1. Introduction
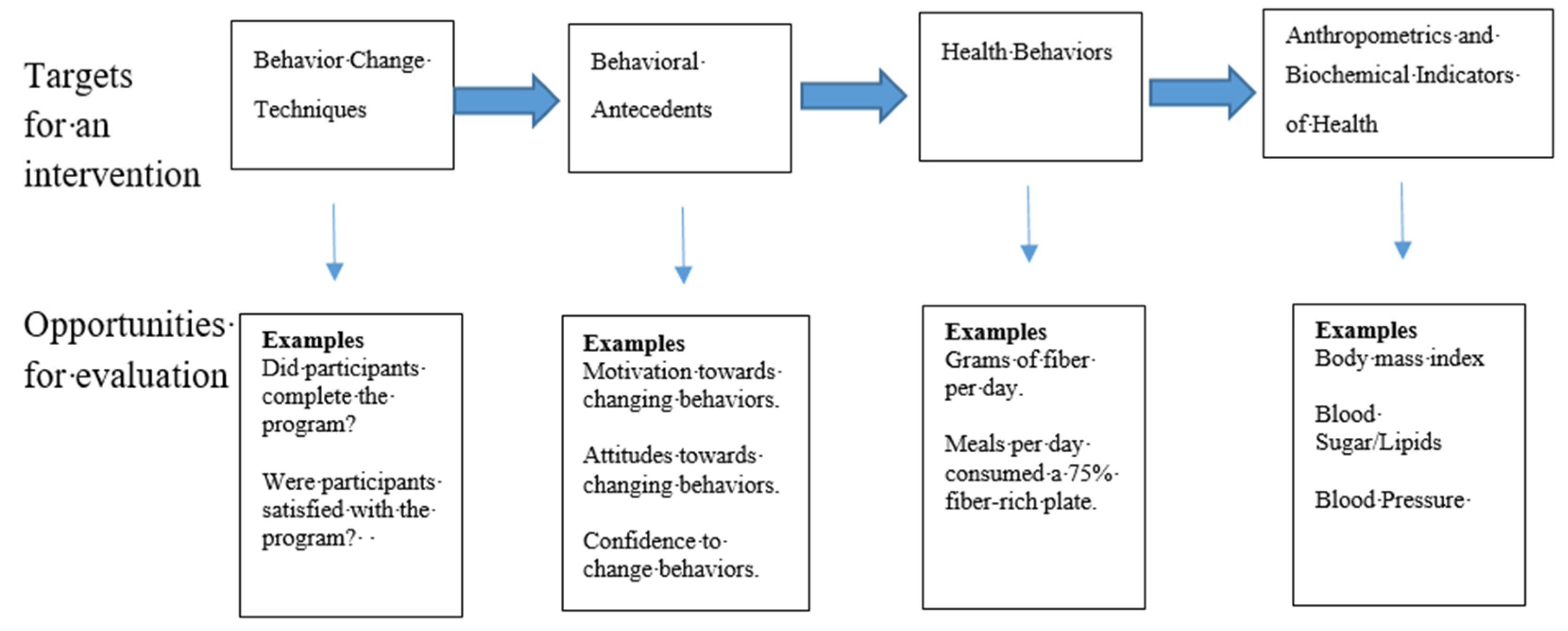
Evaluating behavior change programs in public health, health education and health promotion is a critical step in program development and refinement. A proper evaluation can help determine whether program objectives are met, provide accountability to funders, the community, and other stakeholders, and can help contribute to the scientific basis for behavior change interventions. The logic of a behavior change program is depicted in
Figure 1, which shows a behavior change program (containing behavior change techniques) is implemented to change behavioral antecedents (e.g., motivation/intentions, attitudes, behavioral confidence, skills, knowledge), which in turn, is done to change health behaviors (e.g., fiber consumption), which ultimately leads to changes in anthropometric and biochemical indicators of health (e.g., BMI, blood pressure, blood sugar).
Obesity is one of the most serious public health concerns. Currently, 39% of men and women are obese worldwide, and in the past 20 years in the United States, obesity increased from 30.5% to 42.4% among adults [
1,
2]. Alarmingly, the prevalence of severe obesity almost doubled during the same time, from 4.7% to 9.2% [
1]. Obesity is associated with a number of metabolic, and mental health risks. Metabolic consequences of obesity include having a higher risk of heart disease, certain types of cancers, stroke, and type 2 diabetes [
1]. Obesity among adults has also been associated with having a higher risk of depression and anxiety, and higher discrimination rates in the healthcare setting among numerous health care workers [
3,
4,
5,
6].
Consuming a high fiber diet is among the top modifiable risk factors oftentimes promoted to reduce and prevent obesity [
7,
8]. Fiber has long been promoted for its effect on laxation and having a healthy bowel, but new evidence points to the benefits fiber intake has on preventing and treating chronic diseases, such as type 2 diabetes, cardiovascular disease, and certain types of cancer [
9]. Consuming a high fiber diet is also associated with having a lower body weight, and facilitating weight loss [
9,
10]. For example, in one study with African American women enrolled in a weight loss intervention, while fiber intake was not associated with weight status at baseline, fiber consumption had a strong inverse association with weight status during the 6 and 18 month check in periods of the intervention [
11].
In recent years, researchers have evaluated theory-based behavioral determinants of a number of fiber-rich foods, in order to understand what factors contribute to behavior change. For example, in a study using the Theory of Planned Behavior as a framework for predicting fruit and vegetable consumption, researchers found that all of the theory’s constructs (e.g., intentions and attitudes) were significant predictors, accounting for 42% of the variance of the behavior [
12]. Additionally, in a separate study, researchers again used the Theory of Planned Behavior as a framework with older adults, and reported which specific beliefs led to the development of attitudes, norms and perceived behavioral control pertaining to fruit and vegetable consumption [
13]. Besides fruit and vegetable consumption, whole-grain intake has also been evaluated using similar theory-based approaches [
14,
15]. However, while individual components of consuming a high fiber diet have been previously evaluated, theory-based determinants of consuming a high-fiber diet as a whole have not been well established. Therefore, the purpose of this study was to develop and validate an instrument to evaluate theory-based behavioral antecedents of consuming a high-fiber diet. In addition, determinants of intentions to consume a high-fiber diet were explored.
4. Discussion
The purpose of this study was to develop a theory-based instrument to evaluate determinants of consuming a high-fiber diet, and evaluate the validity and reliability of the instrument. The approach used for this instrument was one based on a whole-diet approach, rather than evaluating single components of a diet. As previous reviews have noted, while it may seem simple, defining a ‘healthy diet’ can in fact be a difficult task [
21]. The United States Dietary Guidelines, the World Health Organization, and the American Academy of Nutrition and Dietetics all have slightly different variations on what is included in a healthy diet, yet there is no universal definition [
21]. A common thread, however, through these different definitions of a ‘healthy diet’ is that it contains an adequate amount of micro and macronutrients, contains enough calories to prevent weight loss, yet not an excess of calories that would promote weight gain, and it would balance fiber-rich foods, such as fruits, vegetables, and whole grains, with other types of foods containing high amounts of salt, sugar and fat. The advantage of evaluating one’s diet using a whole-diet approach, as done in the instrument in this study, is that it sets simple guidelines for every meal (e.g., 75% of your plate should have fiber-rich foods), while being flexible for the types of foods that are used to meet this recommendation. Also, counting calories and food groups throughout the day can be a laborious task for consumers, whereas observing what is on a plate is a simpler task.
Overall, the instrument was found to have a high degree of both validity and reliability for all of the constructs of the theory. This type of research is important, as others have noted surveys used in public health, and social and behavioral research, are oftentimes not evaluated to this standard [
19,
22]. Furthermore, survey development and validation is an essential skill for health educators and public health professionals, as outlined in the core competencies in the field [
19]. Yet, despite the need for validity and reliability assessment, a review of the top health education and promotion journals revealed that many times researchers fail to report measures of validity and reliability, and almost no studies evaluated multiple forms of validity as done in this study [
23].
The theoretical basis for which this survey was developed should also be noted as a strength to this study, since it is oftentimes the case that a lack of theory is a limitation in survey development [
18,
19]. As Sharma [
24] notes the use of theory in public health and health education is important, as there are many advantages to using theory over having an a-theoretical approach. Such advantages include: theory gives discernible and measurable outcomes for public health interventions, theory guides the selection of behavior change methods and techniques, theory helps identify the optimal timing for interventions, and theory helps researchers and practitioners understand which elements of an intervention are working or are ineffective.
A review of the literature by an expert advisory group found that in the field of health behavior, the Theory of Planned Behavior (TPB—an iteration of the RAA) was the second most utilized model [
25]. The RAA represents an advancement in the TPB, since it recognizes differences in cognitive and affective attitudes, and adds a new source of normative pressure, descriptive norms [
20]. Both the TPB and RAA have been shown as useful theories in public health. Meta-analyses of TPB [
26] and RAA [
16] prospective studies showed that behavioral intentions and PBC explain 19.3% to 30.9% of the variance of health behaviors. Additionally, a meta-analysis on TPB-based health behavior change interventions showed on average they contain a weighted effect size (δ^) of 0.50 [
17].
The second purpose of this study was to evaluate the prediction model for behavioral intentions, as predicted by the independent variables attitudes, perceived norms, and PBC. Results showed this set of independent variables predicted a substantial amount of the variance of behavioral intentions (37.7%). Furthermore, perceived norms was the strongest predictor (β = 0.402), followed by PBC (β = 0.233), and attitudes (β = 0.135). These results are similar to what has been observed with the aforementioned meta-analyses on the TPB and RAA [
16,
26], as well as other studies with adults that evaluated determinants of fruit and vegetable consumption [
12], sleep behaviors [
21], sugar-sweetened beverage consumption [
27], and physical activity [
28]. More work should be done however, to evaluate additional determinants of intentions to broaden the scope of the RAA. Potential constructs that are not contained within the RAA, such as moral norms, anticipated regret, and social support, should be considered in future research.
To put these results into recommendations for behavior change interventions health practitioners can utilize, it is important to consider the difference between motivational processes (techniques to enhance intentions by changing attitudes and perceived norms) and implementational processes (techniques to enhance PBC by changing skills and the environment) [
17]. From the results found in this study, a mix of motivational and implementation processes are likely warranted. Since perceived norms was the strongest predictor, motivational processes should start with reinforcing normative beliefs that consuming a high-fiber diet is something that others in one’s life wants them to perform, and adding additional beliefs that others in one’s life are currently consuming more fiber-rich foods than they may know. PBC can be enhanced by skills-training for identifying fiber-rich foods, and helping individuals set goals around routinely consuming fiber-rich foods. Processes that can help individuals achieve such goals including action planning (e.g., being specific about what foods the individual will consume, and when), and self-monitoring.
This study has a few limitations that should be addressed. First, all of the responses were based on self-reported data, increasing the changes that the data could be biased, as the beliefs reported might not truly represent participants’ actual beliefs. Participants may have also misinterpreted certain questions and mistakenly provided untrue answers. Second, this study used a convenience sample of adults. This sample was mostly female, educated and Caucasian which have all been shown to influence dietary behaviors. For example, in a sample of adults in the United States, it was shown that women and individuals with a higher socioeconomic status had a higher diet quality [
29]. Specific gender dietary differences that have been noted included women shop at the grocery store more often, eat less fast food and take-out meals, and consume more whole-grains, fruit and overall fiber compared to men [
30,
31]. Caucasian individuals also typically have higher diet quality than other racial and ethnic minorities [
32,
33]. Therefore, caution should be given when attempting to generalize to other groups, and the instrument should be re-tested for validity and reliability when implemented with other groups. Furthermore, this sample was derived from adults on a list serve of individuals in the Full Plate Living community, a community already promoting a high-fiber diet. Efforts should be made to re-validate this survey with adults who are not already predisposed towards consuming a high-fiber diet. Finally, stability (or test–retest reliability) was not established. Future researchers should consider establishing this additional form of reliability.















{kind=link}