Mutation in ROBO3 Gene in Patients with Horizontal Gaze Palsy with Progressive Scoliosis Syndrome: A Systematic Review

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
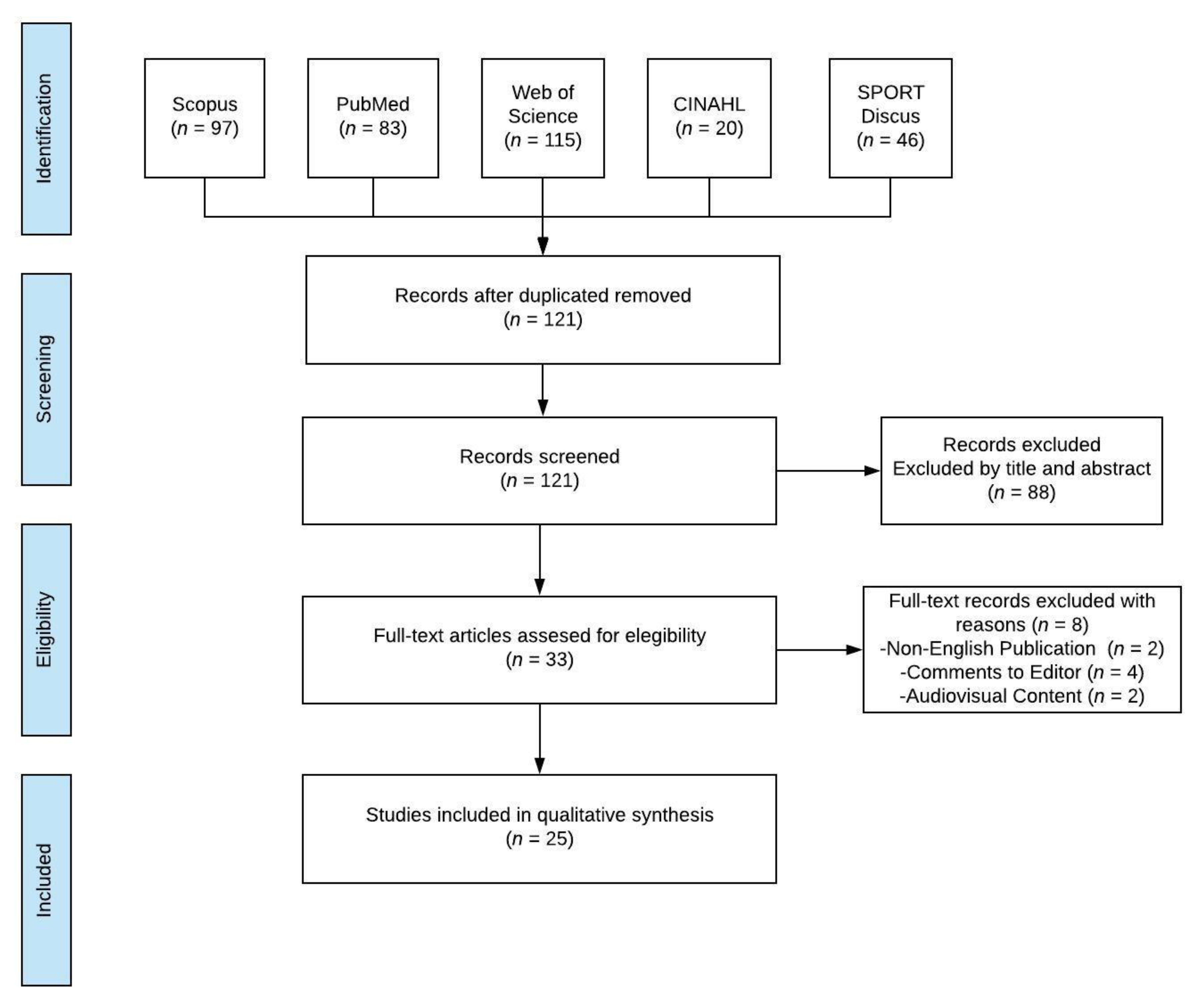
2. Materials and Methods
3. Results
4. Discussion
4.1. Future Research Directions
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dretakis, E.K.; Kondoyannis, P.N. Congenital scoliosis associated with encephalopathy in five children of two families. J. Bone Jt. Surg. Ser. A 1974, 56, 1747–1750. [Google Scholar] [CrossRef]
- Crisfield, R.J. Scoliosis with progressive external ophthalmoplegia in four siblings. J. Bone Jt. Surg. 1974, 56, 484–489. [Google Scholar] [CrossRef]
- Rousan, L.A.; Qased, A.B.L.; Audat, Z.A.; Ababneh, L.T.; Jaradat, S.A. Horizontal gaze palsy and progressive scoliosis with two novel ROBO3 gene mutations in two Jordanian families. Ophthalmic Genet. 2019, 40, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Amouri, R.; Nehdi, H.; Bouhlal, Y.; Kefi, M.; Larnaout, A.; Hentati, F. Allelic ROBO3 heterogeneity in Tunisian patients with horizontal gaze palsy with progressive scoliosis. J. Mol. Neurosci. 2009, 39, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Bosley, T.M.; Salih, M.A.M.; Jen, J.C.; Lin, D.D.M.; Oystreck, D.; Abu-Amero, K.K.; MacDonald, D.B.; Al Zayed, Z.; Al Dhalaan, H.; Kansu, T.; et al. Neurologic features of horizontal gaze palsy and progressive scoliosis with mutations in ROBO3. Neurology 2005, 64, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Amoiridis, G.; Tzagournissakis, M.; Christodoulou, P.; Karampekios, S.; Latsoudis, H.; Panou, T.; Simos, P.; Plaitakis, A. Patients with horizontal gaze palsy and progressive scoliosis due to ROBO3 E319K mutation have both uncrossed and crossed central nervous system pathways and perform normally on neuropsychological testing. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Jen, J.C.; Chan, W.M.; Bosley, T.M.; Wan, J.; Carr, J.R.; Rüb, U.; Shattuck, D.; Salamon, G.; Kudo, L.C.; Ou, J.; et al. Mutations in a Human ROBO Gene Disrupt Hindbrain Axon Pathway Crossing and Morphogenesis. Science 2006, 304, 1509–1513. [Google Scholar] [CrossRef] [Green Version]
- Jen, J.; Coulin, C.J.J.; Bosley, T.M.M.; Salih, M.A.M.A.M.; Sabatti, C.; Nelson, S.F.F.; Baloh, R.W.W. Familial horizontal gaze palsy with progressive scoliosis maps to chromosome 11q23-25. Neurology 2002, 59, 432–435. [Google Scholar] [CrossRef]
- Sabatier, C.; Plump, A.S.; Ma, L.; Brose, K.; Tamada, A.; Murakami, F.; Lee, E.Y.H.P.; Tessier-Lavigne, M. The divergent robo family protein Rig-1/Robo3 is a negative regulator of slit responsiveness required for midline crossing by commissural axons. Cell 2004. [Google Scholar] [CrossRef] [Green Version]
- Friocourt, F.; Chédotal, A. The Robo3 receptor, a key player in the development, evolution, and function of commissural systems. Dev. Neurobiol. 2017, 77, 876–890. [Google Scholar] [CrossRef] [Green Version]
- Ng, A.S.L.L.; Sitoh, Y.-Y.Y.; Zhao, Y.; Teng, E.W.L.L.; Tan, E.K.; Tan, L.C.S.S. Ipsilateral stroke in a patient with horizontal gaze palsy with progressive scoliosis and a subcortical infarct. Stroke 2011, 42, e1–e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieh, C.; Lengyel, D.; Neff, A.; Fretz, C.; Gottlob, I. Brainstem hypoplasia in familial horizontal gaze palsy and scoliosis. Neurology 2002, 59, 462–463. [Google Scholar] [CrossRef]
- Samoladas, E.P.; O’Dowd, J.; Cardoso-Almeida, A.; Demetriades, A.K. Horizontal gaze palsy and scoliosis: A case report and review of the literature. Hippokratia 2013, 17, 370–372. [Google Scholar] [PubMed]
- Abu-Amero, K.K.; Faletra, F.; Gasparini, P.; Parentin, F.; Pensiero, S.; Alorainy, I.A.; Hellani, A.M.; Catalano, D.; Bosley, T.M. Horizontal gaze palsy and progressive scoliosis without ROBO3 mutations. Ophthalmic Genet. 2011, 32, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools|National Heart; Lung, and Blood Institute (NHLBI). Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 15 December 2018).
- Steffen, H.; Rauterberg-Ruland, I.; Breitbach, N.; Thomsen, M.; Kolling, G. Familial congenital horizontal gaze paralysis and kyphoscoliosis. Neuropediatrics 1998, 29, 220–222. [Google Scholar] [CrossRef]
- Lo, B.; Faiyaz-Ul-Haque, M.; Banwell, B.; Blaser, S.; Paterson, A.; Tsui, L.-C.; Teebi, A. The locus responsible for horizontal gaze palsy/progressive scoliosis and brainstem hypoplasia is refined to a 9-cM region on chromosome 11q23. Clin. Genet. 2004, 65, 137–142. [Google Scholar] [CrossRef]
- Incecik, F.; Elkay, M.M.; Herguner, M.O.; Yerdelen, D.; Ozcan, K.; Atlunbasak, S.; Incecik, F.; Hergüner, M.Ö.; Yerdelen, D.; Özcan, K.; et al. Two siblings with familial idiopathic scoliosis with conjugate gaze palsy. J. Child Neurol. 2005, 20, 81–83. [Google Scholar] [CrossRef]
- Chan, W.M.; Traboulsi, E.I.; Arthur, B.; Friedman, N.; Andrews, C.; Engle, E.C. Horizontal gaze palsy with progressive scoliosis can result from compound heterozygous mutations in ROBO3. J. Med. Genet. 2006, 43, e11. [Google Scholar] [CrossRef] [Green Version]
- Abu-Amero, K. Gene symbol: ROBO3. Disease: Gaze Palsy, horizontal, with progressive scoliosis. Hum. Genet. 2008, 123, 540. [Google Scholar] [PubMed]
- Jain, N.; Jethani, J.; Narendran, K.; Kanth, L. Synergistic convergence and split pons in horizontal gaze palsy and progressive scoliosis in two sisters. Indian J. Ophthalmol. 2011, 59, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Bakbak, B.; Kansu, T. Acquired convergence substitution in horizontal gaze palsy and progressive scoliosis associated with ROBO3 mutations. Neuro-Ophthalmol. 2012, 36, 203–207. [Google Scholar] [CrossRef]
- Kurian, M.; Megevand, C.; De Haller, R.; Merlini, L.; Boex, C.; Truffert, A.; Kaelin, A.; Burglen, L.; Korff, C.M. Early-onset or rapidly progressive scoliosis in children: Check the eyes. Eur. J. Paediatr. Neurol. 2013, 17, 671–675. [Google Scholar] [CrossRef]
- Marques, N.B.P.S.M.; Barros, S.R.; Miranda, A.F.; Nobre Cardoso, J.; Parreira, S.; Fonseca, T.; Donaire, N.M.; Campos, N. Horizontal Gaze Palsy and Progressive Scoliosis with ROBO 3 Mutations in Patients from Cape Verde. J. Neuro-Ophthalmol. 2017, 37, 162–165. [Google Scholar] [CrossRef]
- Rossi, A.; Catala, M.; Biancheri, R.; Di Comite, R.; Tortori-Donati, P. MR imaging of brain-stem hypoplasia in horizontal gaze palsy with progressive scoliosis. Am. J. Neuroradiol. 2004, 25, 1046–1048. [Google Scholar]
- dos Santos, A.V.; Matias, S.; Saraiva, P.; Goulão, A. MR imaging features of brain stem hypoplasia in familial horizontal gaze palsy and scoliosis. Am. J. Neuroradiol. 2006, 27, 1382–1383. [Google Scholar]
- Haller, S.; Wetzel, S.G.; Lutschg, J. Functional MRI, DTI and neurophysiology in horizontal gaze palsy with progressive scoliosis. Neuroradiology 2008, 50, 453–459. [Google Scholar] [CrossRef]
- Bomfim, R.C.; Távora, D.G.F.; Nakayama, M.; Gama, R.L. Horizontal gaze palsy with progressive scoliosis: CT and MR findings. Pediatr. Radiol. 2009, 39, 184–187. [Google Scholar] [CrossRef]
- Avadhani, A.; Ilayaraja, V.; Shetty, A.P.; Rajasekaran, S. Diffusion tensor imaging in horizontal gaze palsywith progressive scoliosis. Magn. Reson. Imaging 2010, 28, 212–216. [Google Scholar] [CrossRef]
- Abu-Amero, K.K.; Kapoor, S.; Hellani, A.; Monga, S.; Bosley, T.M. Horizontal gaze palsy and progressive scoliosis due to a deleterious mutation in ROBO3. Ophthalmic Genet. 2011, 32, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Volk, A.E.; Carter, O.; Fricke, J.; Herkenrath, P.; Poggenborg, J.; Borck, G.; Demant, A.W.; Ivo, R.; Eysel, P.; Kubisch, C.; et al. Horizontal gaze palsy with progressive scoliosis: Three novel ROBO3 mutations and descriptions of the phenotypes of four patients. Mol. Vis. 2011, 17, 1978–1986. [Google Scholar] [PubMed]
- Pina, S.; Pedrosa, C.; Feijóo, B.; Machado, S.; Prieto, I.; Costa, C.; Santos, M.J. Horizontal Gaze Palsy With Progressive Scoliosis and Severe Keratoconus With a Compound Heterozygous Mutation in ROBO3. J. Pediatr. Ophthalmol. Strabismus 2014, 51, e29–e32. [Google Scholar] [CrossRef] [PubMed]
- Bozdoğan, S.T.; Dinç, E.; Sarı, A.A.; Özgür, A.; Bişgin, A. A novel mutation of ROBO3 in horizontal gaze palsy with progressive scoliosis. Ophthalmic Genet. 2017, 38, 284–285. [Google Scholar] [CrossRef]
- Lin, C.-W.; Lo, C.-P.; Tu, M.-C. Horizontal gaze palsy with progressive scoliosis: A case report with magnetic resonance tractography and electrophysiological study. BMC Neurol. 2018, 18, 75. [Google Scholar] [CrossRef] [Green Version]
- Abu-Amero, K.K.; Dhalaan, H.A.; Zayed, Z.A.; Hellani, A.; Bosley, T.M.; Al Dhalaan, H.; Al Zayed, Z.; Hellani, A.; Bosley, T.M. Five new consanguineous families with horizontal gaze palsy and progressive scoliosis and novel ROBO3 mutations. J. Neurol. Sci. 2009, 276, 22–26. [Google Scholar] [CrossRef]
- Marillat, V.; Sabatier, C.; Failli, V.; Matsunaga, E.; Sotelo, C.; Tessier-Lavigne, M.; Chédotal, A. The slit receptor Rig-1/Robo3 controls midline crossing by hindbrain precerebellar neurons and axons. Neuron 2004, 43, 69–79. [Google Scholar] [CrossRef]
- Chen, Z.; Gore, B.B.; Long, H.; Ma, L.; Tessier-Lavigne, M. Alternative Splicing of the Robo3 Axon Guidance Receptor Governs the Midline Switch from Attraction to Repulsion. Neuron 2008. [Google Scholar] [CrossRef] [Green Version]
- Zelina, P.; Blockus, H.; Zagar, Y.; Péres, A.; Friocourt, F.; Wu, Z.; Rama, N.; Fouquet, C.; Hohenester, E.; Tessier-Lavigne, M.; et al. Signaling switch of the axon guidance receptor Robo3 during vertebrate evolution. Neuron 2014. [Google Scholar] [CrossRef] [Green Version]
- Comer, J.D.; Pan, F.C.; Willet, S.G.; Haldipur, P.; Millen, K.J.; Wright, C.V.E.; Kaltschmidt, J.A. Sensory and spinal inhibitory dorsal midline crossing is independent of Robo3. Front. Neural Circuits 2015. [Google Scholar] [CrossRef] [Green Version]
- Engle, E.C. Human genetic disorders of axon guidance. Cold Spring Harb. Perspect. Biol. 2010, 2, a001784. [Google Scholar] [CrossRef] [PubMed]
- Camurri, L.; Mambetisaeva, E.; Davies, D.; Parnavelas, J.; Sundaresan, V.; Andrews, W. Evidence for the existence of two Robo3 isoforms with divergent biochemical properties. Mol. Cell. Neurosci. 2005, 30, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Hackenberg, A.; Boltshauser, E.; Gerth-Kahlert, C.; Stahr, N.; Azzarello-Burri, S.; Plecko, B. Horizontal gaze palsy in two brothers with compound heterozygous ROBO3 gene mutations. Neuropediatrics 2016, 48, 57–58. [Google Scholar] [PubMed]
- Fernández-Vega Cueto, A.; Rodríguez-Ezcurra, J.J.; Rodríguez-Maiztegui, I. Parálisis de la mirada horizontal y escoliosis progresiva en un paciente con endotropia congénita y limitación de abducción. A propósito de un caso. Arch. Soc. Esp. Oftalmol. 2016, 91, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Ungaro, C.; Valentini, S.; Cerasa, A.; Lanza, P.L.; Mazzei, R. Horizontal Gaze Palsy With Progressive Scoliosis. J. Neuro-Ophthalmol. 2018, 38, 131–132. [Google Scholar] [CrossRef]
- Khan, A.O.; Oystreck, D.T.; Al-Tassan, N.; Al-Sharif, L.; Bosley, T.M. Bilateral synergistic convergence associated with homozygous ROB03 mutation (p.Pro771Leu). Ophthalmology 2008, 115, 2262–2265. [Google Scholar] [CrossRef]
- Yamada, S.; Okita, Y.; Shofuda, T.; Yoshioka, E.; Nonaka, M.; Mori, K.; Nakajima, S.; Kanemura, Y. Ipsilateral hemiparesis caused by putaminal hemorrhage in a patient with horizontal gaze palsy with progressive scoliosis: A case report. BMC Neurol. 2015. [Google Scholar] [CrossRef] [Green Version]
- Arlt, E.M.; Keindl, T.K.; Grabner, G.; Krall, E.M.; Meissnitzer, M.W. Horizontale Blickparese mit progredienter Skoliose. Klin. Monbl. Augenheilkd. 2015, 232, 281–282. [Google Scholar] [CrossRef]
- Khan, A.O.; Abu-Amero, K. Infantile esotropia with cross-fixation, inability to abduct, and underlying horizontal gaze palsy with progressive scoliosis. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2014, 18, 389–391. [Google Scholar] [CrossRef]
- Nugent, A.A.; Kolpak, A.L.; Engle, E.C. Human disorders of axon guidance. Curr. Opin. Neurobiol. 2012, 22, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Bouvier, J.; Thoby-Brisson, M.; Renier, N.; Dubreuil, V.; Ericson, J.; Champagnat, J.; Pierani, A.; Chédotal, A.; Fortin, G. Hindbrain interneurons and axon guidance signaling critical for breathing. Nat. Neurosci. 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungaro, C.; Mazzei, R.; Sprovieri, T. Horizontal gaze palsy with progressive scoliosis: Is scoliosis linked to ROBO3 mutations? Neurol. Sci. 2019, 40, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Ungaro, C.; Mazzei, R.; Cavallaro, S.; Sprovieri, T. The spectrum of ROBO3 mutations in horizontal gaze palsy with progressive scoliosis: An update. Neurosci. Med. 2018, 9, 187–197. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author (Year) | Design | Conflict | Age (Years) | Subjects | % Females | Cases Relationship | Ethnicity | Parents Relationship |
|---|---|---|---|---|---|---|---|---|
| Steffen et al. [18] (1998) | CS | NR | 6.75 | 2 | 100 | Sisters | NR | C |
| Jen et al. [8] (2002) | CS | NR | 0.1–18 | 6 | 33 | Family | Indian/Arabian | C |
| Pieh et al. [12] (2002) | CS | NR | 32 | 2 | 0 | Brothers | Italian | C |
| Lo et al. [19] (2004) | CS | NR | 12 | 3 | 66.6 | Siblings | Pakistani | NC |
| Rossi et al. [27] (2004) | CR | NR | 13 | 1 | 100 | NA | NR | C |
| Incecik et al. [20] (2005) | CS | NR | 15 | 2 | 50 | Siblings | NR | C |
| Chan et al. [21] (2006) | CS | No | 3 | 2 | 50 | None | Caucasian | NC |
| Dos Santos et al. [28] (2006) | CR | NR | 2 | 1 | 0 | NA | NR | NC |
| Haller et al. [29] (2008) | CR | No | 14 | 1 | 0 | NA | Kosovar | NR |
| Abu-Amero et al. [37] (2009) | CS | No | 11.1 | 7 | 71 | Brothers/Sisters | Saudi Arabian/Sudanese | C |
| Amouri et al. [4] (2009) | CS | NR | 6–34 | 10 | NR | NR | Tunisian | C |
| Bomfim et al. [30] (2009) | CR | NR | 7 | 1 | 0 | NA | Brazilian | C |
| Avadhani et al. [31] (2010) | CR | NR | 14 | 1 | 0 | NA | Indian | NC |
| Abu-Amero et al. [32] (2011) | CS | No | 11.2 | 4 | 0 | Brothers | Afghani | C |
| Abu-Amero et al. [14] (2011) | CR | No | 8 | 1 | 0 | Mother | Serbian | NC |
| Jain et al. [23] (2011) | CS | NR | 10.5 | 2 | 100 | Sisters | Indian | NR |
| Ng et al. [11] (2011) | CR | NR | 55 | 1 | 0 | NA | Indian | C |
| Volk et al. [33] (2011) | CR | NR | 6.9 | 4 | 100 | Sisters/None | Turkish/Saudi Arabian | C |
| Bakbak and Kansu [24] (2012) | CS | No | 13 | 2 | 100 | Sisters | Turkish | C |
| Kurian et al. [25] (2013) | CS | NR | 6.75 | 2 | 100 | None | Kosovar/Qatari | C |
| Pina et al. [34] (2014) | CR | NR | 13 | 1 | 100 | NA | Portuguese | NC |
| Bozdoğan et al. [35] (2017) | CR | No | 22 | 1 | 100 | None | Turkish | C |
| Mendes Marques et al. [26] (2017) | CS | No | 12 | 2 | 50 | NA | African | NC |
| Lin et al. [36] (2018) | CR | NR | 55 | 1 | 100 | None | NR | NC |
| Rousan et al. [3] (2019) | CS | No | 12.8 | 6 | 66.6 | Family | Jordanian | C |
| Author (Year) | BCVA | Tropias | Horizontal Gaze | Vertical Gaze | MRI | Spine |
|---|---|---|---|---|---|---|
| Steffen et al. [18] (1998) | 20/30 | NR | Absence | Normal | Normal | Cobb’s angle 45° |
| Jen et al. [8] (2002) | NR | ET (33%) | Absence | Normal | NR | Moderate scoliosis |
| Pieh et al. [12] (2002) | 20/30 | NR | Absence | Normal | BH and MO | NR |
| Lo et al. [19] (2004) | NR | Right ET | Palsy | Limited | BH and MO | Cobb’s angle 12° |
| Rossi et al. [27] (2004) | NR | NR | Absence | Normal | BH and MO | Severe scoliosis |
| Incecik et al. [20] (2005) | 20/30 | Normal | Restricted | Normal | NB and MM | Thoracolumbar scoliosis |
| Chan et al. [21] (2006) | 20/40 | 15 ∆ ET | Absence | Normal | BH and MO | Profound scoliosis |
| Dos Santos et al. [28] (2006) | NR | Normal | Absence | Normal | BH and MO | Thoracolumbar scoliosis |
| Haller et al. [29] (2008) | NR | NR | Absence | Normal | BH and MO | Cobb´s angle 20° |
| Abu-Amero et al. [37] (2009) | NR | NR | Absence | Normal | BH | Left concave |
| Amouri et al. [4] (2009) | NR | NR | Absence | Normal | BH and MO | Thoracolumbar scoliosis |
| Bomfim et al. [30] (2009) | NR | NR | Absence | Normal | BH and MO | Mild thoracolumbar scoliosis |
| Avadhani et al. [31] (2010) | NR | NR | Absence | Normal | BH and MO | Cobb´s angle 32° and 63° |
| Abu-Amero et al. [32] (2011) | 20/25 | Mild ET | Absence | Normal | BH and MO | Kyphoscoliosis |
| Abu-Amero et al. [14] (2011) | NR | Mild left hypertropia | Absence | Normal | BH and MO | Concave 125° thoracolumbar kyphoscoliosis |
| Jain et al. [23] (2011) | 20/32 | 25 ∆ ET | Absence | Normal | BH | Left kyphosis |
| Ng et al. [11] (2011) | NR | NR | Absence | Normal | BH and MO | NR |
| Volk et al. [33] (2011) | 20/32 | −10° XT | Absence | Normal | BH | Cobb’s angle 30° |
| Bakbak and Kansu [24] (2012) | 20/35 | NR | Absence | Normal | BH and MO | Moderate scoliosis |
| Kurian et al. [25] (2013) | NR | Left Tropia | Absence | Normal | BH and MO | Cobb’s angle 125° |
| Pina et al. [34] (2014) | 20/80 | Orthotropic | Palsy | NR | BH and AFC | Dorsal thoracolumbar scoliosis with torticollis over the left shoulder |
| Bozdoğan et al. [35] (2017) | 20/32 | Over 40 ∆ XT | Limited | Normal | BH and MO | Severe thoracic scoliosis |
| Mendes Marques et al. [26] (2017) | Normal | Orthophoria | Palsy | Normal | BH | Thoracolumbar scoliosis |
| Lin et al. [36] (2018) | Normal | NR | Palsy | Normal | BH and MO | Scoliosis thoracic and lumbar spine |
| Rousan et al. [3] (2019) | NR | Left hypertropia | Limited abduction | Normal | BH | Severe thoracic scoliosis |
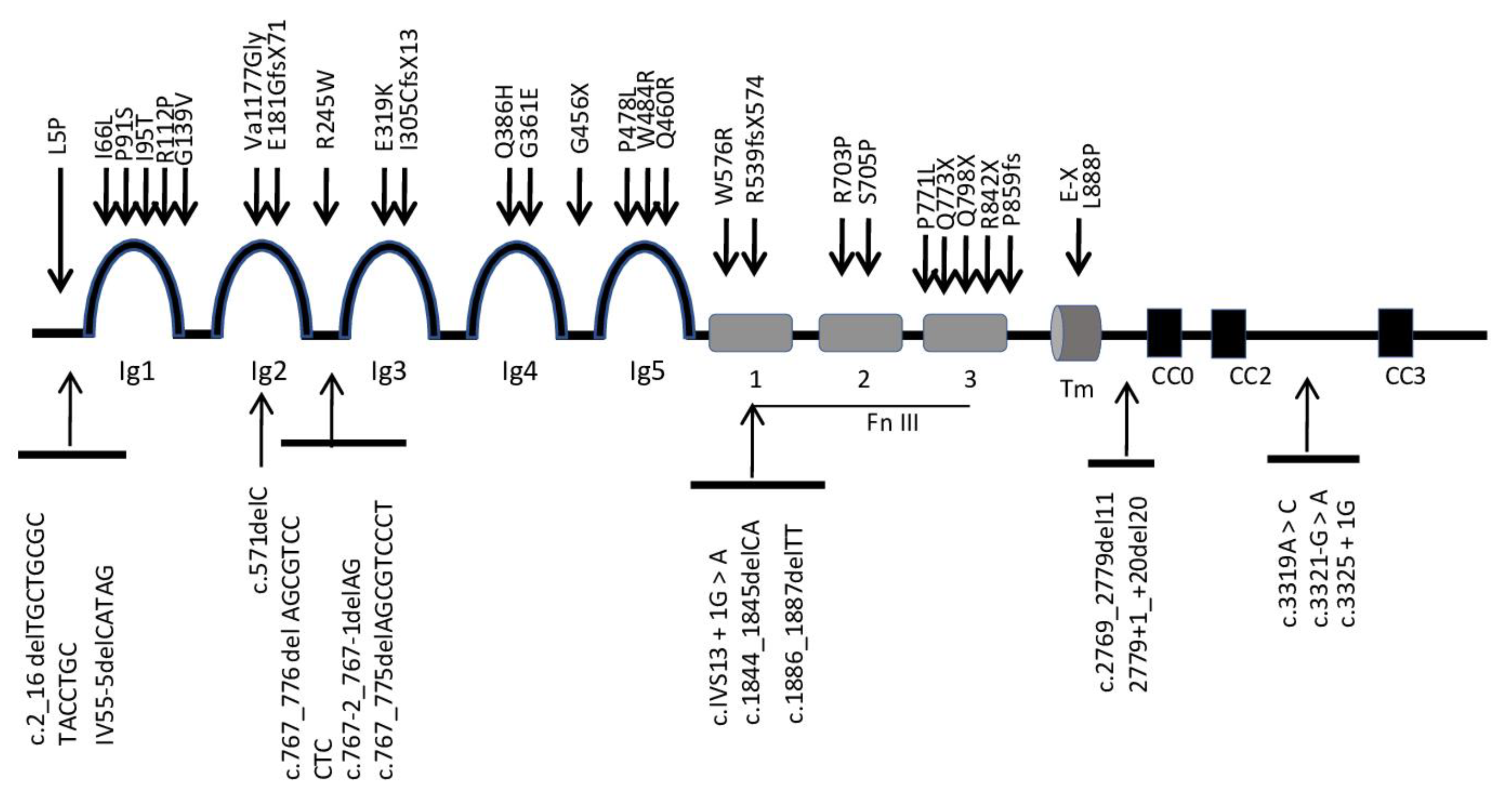
| Nucleotide Change | Exon | Amino Acid Change | Domain | Ethnicity | Reference |
|---|---|---|---|---|---|
| c.14T > C | 1 | L5P | Nter | Italian | Jen et al., [7] 2004 |
| c.2_16 delTGCTGCGCTACCTGC | 1 | Saudi | Abu-Amero et al., [32] 2011 | ||
| IV55-5delCATAG | 2 | Cape Verde | Mendes Marques et al., [26] 2017 | ||
| c.196A > C | 2 | I66L | Ig1 | Greek | Jen et al., [7] 2004 |
| c.271C > T | 2 | P91S | Ig1 | Sudanese | Abu-Amero et al., [37] 2009 |
| c.335G > C | 2 | R112P | Ig1 | Saudi | Abu-Amero et al., [37] 2009 |
| c.283T > C | 2 | I95T | Ig1 | Tunisian | Amouri et al., [4] 2009 |
| c.416G > T | 2 | G139V | Ig1 | Switzerland | Hackenberg et al., [44] 2016 |
| c.571delC | 2 | frameshift | Ig2 | Saudi | Abu-Amero et al., [37] 2009 |
| c.530dlT | 3 | Va1177Glyfs * 45 frameshift | Ig2 | Jordanian | Rousan et al., [3] 2019 |
| c.541dup | 3 | E181GfsX71 | Ig2 | Kosovar | Kurian et al., [25] 2013 |
| c.733C > T | 4 | R245W | Ig2–3 | Irish/English | Chan et al., [21] 2006 |
| c.733C > T | 4 | R245W | Ig2–3 | Tunisian | Amouri et al., [4] 2009, Chan 2006 [21] |
| c.767_776delAGCGTCCCTC | 5 | c.767_776delAGCGTCCCTC | Ig2–3 | Portuguese | Pina et al. [34] 2014 |
| c.767-2_767-1delAG | 5 | c.767-2_767-1delAG | Ig2–3 | Portuguese | Pina et al. [34] 2014 |
| c.767_775delAGCGTCCCT | 5 | c.767_775delAGCGTCCCT | Ig2–3 | Cape Verde | Mendes Marques et al., [26] 2017 |
| c.955G > A | 6 | E319K | Ig3 | Greek | Jen et al., [7] 2004 |
| c.913delAinsTGC | 6 | I305CfsX13 | Ig3 | Caucasian/Turkish | Volk et al., [33] 2011 |
| c.1082G > A | 7 | G361E | Ig4 | Indian | Jen et al., [7] 2004 |
| c.1158G > C | 7 | Q386H | Ig4 | Spanish | Fernández-Vega Cueto et al., [45] 2016 |
| c.1366G > T | 9 | G456X | Ig4–5 | Turkish | Jen et al., [7] 2004 |
| c.1379A > G | 9 | Q460R | Ig5 | Saudi | Abu-Amero et al., [37] 2009 |
| c.1450T > C | 9 | W484R | Ig5 | Tunisian | Amouri et al., [4] 2009 |
| c.1433C > T | 9 | P478L | Ig5 | Italian | Ungaro et al., [46] 2018 |
| c.1618delG | 10 | R539fsX574 | Fn III 1 | Tunisian | Amouri et al., [4] 2009 |
| c.1726T > C | 11 | W576R | Fn III 1 | Saudi | Abu-Amero et al., [37] 2009 |
| c.1886_1887delTT | 12 | frameshift | Fn III 1 | Irish/German | Chan et al., [21] 2006 |
| c.1844_1845delCA | 12 | frameshift | Fn III 1 | Irish/German | Chan et al., [21] 2006 |
| c.IVS13 + 1G > A | 13 | frameshift | Fn III 2 | Saudi | Jen et al., [7] 2004 |
| c.2108G > C | 14 | R703P | Fn III 2 | Turkish | Jen et al., [7] 2004 |
| c.2113T > C | 14 | S705P | Fn III 2 | Saudi | Jen et al., [7] 2004 |
| c.2310 + 1C | 15 | frameshift | Fn III 3 | Pakistani | Jen et al., [7] 2004 |
| c.2317C > T | 15 | Q773X | Fn III 3 | Irish/English | Chan et al., [21] 2006 |
| c.2312C > T | 15 | P771L | Fn III 3 | Saudi | Khan et al., [47] 2008 |
| c.2392C > T | 15 | Q798X | Fn III 3 | Japanese | Yamada et al., [48] 2015 |
| c.2576del | 16 | P859fs | Fn III 3 | Austrian | Arlt et al., [49] 2015 |
| c.2524C > T | 16 | R842X | Fn III 3 | Turkish | Bozdoğan et al., [35] 2017 |
| G > T * | 17 | ^E-X | TM | Indian | Ng et al., [11] 2011 |
| c.2663T > C | 17 | L888P | TM | Saudi | Khan and Abu-Amero, [50] 2014 |
| c.2769_2779del11 | 17 | Splicing defect + frameshift | TM-CC0 | Caucasian/Turkish | Volk et al., [33] 2011 |
| 2779+1_+20del20 | 17 | Splicing defect + frameshift | TM-CC0 | Caucasian/Turkish | Volk et al., [33] 2011 |
| c.3319A > C | 22 | skip + frameshift | CC2-CC3 | Caucasian/Turkish | Volk et al., [33] 2011 |
| c.3321-G > A | 22 | int 22 Splice site mut | CC2-CC3 | Italian | Ungaro et al., [46] 2018 |
| c.3325 + 1G | 23 | frameshift | CC2-CC | Saudi | Jen et al., [7] 2004 |
| c.3742C > T | 25 | (Arg1248 *) nonsense | CC3 | Jordanian | Rousan et al., [3] 2019 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinero-Pinto, E.; Pérez-Cabezas, V.; Tous-Rivera, C.; Sánchez-González, J.-M.; Ruiz-Molinero, C.; Jiménez-Rejano, J.-J.; Benítez-Lugo, M.-L.; Sánchez-González, M.C. Mutation in ROBO3 Gene in Patients with Horizontal Gaze Palsy with Progressive Scoliosis Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4467. https://doi.org/10.3390/ijerph17124467
Pinero-Pinto E, Pérez-Cabezas V, Tous-Rivera C, Sánchez-González J-M, Ruiz-Molinero C, Jiménez-Rejano J-J, Benítez-Lugo M-L, Sánchez-González MC. Mutation in ROBO3 Gene in Patients with Horizontal Gaze Palsy with Progressive Scoliosis Syndrome: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(12):4467. https://doi.org/10.3390/ijerph17124467
Chicago/Turabian StylePinero-Pinto, Elena, Verónica Pérez-Cabezas, Cristina Tous-Rivera, José-María Sánchez-González, Carmen Ruiz-Molinero, José-Jesús Jiménez-Rejano, María-Luisa Benítez-Lugo, and María Carmen Sánchez-González. 2020. "Mutation in ROBO3 Gene in Patients with Horizontal Gaze Palsy with Progressive Scoliosis Syndrome: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 12: 4467. https://doi.org/10.3390/ijerph17124467