The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. General Demographic Data
3.2. Reasons for Continuing or Suspending Clinical Work during the COVID-19 Outbreak
3.3. Factors Influencing Dentists’ Decisions and Professional Attitudes
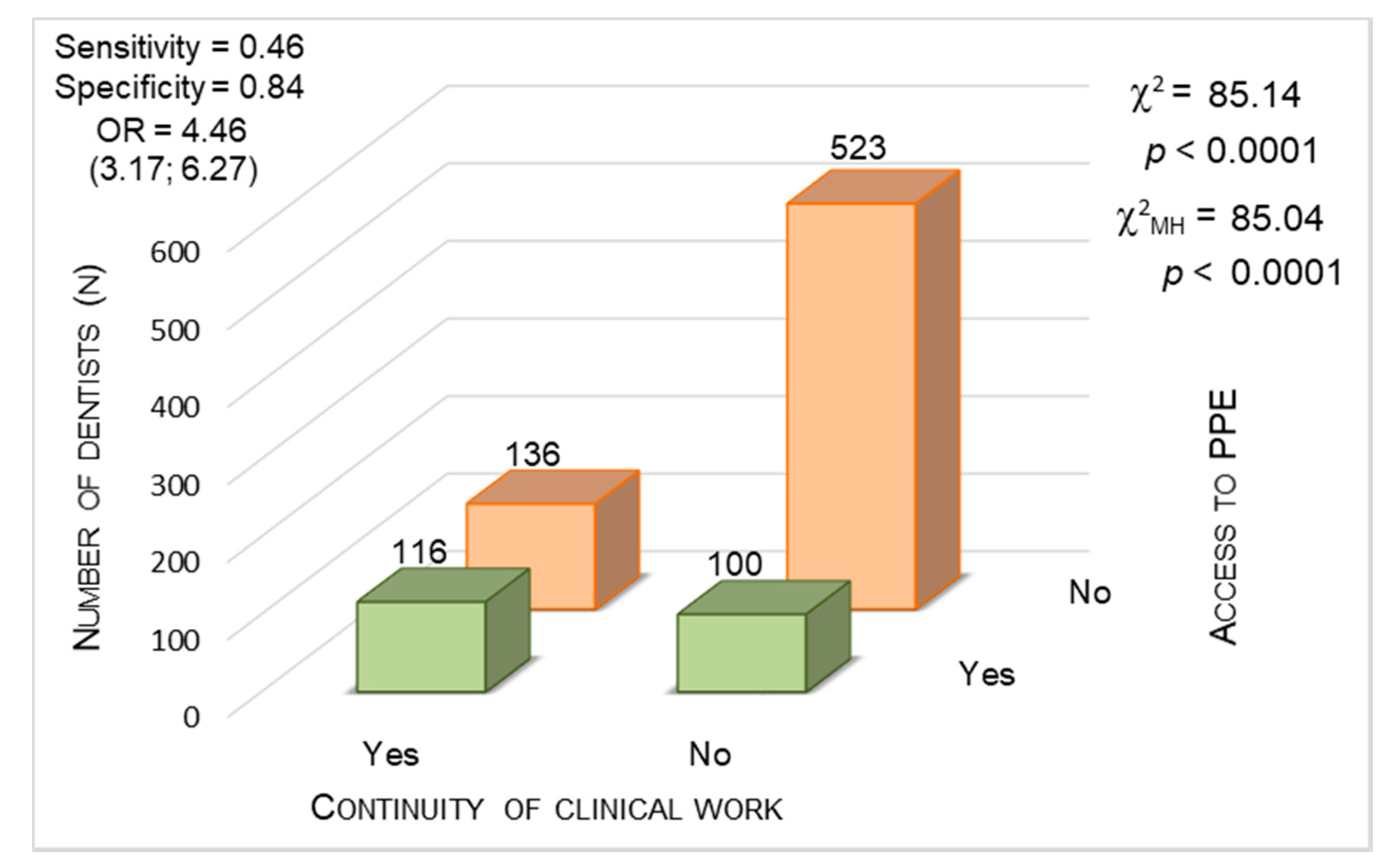
3.3.1. Access to Adequate PPE
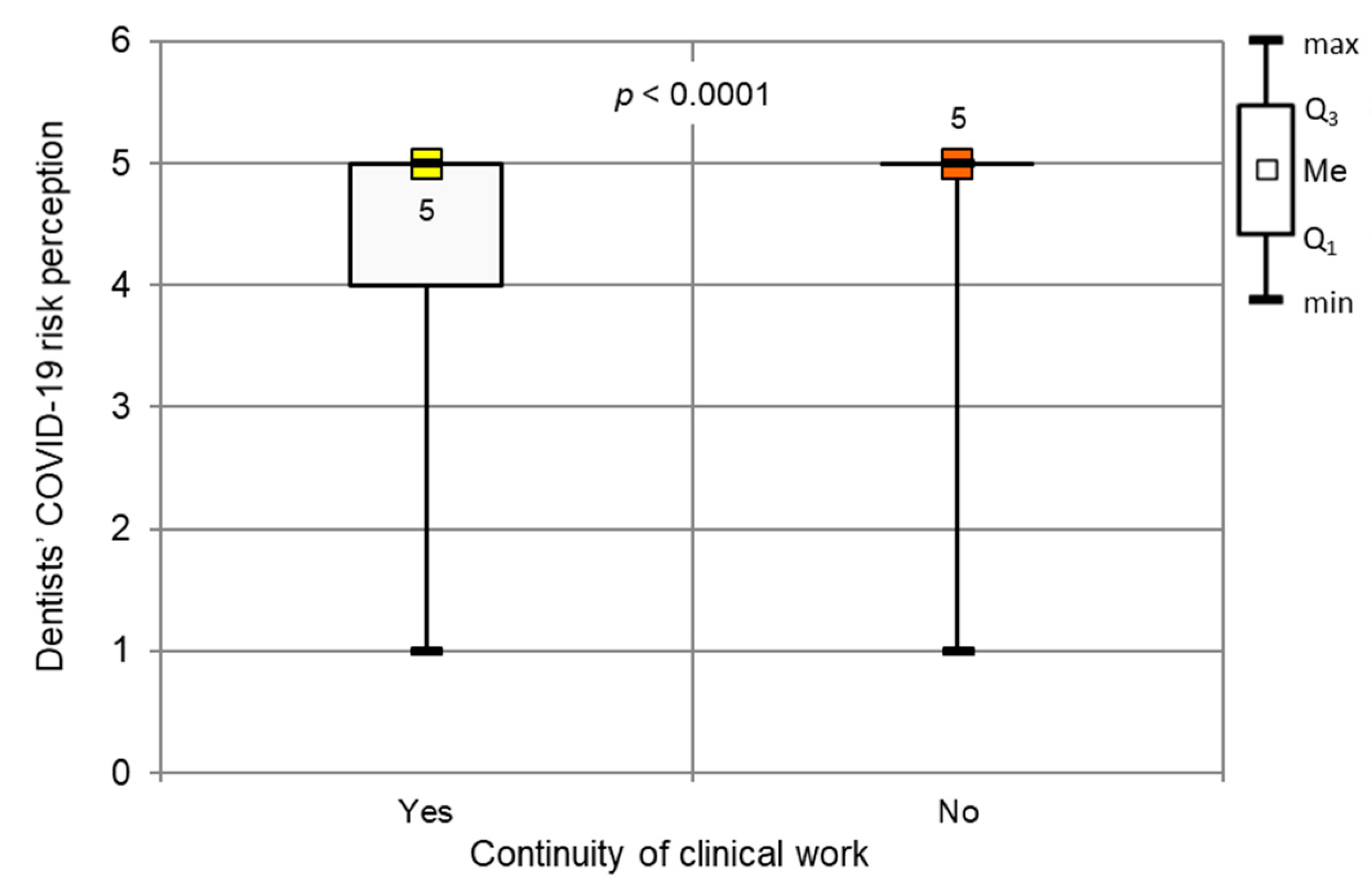
3.3.2. Subjective Risk Assessment of COVID-19 Contraction
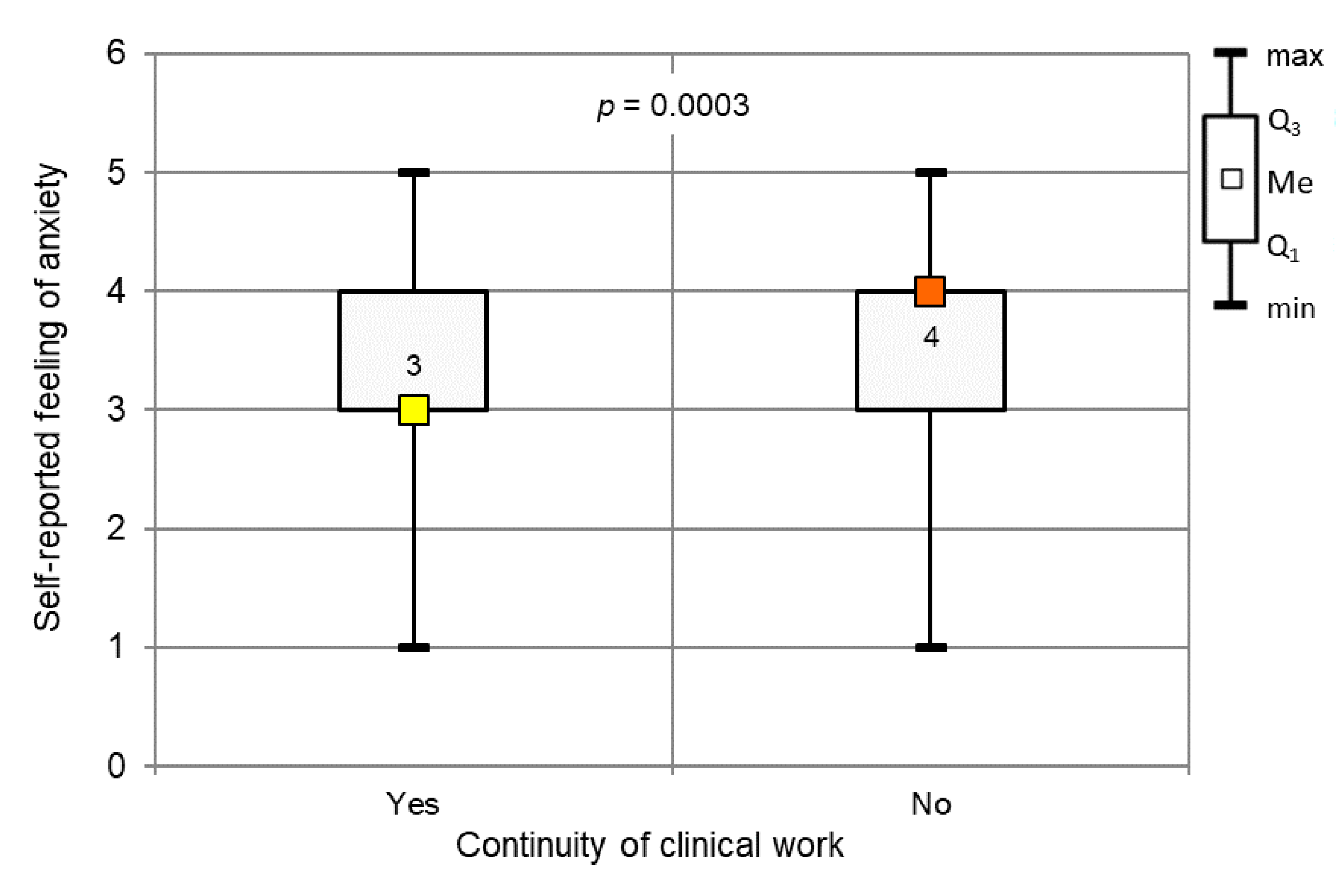
3.3.3. Self-Reported Anxiety Level
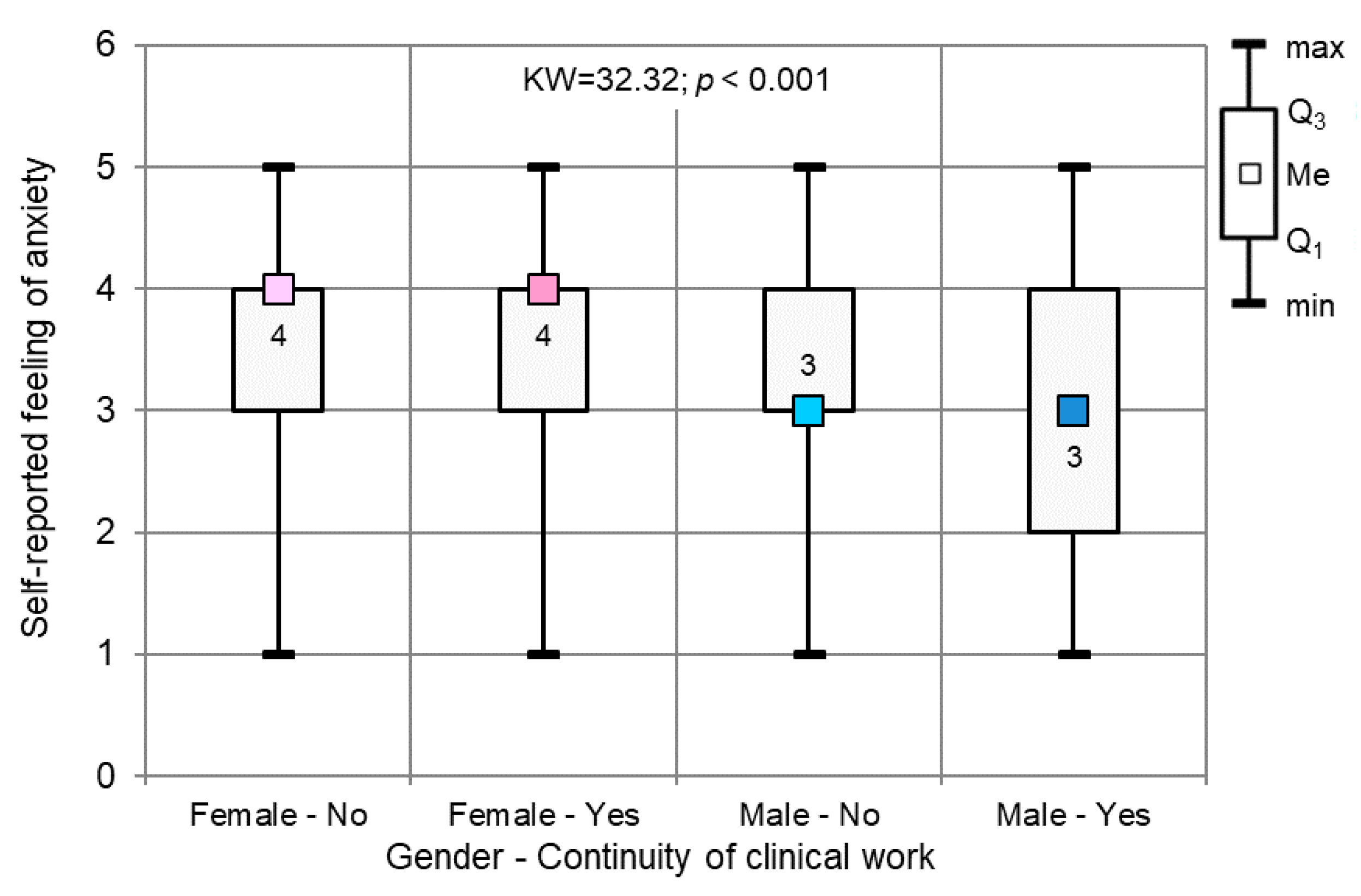
3.3.4. Gender
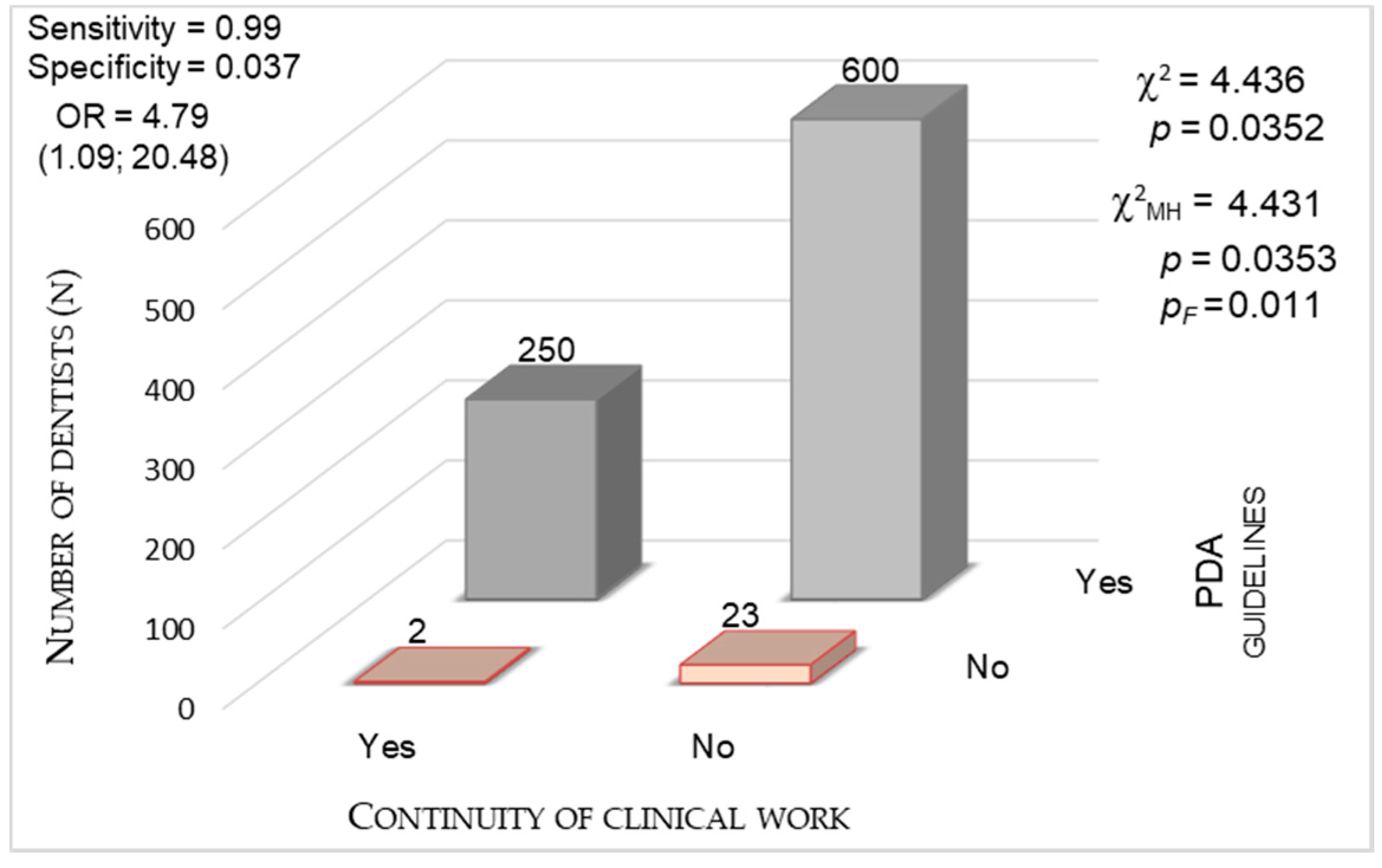
3.3.5. The Impact of National Guidance (PDA and PMH Guidelines)
3.4. The Decrease in the Number of Admitted Patients
3.5. Other Investigated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet Lond. Engl. 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 14 May 2020).
- Poland: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/euro/country/pl (accessed on 9 June 2020).
- Ministerstwo Żongluje Danymi o Liczbie Zakażonych Pielęgniarek-Portal Pielęgniarek i Położnych. Available online: https://www.pielegniarki.info.pl/article/view/id/10941 (accessed on 10 June 2020).
- Dar Odeh, N.; Babkair, H.; Abu-Hammad, S.; Borzangy, S.; Abu-Hammad, A.; Abu-Hammad, O. COVID-19: Present and Future Challenges for Dental Practice. Int. J. Environ. Res. Public. Health 2020, 17, 3151. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Y.F.; Rasubala, L.; Malmstrom, H.; Eliav, E. Dental Care and Oral Health under the Clouds of COVID-19. JDR Clin. Transl. Res. 2020, 5, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Cao, J. Airborne Transmission of SARS-CoV-2: The World Should Face the Reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- Severe Acute Respiratory Syndrome and Dentistry|Elsevier Enhanced Reader. Available online: https://reader.elsevier.com/reader/sd/pii/S0002817714625423?token=1255DC69A5E5FA47E7AFE992FE704D462751E84B6DCC19C0C492DD54E4BA33F90A37F2FC5E13864D8742865D7F0328A8 (accessed on 13 May 2020). [CrossRef] [Green Version]
- Duruk, G.; Gümüşboğa, Z.Ş.; Çolak, C. Investigation of Turkish Dentists’ Clinical Attitudes and Behaviors towards the COVID-19 Pandemic: A Survey Study. Braz. Oral Res. 2020, 34, e054. [Google Scholar] [CrossRef]
- Pinkas, J.; Jankowski, M.; Szumowski, Ł.; Lusawa, A.; Zgliczyński, W.S.; Raciborski, F.; Wierzba, W.; Gujski, M. Public Health Interventions to Mitigate Early Spread of SARS-CoV-2 in Poland. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924730. [Google Scholar] [CrossRef]
- COVID-19 a Praca Lekarza Dentysty: Wytyczne PTS Uaktualnione. Polskie Towarzystwo Stomatologiczne. 2020. Available online: https://pts.net.pl/covid-19-a-praca-lekarza-dentysty-wytyczne-pts-uaktualnione/ (accessed on 9 June 2020).
- NIL-Wytyczne MZ-Stomatologia. Available online: https://nil.org.pl/dla-lekarzy/dla-stomatologow/4558-wytyczne-mz-stomatologia (accessed on 5 June 2020).
- Baghizadeh Fini, M. What Dentists Need to Know about COVID-19. Oral Oncol. 2020, 105, 104741. [Google Scholar] [CrossRef]
- Interpelacja nr 1160-Tekst. Available online: http://sejm.gov.pl/Sejm9.nsf/InterpelacjaTresc.xsp?key=BKMBD9 (accessed on 10 June 2020).
- GUS. Ambulatoryjna Opieka Zdrowotna w 2018 Roku. Available online: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/ambulatoryjna-opieka-zdrowotna-w-2018-roku,13,3.html (accessed on 10 June 2020).
- Plany Finansowe NFZ-Ministerstwo Zdrowia-Portal Gov.pl. Available online: https://www.gov.pl/web/zdrowie/plany-finansowe-nfz (accessed on 10 June 2020).
- Interpelacja nr 5167-Tekst. Available online: http://www.sejm.gov.pl/Sejm8.nsf/InterpelacjaTresc.xsp?key=2B0F68F7&view=5 (accessed on 10 June 2020).
- Italy: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/euro/country/it (accessed on 10 June 2020).
- Spain: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/euro/country/es (accessed on 10 June 2020).
- NIL-Informacje Statystyczne. Available online: https://nil.org.pl/rejestry/centralny-rejestr-lekarzy/informacje-statystyczne (accessed on 18 May 2020).
- Ministerstwo Zdrowia na Twitterze: W Ciągu Doby Wykonano Ponad 4,7 tys. Testów na #Koronawirus. Available online: https://t.co/KmCYj8FQqM” (accessed on 13 May 2020).
- Ministerstwo Zdrowia na Twitterze: „W Ciągu Doby Wykonano Ponad 12,5 tys. Testów na #Koronawirus. Available online: https://t.co/4TLmdcCCCe” (accessed on 13 May 2020).
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public. Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Toit, J.D.; Jain, S.; Montalli, V.; Govender, U. Dental Students’ Motivations for Their Career Choice: An International Investigative Report. J. Dent. Educ. 2014, 78, 605–613. [Google Scholar] [CrossRef]
- Lee, S.-H.; Juang, Y.-Y.; Su, Y.-J.; Lee, H.-L.; Lin, Y.-H.; Chao, C.-C. Facing SARS: Psychological Impacts on SARS Team Nurses and Psychiatric Services in a Taiwan General Hospital. Gen. Hosp. Psychiatry 2005, 27, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, E.E.; Temsah, M.H.; Aleyadhy, A.A.; Alrabiaa, A.A.; Alhboob, A.A.; Jamal, A.A.; Binsaeed, A.A. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Outbreak Perceptions of Risk and Stress Evaluation in Nurses. J. Infect. Dev. Ctries. 2016, 10, 845–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The Immediate Psychological and Occupational Impact of the 2003 SARS Outbreak in a Teaching Hospital. CMAJ Can. Med. Assoc. J. J. Assoc. Medicale Can. 2003, 168, 1245–1251. [Google Scholar]
- Wspieramy Akcję #NiePanikuję #LeczęOdpowiedzialnie. Polskie Towarzystwo Stomatologiczne. 2020. Available online: https://pts.net.pl/niepanikuje-leczeodpowiedzialnie/ (accessed on 9 June 2020).
- Dla Pacjentów i Lekarzy: Mapa Pracujących Gabinetów Stomatologicznych. Polskie Towarzystwo Stomatologiczne. 2020. Available online: https://pts.net.pl/dla-pacjentow-i-lekarzy-mapa-pracujacych-gabinetow-stomatologicznych/ (accessed on 9 June 2020).
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public. Health 2020, 17. [Google Scholar] [CrossRef]
- Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. Available online: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 13 May 2020).
- Binkley, C.E.; Kemp, D.S. Ethical Rationing of Personal Protective Equipment to Minimize Moral Residue During the COVID-19 Pandemic. J. Am. Coll. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Artenstein, A.W. In Pursuit of PPE. N. Engl. J. Med. 2020, 382, e46. [Google Scholar] [CrossRef]
- Covid-19: Third of surgeons do not have adequate PPE, royal college warns|The BMJ. Available online: https://www.bmj.com/content/369/bmj.m1492.long (accessed on 13 May 2020).
- O’Sullivan, E.D. PPE Guidance for Covid-19: Be Honest about Resource Shortages. BMJ 2020, 369. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package. Int. J. Environ. Res. Public. Health 2020, 17. [Google Scholar] [CrossRef]
- Dargaville, T.; Spann, K.; Celina, M. Opinion to Address a Potential Personal Protective Equipment Shortage in the Global Community during the COVID-19 Outbreak. Polym. Degrad. Stab. 2020. [Google Scholar] [CrossRef]
- Cagetti, M.G.; Cairoli, J.L.; Senna, A.; Campus, G. COVID-19 Outbreak in North Italy: An Overview on Dentistry. A Questionnaire Survey. Int. J. Environ. Res. Public. Health 2020, 17, 3835. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- De Stefani, A.; Bruno, G.; Mutinelli, S.; Gracco, A. COVID-19 Outbreak Perception in Italian Dentists. Int. J. Environ. Res. Public. Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; AlShurman, B.A. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study Among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Goulia, P.; Mantas, C.; Dimitroula, D.; Mantis, D.; Hyphantis, T. General Hospital Staff Worries, Perceived Sufficiency of Information and Associated Psychological Distress during the A/H1N1 Influenza Pandemic. BMC Infect. Dis. 2010, 10, 322. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious Traumatization in the General Public, Members, and Non-Members of Medical Teams Aiding in COVID-19 Control. Brain. Behav. Immun. 2020. [Google Scholar] [CrossRef]
- Choy, H.; Wong, M.C. Occupational Stress and Burnout among Hong Kong Dentists. Hong Kong Med. J. 2017. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Zhou, Y.; Liu, X.; Tan, J. The Impact of the COVID-19 Epidemic on the Utilization of Emergency Dental Services. J. Dent. Sci. 2020. [Google Scholar] [CrossRef]
- Dominiak, M.; Różyło-Kalinowska, I.; Gedrange, T.; Konopka, T.; Hadzik, J.; Bednarz, W.; Matys, J.; Lella, A.; Rayad, S.; Maksymowicz, R.; et al. COVID-19 and Professional Dental Practice. The Polish Dental Association Working Group Recommendations for Procedures in Dental Office during an Increased Epidemiological Risk. J. Stomatol. 2020, 73, 1–10. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission Routes of 2019-NCoV and Controls in Dental Practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Barabari, P.; Moharamzadeh, K. Novel Coronavirus (COVID-19) and Dentistry–A Comprehensive Review of Literature. Dent. J. 2020, 8, 53. [Google Scholar] [CrossRef]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) in Dentistry. Management of Biological Risk in Dental Practice. Int. J. Environ. Res. Public. Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- NIL-Petycja w Sprawie Zasad Finansowania Świadczeń Stomatologicznych. Available online: https://nil.org.pl/dla-lekarzy/dla-stomatologow/kontrakty/4803-petycja-w-sprawie-zasad-finansowania-swiadczen-stomatologicznych (accessed on 10 June 2020).
- NIL-Stanowisko Opiniujące Projekt Zarządzenia NFZ. Available online: https://nil.org.pl/dla-lekarzy/dla-stomatologow/kontrakty/4877-stanowisko-opiniujace-projekt-zarzadzenia-nfz (accessed on 10 June 2020).
- Molga, T. Koronawirus w Polsce. Niemiłe Zaskoczenie u Dentystów. “Doliczają do Wizyty 100 zł”. Available online: https://wiadomosci.wp.pl/koronawirus-w-polsce-niemile-zaskoczenie-u-dentystow-doliczaja-do-wizyty-100-zl-6502698955651201a (accessed on 10 June 2020).
- Ferneini, E.M. The Financial Impact of COVID-19 on Our Practice. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- ZWIĄZEK PRACODAWCÓW STOMATOLOGII|Rejestr.io. Available online: https://rejestr.io/krs/838437/zwiazek-pracodawcow-stomatologii (accessed on 10 June 2020).
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, H.; Syed, S.; Rezaie, S. The Twitter Pandemic: The Critical Role of Twitter in the Dissemination of Medical Information and Misinformation during the COVID-19 Pandemic. CJEM 2020, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Variable | Dentists, n (%) |
|---|---|---|
| Gender | Female Male | 722 (82.5%) 153 (17.5%) |
| Age | 24–30 31–40 41–55 ≥56 | 255 (29.1%) 293 (33.5%) 223 (25.5%) 104 (11.9%) |
| Years of clinical experience | ≤10 11–20 21–30 ≥31 | 419 (47.9%) 209 (23.9%) 169 (19.3%) 78 (8.9%) |
| Marital Status | Single Married Widowed Divorced | 216 (24.7%) 558 (63.8%) 39 (4.5%) 62 (7.1%) |
| Number of children | 0 1 2 ≥3 | 302 (34.5%) 239 (27.3%) 271 (31.0%) 63 (7.2%) |
| Place of residence | Urban areas Rural areas | 623 (71.2%) 252 (28.8%) |
| Belonging to the risk group for coronavirus infection due to comorbidities (diabetes, cardiovascular diseases, respiratory diseases, autoimmune diseases, oncological diseases) | Yes No | 252 (28.8%) 623 (71.2%) |
| The Reasons Why Dentists Decided to Continue Their Clinical Work During The COVID-19 Pandemic | Number Of Dentists Who Chose The Answer (N)/(%) From The Group of 252 Dentists Who Continued Clinical Practice |
|---|---|
| I do not want to leave my regular patients without help. | 130 (51.6%) |
| I do not want to leave patients suffering from pain unattended. | 151 (59.9%) |
| My employer instructed me to continue my clinical practice. | 39 (15.5%) |
| I work in a sufficiently equipped dental office. | 82 (30.1%) |
| My financial situation forces me to continue my clinical practice irrespective of the COVID-19 pandemic. | 78 (31 %) |
| Other. | 23 (9.1%) |
| The Reasons Why Dentists Decided Not To Continue Their Clinical Work During the COVID-19 Pandemic | Number Of Dentists Who Chose the Answer (n)/% From of the Group of 623 Dentists Who Did Not Continue Clinical Practice |
| I fear for my health and life. | 319 (51.2%) |
| I fear for the health and life of the members of my family. | 359 (57.6%) |
| I work in an insufficiently equipped dental office. | 395 (63.4%) |
| I believe that during the COVID-19 pandemic, patients should only be admitted to dental clinics designated by the Polish Ministry of Health. | 333 (53.5%) |
| My financial situation allows me to suspend my clinical work until the number of COVID-19 cases starts to decline. | 145 (23.3%) |
| Patients cancelled their appointments because they are afraid of contracting COVID-19 in the dental office. | 230 (36.9%) |
| The dental office where I am employed is closed. | 219 (35.5%) |
| Other. | 59 (9.5%) |
| Crucial Needs in Dental Practices During the COVID-19 Outbreak | Number of Dentists Who Chose The Answer (n)/% from the Group of 569 Dentists Who Answered the Question |
|---|---|
| Personal protective equipment: filtering face piece (FPP3, FPP2) respirators, fluid-resistant surgical masks, airtight googles, full face shields, scrub caps, fluid-resistant gowns, fluid-resistant aprons, shoe covers | 563 (98.9%) |
| Disinfectants (skin, surfaces) | 92 (16.16%) |
| Equipment (UV lamps, vaporized hydrogen peroxide fumigation systems, non-thermal plasm disinfection devices, ozone generators) | 72 (12.65%) |
| Adapted dental offices (separate rooms for doffing and donning of PPE, efficient ventilation systems) | 63 (11.07%) |
| Procedures (no update on disinfection and work safety protocols, lack of goodwill from management to adjust the dental office to the new procedures) | 53 (9.31%) |
| Conover Post-Hoc Test | ||||||
|---|---|---|---|---|---|---|
| Compared subgroups | Female–No | Female–No | Female–No | Female–Yes | Female–Yes | Male–No |
| Female–Yes | Male–No | Male–Yes | Male–No | Male–Yes | Male–Yes | |
| p | 0.0723 | 0.0361 | 0.0064 | 0.1709 | 0.0165 | 0.0460 |
| Variable | Statistical characteristic | Continuity of Clinical Work During the COVID-19 Outbreak in Poland | Mann–Whitney Test | |
|---|---|---|---|---|
| Yes | No | |||
| Age | Mean | 39.5 | 39 | p = 0.283 |
| SD | 10.9 | 11.1 | ||
| Min | 24 | 24 | ||
| Q1 | 29 | 30 | ||
| Median | 37 | 36 | ||
| Q3 | 48.3 | 47 | ||
| Max | 72 | 75 | ||
| Years of clinical experience | Mean | 14.4 | 14 | p = 0.324 |
| SD | 11.1 | 11.1 | ||
| Min | 0 | 0 | ||
| Q1 | 4 | 5 | ||
| Median | 12 | 11 | ||
| Q3 | 24 | 23 | ||
| Max | 52 | 50 | ||
| Variable | Category | Continuity of Clinical Work During the COVID-19 Outbreak in Poland | Chi-Square Test | |
|---|---|---|---|---|
| Yes | No | |||
| Marital status | Married | 159 93 | 399 224 | Χ2 = 0.035 p = 0.852 |
| Single/widowed/ divorced | ||||
| Having children | Yes | 169 | 404 | Χ2 = 0.298 p = 0.585 |
| No | 83 | 219 | ||
| Place of residence | Urban areas | 213 | 537 | Χ 2 = 0.285 p = 0.594 |
| Rural areas | 39 | 86 | ||
| Belonging to the risk group for coronavirus infection due to comorbidities | Yes No | 55 197 | 167 456 | Χ2 = 2.095 p = 0.148 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. https://doi.org/10.3390/ijerph17134703
Tysiąc-Miśta M, Dziedzic A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2020; 17(13):4703. https://doi.org/10.3390/ijerph17134703
Chicago/Turabian StyleTysiąc-Miśta, Monika, and Arkadiusz Dziedzic. 2020. "The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 17, no. 13: 4703. https://doi.org/10.3390/ijerph17134703