Physical Activity Promotion: A Systematic Review of The Perceptions of Healthcare Professionals


Abstract
:1. Introduction
- What are HCPs’ perceptions regarding key determinants of PA promotion?
- What are HCPs’ perceptions about the barriers and facilitators to the achievement of PA promotional goals?
2. Methods
2.1. Inclusion and Exclusion Criteria
- Included adult participants aged 18 years and above.
- Considered HCPs’ attitudes or perceptions to PA promotion
- Considered opinions other than those of HCPs (e.g., patients)
- Were review papers and
- Perceptions of HCPs about PA promotion was not specifically discussed.
2.2. Search Strategy
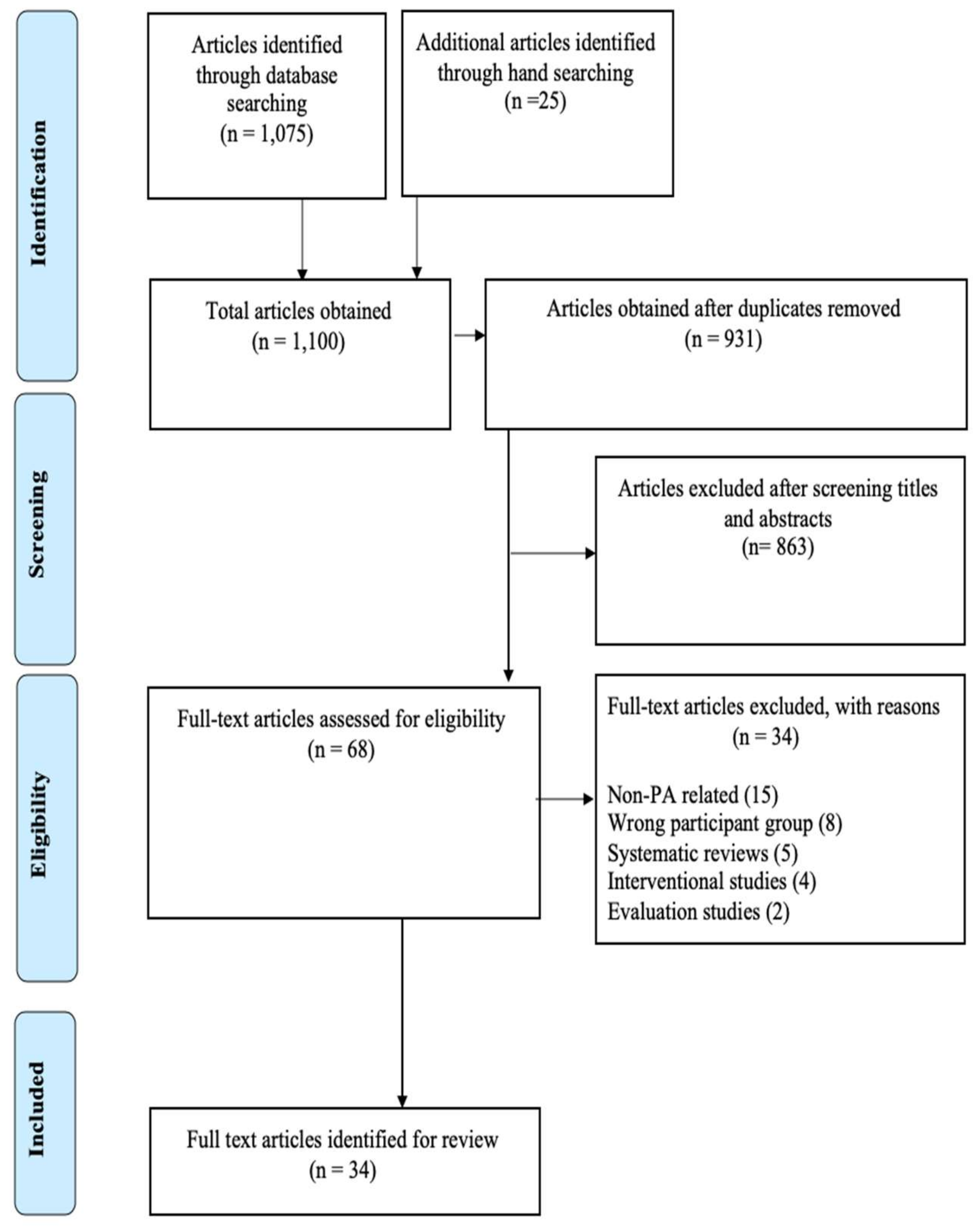
2.3. Study Selection
2.4. Data Synthesis and Analysis
2.5. Risk of Bias Assessment
3. Results
3.1. Included Studies
3.2. Study Characteristics
3.3. Healthcare Professionals (HCPs)’ Perceived Knowledge of Physical Activity (PA)
3.4. HCPs’ Perceived Confidence in Promoting PA
3.5. HCPs’ Perceived Importance of PA and Its Promotion
3.6. HCPs’ Perceived Role in PA Promotion
3.7. HCPs’ Perceptions on PA Assessment
3.8. HCPs’ Perceptions on how PA Was Promoted
3.9. HCPs’ Perceived Effectiveness in Promoting PA
3.10. HCPs’ Perceived Barriers and Facilitators to PA Promotion
3.11. Assessment of Methodological Quality
4. Discussion
4.1. Implications for Practice and Research
4.2. Strength and Limitation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A: Study Search Terms
Appendix B: Table Legend
References
- McNally, S. Exercise: The miracle cure for surgeons to fix the NHS and social care. Bull. R. Coll. Surg. Engl. 2020, 102, 28–33. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Health Organization Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Groessl, E.J. Effect of structured physical activity on prevention of major mobility disability in older adults: The LIFE study randomized clinical trial. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Action Plan on Physical Activity 2018-2030: More Active People for A Healthier World; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Berra, K.; Rippe, J.; Manson, J.E. Making physical activity counseling a priority in clinical practice: The time for action is now. JAMA 2015, 314, 2617–2618. [Google Scholar] [CrossRef]
- Kohl 3rd, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S.; Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Wen, C.P.; Wu, X. Stressing harms of physical inactivity to promote exercise. Lancet 2012, 380, 192–193. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.; Sallis, R.; Hutber, A.; Archer, E. Exercise therapy–the public health message. Scand. J. Med. Sci. Sports 2012, 22, e24–e28. [Google Scholar] [CrossRef]
- Lobelo, F.; Stoutenberg, M.; Hutber, A. The exercise is medicine global health initiative: A 2014 update. Br. J. Sports Med. 2014, 48, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Miura, S.-I.; Yamaguchi, Y.; Urata, H.; Himeshima, Y.; Otsuka, N.; Tomita, S.; Yamatsu, K.; Nishida, S.; Saku, K. Efficacy of a multicomponent programme (patient-centered assessment and counseling for exercise plus nutrition [PACE+ Japan]) for lifestyle modification in patients with essential hypertension. Hypertens. Res. 2004, 27, 859–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, R. Developing healthcare systems to support exercise: Exercise as the fifth vital sign. Br. Assoc. Sport Excer. Med. 2011, 45, 473–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Sluijs, E.M.; van Poppel, M.N.; Stalman, W.A.; van Mechelen, W. Feasibility and acceptability of a physical activity promotion programme in general practice. Fam. Pract. 2004, 21, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Petrella, R.J.; Lattanzio, C.N. Does counseling help patients get active? Systematic review of the literature. Can. Fam. Physician 2002, 48, 72–80. [Google Scholar]
- Carroll, J.K.; Antognoli, E.; Flocke, S.A. Evaluation of physical activity counseling in primary care using direct observation of the 5As. Anna. Fam. Med. 2011, 9, 416–422. [Google Scholar] [CrossRef]
- HP. Healthy People 2020. Available online: http://www.healthypeople.gov/2020/data-search/%20Search-the-Data?nid=5056 (accessed on 23 March 2020).
- Joy, E.L.; Blair, S.N.; McBride, P.; Sallis, R. Physical activity counselling in sports medicine: A call to action. Br. J. Sports Med. 2013, 47, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Cowan, R.E. Exercise is medicine initiative: Physical activity as a vital sign and prescription in adult rehabilitation practice. Arch. Phys. Med. Rehabil. 2016, 97, S232–S237. [Google Scholar] [CrossRef]
- Orrow, G.; Kinmonth, A.L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [Green Version]
- Varney, J.; Brannan, M.; Aaltonen, G. Everybody active, every day: An evidence-based approach to physical activity. Public Health Engl. 2014, 1, 26. [Google Scholar]
- Webb, J.; Hall, J.; Hall, K.; Fabunmi-Alade, R. Increasing the frequency of physical activity very brief advice by nurses to cancer patients. A mixed methods feasibility study of a training intervention. Public Health 2016, 139, 121–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, A.; Williams, K.; Beeken, R.; Wardle, J. Recall of physical activity advice was associated with higher levels of physical activity in colorectal cancer patients. BMJ Open 2015, 5, e006853. [Google Scholar] [CrossRef] [PubMed]
- Keyworth, C.; Epton, T.; Goldthorpe, J.; Calam, R.; Armitage, C.J. Are healthcare professionals delivering opportunistic behaviour change interventions? A multi-professional survey of engagement with public health policy. Implement. Sci. 2018, 13, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, C.; Shilton, T.; Westerman, L.; Varney, J.; Bull, F. World Health Organisation to develop global action plan to promote physical activity: Time for action. Br. Assoc. Sport Exer. Med. 2018, 52, 484–485. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Bull, F. Translating science to inform global policy on physical activity. J. Sport Health Sci. 2018, 7, 3. [Google Scholar] [CrossRef]
- Smith-Turchyn, J.; Richardson, J.; Tozer, R.; McNeely, M.; Thabane, L. Physical activity and breast cancer: A qualitative study on the barriers to and facilitators of exercise promotion from the perspective of health care professionals. Physiother. Can. 2016, 68, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Spellman, C.; Craike, M.; Livingston, P. Knowledge, attitudes and practices of clinicians in promoting physical activity to prostate cancer survivors. Health Educ. J. 2014, 73, 566–575. [Google Scholar] [CrossRef]
- Huijg, J.M.; Gebhardt, W.A.; Verheijden, M.W.; van der Zouwe, N.; de Vries, J.D.; Middelkoop, B.J.; Crone, M.R. Factors influencing primary health care professionals’ physical activity promotion behaviors: A systematic review. Int. J. Behav. Med. 2015, 22, 32–50. [Google Scholar] [CrossRef]
- Keogh, J.W.; Pühringer, P.; Olsen, A.; Sargeant, S.; Jones, L.M.; Climstein, M. Physical activity promotion, beliefs, and barriers among australasian oncology nurses. Oncol. Nurs. Forum 2017, 44, 235–245. [Google Scholar]
- Lowson, K.; Jenks, M.; Filby, A.; Carr, L.; Campbell, B.; Powell, J. Examining the implementation of NICE guidance: Cross-sectional survey of the use of NICE interventional procedures guidance by NHS Trusts. Implement. Sci. 2015, 10, 93. [Google Scholar] [CrossRef] [Green Version]
- Nelson, P.A.; Kane, K.; Chisholm, A.; Pearce, C.J.; Keyworth, C.; Rutter, M.K.; Chew-Graham, C.A.; Griffiths, C.E.; Cordingley, L.; Team, I. ‘I should have taken that further’–missed opportunities during cardiovascular risk assessment in patients with psoriasis in UK primary care settings: A mixed-methods study. Health Expect. 2016, 19, 1121–1137. [Google Scholar] [CrossRef] [PubMed]
- Noordman, J.; Verhaak, P.; van Dulmen, S. Discussing patient’s lifestyle choices in the consulting room: Analysis of GP-patient consultations between 1975 and 2008. BMC Fam. Pract. 2010, 11, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-H.; Oh, M.; Yoon, Y.J.; Lee, C.W.; Jones, L.W.; Kim, S.I.; Kim, N.K.; Jeon, J.Y. Characteristics of attitude and recommendation of oncologists toward exercise in South Korea: A cross sectional survey study. BMC Cancer 2015, 15, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dillen, S.; Noordman, J.; Van Dulmen, S.; Hiddink, G. Examining the content of weight, nutrition and physical activity advices provided by Dutch practice nurses in primary care: Analysis of videotaped consultations. Eur. J. Clin. Nutr. 2014, 68, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, K.; Beeken, R.J.; Fisher, A.; Wardle, J. Health professionals’ provision of lifestyle advice in the oncology context in the United Kingdom. Eur. J. Cancer Care 2015, 24, 522–530. [Google Scholar] [CrossRef]
- Bardach, S.H.; Schoenberg, N.E. The content of diet and physical activity consultations with older adults in primary care. Patient Educ. Couns. 2014, 95, 319–324. [Google Scholar] [CrossRef] [Green Version]
- Delgado, C.; Johansen, K.L. Deficient counseling on physical activity among nephrologists. Nephron Clin. Pract. 2010, 116, c330–c336. [Google Scholar] [CrossRef]
- Persson, G.; Brorsson, A.; Hansson, E.E.; Troein, M.; Strandberg, E.L. Physical activity on prescription (PAP) from the general practitioner’s perspective–a qualitative study. BMC Fam. Pract. 2013, 14, 128. [Google Scholar] [CrossRef] [Green Version]
- AuYoung, M.; Linke, S.E.; Pagoto, S.; Buman, M.P.; Craft, L.L.; Richardson, C.R.; Hutber, A.; Marcus, B.H.; Estabrooks, P.; Gorin, S.S. Integrating physical activity in primary care practice. Amer. J. Med. 2016, 129, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Elwell, L.; Povey, R.; Grogan, S.; Allen, C.; Prestwich, A. Patients’ and practitioners’ views on health behaviour change: A qualitative study. Psychol. Health 2013, 28, 653–674. [Google Scholar] [CrossRef]
- Keyworth, C.; Nelson, P.; Chisholm, A.; Griffiths, C.; Cordingley, L.; Bundy, C.; Identification and Management of Psoriasis-Associated Co-morbidiTy (IMPACT) team. Providing lifestyle behaviour change support for patients with psoriasis: An assessment of the existing training competencies across medical and nursing health professionals. Br. J. Derm. 2014, 171, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Weiler, R.; Chew, S.; Coombs, N.; Hamer, M.; Stamatakis, E. Physical activity education in the undergraduate curricula of all UK medical schools. Are tomorrow’s doctors equipped to follow clinical guidelines? Br. J. Sports Med. 2012, 46, 1024–1026. [Google Scholar] [CrossRef] [PubMed]
- Bonner, C.; Jansen, J.; McKinn, S.; Irwig, L.; Doust, J.; Glasziou, P.; McCaffery, K. How do general practitioners and patients make decisions about cardiovascular disease risk? Health Psychol. 2015, 34, 253. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; McKinn, S.; Bonner, C.; Irwig, L.; Doust, J.; Glasziou, P.; Bell, K.; Naganathan, V.; McCaffery, K. General practitioners’ decision making about primary prevention of cardiovascular disease in older adults: A qualitative study. PLoS ONE 2017, 12, e0170228. [Google Scholar] [CrossRef] [PubMed]
- Raghupathi, W.; Raghupathi, V. An empirical study of chronic diseases in the United States: A visual analytics approach to public health. Int. J. Env. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [Green Version]
- McPhail, S.M. Multimorbidity in chronic disease: Impact on health care resources and costs. Risk Manag. Healthc. Policy 2016, 9, 143. [Google Scholar] [CrossRef] [Green Version]
- Barnes, K.; Ball, L.; Galvão, D.A.; Newton, R.U.; Chambers, S.K.; Harrison, C. Physical activity counselling and referrals by general practitioners for prostate cancer survivors in Australia. Aust. J. Prim. Health 2019, 25, 152–156. [Google Scholar] [CrossRef]
- Din, N.U.; Moore, G.F.; Murphy, S.; Wilkinson, C.; Williams, N.H. Health professionals’ perspectives on exercise referral and physical activity promotion in primary care: Findings from a process evaluation of the National Exercise Referral Scheme in Wales. Health Educ. J. 2015, 74, 743–757. [Google Scholar] [CrossRef] [Green Version]
- Haussmann, A.; Gabrian, M.; Ungar, N.; Jooß, S.; Wiskemann, J.; Sieverding, M.; Steindorf, K. What hinders healthcare professionals in promoting physical activity towards cancer patients? The influencing role of healthcare professionals’ concerns, perceived patient characteristics and perceived structural factors. Eur. J. Cancer Care 2018, 27, e12853. [Google Scholar] [CrossRef]
- Aromataris, E.; Pearson, A. The systematic review: An overview. AJN Am. J. Nurs. 2014, 114, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleuren, M.; Wiefferink, K.; Paulussen, T. Determinants of innovation within health care organizations: Literature review and Delphi study. Int. J. Qual. Health Care 2004, 16, 107–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudoir, S.R.; Dugan, A.G.; Barr, C.H. Measuring factors affecting implementation of health innovations: A systematic review of structural, organizational, provider, patient, and innovation level measures. Implement. Sci. 2013, 8, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A. Making psychological theory useful for implementing evidence based practice: A consensus approach. BMJ Qual. Saf. 2005, 14, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef]
- Cantwell, M.; Walsh, D.; Furlong, B.; Moyna, N.; McCaffrey, N.; Boran, L.; Smyth, S.; Woods, C. Healthcare professionals’ knowledge and practice of physical activity promotion in cancer care: Challenges and solutions. Eur. J. Cancer Care 2018, 27. [Google Scholar] [CrossRef]
- Eisele, A.; Schagg, D.; Göhner, W. Exercise promotion in physiotherapy: A qualitative study providing insights into German physiotherapists’ practices and experiences. Musculoskelet. Sci. Pract. 2020, 45. [Google Scholar] [CrossRef]
- Haussmann, A.; Ungar, N.; Gabrian, M.; Tsiouris, A.; Sieverding, M.; Wiskemann, J.; Steindorf, K. Are healthcare professionals being left in the lurch? The role of structural barriers and information resources to promote physical activity to cancer patients. Support. Care Cancer 2018, 26, 4087–4096. [Google Scholar] [CrossRef] [PubMed]
- Hurkmans, E.J.; De Gucht, V.; Maes, S.; Peeters, A.J.; Ronday, H.K.; Vlieland, T.P.V. Promoting physical activity in patients with rheumatoid arthritis: Rheumatologists’ and health professionals’ practice and educational needs. Clin. Rheumatol. 2011, 30, 1603–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorgensen, T.K.; Nordentoft, M.; Krogh, J. How do general practitioners in Denmark promote physical activity? Scand. J. Prim. Health Care 2012, 30, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemrijse, C.J.; De Bakker, D.H.; Ooms, L.; Veenhof, C. Collaboration of general practitioners and exercise providers in promotion of physical activity a written survey among general practitioners. BMC Fam. Pract. 2015, 16, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulligan, H.; Fjellman-Wiklund, A.; Hale, L.; Thomas, D.; Häger-Ross, C. Promoting physical activity for people with neurological disability: Perspectives and experiences of physiotherapists. Physiother. Theory Pract. 2011, 27, 399–410. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.; Prihodova, L.; Heffron, M.; Wright, P. Physical activity counselling in Ireland: A survey of doctors’ knowledge, attitudes and self-reported practice. BMJ Open Sport Exer. Med. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Sassen, B.; Kok, G.; Vanhees, L. Predictors of healthcare professionals’ intention and behaviour to encourage physical activity in patients with cardiovascular risk factors. BMC Public Health 2011, 11, 246. [Google Scholar] [CrossRef] [Green Version]
- Suija, K.; Pechter, U.; Maaroos, J.; Kalda, R.; Ratsep, A.; Oona, M.; Maaroos, H.I. Physical activity of Estonian family doctors and their counselling for a healthy lifestyle: A cross-sectional study. BMC Fam. Pract. 2010, 11, 48. [Google Scholar] [CrossRef] [Green Version]
- Barrett, E.M.; Darker, C.D.; Hussey, J. Promotion of physical activity in primary care: Knowledge and practice of general practitioners and physiotherapists. J. Public Health 2013, 21, 63–69. [Google Scholar] [CrossRef]
- Burton, N.W.; Pakenham, K.I.; Brown, W.J. Are psychologists willing and able to promote physical activity as part of psychological treatment? Int. J. Behav. Med. 2010, 17, 287–297. [Google Scholar] [CrossRef]
- Frantz, J.M.; Ngambare, R. Physical activity and health promotion strategies among physiotherapists in Rwanda. Afr. Health Sci. 2013, 13, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freene, N.; Cools, S.; Bissett, B. Are we missing opportunities? Physiotherapy and physical activity promotion: A cross-sectional survey. BMC Sports Sci. Med. Rehabilit. 2017, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Kolt, G.S.; Keogh, J.W.L.; Schofield, G.M. The green prescription and older adults: What do general practitioners see as barriers? J. Prim. Health Care 2012, 4, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Schofield, G.M.; Kolt, G.S.; Keogh, J.W. General practitioners’ views and experiences of counselling for physical activity through the New Zealand Green Prescription programme. BMC Fam. Pract. 2011, 12, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirley, D.; Van der Ploeg, H.P.; Bauman, A.E. Physical activity promotion in the physical therapy setting: Perspectives from practitioners and students. Phys. Ther. 2010, 90, 1311–1322. [Google Scholar] [CrossRef] [Green Version]
- Speake, H.; Copeland, R.; Breckon, J.; Till, S. Challenges and opportunities for promoting physical activity in health care: A qualitative enquiry of stakeholder perspectives. Eur. J. Physiother. 2019, 1–8. [Google Scholar] [CrossRef]
- Kinnafick, F.E.; Papathomas, A.; Regoczi, D. Promoting exercise behaviour in a secure mental health setting: Healthcare assistant perspectives. Int. J. Ment. Health Nurs. 2018, 27, 1776–1783. [Google Scholar] [CrossRef] [Green Version]
- Litchfield, I.; Narendran, P.; Andrews, R.; Greenfield, S. Patient and healthcare professionals perspectives on the delivery of exercise education for patients with type 1 diabetes. Front. Endocrinol. 2019, 10, 76. [Google Scholar] [CrossRef]
- Lowe, A.; Littlewood, C.; McLean, S. Understanding physical activity promotion in physiotherapy practice: A qualitative study. Musculoskelet. Sci. Pract. 2018, 35, 1–7. [Google Scholar] [CrossRef]
- Williams, T.L.; Smith, B.; Papathomas, A. Physical activity promotion for people with spinal cord injury: Physiotherapists’ beliefs and actions. Disabil. Rehabil. 2018, 40, 52–61. [Google Scholar] [CrossRef]
- Courtney-Long, E.A.; Stevens, A.C.; Carroll, D.D.; Griffin-Blake, S.; Omura, J.D.; Carlson, S.A. Primary care providers’ level of preparedness for recommending physical activity to adults with disabilities. Prev. Chronic Dis. 2017, 14, E114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omura, J.D.; Bellissimo, M.P.; Watson, K.B.; Loustalot, F.; Fulton, J.E.; Carlson, S.A. Primary care providers’ physical activity counseling and referral practices and barriers for cardiovascular disease prevention. Prev. Med. 2018, 108, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.A.; Mangold, K.; Kosiorek, H.E.; Montez, M.; Smith, D.M.; Tyler, B.J. Registered nurse intent to promote physical activity for hospitalised liver transplant recipients. J. Nurs. Manag. 2018, 26, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Pojednic, R.M.; Polak, R.; Arnstein, F.; Kennedy, M.A.; Bantham, A.; Phillips, E.M. Practice patterns, counseling and promotion of physical activity by sports medicine physicians. J. Sci. Med. Sport 2017, 20, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Tucker, C.M.; Shah, N.R.; Ukonu, N.A.; Bilello, L.A.; Kang, S.; Good, A.J.; Arthur, T.M. Views of primary care physicians regarding the promotion of healthy lifestyles and weight management among their patients. J. Clin. Outcomes Manag. 2017, 24, 259–266. [Google Scholar]
- Abaraogu, U.O.; Edeonuh, J.C.; Frantz, J. Promoting physical activity and exercise in daily practice: Current practices, barriers, and training needs of physiotherapists in eastern Nigeria. Physiother. Can. 2016, 68, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Patra, L.; Mini, G.K.; Mathews, E.; Thankappan, K.R. Doctors’ self-reported physical activity, their counselling practices and their correlates in urban Trivandrum, South India: Should a full-service doctor be a physically active doctor? Br. J. Sports Med. 2015, 49, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Freene, N.; Cools, S.; Hills, D.; Bissett, B.; Pumpa, K.; Cooper, G. A wake-up call for physical activity promotion in Australia: Results from a survey of Australian nursing and allied health professionals. Aust. Health Rev. 2019, 43, 165–170. [Google Scholar] [CrossRef]
- Hébert, E.T.; Caughy, M.O.; Shuval, K. Primary care providers’ perceptions of physical activity counselling in a clinical setting: A systematic review. Br. J. Sports Med. 2012, 46, 625–631. [Google Scholar] [CrossRef]
- Aveyard, P.; Lewis, A.; Tearne, S.; Hood, K.; Christian-Brown, A.; Adab, P.; Begh, R.; Jolly, K.; Daley, A.; Farley, A. Screening and brief intervention for obesity in primary care: A parallel, two-arm, randomised trial. Lancet 2016, 388, 2492–2500. [Google Scholar] [CrossRef] [Green Version]
- Vuori, I.M.; Lavie, C.J.; Blair, S.N. Physical activity promotion in the health care system. Mayo Clin. Proc. 2013, 88, 1446–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.; Bright, P.; Hansen, L.; Ihnatsenka, O.; Carek, P.J. Promoting Physical Activity in a Primary Care Practice: Overcoming the Barriers. Am. J. Lifestyle Med. 2019, 1559827619867693. [Google Scholar] [CrossRef]
- Bartlem, K.; Bowman, J.; Ross, K.; Freund, M.; Wye, P.; McElwaine, K.; Gillham, K.; Doherty, E.; Wolfenden, L.; Wiggers, J. Mental health clinician attitudes to the provision of preventive care for chronic disease risk behaviours and association with care provision. BMC Psychiatr. 2016, 16, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobelo, F.; Rohm Young, D.; Sallis, R.; Garber, M.D.; Billinger, S.A.; Duperly, J.; Hutber, A.; Pate, R.R.; Thomas, R.J.; Widlansky, M.E. Routine assessment and promotion of physical activity in healthcare settings: A scientific statement from the American Heart Association. Circulation 2018, 137, e495–e522. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.; Littlewood, C.; McLean, S.; Kilner, K. Physiotherapy and physical activity: A cross-sectional survey exploring physical activity promotion, knowledge of physical activity guidelines and the physical activity habits of UK physiotherapists. BMJ Open Sport Exer. Med. 2017, 3, e000290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, E.L.; Ewald, B.D.; Johnson, N.A.; Stacey, F.G.; Brown, W.J.; Holliday, E.G.; Jones, M.; Yang, F.; Hespe, C.; Plotnikoff, R.C. Referral for expert physical activity counseling: A pragmatic RCT. Am. J. Prev. Med. 2017, 53, 490–499. [Google Scholar] [CrossRef]
- Soan, E.J.; Street, S.J.; Brownie, S.M.; Hills, A.P. Exercise physiologists: Essential players in interdisciplinary teams for noncommunicable chronic disease management. J. Multidiscip. Healthc. 2014, 7, 65. [Google Scholar] [CrossRef] [Green Version]
- Cheema, B.S.; Robergs, R.A.; Askew, C.D. Exercise physiologists emerge as allied healthcare professionals in the era of non-communicable disease pandemics: A report from Australia, 2006–2012. Sports Med. 2014, 44, 869–877. [Google Scholar] [CrossRef]
- Craike, M.; Britt, H.; Parker, A.; Harrison, C. General practitioner referrals to exercise physiologists during routine practice: A prospective study. J. Sci. Med. Sport 2018, 21, 21. [Google Scholar] [CrossRef]
- Buchan, J.; O’May, F. The Allied Health Professional Workforce: Evidence and Impact. 2011. Available online: https://pdfs.semanticscholar.org/3df9/e240d296923fd06e708d5bf9fa44e7cebc23.pdf?_ga=2.254911112.1289454358.1592397343-917084308.1591609408 (accessed on 14 June 2020).
- O’Brien, M.W.; Shields, C.A.; Oh, P.I.; Fowles, J.R. Health care provider confidence and exercise prescription practices of Exercise is Medicine Canada workshop attendees. Appl. Physiol. Nutr. Metab. 2017, 42, 384–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author, Study Year & Reference | Country of Study | Study Design | Type of Healthcare Professional(s) (HCPs) | Participants (No., Gender, Mean Age [yrs.]) |
|---|---|---|---|---|
| Spellman et al. 2014 [31] | Australia | Cross sectional study | HCPs (Clinicians i.e., Urologists*; Medical Oncologists*; Radiation Oncologists* and Nurses*) | N = 31; Females (29%, n = 9); Age: (43.5 ± 16.2) |
| Barnes et al. 2019 [51] | Australia | Longitudinal study | GPs | N = 2846; Females (20%, n = 570); Age: (49.8 ± 4.08) |
| Din et al. 2015 [52] | UK | Qualitative study | HCPs (GPs – 67.3%, Nurses – 19.5% & Practice Managers – 13.0%) | N = 46; Females (56.5%, n =26) Age: * |
| Haussmann et al. 2018 [53] | Germany | Qualitative study | HCPs (GPs – 33.3%; Physicians – 33.3% & Nurses – 33.3%) | N = 30; Females (63%, n = 19); Age: (45.0 ± 11.5) |
| Cantwell et al. 2018 [63] | Ireland | Multi-methods (Delphi method) | HCPs (Nurses – 48%; Oncologists – 27%; GPs – 8%; Surgeons – 19.5%: Physiotherapists – 2% & Radiation therapists – 0.5%) | N = 91; Females (67%, n = 61); Age: (44.02 ± 15.6) |
| Eisele et al. 2020 [64] | Germany | Qualitative study | Physiotherapists | N = 9; Females (66.6%, n = 6); Age: (39 ± 12.0) |
| Haussmann et al. 2018 [65] | Germany | Cross Sectional Study | HCPs (GPs – 17.2%; Physicians – 40.5% & Nurses – 42.3%) | N = 917; Females (61.3%, n = 563); Age: (30.2 ± 9.8) |
| Hurkmans et al. 2011 [66] | The Netherlands | Cross Sectional Study | HCPs (Rheumatologists – 34.2%; Nurse – 35.6% & Physical Therapist – 30.2%) | N = 370; Females (66.7%, n = 247); Age: (46 ± 6.0) |
| Jorgensen et al. 2012 [67] | Denmark | Cross Sectional Study | GPs | N = 223; Females (50.7%, n = 113); Age: (53.4 ± 8.0) |
| Leemrijse et al. 2015 [68] | The Netherlands | Cross Sectional Study | GPs | N = 340; Females (41.1%, n = 140); Age* |
| Mulligan et al. 2011 [69] | New Zealand & Sweden | Qualitative study | Physiotherapists | N = 9; Females (88.8%, n = 8); Age** |
| O’Brien et al. 2019 [70] | Ireland | Cross Sectional Study | Physicians | N = 595; Females (56.3%, n = 335); Age: (42.6 ± 12.1) |
| Sassen et al. 2011 [71] | The Netherlands | Cross sectional study | HCPs (Nurses– 40% & Physiotherapists – 60%) | N = 278; Females (73.7%, n = 205); Age: (36.2 ± 10.1) |
| Suija et al. 2010 [72] | Estonia | Cross sectional study | Physicians** | N = 198; All Females; Age: (47.1 ± 9.4) |
| Barrett et al. 2013 [73] | Ireland | Cross-sectional study | GPs and Physiotherapists | N = 431; Females (43.4%, n = 187); Age: * |
| Burton et al. 2010 [74] | Australia | Cross-sectional study | Psychologists | N = 236; Females (84.7%, n = 200); Age: (42.12 ± 11.03) |
| Frantz & Ngambare 2013 [75] | Rwanda | Mixed Methods | Physiotherapists | N = 92; Females (30%, n = 28); Age: (32.49 ± 6.56) |
| Freene et al. 2017 [76] | Australia | Cross Sectional Study | Physiotherapists | N = 257; Females (77.8%, n = 200); Age: (43.2 ± 15.4) |
| Patel et al. 2012 [77] | New Zealand | Qualitative study | GPs | N = 15; Females (66.6%, n = 10); Age: (50.8 ± 7.1) |
| Patel et al. 2011 [78] | New Zealand | Qualitative study | GPs | N = 15; Females (66.6%, n = 10); Age: (50.8 ± 7.1) |
| Shirley et al. 2010 [79] | Australia | Cross sectional study | Physical Therapy practitioners | N = 318; Females (73%, n = 233); Age: (41.8 ± 9.4) |
| Speake et al. 2019 [80] | Australia | Qualitative study | HCPs (Clinical specialists in pain management*; Occupational therapists*; Nurses* (Continence and diabetes), Consultants in diabetes* and Orthopaedics*; Specialist diabetes dieticians*; Physiotherapists* (continence and MSK), specialist and advanced* Podiatrists) | N = 22; Females (68.1%, n = 15); Age* |
| Kinnafick et al. 2018 [81] | UK | Qualitative study | Healthcare Assistants | N = 11; Females (54.5%, n = 6); Age: (30.27 ± 7.75) |
| Litchfield et al. 2019 [82] | UK | Qualitative study | HCPs (Dietitians – 33.3%; Specialist physicians – 16.6%; Nurses – 50%) | N = 6; Females*; Age* |
| Lowe et al. 2018 [83] | UK | Qualitative study | Physiotherapists | N = 12; Females (58%, n = 7); Age* |
| Williams et al. 2018 [84] | UK | Qualitative | Physiotherapists | N = 18; Females (72.2%, n = 13); Age** |
| Courtney-Long et al. 2017 [85] | USA | Cross-sectional study | HCPs (Family/GPs – 44.1%; Internists – 37.1% & Nurse practitioners – 18.9%) | N = 1760; Females (38.5%, n = 678); Age: (59.9 ± 5.7) |
| Omura et al. 2018 [86] | USA | Cross Sectional Study | HCPs (Physicians – 57.1%; Paediatricians – 14.2%; Obstetrician & Gynaecologists – 14.2% & Nurses – 14.3%) | N = 1751; Females (14.5%, n = 254); Age: (51.5 ± 11.5) |
| Pearson et al. 2018 [87] | USA | Cross sectional study | Nurses | N = 111; Females (78.3%, n = 87); Age: (36.8 ± 11.9) |
| Pojednic et al. 2017 [88] | USA | Cross sectional study | Sport Medicine Physicians | N = 412; Females (47%, n = 194); Age: (47.1 ± 2) |
| Tucker et al. 2017 [89] | USA | Cross sectional study | Physicians** | N = 25; Females (64%, n = 16); Age** |
| Abaraogu et al. 2016 [90] | Nigeria | Cross-sectional study | Physiotherapists | N = 103; Females (30%, n = 31); Age: (34.5 ± 9.5) |
| Patra et al. 2015 [91] | India | Cross sectional study | HCPs (GPs– 32.8% & Physicians – 67.2%) | N = 146; Females (41%, n = 60); Age: (43 ± 11.3) |
| Freene et al. 2019 [92] | Australia | Cross Sectional Study | HCPs (Physiotherapists – 59%; Nurses – 16%; Exercise Physiologists – 13%; Occupational therapists – 6%; Dietitians – 3% & Pharmacists – 2%) | N = 433; Females (79%, n = 340); Age: (41.7 ± 15.3) |
| Author, Study year & Reference | Knowledge of PA | Confidence in Promoting PA | Importance of PA and its Promotion | Role in PA Promotion | PA Assessment | How PA was Promoted | Perceived Effectiveness of PA Promotion |
|---|---|---|---|---|---|---|---|
| Spellman et al. 2014 [31] | 83.9% (n=26; M=4.2, SD=0.76) of the HCPs agreed or strongly agreed that they were confident in providing general advice about physical activity to prostate cancer survivors | Almost all the HCPs (n=29, 93.6%; mean (M)=4.52, standard deviation (SD)=0.51) strongly agreed or agreed that regular physical activity can improve cancer patients’ quality of life | On who’s role to recommend PA, over 50% of HCPs (n=16) nominated a Physiotherapist; followed by a Urology Nurse (n=14, 46.7%) and an Exercise Specialist (n=14, 46.7%) | NA | On recommended PA, 3.2% (n=1) of HCPs always gave advice; 36% (n=11) often gave advice, 45.2% (n=14) sometimes gave advice and 16% (n=5) rarely gave advice, 80.8% (n=25) recommended cardiovascular PA followed by weights training. On how PA was recommended; all participants (n=31) gave advice verbally and 9.7% (n=3) provided pamphlets to their patients. No participant reported the referral of patients to an exercise specialist | NA | |
| Barnes et al. 2019 [51] | NA | GPs provided Physical Activity Management (PAM) for 58, (2.0%) prostate cancer survivors. The PAM provided was physical activity counselling on 39 and a physical activity referral on 19 occasions. | NA | ||||
| Din et al. 2015 [52] | NA | Most HCPs acknowledged the importance of promoting physical activity in order to improve public health | HCPs commonly saw their role as giving advice when asked for, rather than ‘coercing’ patients into changing their behavior | HCP’s selectively provided PA advice to patients. The advice was targeted at individuals they felt would be motivated to change. Such judgements were sometimes based on patients’ physical appearance, conditions, age and/or gender | |||
| Haussmann et al. 2018 [53] | HCPs expressed their wish for more PA related information for themselves and their patients with cancer | NA | The perceived patient characteristics influencing HCPs impression for PA assessment were patients’ physical condition (n = 16), patients’ assumed interest in PA (n = 11) and patients’ former PA lifestyle (n = 10). | NA | |||
| Cantwell et al. 2018 [63] | NA | Over 86% of HCPs agreed or strongly agreed that PA has so many health benefits and can improve quality of life | Almost 88% of HCPs either agreed or strongly agreed that discussing physical activity with cancer patients was part of their role | NA | PA was frequently recommended to myriads of cancer patients depending on the stage of cancer. PA promotion was given verbally or by a referral to a physiotherapist or exercise specialist (40%) or referral to a community-based programme (28%) | NA | |
| Eisele et al. 2020 [64] | NA | Physiotherapists indicated that they felt responsible to instruct PA. Some also regarded it as their role to advice and motivate patients on routine PA implementation | Some physiotherapists design home-based PA for their clients (goal setting behavior). Client’s choice of activities is considered by some physiotherapists while others do not | ||||
| Haussmann et al. 2018 [65] | 69.5% of all HCPs requested at least one offered PA information resource. 53.5% requested a booklet, scientific paper by 53.0%, and educational course by 27.6%. | NA | PA was recommended often or routinely in 88.5% of physicians working in outpatient care, 78.1% of physicians working in inpatient care, and 73.1% of oncology nurses. Three HCPs (indicated that they advised against doing PA | NA | |||
| Hurkmans et al. 2011 [66] | 54% (n = 68) of Rheumatologists indicated that they were interested in additional education on the promotion of PA compared to Clinical Nurse specialists (n = 112, 85%) and Physical therapists (n=81, 72%) (both p < 0.001) | NA | Majority of Rheumatologists (n=118, 94%), Clinical Nurse specialists (n=132, 100%), and Physical therapists (n = 109, 100%) agreed that obtaining and/or maintaining a sufficient level of PA is an important health goal in the management of patients with rheumatoid arthritis | NA | 86% (n = 107) of Rheumatologists gave advice on PA, 95% of Clinical Nurse specialists (122) and 99% of Physical therapists (n = 109). More Clinical Nurse specialists (n = 52, 41%) and Physical therapists (n = 54, 49%), use the public health recommendation on moderate-intensity PA for patients’ advice | ||
| Jorgensen et al. 2012 [67] | NA | 80.2% of GPs reported that promoting PA was one of their work tasks while 19.8% (43/217) did not perceive it as their job or were in doubt | NA | 57% of GPs promoted PA daily, 38.6% weekly and 4.5% monthly or seldomly. In about 60% of cases GPs gave PA advice with recommended exercise type, duration, frequency, and intensity and in 40% of cases PA promotion included written material | |||
| Leemrijse et al. 2015 [68] | NA | Half of the GPs thought that they had an important role in stimulating physical activity, while the other half considered their role present but ‘limited | NA | All GPs said they recommend PA to their patients. This was given when PA was relevant for the patients’ health problem or health status. About 70% of GPs referred patients for PA interventions | NA | ||
| Mulligan et al. 2011 [69] | Physiotherapists have developed knowledge on and were aware of and supported current national health policies toward PA enhancement | NA | Physiotherapists perceived that they had moved away from what they considered traditional physiotherapy practice and now practiced with a wider scope. | NA | Educational seminars provided opportunities for people with neurological conditions to support and learn from one another while building efficacy and acquiring strategies to take responsibility for their own future health and well-being | ||
| O’Brien et al. 2019 [70] | 64.1% of physicians indicated the correct weekly levels of PA recommended by the National PA Guidelines for Ireland. 29% of participants accumulated 4 h of PA promotion training. | Confidence was identified by physicians as an important factor in undertaking PA counselling activities, with a significant association between confidence and PA enquiry and counselling activities observed | NA | 88.0% of physicians enquired about PA levels and 86.2% provided verbal PA counselling to at least some of their patients. The majority of participants reported that they did not provide either written advice (82.6%) or PA prescriptions (89.3%) | |||
| Sassen et al. 2011 [71] | NA | 56.8% of the HCPs encourage PA among cardiovascular patients. | |||||
| Suija et al. 2010 [72] | NA | Physicians claimed that they counsel over 94% of their patients about physical activity | |||||
| Barrett et al. 2013 [73] | Below 1/3 of GPs and 1/2 of PTs reported the correct PA guidelines. More PTs compared to GPs significantly recalled the PA guidelines (PTs - 50.5%, n = 45; GPs – 28%, n = 97; p < 0.005; χ2 = 16.56; df = 1) while 58% (n = 197) of GPs and 37% (n = 33) of PTs were unsure about the frequency of PA. | Seventy two percent (72%, n =247) and 92% (n = 82) of PTs noted that they were confident in providing PA advice to their patients | NA | Ninety five percent (95%) of both GPs (325) and PTs (85) perceived PA promotion to be part of their role | About 41%, (n = 139) of GPs reported opportunistic screening of patients, 37% (n =126) screened patients for PA if relevant to patients’ presentations and 8% (n = 28) routinely screened all their patients for PA. For PTs, 34% (n = 30) screened all patients for PA, 28% (n = 25) screened patients if related to presentations and 24% (n = 21) reported opportunistic screening | Education and advice (GPs = 76%, n = 258 and PTs 97%, n = 86); referrals to other services by GPs (practice nurse = 16%, n = 56; exercise specialist = 14%; n = 49; exercise prescription schemes = 11%; n = 37, gyms = 44%; n = 150). PTs utilised written materials (73%; n = 65), exercise diaries (57%; n = 51), follow up appointments (53%; n = 47) and behavioural modification (GP = 50%, n = 172; PT = 53%, n =47) | NA |
| Burton et al. 2010 [74] | 12% (n=29) of psychologists said they had received PA advice or counselling instructions during undergraduate, 31% (n=61) during postgraduate training and 18% (n = 41) during a workshop/seminar | Over 80% of psychologists were confident to provide general activity advice, discuss options, identify and manage barriers to activity | 12% of psychologists (n = 29) strongly agreed/agreed that PA was important for preventing chronic health problems | NA | 61% (n = 142) of psychologists reported always asking about PA in the past month | 59% of psychologists (n = 139) always discussed PA, 53% (n=22) recommended PA, 33% (n = 77) always gave PA advice | 93% (n = 220) of psychologists strongly agreed/agreed that PA advice and counselling could be a useful component of psychological treatment |
| Frantz & Ngambare 2013 [75] | NA | PA counselling was the predominant health promotions strategy used by physiotherapists (98%) while 9% used written materials. | |||||
| Freene et al. 2017 [76] | On general knowledge regarding PA, physiotherapists recommended the following: taking the stairs by 54%; 30 min walk on most days by 43%; exercise that makes you puff and pant by 32%; several 10 min shot walks on most days by 78% | 95.3% of physiotherapists indicated that they would feel confident in giving general PA advice to patients while 93% of participants indicated that they would feel confident in suggesting specific PA | Over 97% of physiotherapists indicated that some parts of their role to patients are: discussing the benefits of PA, suggesting ways to improve PA and also acting as PA role model | 93.8% of physiotherapists practiced brief PA during consultations with patients, separate one-on-one consultations was practiced by 52.5% of participants, group sessions by 67.3% and distribution of resources (such as brochures) by 93.4% of physiotherapists | |||
| Patel et al. 2012 [77] | NA | ||||||
| Patel et al. 2011 [78] | NA | GPs perceived Green Prescription to be a beneficial PA tool for drug-free therapeutic processes and health gain, endorsed by them and presented in the same format as prescription medication | NA | ||||
| Shirley et al. 2010 [79] | Only one third of the respondents could name the national physical activity recommendation for Australian adults | Physical therapists who gave more patients physical activity advice were more likely to feel confident in suggesting specific physical activity programmes | NA | In both groups, almost all physical therapists thought it should be part of their role to give their patients physical activity advice | NA | Above half of the physical therapists (54%) reported that they encouraged 10 or more patients each month to lead a more physically active lifestyle | |
| Speake et al. 2019 [80] | NA | HCPs found it challenging to give advice that reflected individual differences. In particular they perceived a need for lower entry points to PA interventions that might be more palatable for their most inactive patients | There was a lack of consensus about roles and responsibilities for promoting PA. HCPs indicated that their primary role was to focus on their patient’s physical health and the specialty of their training. Bringing PA into consultation, had to be linked to the health condition | NA | |||
| Kinnafick et al. 2018 [81] | NA | All health care assistants agreed that exercise was beneficial for patients’ physical and mental health | health care assistants agreed that PA promotion was part of their role, but the extent to which they should encourage PA was unclear to them | NA | |||
| Litchfield et al. 2019 [82] | NA | Dietitians were comfortable presenting advice to individuals who consistently indulge in PA like running or cycling. The standard at which Dietitians exercised or played sport informs the confidence in promoting PA | NA | HCPs promoted PA based on their personal experiences of a particular sport or activity | |||
| Lowe et al. 2018 [83] | NA | Physiotherapists role in educating patients on PA came through strongly as a means of supporting self-management | Physiotherapists integrated PA questions into the subjective assessment and specifically into the social history of their patient | Physiotherapists promoted PA by providing brief advice, brief intervention, cognitive behavioral therapy, and motivational interviewing to their clients | |||
| Williams et al. 2018 [84] | PA knowledge was gained through the practical experience of caring for people with Spinal Cord Injuries (SCI) over time. Participants revealed that: they were not educated on PA during their degree course and had a limited range of other sources of PA knowledge. The value of PA was learnt through seeing the perceived detrimental effects of physical inactivity. | NA | Physiotherapists recognized the value that PA played both in Spinal Cord Injury (SCI) rehabilitation and upon discharge to the community. They drew upon PA in rehabilitation to improve balance, flexibility, strength, and cardiovascular fitness with the aim to improve function and independence | One reason why most of the Physiotherapists failed to promote PA was because it was deemed not to be part of their role | NA | Physiotherapists promoted PA for SCI rehabilitation by providing structured gym sessions and group exercises and recreational sport activities organized by other health professionals | NA |
| Courtney-Long et al. 2017 [85] | 53.7% of HCPs knew the guideline on aerobic activity applied to adults with disabilities with the percentage been highest among those who strongly agreed they felt prepared (62.0%) | NA | About 79% of HCPs or somewhat agreed they felt prepared to recommend physical activity to their patients with disabilities | About 50.6% of HCPs reported recommending PA to patients with disabilities at most clinic visits | |||
| Omura et al. 2018 [86] | NA | Discussing PA with at-risk patients was higher among non-Hispanic HCPs compared to others. | 92% of HCPs who encouraged their clients to increased PA used counselling, 78.7% by assessing PA levels, 41.5% provided educational materials, 25.6% by written exercise prescription and 15.1% referred patients for PA interventions. | ||||
| Pearson et al. 2018 [87] | In the perceived behavioral control category, high mean scores were noted regarding knowledge, skills and intention to promote PA | The item with the highest mean score (i.e., most agreement with the statement) was PA increases activity tolerance. Mean attitude scores were lowest related to PA causes harm | Mean scores were noted to be highest in the subjective norm category in regard to promotion of PA being a priority of nursing and that engaging patients in PA is the responsibility of RNs. | NA | |||
| Pojednic et al. 2017 [88] | Physicians were most familiar with four activities: walking, aerobic activity, strength training and cycling. 37% of physicians used Exercise is Medicine resources, 19% used tools created individually by clinicians drawn from the internet, books, or elsewhere, and 12% used American Heart Association resources | NA | 49% of physicians included PA assessment as a vital sign. | About 74% of physicians recommended and talked about PA 26% provided a written PA prescription. Physicians who provided a written PA prescription reported seeing more improvement in their patients’ physical activity levels | NA | ||
| Tucker et al. 2017 [89] | NA | Physicians expressed confidence in their ability to counsel their patients to engage in adequate amounts of PA (68% strongly agreed, 24% somewhat agreed) | Approximately 88% of the Physicians agreed that patients were more likely to adopt healthier lifestyles if their healthcare providers counselled them to do so (44% strongly agreed, 44% agreed somewhat) | 88% of Physicians strongly agreed that it was their responsibility to promote a PA, weight loss and healthy weight maintenance among their patients | NA | Most Physicians at least somewhat agreed that they were effective in encouraging patients to engage in health-promoting PA (44% strongly agreed, and 44% somewhat agreed) | |
| Abaraogu et al. 2016 [90] | NA | Over 90% (n = 93) of physiotherapists rated themselves confident in assessing physical inactivity | Counselling patients on PA was considered very important by 87%; (n = 90) of physiotherapists | Addressing physical inactivity was considered high priority and a normal clinical role by 82% (n = 84) of physiotherapists | 56%; (n = 58) of physiotherapists ‘‘always’’ or ‘‘usually’’ assess their client’s PA profile | PA was promoted by providing advice; written materials; referral; and managing risk factors. Over 78% regularly advised clients on PA while about 24% gave written PA advice | 66% (n = 68) of physiotherapists believed that their counselling is effective |
| Patra et al. 2015 [91] | 24.7% of HCPs reported that they had attended classes on PA in medical college and 26% received formal training for PA counselling | NA | 81% of HCPs perceived PA to be important. 52% perceived PA to be beneficial in depression, 22.6% in chronic respiratory disease and 19.8% in cancers | 78% of HCPs agreed that PA has a role in primary, 91% in secondary prevention of chronic diseases and a beneficial role in the prevention of heart diseases, obesity and diabetes | 42.5% HCPs reported that they always ‘asked’ their patients about their current PA levels | 46.6% HCPs always gave ‘verbal advice’. 25.3% always asked and advised’ their patients regarding PA. | NA |
| Freene et al. 2019 [92] | All HCPs felt they had the skills to promote PA | PTs and EPs were more confident giving general (p < 0.001) and specific (p < 0.001) PA advice to patients | NA | All HCPs agreed that providing PA advice was part of their role, although nurses were less likely to agree | NA | Brief counselling (n = 392, 91%) and giving out brochures (n = 404, 93%) were reported to be the most feasible methods for PA promotion by HCPs | |
| TDF Domains | Rank (B - Barrier and F-Facilitator) | Barrier Constructs & Reference Numbers | Facilitator Constructs & Reference Numbers |
|---|---|---|---|
| TDF domain 1: knowledge (This is the recognition that something exists) | B2; F3 | Lack of knowledge or training on PA: [64,70,76,81,82,85,86,90,92] | Providing education to HCP’s and patients about the benefits of PA and available promotional programmes: [63] |
| Lack of knowledge of PA & promotional pathways: [63,67,70,71,73,80,84,86,88] | Assessable resources on PA promotional programmes (e.g., smart phone apps, assessment tools etc): [63,68,83,89] | ||
| TDF domain 2: skill (This is talent acquired by repeated practice) | B5; F5 | Lack of knowledge or training on PA: [64,70,76,81,82,85,86,90,92] | Providing supportive and individualized PA programmes: [52] |
| Lack of motivational skills to encourage participants: [64] | |||
| TDF domain 3: social/professional role and identify (This is the logical sequence of character exhibited by a person) | B10; F3 | Perception of limited role in PA promotion: [84] | Professional collaboration among HCPs: [68,83] |
| Lack of cooperation among HCP’s: [69,83] | HCPs physical active lifestyles: [52] | ||
| TDF domain 4: beliefs about capabilities (This is the honest and rational acceptance of a particular talent or expertise that can be useful to an individual) | B10; F(Non) | Language barrier: [64] | Not indicated |
| Lack of motivational skills to encourage participants: [64] | |||
| Lack of confidence in promoting PA: [77] | |||
| TDF domain 5: optimism (This is the conviction that an event will occur, or an expected aim will be achieved) | B6; F(Non) | Perceived feeling that PA advice will not convince patient to change behavior: [76,86,92] | Not indicated |
| Perceived feeling that PA will not be beneficial for patient: [76,81,84,86,92] | |||
| TDF domain 6: beliefs about consequences (This is the act of embracing the honest and rational result of a particular conduct in a certain circumstance) | B3; F(Non) | Perceived fear of liability and litigation: [52,71,86] | Not indicated |
| Perceiving investments in PA promotion to be a misuse of government funds: [52] | |||
| Perceived feeling that PA advice will not convince patient to change behavior: [76,86,92] | |||
| Perceived feeling that PA will not be beneficial for patient: [76,81,84,86,92] | |||
| Perception that PA could be counter-productive: [53,77] | |||
| TDF domain 7: Reinforcements (This is an enhancement of the likelihood of reaction by organizing a conditioner connection between the reaction and the stimulus) | B8; F1 | Lack of remuneration or incentives: [65,76,84,85,88,92] | Reported beneficial outcomes of PA: [63,68] |
| Repeat appointments with patients: [83] | |||
| Feedback to HCPs on patient’s progress in a programme: [63] | |||
| Affordability of PA and referral pathways services: [68] | |||
| Positive feedback from other patients on PA referral: [52,64] | |||
| Financial incentives to patients: [52] | |||
| TDF domain 8: Intentions (This is the deliberate resolve to perform an act in a particular manner) | B7; F5 | Patient’s comorbidities or other immediate health issues: [83,85] | Self-motivation and interest by patient to participate in PA: [64] |
| Patient’s reduced health status: [68] | |||
| Prioritizing other interventions: [83] | |||
| Feeling uncomfortable/inappropriate to speak to patient about PA: [85] | |||
| Not interested in promoting PA: [76,92] | |||
| TDF domain 9: Goals (This is the intellectual depiction of results that one desires to attain) | B12; F5 | Patient’s comorbidities or other immediate health issues: [83,85] | Pre-existing indication for PA intervention: [78] |
| TDF domain 10: Memory, Attention, Decision process (This is the capacity to keep details, critically concentrate on different parts of the environment and select between different options) | B13; F5 | Prioritizing other interventions: [83] | Self-motivation and interest by patient to participate in PA: [64] |
| TDF domain 11: Environmental Context and Resources (This is an individual’s conditions that enables or prevents the development of expertise, social capabilities, and modifiable habits) | B1; F2 | Lack of PA resources (e.g., education leaflets and materials): [31,63,70,73,82,88,89,90] | Assessable resources on PA promotional programmes (e.g., smart phone apps, assessment tools, etc.): [63,68,83,89] |
| Inadequate staffing: [81] | Formal and central process for PA intervention: [71] | ||
| Inaccessible PA supportive environment: [69,84] | Promotion of active treatment, home services and sporting activities: [64] | ||
| Inadequate or lack of PA support services: [69,84] | |||
| Lack of specific PA guidelines: [65] | |||
| Limited counselling time: [31,52,53,63,65,67,71,73,76,78,80,82,86,88,89,90,92] | |||
| Lack of PA infrastructure and funding: [75] | |||
| Poor implementation and inconsistent support: [75] | |||
| Lack of PA facilities and funding: [64,75,84] | |||
| Paucity of PA specialist: [52,65,73,82] | |||
| Patient safeguarding procedures (i.e., for patient with mental health challenges): [81] | |||
| Long awaiting list to asses PA services: [69] | |||
| Transportation barrier: [77] | |||
| Lack of referral pathways for promotion: [52,67,86] | |||
| TDF domain 12: Social influence (They are relational procedures that can influence the thinking and behavioral processes of a person) | B3; F4 | Lack of support from practice or other colleagues: [82] | Encouraging informal communication strategies (e.g., building rapport, providing information, social support and understanding patient needs): [81] |
| Lack of patient interest or motivation in PA: [31,64,67,68,69,73,80,85,89] | Opportunities for empathy and connection among HCPs and patients: [83] | ||
| Patient preference for other intervention (e.g., drugs): [70] | |||
| Lack of cooperation among HCP’s: [69,83] | |||
| TDF domain 13: Emotion (This is a complicated pattern of reaction, including practical, psychological and biological components which a person tries to use in the management of a crucial issue) | B9; F5 | Feeling uncomfortable/inappropriate to speak to patient about PA: [82] | Opportunities for empathy and connection among HCPs and patients: [83] |
| Perceived fear of liability and litigation: [52,71,86] | |||
| TDF domain 14: Behavioural Regulation (This is anything intended for controlling or modifying a neutral event or measures) | B13; F5 | Cultural restriction: [75] | Compulsory PA interventions to patients: [81] |
| QATSDD Criteria | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author & Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | Total Score | Max Score (%) |
| Spellman et al. 2014 [31] | 0 | 3 | 1 | 0 | 1 | 1 | 2 | 2 | 0 | 2 | NA | 2 | 1 | NA | 0 | 3 | 18/42 | 43 |
| Barnes et al. 2019 [51] | 0 | 3 | 3 | 2 | 3 | 3 | 0 | 2 | 0 | 3 | NA | 0 | 0 | NA | 0 | 2 | 21/42 | 50 |
| Din et al. 2015 [52] | 0 | 2 | 3 | 2 | 2 | 2 | 1 | 2 | NA | NA | 3 | 3 | 3 | 2 | 0 | 3 | 28/42 | 66.7 |
| Haussmann et al. 2018 [53] | 0 | 3 | 2 | 1 | 2 | 2 | 1 | 1 | NA | NA | 2 | 3 | 2 | 2 | 1 | 2 | 24/42 | 57.1 |
| Cantwell et al. 2018 [63] | 0 | 3 | 3 | 1 | 2 | 3 | 2 | 3 | 1 | 3 | 2 | 3 | 2 | 1 | 1 | 3 | 33/48 | 68.8 |
| Eisele et al. 2020 [64] | 0 | 3 | 3 | 2 | 3 | 3 | 2 | 2 | NA | NA | 2 | 3 | 3 | 2 | 3 | 3 | 34/42 | 81.0 |
| Haussmann et al. 2018 [65] | 0 | 3 | 2 | 1 | 3 | 3 | 2 | 3 | 0 | 2 | NA | 2 | 3 | NA | 2 | 3 | 29/42 | 69 |
| Hurkmans et al. 2011 [66] | 0 | 3 | 2 | 2 | 3 | 2 | 1 | 2 | 0 | 0 | NA | 2 | 3 | NA | 2 | 3 | 25/42 | 59.5 |
| Jorgensen et al. 2012 [67] | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 1 | 2 | 2 | NA | 2 | 3 | NA | 2 | 3 | 24/42 | 57.1 |
| Leemrijse et al. 2015 [68] | 0 | 3 | 1 | 0 | 3 | 1 | 1 | 1 | 0 | 1 | NA | 1 | 0 | NA | 0 | 3 | 15/42 | 35.7 |
| Mulligan et al. 2011 [69] | 0 | 3 | 2 | 1 | 2 | 3 | 2 | 2 | NA | NA | 1 | 2 | 3 | 2 | 0 | 3 | 26/42 | 59 |
| O’Brien et al. 2019 [70] | 0 | 3 | 2 | 3 | 3 | 3 | 2 | 3 | 3 | 2 | NA | 3 | 2 | NA | 3 | 3 | 35/42 | 83.3 |
| Sassen et al. 2011 [71] | 3 | 3 | 2 | 1 | 3 | 3 | 1 | 2 | 0 | 2 | NA | 2 | 2 | NA | 1 | 2 | 26/42 | 62 |
| Suija et al. 2010 [72] | 0 | 0 | 3 | 1 | 2 | 2 | 1 | 3 | 1 | 2 | NA | 0 | 2 | NA | 0 | 3 | 20/42 | 47.6 |
| Barrett et al. 2013 [73] | 0 | 3 | 3 | 2 | 3 | 3 | 1 | 3 | 0 | 2 | NA | 2 | 0 | NA | 1 | 0 | 23/42 | 54.8 |
| Burton et al. 2010 [74] | 0 | 3 | 2 | 0 | 3 | 3 | 2 | 3 | 0 | 2 | NA | 2 | 3 | NA | 2 | 3 | 28/42 | 66.7 |
| Frantz & Ngambare 2013 [75] | 0 | 2 | 2 | 1 | 3 | 3 | 3 | 2 | 1 | 3 | 3 | 2 | 1 | 0 | 0 | 0 | 26/48 | 54.1 |
| Freene et al. 2017 [76] | 0 | 3 | 3 | 3 | 2 | 2 | 2 | 2 | 0 | 3 | NA | 3 | 3 | NA | 0 | 2 | 28/42 | 66.7 |
| Patel et al. 2012 [77] | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | NA | NA | 3 | 3 | 2 | 3 | 0 | 3 | 34/42 | 81.0 |
| Patel et al. 2011 [78] | 0 | 2 | 3 | 2 | 3 | 3 | 3 | 2 | NA | NA | 2 | 2 | 2 | 2 | 0 | 3 | 29/42 | 69 |
| Shirley et al. 2010 [79] | 0 | 3 | 1 | 1 | 3 | 2 | 2 | 2 | 0 | 2 | NA | 2 | 2 | NA | 0 | 3 | 23/42 | 54.8 |
| Speake et al. 2019 [80] | 0 | 3 | 2 | 3 | 3 | 3 | 3 | 2 | NA | NA | 2 | 3 | 3 | 3 | 2 | 3 | 35/42 | 83.3 |
| Kinnafick et al. 2018 [81] | 0 | 2 | 2 | 1 | 2 | 3 | 2 | 2 | NA | NA | 2 | 2 | 2 | 2 | 0 | 3 | 25/42 | 59.5 |
| Litchfield et al. 2019 [82] | 0 | 1 | 3 | 1 | 2 | 2 | 2 | 3 | NA | NA | 2 | 1 | 1 | 1 | 0 | 3 | 22/42 | 52.3 |
| Lowe et al. 2018 [83] | 3 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | NA | NA | 3 | 3 | 3 | 2 | 0 | 3 | 34/42 | 81.0 |
| Williams et al. 2018 [84] | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | NA | NA | 3 | 3 | 2 | 3 | 0 | 2 | 35/42 | 83.3 |
| Courtney-Long et al. 2017 [85] | 0 | 3 | 2 | 0 | 2 | 3 | 1 | 2 | 0 | 1 | NA | 2 | 3 | NA | 0 | 2 | 21/42 | 50 |
| Omura et al. 2018 [86] | 0 | 3 | 2 | 1 | 2 | 3 | 2 | 3 | 0 | 3 | NA | 3 | 3 | NA | 0 | 3 | 28/42 | 66.7 |
| Pearson et al. 2018 [87] | 2 | 3 | 3 | 1 | 1 | 3 | 2 | 2 | 0 | 2 | NA | 3 | 2 | NA | 0 | 2 | 26/42 | 62 |
| Pojednic et al. 2017 [88] | 0 | 3 | 2 | 1 | 1 | 3 | 1 | 2 | 0 | 3 | NA | 2 | 0 | NA | 0 | 3 | 21/42 | 50 |
| Tucker et al. 2017 [89] | 0 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 0 | 2 | NA | 2 | 1 | NA | 0 | 2 | 19/42 | 45.2 |
| Abaraogu et al. 2016 [90] | 0 | 3 | 3 | 1 | 3 | 3 | 2 | 2 | 3 | 2 | NA | 2 | 1 | NA | 2 | 1 | 28/42 | 66.7 |
| Patra et al. 2015 [91] | 0 | 1 | 3 | 1 | 3 | 1 | 1 | 2 | 0 | 2 | NA | 2 | 2 | NA | 0 | 2 | 20/42 | 47.6 |
| Freene et al. 2019 [92] | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 1 | NA | 3 | 3 | NA | 0 | 2 | 22/42 | 52.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albert, F.A.; Crowe, M.J.; Malau-Aduli, A.E.O.; Malau-Aduli, B.S. Physical Activity Promotion: A Systematic Review of The Perceptions of Healthcare Professionals. Int. J. Environ. Res. Public Health 2020, 17, 4358. https://doi.org/10.3390/ijerph17124358
Albert FA, Crowe MJ, Malau-Aduli AEO, Malau-Aduli BS. Physical Activity Promotion: A Systematic Review of The Perceptions of Healthcare Professionals. International Journal of Environmental Research and Public Health. 2020; 17(12):4358. https://doi.org/10.3390/ijerph17124358
Chicago/Turabian StyleAlbert, Francis A., Melissa J. Crowe, Aduli E. O. Malau-Aduli, and Bunmi S. Malau-Aduli. 2020. "Physical Activity Promotion: A Systematic Review of The Perceptions of Healthcare Professionals" International Journal of Environmental Research and Public Health 17, no. 12: 4358. https://doi.org/10.3390/ijerph17124358