | 0.2 | |
| Pupil/Student | 583 | 31.8 | |
| Employee | 1033 | 56.4 | |
| Freelancer | 95 | 5.2 | |
| Unemployed | 17 | 0.9 | |
| Retired | 54 | 3 | |
| Housewife/househusband | 45 | 2.5 | |
| s7 | Travel abroad in the last month | ||
| Yes | 55 | 3 | |
| No | 1775 | 97 | |
| s8 | Contact with a confirmed SARS-CoV-2 case | ||
| Yes | 6 | 0.3 | |
| No | 1294 | 70.7 | |
| I don’t know | 530 | 29 | |
| s9 | Current situation related to the social distancing imposed by law | ||
| Quarantine | 69 | 3.8 | |
| Self-insulated | 831 | 45.4 | |
| Hospitalized | 1 | 0.1 | |
| Confined at home | 417 | 22.8 | |
| In the workplace | 253 | 13.8 | |
| Another situation | 259 | 14.1 | |
| s10 | Average number of contacts with people in the last two weeks | ||
| None | 165 | 9 | |
| 1–5 people | 1246 | 68.1 | |
| 6–10 people | 197 | 10.8 | |
| More than 10 people | 222 | 12. |
| Item Code | Variable | Frequency (n) | Percent (%) |
|---|---|---|---|
| h1 | Qualitative self-assessment of the health status | ||
| Excellent | 363 | 19.8 | |
| Very good | 821 | 44.9 | |
| Good | 560 | 30.6 | |
| Satisfying | 75 | 4.1 | |
| Weak | 11 | 0.6 | |
| h2 | Testing for SARS-CoV-2 virus | ||
| Tested positive | 0 | 0 | |
| Tested negative | 8 | 0.4 | |
| Non-tested | 1822 | 99.6 | |
| h3 | Maximum level of physical activity achieved in the last two weeks | ||
| Very easy | 438 | 23.9 | |
| Mild | 462 | 25.3 | |
| Moderate | 745 | 40.7 | |
| Vigorous | 142 | 7.8 | |
| Very heavy | 22 | 1.2 | |
| Maximal | 21 | 1.1 | |
| h4 | Smoking | ||
| Yes | 510 | 27.9 | |
| No | 1320 | 72.1 | |
| h5 | Pathological personal history 1—chronic cardiovascular diseases | ||
| Yes | 112 | 6.1 | |
| No | 1718 | 93.9 | |
| Pathological personal history 2—chronic respiratory diseases | |||
| Yes | 56 | 3.1 | |
| No | 1774 | 96.9 | |
| Pathological personal history 3—chronic neurological diseases | |||
| Yes | 19 | 1 | |
| No | 1811 | 99 | |
| Pathological personal history 4—chronic renal diseases | |||
| Yes | 26 | 1.4 | |
| No | 1804 | 98.6 | |
| Pathological personal history 5—chronic rheumatic diseases | |||
| Yes | 87 | 4.8 | |
| No | 1743 | 95.2 | |
| Pathological personal history 6—diabetes mellitus | |||
| Yes | 22 | 1.2 | |
| No | 1808 | 98.8 | |
| Pathological personal history 7—oncological diseases | |||
| Yes | 12 | 0.7 | |
| No | 1818 | 99.3 | |
| Pathological personal history 8—others | |||
| Yes | 97 | 5.3 | |
| No | 1733 | 94.7 | |
| Pathological personal history 9—none | |||
| Without chronic diseases | 1484 | 81.1 | |
| With chronic diseases | 346 | 18.9 | |
| h6 | Influenza or acute respiratory infections in the last 6 months | ||
| Yes | 457 | 25 | |
| No | 1373 | 75 | |
| h7 | Influenza vaccination in the last 6 months | ||
| Yes | 150 | 8.2 | |
| No | 1680 | 91.8 | |
| h8 | Clinical feature 1—fever in the last 14 days | ||
| Yes | 21 | 1.1 | |
| No | 1809 | 98.9 | |
| h9 | Clinical feature 2—maximum body temperature measured in the last 14 days | ||
| 36.5 °C | 684 | 37.4 | |
| 37 °C | 186 | 10.2 | |
| 37.5 °C | 40 | 2.2 | |
| 38 °C | 7 | 0.4 | |
| 38.5 °C | 6 | 0.3 | |
| Non-measured | 907 | 49.5 | |
| h10 | Clinical feature 3—chills and/or increased perspiration in the last 14 days | ||
| Yes | 61 | 3.3 | |
| No | 1769 | 96.7 | |
| h11 | Clinical feature 4—increased fatigue in the last 14 days | ||
| Yes | 161 | 8,8 | |
| No | 1669 | 91.2 | |
| h12 | Clinical feature 5—episodes of persistent dry or productive cough in the last 14 days | ||
| Yes | 154 | 8.4 | |
| No | 1676 | 91.6 | |
| h13 | Clinical feature 6—sore throat or dry throat sensation in the last 14 days | ||
| Yes | 355 | 19.4 | |
| No | 1475 | 80.6 | |
| h14 | Clinical feature 7—chest pain or chest pressure sensation in the last 14 days | ||
| Yes | 99 | 5.4 | |
| No | 1731 | 94.6 | |
| h15 | Clinical feature 8—dyspnoea (breathing difficulty), suffocation and/or shortness of breath in the last 14 days | ||
| Yes | 82 | 4.5 | |
| No | 1748 | 95.5 | |
| h16 | Clinical feature 9—headache in the last 14 days | ||
| Yes | 606 | 33.1 | |
| No | 1224 | 66.9 | |
| h17 | Clinical feature 10—muscle and/or joint pain in the last 14 days | ||
| Yes | 265 | 14.5 | |
| No | 1565 | 85.5 | |
| h18 | Clinical feature 11—nasal congestion/leakage of nasal secretions in the last 14 days | ||
| Yes | 381 | 20.8 | |
| No | 1449 | 79.2 | |
| h19 | Clinical feature 12—diarrhoea, nausea, loss of appetite and/or vomiting in the last 14 days | ||
| Yes | 93 | 5.1 | |
| No | 1737 | 94.9 | |
| h20 | Clinical feature 13—loss of taste and/or odour in the last 14 days | ||
| Yes | 14 | 0.8 | |
| No | 1816 | 99.2 | |
| h21 | Face mask wearing outside the home in the last 14 days | ||
| Always | 852 | 46.6 | |
| Occasionally | 566 | 30.9 | |
| Never | 412 | 22.5 | |
| h22 | Anxiety level in the context of the pandemic with SARS-CoV-2 | ||
| Not anxious | 350 | 19.1 | |
| Mild anxious | 747 | 40.8 | |
| Moderately anxious | 563 | 30.8 | |
| Very anxious | 133 | 7.3 | |
| Extremely anxious | 37 | 2 |
| Responses | Percent of Cases | |||
|---|---|---|---|---|
| n | Percent | |||
| Items a | h8 | 21 | 0.9% | 2.1% |
| h10 | 61 | 2.7% | 6.0% | |
| h11 | 161 | 7.0% | 15.8% | |
| h12 | 154 | 6.7% | 15.2% | |
| h13 | 355 | 15.5% | 34.9% | |
| h14 | 99 | 4.3% | 9.7% | |
| h15 | 82 | 3.6% | 8.1% | |
| h16 | 606 | 26.4% | 59.6% | |
| h17 | 265 | 11.6% | 26.1% | |
| h18 | 381 | 16.6% | 37.5% | |
| h19 | 93 | 4.1% | 9.2% | |
| h20 | 14 | 0.6% | 1.4% | |
| Total | 2292 | 100.0% | 225.6% | |
| h8 | h10 | h11 | h12 | h13 | h14 | h15 | h16 | h17 | h18 | h19 | h20 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| h8 | 1.000 | |||||||||||
| h10 | 0.237 | 1.000 | ||||||||||
| h11 | 0.093 | 0.265 | 1.000 | |||||||||
| h12 | 0.078 | 0.163 | 0.191 | 1.000 | ||||||||
| h13 | 0.103 | 0.186 | 0.218 | 0.269 | 1.000 | |||||||
| h14 | 0.065 | 0.144 | 0.190 | 0.154 | 0.176 | 1.000 | ||||||
| h15 | 0.125 | 0.122 | 0.231 | 0.248 | 0.174 | 0.357 | 1.000 | |||||
| h16 | 0.077 | 0.141 | 0.212 | 0.130 | 0.254 | 0.155 | 0.117 | 1.000 | ||||
| h17 | 0.072 | 0.174 | 0.327 | 0.155 | 0.195 | 0.149 | 0.129 | 0.212 | 1.000 | |||
| h18 | 0.058 | 0.122 | 0.135 | 0.252 | 0.232 | 0.109 | 0.091 | 0.223 | 0.118 | 1.000 | ||
| h19 | 0.092 | 0.096 | 0.165 | 0.073 | 0.144 | 0.154 | 0.106 | 0.154 | 0.159 | 0.151 | 1.000 | |
| h20 | −0.009 | 0.089 | 0.083 | 0.109 | 0.084 | 0.034 | 0.042 | 0.005 | 0.071 | 0.109 | 0.065 | 1.000 |
| Dimension | Cronbach’s Alpha | Variance Accounted For | ||
|---|---|---|---|---|
| Total (Eigenvalue) | Inertia | % of Variance | ||
| 1 | 0.701 | 2.937 | 0.173 | 17.277 |
| 2 | 0.638 | 2.501 | 0.147 | 14.710 |
| Total | 5.438 | 0.320 | ||
| Mean | 0.672 a | 2.719 | 0.160 | 15.993 |
| Dimension | Mean | ||
|---|---|---|---|
| 1 | 2 | ||
| s1 | 0.171 | 0.677 | 0.424 |
| s3 | 0.071 | 0.175 | 0.123 |
| s6 | 0.075 | 0.624 | 0.350 |
| s8 | 0.134 | 0.117 | 0.125 |
| s9 | 0.032 | 0.373 | 0.203 |
| s10 | 0.056 | 0.202 | 0.129 |
| h1 | 0.239 | 0.029 | 0.134 |
| h8 | 0.112 | 0.029 | 0.070 |
| h9 | 0.116 | 0.106 | 0.111 |
| h10 | 0.255 | 0.009 | 0.132 |
| h11 | 0.310 | 0.030 | 0.170 |
| h12 | 0.230 | 0.012 | 0.121 |
| h13 | 0.258 | 0.009 | 0.133 |
| h14 | 0.221 | 0.007 | 0.114 |
| h15 | 0.240 | 0.017 | 0.128 |
| h16 | 0.178 | 0.055 | 0.116 |
| h17 | 0.239 | 0.032 | 0.135 |
| Active Total | 2.937 | 2.501 | 2.719 |
| % of Variance | 17.277 | 14.710 | 15.993 |
| Item Code | Variable | Cluster 1 n = 491 | Cluster 2 n = 619 | Cluster 3 n = 720 | p Value |
|---|---|---|---|---|---|
| s6 | Social status (%) | p < 0.001 a | |||
| Toddler/pre-schooler | 0.6% | 0 | 0 | ||
| Pupil/Student | 81.5% | 29.6% | 0 | ||
| Employee | 14.5% | 58.2% | 83.6% | ||
| Freelance | 0 | 6.1% | 7.9% | ||
| Unemployed | 0.6% | 0.8% | 1.2% | ||
| Retired | 0 | 2.1% | 5.7% | ||
| Housewife/househusband | 2.9% | 3.2% | 1.5% | ||
| h13 | Clinical feature 6—sore throat or dry throat sensation in the last 14 days (%) | p < 0.001 a | |||
| Yes | 0 | 57.4% | 0 | ||
| No | 100% | 42.6% | 100% | ||
| s1 | Age (mean ± SD, years) | 22.77 ± 6.45 | 33.38 ± 12.84 | 41.01 ± 11.59 | p < 0.001 b |
| h17 | Clinical feature 10—muscle and/or joint pain in the last 14 days (%) | p < 0.001 a | |||
| Yes | 1.2% | 39.3% | 2.2% | ||
| No | 98.8% | 60.7% | 97.8% | ||
| h11 | Clinical feature 4—increased fatigue in the last 14 days (%) | p < 0.001 a | |||
| Yes | 0.2% | 25.5% | 0.3% | ||
| No | 99.8% | 74.5% | 99.7% | ||
| h12 | Clinical feature 5—episodes of persistent dry or productive cough in the last 14 days (%) | p < 0.001 a | |||
| Yes | 1% | 23.1% | 0.8% | ||
| No | 99% | 76.9% | 99.2% | ||
| s9 | Current situation related to the social distancing imposed by law | p < 0.001 a | |||
| Quarantine | 7.7% | 4.2% | 0.7% | ||
| Self-insulated | 50.9% | 48% | 39.4% | ||
| Hospitalized | 0.2% | 0 | 0 | ||
| Confined at home | 34.8% | 20.8% | 16.2% | ||
| In the workplace | 0.6% | 16.3% | 20.7% | ||
| Another situation | 5.7% | 10.7% | 22.9% | ||
| h14 | Clinical feature 7—chest pain or chest pressure sensation in the last 14 days (%) | p < 0.001 a | |||
| Yes | 1.2% | 1.4% | 0.1% | ||
| No | 98.8% | 85.1% | 99.9% | ||
| h15 | Clinical feature 8—dyspnoea (breathing difficulty), suffocation and/or shortness of breath in the last 14 days (%) | p < 0.001 a | |||
| Yes | 0.4% | 12.9% | 0 | ||
| No | 99.6% | 87.1% | 100% | ||
| h1 | Qualitative self-assessment of the health status (%) | p < 0.001 a | |||
| Excellent | 32% | 10.8% | 19.3% | ||
| Very good | 51.1% | 38.6% | 46% | ||
| Good | 16.5% | 41% | 31.2% | ||
| Satisfying | 0.2% | 8.4% | 3.1% | ||
| Weak | 0.2% | 1.1% | 0.4% | ||
| h10 | Clinical feature 3—chills and/or increased perspiration in the last 14 days (%) | p < 0.001 a | |||
| Yes | 0% | 9.9% | 0 | ||
| No | 100% | 90.1% | 100% |
| Independent Variable | Omnibus Test of Model Coefficients | Model Summary | Regression Coefficients and Significance Level | |||||
|---|---|---|---|---|---|---|---|---|
| Chi-Square | p-Value | Nagelkerke R Square | Predictor | B | OR = Exp(B) | 95% CI for OR | p-Value | |
| h10 | 37.575 | 0.001 | 0.080 | h6 | 1.188 | 3.281 | 1.942–5.542 | 0.001 |
| h11 | 52.059 | 0.001 | 0.062 | h4 | 0.573 | 1.774 | 1.254–2.509 | 0.001 |
| h5 * | 0.724 | 2.062 | 1.376–3.091 | 0.001 | ||||
| h6 | 0.791 | 2.205 | 1.571–3.095 | 0.001 | ||||
| h21 (1) | −0.549 | 0.578 | 0.382–0.873 | 0.009 | ||||
| h12 | 118.563 | 0.001 | 0.143 | s5 | −0.434 | 0.648 | 0.428–0.982 | 0.041 |
| h4 | 0.662 | 1.938 | 1.348–2.786 | 0.001 | ||||
| h5 * | 0.706 | 2.026 | 1.343–3.058 | 0.001 | ||||
| h6 | 1.554 | 4.729 | 3.341–6.693 | 0.001 | ||||
| h13 | 43.370 | 0.001 | 0.037 | h6 | 0.722 | 2.059 | 1.602–2.646 | 0.001 |
| h14 | 36.785 | 0.001 | 0.058 | h4 | 0.842 | 2.322 | 1.522–3.543 | 0.001 |
| h5 * | 0.621 | 1.860 | 1.126–3.072 | 0.015 | ||||
| h6 | 0.574 | 1.776 | 1.156–2.728 | 0.009 | ||||
| h21 (1) | −0.688 | 0.502 | 0.298–0.847 | 0.010 | ||||
| h15 | 62.828 | 0.001 | 0.110 | h4 | 0.690 | 1.994 | 1.238–3.212 | 0.005 |
| h5 * | 1.334 | 3.796 | 2.271–6.343 | 0.001 | ||||
| h6 | 0.954 | 2.596 | 1.640–4.109 | 0.001 | ||||
| h21 (1) | −0.995 | 0.370 | 0.205–0.666 | 0.001 | ||||
| h21 (2) | −0.709 | 0.492 | 0.282–0.859 | 0.013 | ||||
| h16 | 94.766 | 0.001 | 0.070 | s1 | 0.027 | 1.028 | 1.019–1.037 | 0.001 |
| s2 | −0.384 | 0.681 | 0.538–0.862 | 0.001 | ||||
| h4 | 0.404 | 1.498 | 1.203–1.866 | 0.001 | ||||
| h5 * | 0.299 | 1.348 | 1.021–1.780 | 0.035 | ||||
| h6 | 0.424 | 1.528 | 1.218–1.915 | 0.001 | ||||
| h17 | 58.030 | 0.001 | 0.055 | h4 | 0.429 | 1.536 | 1.154–2.043 | 0.003 |
| h5 * | 0.731 | 2.078 | 1.499–2.882 | 0.001 | ||||
| h6 | 0.612 | 1.844 | 1.392–2.444 | 0.001 | ||||
| h18 | 50.597 | 0.001 | 0.043 | s1 | 0.11 | 1.011 | 1.001–1.021 | 0.028 |
| h4 | 0.294 | 1.342 | 1.045–1.724 | 0.021 | ||||
| h6 | 0.601 | 1.824 | 1.423–2.336 | 0.001 | ||||
| h21 (1) | −0.433 | 0.649 | 0.484–0.869 | 0.004 | ||||
| h21 (2) | −0.399 | 0.712 | 0.544–0.931 | 0.013 | ||||
| h19 | 37.646 | 0.001 | 0.062 | s1 | 0.040 | 1.041 | 1.021–1.062 | 0.001 |
| s7 | 1.020 | 2.772 | 1.126–6.823 | 0.027 | ||||
| h5 * | 0.703 | 2.020 | 1.193–3.419 | 0.009 | ||||
| h6 | 0.721 | 2.057 | 1.325–3.192 | 0.001 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciucurel, C.; Iconaru, E.I. An Epidemiological Study on the Prevalence of the Clinical Features of SARS-CoV-2 Infection in Romanian People. Int. J. Environ. Res. Public Health 2020, 17, 5082. https://doi.org/10.3390/ijerph17145082
Ciucurel C, Iconaru EI. An Epidemiological Study on the Prevalence of the Clinical Features of SARS-CoV-2 Infection in Romanian People. International Journal of Environmental Research and Public Health. 2020; 17(14):5082. https://doi.org/10.3390/ijerph17145082
Chicago/Turabian StyleCiucurel, Constantin, and Elena Ioana Iconaru. 2020. "An Epidemiological Study on the Prevalence of the Clinical Features of SARS-CoV-2 Infection in Romanian People" International Journal of Environmental Research and Public Health 17, no. 14: 5082. https://doi.org/10.3390/ijerph17145082