Shock Index: A Simple and Effective Clinical Adjunct in Predicting 60-Day Mortality in Advanced Cancer Patients at the Emergency Department

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Settings and Subjects
2.3. Measurement of Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Steinhauser, K.E.; Christakis, N.A.; Clipp, E.C.; McNeilly, M.; McIntyre, L.; Tulsky, J.A. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000, 284, 2476–2482. [Google Scholar] [CrossRef] [Green Version]
- Barnato, A.E.; Chang, C.C.; Farrell, M.H.; Lave, J.R.; Roberts, M.S.; Angus, D.C. Is survival better at hospitals with higher “end-of-life” treatment intensity? Med. Care. 2010, 48, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfred, F.C.; Neal, V.D.; Norman, A.D.; William, J.F.; Lee, G.; William, A.K.; Joanne, L.; Robert, K.O.; Marilyn, B.; Anne, D.; et al. A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA 1995, 274, 1591–1598. [Google Scholar]
- den Daas, N.R.N. Estimating length of survival in end-stage cancer: A review of the literature. J. Pain Symptom Manag. 1995, 10, 548–555. [Google Scholar] [CrossRef]
- Grudzen, C.R.; Richardson, L.D.; Johnson, P.N.; Hu, M.; Wang, B.; Ortiz, J.M.; Kistler, E.A.; Chen, A.; Morrison, R.S. Emergency department-initiated palliative care in advanced cancer: A randomized clinical trial. JAMA Oncol. 2016, 2, 591–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, J.W.; Chen, K.; Boscoe, F.P.; Gesten, F.C.; Roohan, P.J.; Weeks, J.C.; Schymura, M.J.; Schrag, D. Underuse of hospice care by Medicaid-insured patients with stage IV lung cancer in New York and California. J. Clin. Oncol. 2013, 31, 2569–2579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, K.; Maeda, I.; Morita, T.; Miura, T.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Baba, M.; Sekine, R.; Yamaguchi, T.; et al. Clinical implications of C-reactive protein as a prognostic marker in advanced cancer patients in palliative care settings. J. Pain Symptom Manag. 2016, 51, 860–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okugawa, Y.; Shirai, Y.; Nodono, H.; Matsutani, F.; Itoh, M.; Hishida, A.; Morimoto, Y.; Nishikawa, R.; Yokoe, T.; Tanaka, K.; et al. Objective predictive score as a feasible biomarker for short-term survival in terminalIy ill patients with cancer. Anticancer Res. 2017, 37, 267–275. [Google Scholar] [CrossRef]
- Laird, B.J.; Kaasa, S.; McMillan, D.C.; Fallon, M.T.; Hjermstad, M.J.; Fayers, P.; Klepstad, P. Prognostic factors in patients with advanced cancer: A comparison of clinicopathological factors and the development of an inflammation-based prognostic system. Clin. Cancer Res. 2013, 19, 5456–5464. [Google Scholar] [CrossRef] [Green Version]
- Heo, S.J.; Kim, G.; Lee, C.K.; Chung, K.S.; Choi, H.J.; Sohn, J.; Lee, S. Prediction of short- and long-term survival for advanced cancer patients after ICU admission. Support. Care Cancer 2015, 23, 1647–1655. [Google Scholar] [CrossRef]
- Gwilliam, B.; Keeley, V.; Todd, C.; Gittins, M.; Roberts, C.; Kelly, L.; Barclay, S.; Stone, P.C. Development of prognosis in palliative care study (PiPS) predictor models to improve prognostication in advanced cancer: Prospective cohort study. BMJ Support. Palliat. Care 2015, 5, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Chiang, J.K.; Kuo, T.B.; Fu, C.H.; Koo, M. Predicting 7-day survival using heart rate variability in hospice patients with non-lung cancers. PLoS ONE 2013, 8, e69482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, T.; Tsunoda, J.; Inoue, S.; Chihara, S. The palliative prognostic index: A scoring system for survival prediction of terminally ill cancer patients. Support. Care Cancer 1999, 7, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Hess, K.; dos Santos, R.; Chisholm, G.; Bruera, E. A diagnostic model for impending death in cancer patients: Preliminary report. Cancer 2015, 121, 3914–3921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geraci, J.M.; Tsang, W.; Valdres, R.V.; Escalante, C.P. Progressive disease in patients with cancer presenting to an emergency room with acute symptoms predicts short-term mortality. Support. Care Cancer 2006, 14, 1038–1045. [Google Scholar] [CrossRef]
- Lee, J.S.; Kwon, O.Y.; Choi, H.S.; Hong, H.P.; Ko, Y.G. Application of the sequential organ failure assessment (SOFA) score in patients with advanced cancer who present to the ED. Am. J. Emerg. Med. 2012, 30, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Allgöwer, M.; Burri, C. “Schockindex” [“Shock index”]. Dtsch. Med. Wochenschr. 1967, 92, 1947–1950. [Google Scholar] [CrossRef]
- Toosi, M.S.; Merlino, J.D.; Leeper, K.V. Prognostic value of the shock index along with transthoracic echocardiography in risk stratification of patients with acute pulmonary embolism. Am. J. Cardiol. 2008, 101, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, P.; Kamath, A.V.; Tariq, S.M.; Ruffell, H.; Smith, A.C.; Prentice, P.; Subramanian, D.N.; Musonda, P.; Myint, P.K. Are shock index and adjusted shock index useful in predicting mortality and length of stay in community-acquired pneumonia? Eur. J. Intern. Med. 2011, 22, 282–285. [Google Scholar] [CrossRef]
- Chung, J.Y.; Hsu, C.C.; Chen, J.H.; Chen, W.L.; Lin, H.J.; Guo, H.R.; Huang, C.C. Shock index predicted mortality in geriatric patients with influenza in the emergency department. Am. J. Emerg. Med. 2019, 37, 391–394. [Google Scholar] [CrossRef]
- Pandit, V.; Rhee, P.; Hashmi, A.; Kulvatunyou, N.; Tang, A.; Khalil, M.; O’Keeffe, T.; Green, D.; Friese, R.S.; Joseph, B. Shock index predicts mortality in geriatric trauma patients: An analysis of the National Trauma Data Bank. J. Trauma Acute Care Surg. 2014, 76, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Yang, Y.; Zhu, J.; Liang, Y.; Tan, H.; Yu, L.; Gao, X.; Li, J. Usefulness of the admission shock index for predicting short-term outcomes in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2014, 114, 1315–1321. [Google Scholar] [CrossRef]
- Talmor, D.; Jones, A.E.; Rubinson, L.; Howell, M.D.; Shapiro, N.I. Simple triage scoring system predicting death and the need for critical care resources for use during epidemics. Crit. Care Med. 2007, 35, 1251–1256. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Sheng, S.; Xian, Y.; Matsouaka, R.A.; Reeves, M.J.; Saver, J.L.; Bhatt, D.L.; Fonarow, G.C.; Schwamm, L.H.; Smith, E.E. Shock index predicts patient-related clinical outcomes in stroke. J. Am. Heart. Assoc. 2018, 7, e007581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, K.; Yokoi, H.; Tsuneto, S. Shock index and decreased devel of consciousness as terminal cancer patients’ survival time predictors: A retrospective cohort study. J. Pain Symptom Manag. 2016, 51, 220–231.e2. [Google Scholar] [CrossRef] [Green Version]
- Llobera, J.; Esteva, M.; Rifà, J.; Benito, E.; Terrasa, J.; Rojas, C.; Pons, O.; Catalán, G.; Avellà, A. Terminal cancer—Duration and prediction of survival time. Eur. J. Cancer 2000, 36, 2036–2043. [Google Scholar] [CrossRef]
- Steensma, D.P.; Loprinzi, C.L. The art and science of prognosis in patients with advanced cancer. Eur. J. Cancer 2000, 36, 2025–2027. [Google Scholar] [CrossRef]
- Kim, S.H.; Shin, D.W.; Kim, S.Y.; Yang, H.K.; Nam, E.; Jho, H.J.; Ahn, E.; Cho, B.L.; Park, K.; Park, J.H. Terminal versus advanced cancer: Do the general population and health care professionals share a common language? Cancer Res. Treat. 2016, 48, 759–767. [Google Scholar] [CrossRef] [Green Version]
- Elsayem, A.F.; Bruera, E.; Valentine, A.D.; Warneke, C.L.; Yeung, S.C.; Page, V.D.; Wood, G.L.; Silvestre, J.; Holmes, H.M.; Brock, P.A.; et al. Delirium frequency among advanced cancer patients presenting to an emergency department: A prospective, randomized, observational study. Cancer 2016, 122, 2918–2924. [Google Scholar] [CrossRef]
- Viganò, A.; Dorgan, M.; Bruera, E.; Suarez-Almazor, M.E. The relative accuracy of the clinical estimation of the duration of life for patients with end of life cancer. Cancer 1999, 86, 170–176. [Google Scholar] [CrossRef]
- Weeks, J.C.; Cook, E.F.; O’Day, S.J.; Peterson, L.M.; Wenger, N.; Reding, D.; Harrell, F.E.; Kussin, P.; Dawson, N.V.; Connors, A.F.; et al. Relationship between cancer patients’ predictions of prognosis and their treatment preferences. JAMA 1998, 279, 1709–1714. [Google Scholar] [CrossRef] [PubMed]
- Rady, M.Y.; Nightingale, P.; Little, R.A.; Edwards, J.D. Shock index: A re-evaluation in acute circulatory failure. Resuscitation 1992, 23, 227–234. [Google Scholar] [CrossRef]
- Tisdale, M.J. Cachexia in cancer patients. Nat. Rev. Cancer 2002, 2, 862–871. [Google Scholar] [CrossRef]
- Belloum, Y.; Rannou-Bekono, F.; Favier, F.B. Cancer-induced cardiac cachexia: Pathogenesis and impact of physical activity (Review). Oncol. Rep. 2017, 37, 2543–2552. [Google Scholar] [CrossRef] [PubMed]
- Barkhudaryan, A.; Scherbakov, N.; Springer, J.; Doehner, W. Cardiac muscle wasting in individuals with cancer cachexia. ESC Heart Fail. 2017, 4, 458–467. [Google Scholar] [CrossRef]
- Springer, J.; Tschirner, A.; Haghikia, A.; von Haehling, S.; Lal, H.; Grzesiak, A.; Kaschina, E.; Palus, S.; Pötsch, M.; von Websky, K.; et al. Prevention of liver cancer cachexia-induced cardiac wasting and heart failure. Eur. Heart J. 2014, 35, 932–941. [Google Scholar] [CrossRef]
- Cramer, L.; Hildebrandt, B.; Kung, T.; Wichmann, K.; Springer, J.; Doehner, W.; Sandek, A.; Valentova, M.; Stojakovic, T.; Scharnagl, H.; et al. Cardiovascular function and predictors of exercise capacity in patients with colorectal cancer. J. Am. Coll. Cardiol. 2014, 64, 1310–1319. [Google Scholar] [CrossRef] [Green Version]
- Pavo, N.; Raderer, M.; Hülsmann, M.; Neuhold, S.; Adlbrecht, C.; Strunk, G.; Goliasch, G.; Gisslinger, H.; Steger, G.G.; Hejna, M.; et al. Cardiovascular biomarkers in patients with cancer and their association with all-cause mortality. Heart 2015, 101, 1874–1880. [Google Scholar] [CrossRef]
- Lamont, E.B.; Siegler, M. Paradoxes in cancer patients’ advance care planning. J. Palliat. Med. 2000, 3, 27–35. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Patients | p-Value | ||
|---|---|---|---|---|
| Total | Survivors | Nonsurvivors | ||
| No. | 305 | 117 | 188 | |
| Age | 63.50 ± 13.29 | 65.10 ± 12.42 | 62.51 ± 13.74 | 0.0971 |
| Male | 195 (63.93) | 71 (60.68) | 124 (65.96) | 0.4179 |
| Primary cancer | ||||
| Thyroid cancer | 2 (0.66) | 2 (1.71) | 0.1464 | |
| Hypopharyngeal cancer | 13 (4.26) | 8 (6.84) | 5 (2.66) | 0.0885 |
| Lung cancer | 86 (28.20) | 34 (29.06) | 52 (27.66) | 0.8939 |
| Oropharyngeal cancer | 10 (3.28) | 3 (2.56) | 7 (3.72) | 0.7464 |
| Nasopharyngeal cancer | 8 (2.62) | 5 (4.27) | 3 (1.60) | 0.2675 |
| Oesophageal cancer | 17 (5.57) | 5 (4.27) | 12 (6.38) | 0.6001 |
| Gastric cancer | 29 (9.51) | 9 (7.69) | 20 (10.64) | 0.5143 |
| Colon cancer | 43 (14.10) | 17 (14.53) | 26 (13.83) | 0.9987 |
| Rectal cancer | 16 (5.25) | 5 (4.27) | 11 (5.85) | 0.7363 |
| Bladder cancer | 4 (1.31) | 1 (0.85) | 3 (1.60) | 0.9700 |
| Renal cancer | 6 (1.97) | 2 (1.71) | 4 (2.13) | 0.7981 |
| Prostate cancer | 7 (2.30) | 3 (2.56) | 4 (2.13) | 0.8045 |
| Cervical cancer | 4 (1.31) | 1 (0.85) | 3 (1.60) | 0.9716 |
| Uterine cancer | 3 (0.98) | 3 (1.60) | 0.2883 | |
| Ovarian cancer | 3 (0.98) | 1 (0.85) | 2 (1.06) | 0.8500 |
| Brain cancer | 2 (0.66) | 2 (1.71) | 0.1464 | |
| Pancreatic cancer | 12 (3.93) | 4 (3.42) | 8 (4.26) | 0.9501 |
| Hepatic cell cancer | 21 (6.89) | 7 (5.98) | 14 (7.45) | 0.7961 |
| Cholangial cancer | 8 (2.62) | 4 (3.42) | 4 (2.13) | 0.4883 |
| Breast cancer | 17 (5.57) | 7 (5.98) | 10 (5.32) | 0.8059 |
| Soft tissue cancer | 6 (1.97) | 6 (3.19) | 0.0857 | |
| Previous treatment | ||||
| Chemotherapy | 255 (83.61) | 98 (83.76) | 157 (83.51) | 0.9543 |
| Radiotherapy | 157 (51.48) | 57 (48.72) | 100 (53.19) | 0.5207 |
| Target therapy | 90 (29.51) | 37 (31.62) | 53 (28.19) | 0.6100 |
| Surgical treatment | 158 (51.80) | 61 (52.14) | 97 (51.60) | 0.9267 |
| Comorbidities | ||||
| Diabetes mellitus | 69 (22.62) | 25 (21.37) | 44 (23.40) | 0.7851 |
| Hypertension | 97 (31.80) | 44 (37.61) | 53 (28.19) | 0.1117 |
| Cerebrovascular accident | 9 (2.95) | 4 (3.42) | 5 (2.66) | 0.9736 |
| Heart failure | 5 (1.64) | 1 (0.85) | 4 (2.13) | 0.6525 |
| Coronary artery disease | 14 (4.59) | 4 (3.42) | 10 (5.32) | 0.6243 |
| Chronic obstructive pulmonary disease | 16 (5.25) | 3 (2.56) | 13 (6.91) | 0.1636 |
| End stage renal disease | 6 (1.97) | 2 (1.71) | 4 (2.13) | 0.7981 |
| Liver cirrhosis | 25 (8.20) | 7 (5.98) | 18 (9.57) | 0.3696 |
| Variable | Patient | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Survivors | Nonsurvivors | p-Value | Univariate OR (95% CI) | Multiple OR ** (95% CI) | |||
| No. | 305 | 117 | 188 | |||||
| Body temperature (℃) * | 36.77 ± 1.32 | 37.11 ± 1.33 | 36.6 ± 1.27 | 0.0006 | 0.73 | (0.61, 0.87) | ||
| Pulse rate (/min) * | 110.31 ± 21.17 | 102.40 ± 19.55 | 115.30 ± 20.67 | <0.0001 | 1.03 | (1.02, 1.05) | ||
| Respiratory rate (/min) * | 22.53 ± 5.49 | 21.10 ± 4.30 | 23.41 ± 5.96 | 0.0006 | 1.1 | (1.04, 1.16) | ||
| Systolic blood pressure (mmHg) * | 104.82 ± 20.91 | 114.50 ± 22.01 | 98.81 ± 17.77 | <0.0001 | 0.96 | (0.95, 0.97) | ||
| Mean arterial pressure (mmHg) * | 77.57 ± 16.13 | 83.61 ± 16.31 | 73.82 ± 14.87 | <0.0001 | 0.96 | (0.95, 0.98) | ||
| Shock index * | 1.11 ± 0.35 | 0.92 ± 0.27 | 1.21 ± 0.35 | <0.0001 | 1.37 | (1.24, 1.51) | 1.39 | (1.24, 1.55) |
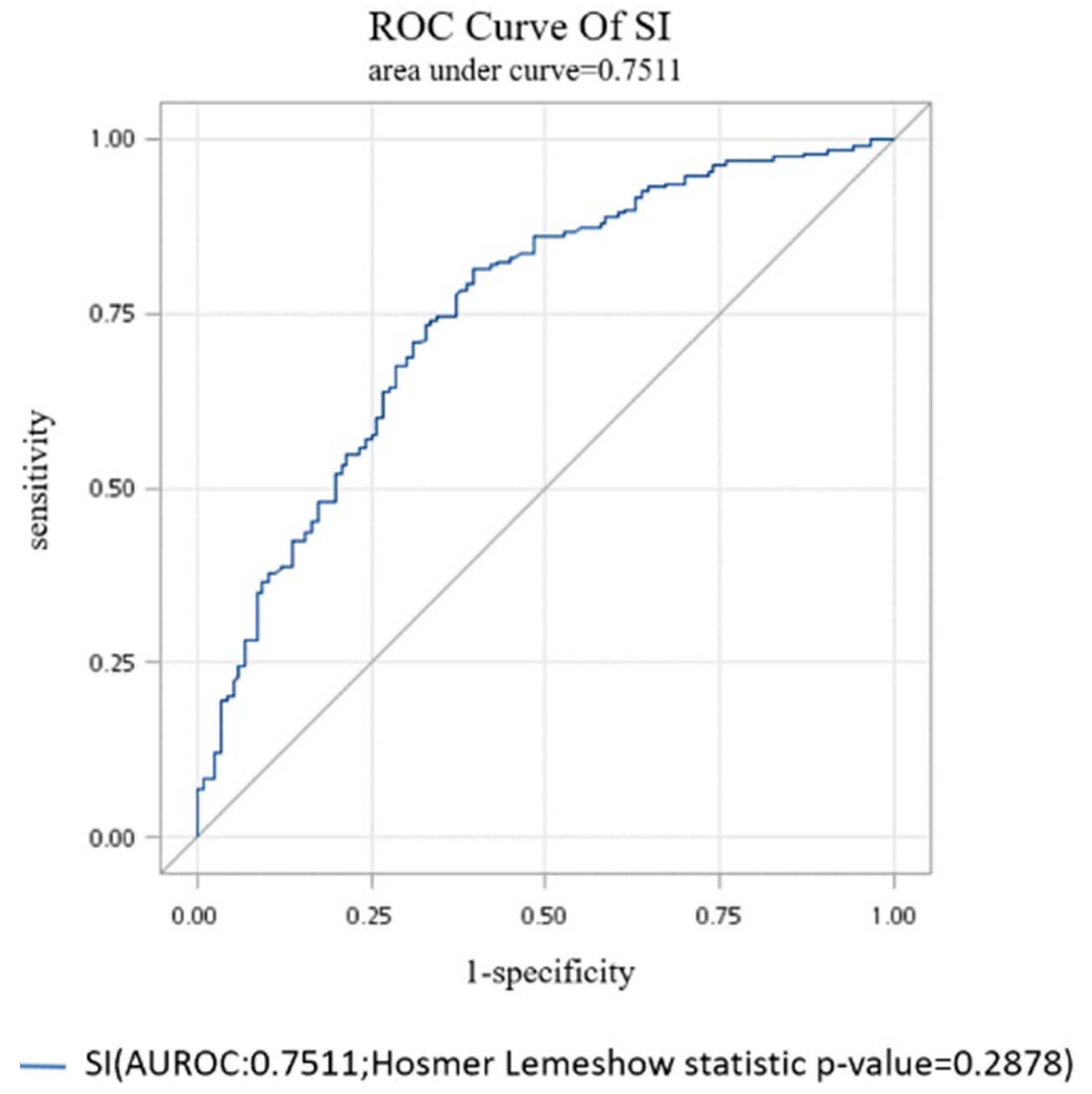
| Optimal Cut-Off | Accuracy Rate | Sen | Sp | PPV | NPV | False +ve | False −ve |
|---|---|---|---|---|---|---|---|
| 0.94 | 73.11% | 81.38% | 59.83% | 76.50% | 66.67% | 15.26% | 11.54% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, T.-H.; Sie, Y.-D.; Hsu, K.-H.; Goh, Z.N.L.; Chien, C.-Y.; Chen, H.-Y.; Ng, C.-J.; Li, C.-H.; Seak, J.C.-Y.; Seak, C.-K.; et al. Shock Index: A Simple and Effective Clinical Adjunct in Predicting 60-Day Mortality in Advanced Cancer Patients at the Emergency Department. Int. J. Environ. Res. Public Health 2020, 17, 4904. https://doi.org/10.3390/ijerph17134904
Cheng T-H, Sie Y-D, Hsu K-H, Goh ZNL, Chien C-Y, Chen H-Y, Ng C-J, Li C-H, Seak JC-Y, Seak C-K, et al. Shock Index: A Simple and Effective Clinical Adjunct in Predicting 60-Day Mortality in Advanced Cancer Patients at the Emergency Department. International Journal of Environmental Research and Public Health. 2020; 17(13):4904. https://doi.org/10.3390/ijerph17134904
Chicago/Turabian StyleCheng, Tzu-Heng, Yi-Da Sie, Kuang-Hung Hsu, Zhong Ning Leonard Goh, Cheng-Yu Chien, Hsien-Yi Chen, Chip-Jin Ng, Chih-Huang Li, Joanna Chen-Yeen Seak, Chen-Ken Seak, and et al. 2020. "Shock Index: A Simple and Effective Clinical Adjunct in Predicting 60-Day Mortality in Advanced Cancer Patients at the Emergency Department" International Journal of Environmental Research and Public Health 17, no. 13: 4904. https://doi.org/10.3390/ijerph17134904