Implementing a Feasible Exercise Programme in an Allogeneic Haematopoietic Stem Cell Transplantation Setting—Impact on Physical Activity and Fatigue


Abstract
:1. Introduction
2. Materials and Methods
2.1. Context and Setting
2.2. The Exercise Programme
2.3. Participants and Procedure
2.4. The Fatigue Instrument
2.5. Statistics and Ethics
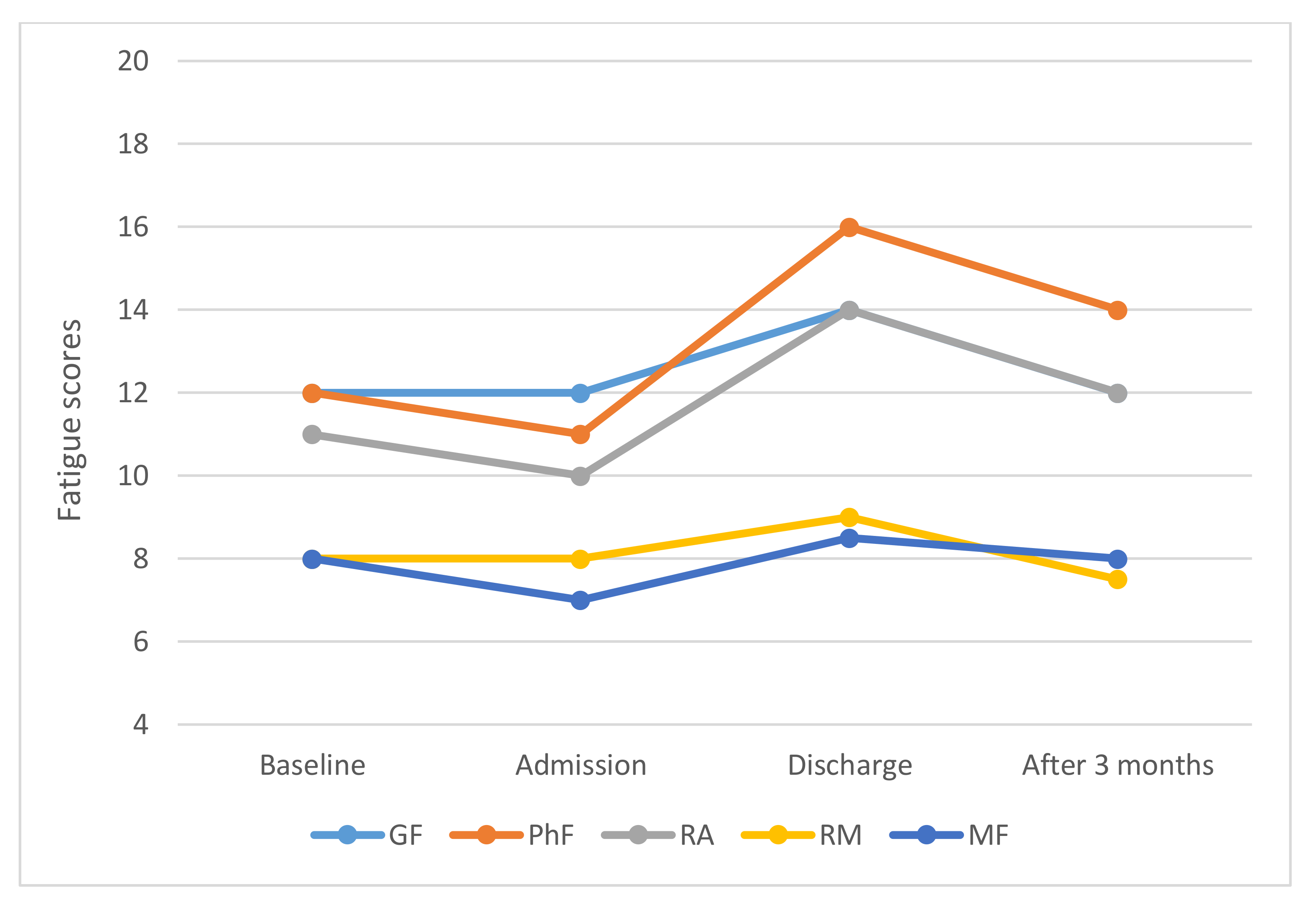
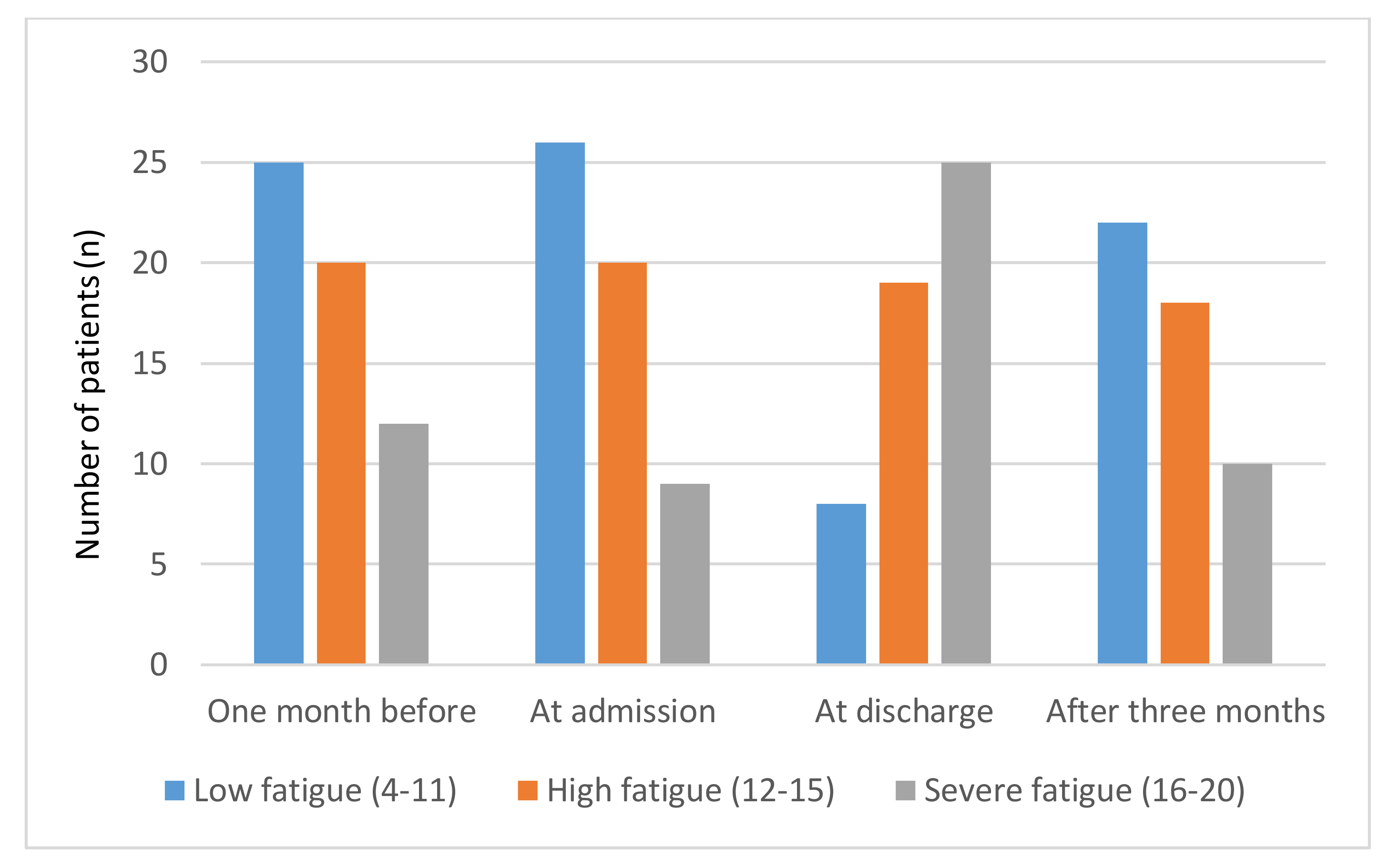
3. Results
3.1. Sub-Group Analysis
3.1.1. Gender
3.1.2. Age
3.1.3. Disease Groups
3.1.4. Conditioning Regimens
4. Discussion
- Despite the significantly longer duration of strength exercises performed by the female patients they were more fatigued both at discharge and three months after the HSCT than the male patients, who were already back to baseline at the time of discharge.
- The younger patients (≤50 years) had already returned to baseline fatigue levels at discharge, while the older patients were persistently fatigued three months after transplantation.
- The high-risk group was more longitudinally affected by fatigue, especially the mental aspects, than the standard-risk group.
- There were no statistical differences in fatigue levels at any measurement point after allo-HSCT between the MAC patients and the non-MAC patients. Three months after HSCT, the non-MAC group reported a significantly lower GF score compared to discharge and the MAC group was less fatigued regarding PhF and RA compared to discharge.
4.1. Considerations Regarding Age Differences
4.2. Reflections on Gender Differences
4.3. Disease Groups
4.4. Conditioning Regimens
4.5. Strengths and Limitations
5. Implications and Future Research
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Passweg, J.R.; Baldomero, H.; Basak, G.W.; Chabannon, C.; Corbacioglu, S.; Duarte, R.; Kuball, J.; Lankester, A.; Montoto, S.; de Latour, R.P.; et al. The EBMT activity survey report 2017: A focus on allogeneic HCT for nonmalignant indications and on the use of non-HCT cell therapies. Bone Marrow Transplant. 2019, 54, 1575–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyurkocza, B.; Rezvani, A.; Storb, R.F. Allogeneic hematopoietic cell transplantation: The state of the art. Expert Rev. Hematol. 2010, 3, 285–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuba, K.; Esser, P.; Scherwath, A.; Schirmer, L.; Schulz-Kindermann, F.; Dinkel, A.; Balck, F.; Koch, U.; Kröger, N.; Götze, H.; et al. Cancer-and-treatment-specific distress and its impact on posttraumatic stress in patients undergoing allogeneic hematopoietic stem cell transplantation (HSCT). Psychooncology 2017, 26, 1164–1171. [Google Scholar] [CrossRef]
- Im, A.; Mitchell, S.A.; Steinberg, S.M.; Curtis, L.; Berger, A.; Baird, K.; Kuzmina, Z.; Joe, G.; Comis, L.E.; Juckett, M.; et al. Prevalence and determinants of fatigue in patients with moderate to severe chronic GvHD. Bone Marrow Transplant. 2016, 51, 705–712. [Google Scholar] [CrossRef] [Green Version]
- Pillay, B.; Lee, S.J.; Katona, L.; De Bono, S.; Burney, S.; Avery, S. A prospective study of the relationship between sense of coherence, depression, anxiety, and quality of life of haematopoietic stem cell transplant patients over time. Psychooncology 2015, 24, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Dirou, S.; Chambellan, A.; Chevallier, P.; Germaud, P.; Lamirault, G.; Gourraud, P.A.; Perrot, B.; Delasalle, B.; Forestier, B.; Guillaume, T.; et al. Deconditioning, fatigue and impaired quality of life in long-term survivors after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, Version 2.2015. J. Natl. Compr. Canc. Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef]
- Wang, X.S.; Zhao, F.; Fisch, M.J.; O’Mara, A.M.; Cella, D.; Mendoza, T.R.; Cleeland, C.S. Prevalence and characteristics of moderate to severe fatigue: A multicenter study in cancer patients and survivors. Cancer 2014, 120, 425–432. [Google Scholar] [CrossRef]
- Bergkvist, K.; Winterling, J.; Johansson, E.; Johansson, U.B.; Svahn, B.M.; Remberger, M.; Mattsson, J.; Larsen, J. General health, symptom occurrence, and self-efficacy in adult survivors after allogeneic hematopoietic stem cell transplantation: A cross-sectional comparison between hospital care and home care. Support Care Cancer 2015, 23, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Wehrlen, L.; Mitchell, S.A.; Yang, L.; Bevans, M.F. Fatigue predicts impaired social adjustment in survivors of allogeneic hematopoietic cell transplantation (HCT). Support. Care Cancer 2019, 27, 1355–1363. [Google Scholar] [CrossRef]
- Jim, H.S.L.; Sutton, S.K.; Jacobsen, P.B.; Martin, P.; Flowers, M.E.; Lee, S.J. Risk factors for depression and fatigue among hematopoietic cell transplant survivors. Cancer 2016, 122, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Mosher, C.E.; DuHamel, K.N.; Rini, C.; Corner, G.; Lam, J.; Redd, W.H. Quality of life concerns and depression among hematopoietic stem cell transplant survivors. Support. Care Cancer 2011, 19, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Tsubaki, A.; Hotta, K.; Fu, J.B.; Fuji, S. The benefit of exercise in patients who undergo allogeneic hematopoietic stem cell transplantation. J. Int. Soc. Phys. Rehabil. Med. 2019, 2, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Van Vulpen, J.K.; Velthuis, M.J.; Steins Bisschop, C.N.; Travier, N.; Van Den Buijs, B.J.; Backx, F.J.; Los, M.; Erdkamp, F.L.; Bloemendal, H.J.; Koopman, M.; et al. Effects of an Exercise Program in Colon Cancer Patients undergoing Chemotherapy. Med. Sci. Sports Exerc. 2016, 48, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Furmaniak, A.C.; Menig, M.; Markes, M.H. Exercise for women receiving adjuvant therapy for breast cancer. Cochrane Database Syst. Rev. 2016, 9, CD005001. [Google Scholar] [CrossRef]
- Mijwel, S.; Jervaeus, A.; Bolam, K.A.; Norrbom, J.; Bergh, J.; Rundqvist, H.; Wengstrom, Y. High-intensity exercise during chemotherapy induces beneficial effects 12 months into breast cancer survivorship. J. Cancer Surviv. 2019, 13, 244–256. [Google Scholar] [CrossRef] [Green Version]
- Van Vulpen, J.K.; Peeters, P.H.; Velthuis, M.J.; van der Wall, E.; May, A.M. Effects of physical exercise during adjuvant breast cancer treatment on physical and psychosocial dimensions of cancer-related fatigue: A meta-analysis. Maturitas 2016, 85, 104–111. [Google Scholar] [CrossRef]
- Hacker, E.D.; Collins, E.; Park, C.; Peters, T.; Patel, P.; Rondelli, D. Strength Training to Enhance Early Recovery after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2017, 23, 659–669. [Google Scholar] [CrossRef] [Green Version]
- Wiskemann, J.; Dreger, P.; Schwerdtfeger, R.; Bondong, A.; Huber, G.; Kleindienst, N.; Ulrich, C.M.; Bohus, M. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011, 117, 2604–2613. [Google Scholar] [CrossRef]
- Liang, Y.; Zhou, M.; Wang, F.; Wu, Z. Exercise for physical fitness, fatigue and quality of life of patients undergoing hematopoietic stem cell transplantation: A meta-analysis of randomized controlled trials. JPN J. Clin. Oncol. 2018, 48, 1046–1057. [Google Scholar] [CrossRef]
- Oberoi, S.; Robinson, P.D.; Cataudella, D.; Culos-Reed, S.N.; Davis, H.; Duong, N.; Gibson, F.; Gotte, M.; Hinds, P.; Nijhof, S.L.; et al. Physical activity reduces fatigue in patients with cancer and hematopoietic stem cell transplant recipients: A systematic review and meta-analysis of randomized trials. Crit. Rev. Oncol. Hematol. 2018, 122, 52–59. [Google Scholar] [CrossRef]
- Mohammed, J.; Smith, S.R.; Burns, L.; Basak, G.; Aljurf, M.; Savani, B.N.; Schoemans, H.; Peric, Z.; Chaudhri, N.A.; Chigbo, N.; et al. Role of Physical Therapy before and after Hematopoietic Stem Cell Transplantation: White Paper Report. Biol. Blood Marrow Transplant. 2019, 25, e191–e198. [Google Scholar] [CrossRef]
- Smets, E.M.; Garssen, B.; Bonke, B.; De Haes, J.C. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef] [Green Version]
- Hagelin, C.L.; Wengstrom, Y.; Runesdotter, S.; Furst, C.J. The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different populations. Acta Oncol. 2007, 46, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, A.; Lennerling, A.; Kisch, A.; Jakobsson, S. Fatigue 1-5 years after lung transplantation: A multicenter cross-sectional cohort study. Nord. J. Nurs. Res. 2019, 39, 68–75. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Age, years; mean (SD) range ≤50 years >50 years | 55.5 (12.4) 21–70 17 (25) 50 (75) |
| Gender, n (%) | |
| male | 34 (51) |
| female | 33 (49) |
| Primary diagnosis | |
| AML | 25 (37) |
| MDS | 14 (21) |
| MPS | 9 (13) |
| NHL | 8 (12) |
| ALL | 6 (9) |
| CML | 4 (6) |
| CLL | 1 (2) |
| Disease status at transplant | |
| standard-risk | 28 (42) |
| high-risk | 39 (58) |
| Donor | |
| sibling | 16 (24) |
| URD | 47 (70) |
| haplo | 4 (6) |
| Stem cell source | |
| BM | 0 (0) |
| PBSC | 67 (100) |
| Conditioning regimen | |
| MAC | 13 (19) |
| Non-MAC | 54 (81) |
| Marital status at transplant | |
| Married/cohabiting | 48 (72) |
| Living alone | 19 (28) |
| Fatigue Dimensions | Baseline: One Month Before Admission Median (p25; p75) | On Admission For HSCT Median (p25; p75) | At Discharge After HSCT Median (p25; p75) | 3 Months After HSCT Median (p25; p75) | ||||
|---|---|---|---|---|---|---|---|---|
| Gender | Men (n = 29) | Women (n = 28) | Men (n = 28) | Women (n = 27) | Men (n = 25) | Women (n = 27) | Men (n = 26) | Women (n = 24) |
| General fatigue (GF) | 12 (7; 16) | 13 (8.25; 15) | 10.5 (7.25; 14.5) | 12 (9; 14) | 13 (12; 16.5) | 14 (12; 18) | 12 (10.75; 14.25) | 13 (8.25; 15.75) |
| Physical fatigue (PhF) | 12 (8; 18.5) | 13 (10; 17) | 11 (7; 14.5) | 12 (10; 14) | 17 (12.5; 18.5) | 15 (13; 18) | 13 (10.75; 16) | 15 (10.25; 17) |
| Reduced activity (RA) | 11 (8; 14) | 11.5 (8.25; 15) | 9.5 (7; 14.75) | 10 (8; 13) | 14 (10.5; 16) | 14 (12; 15) | 11.5 (8; 14.25) | 13 (7; 16) |
| Reduced motivation (RM) | 8 (6; 10.5) | 8.5 (6; 12) | 7.5 (5; 10.75) | 9 (7; 14) | 10 (7.5; 12) | 9 (6; 13) | 7 (5; 10.25) | 8 (5; 13.5) |
| Mental fatigue (MF) | 8 (4; 12) | 8 (4; 9.75) | 7.5 (4.25; 10.5) | 7 (4; 12) | 11 (7.5; 11.5) | 7 (4; 11) | 8 (4; 11) | 8 (4; 12) |
| Fatigue Dimensions | Baseline: One Month Before Admission Median (p25; p75) | On Admission For HSCT Median (p25; p75) | At Discharge After HSCT Median (p25; p75) | 3 Months After HSCT Median (p25; p75) | ||||
|---|---|---|---|---|---|---|---|---|
| Age group | ≤50 years (n = 16) | >50 years (n = 41) | ≤50 years (n = 14) | >50 years (n = 41) | ≤50 years (n = 15) | >50 years (n = 37) | ≤50 years (n = 13) | >50 years (n = 37) |
| General fatigue (GF) | 13.5 (9.75; 15) | 11 (7.5; 15) | 12 (8.75; 16) | 11 (8; 13.5) | 14 (13; 18) | 14 (12; 17.5) | 13 (11; 15.5) | 12 (8.5; 15) |
| Physical fatigue (PhF) | 14 (10.25; 17) | 12 (10; 18) | 11.5 (9; 15.25) | 11 (9; 14) | 16 (13; 18) | 16 (13; 18) | 12 (10.5; 16) | 14 (10.5; 17) |
| Reduced activity (RA) | 13 (9.25; 15) | 11 (8; 13.5) | 9.5 (7; 14.25) | 10 (6.5; 14) | 13 (11; 15) | 14 (12; 17) | 10 (7; 15.5) | 12 (8; 15) |
| Reduced motivation (RM) | 8.5 (6; 11.5) | 8 (6; 12) | 7.5 (4.75; 11) | 9 (5.5; 12.5) | 7 (6; 10) | 11 (8; 13) | 8 (5; 11.5) | 7 (5; 11.5) |
| Mental fatigue (MF) | 9.5 (7; 12) | 5 (4; 10) | 8.5 (6.25; 12.25) | 7 (4; 10) | 9 (7; 11) | 8 (4; 12) | 9 (7; 12) | 8 (4; 11) |
| Fatigue Dimensions | Baseline: One Month Before Admission Median (p25; p75) | On Admission For HSCT Median (p25; p75) | At Discharge After HSCT Median (p25; p75) | 3 Months After HSCT Median (p25; p75) | ||||
|---|---|---|---|---|---|---|---|---|
| Disease group | standard-risk (n = 25) | high-risk (n = 32) | standard-risk (n = 24) | high-risk (n = 31) | standard-risk (n = 23) | high-risk (n = 29) | standard-risk (n = 23) | high-risk (n = 27) |
| General fatigue (GF) | 13 (8; 15.5) | 12 (8; 14.75) | 11.5 (8; 14.75) | 12 (8; 14) | 14 (12; 18) | 14 (12; 16.5) | 12 (10; 15) | 13 (9; 15) |
| Physical fatigue (PhF) | 12 (10; 17.5) | 12.5 (10; 17.5) | 11 (9; 13.75) | 11 (10; 15) | 16 (13; 17) | 16 (13.5; 18) | 13 (10; 17) | 15 (12; 16) |
| Reduced activity (RA) | 12 (6; 15.5) | 11 (9; 13) | 10 (6.25; 15) | 10 (8; 14) | 14 (11; 16) | 14 (12; 16) | 12 (7; 15) | 12 (8; 15) |
| Reduced motivation (RM) | 8 (6; 11.5) | 8 (6; 12) | 8 (5; 12.75) | 9 (6; 12) | 10 (6; 13) | 9 (6.5; 12) | 7 (5; 12) | 8 (5; 11) |
| Mental fatigue (MF) | 10 (4; 12.5) | 6 (4; 8.75) | 8 (4.25; 11.75) | 7 (4; 11) | 9 (7; 11) | 8 (4; 12) | 7 (4; 11) | 9 (4; 12) |
| Fatigue Dimensions | Baseline: One Month Before Admission Median (p25; p75) | On Admission For HSCT Median (p25; p75) | At Discharge After HSCT Median (p25; p75) | 3 Months After HSCT Median (p25; p75) | ||||
|---|---|---|---|---|---|---|---|---|
| Conditioning regimen | non-Mac (n = 45) | Mac (n = 12) | non-Mac (n = 44) | Mac (n = 11) | non-Mac (n = 41) | Mac (n = 11) | non-Mac (n = 39) | Mac (n = 11) |
| General fatigue (GF) | 12 (8; 15) | 12.5 (6; 15.75) | 11.5 (8, 13.75) | 12 (8; 16) | 14 (12; 16.5) | 14 (13; 19) | 12 (9; 15) | 15 (11; 20) |
| Physical fatigue (PhF) | 12 (10; 17) | 16.5 (7.75,17.75) | 11 (9; 14) | 12 (9; 16) | 15 (12.5; 17.5) | 17 (13; 20) | 14 (11; 17) | 15 (10; 16) |
| Reduced activity (RA) | 11 (8; 13.5) | 13 (7.5,15.7) | 10 (7.25; 14) | 9 (7; 15) | 14 (12; 16) | 14 (11; 16) | 12 (8; 15) | 10 (7; 16) |
| Reduced motivation (RM) | 8 (6; 12) | 7.5 (6, 11.25) | 9 (6; 12.75) | 6 (4; 9) | 10 (6.5; 13) | 9 (6; 11) | 7 (5; 11) | 8 (5, 12) |
| Mental fatigue (MF) | 7 (4; 9) | 11 (9, 12.75) | 7 (4; 9) | 9 (4; 13) | 8 (4; 11.5) | 11 (7; 11) | 8 (4; 11) | 9 (7; 12) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kisch, A.; Jakobsson, S.; Forsberg, A. Implementing a Feasible Exercise Programme in an Allogeneic Haematopoietic Stem Cell Transplantation Setting—Impact on Physical Activity and Fatigue. Int. J. Environ. Res. Public Health 2020, 17, 4302. https://doi.org/10.3390/ijerph17124302
Kisch A, Jakobsson S, Forsberg A. Implementing a Feasible Exercise Programme in an Allogeneic Haematopoietic Stem Cell Transplantation Setting—Impact on Physical Activity and Fatigue. International Journal of Environmental Research and Public Health. 2020; 17(12):4302. https://doi.org/10.3390/ijerph17124302
Chicago/Turabian StyleKisch, Annika, Sofie Jakobsson, and Anna Forsberg. 2020. "Implementing a Feasible Exercise Programme in an Allogeneic Haematopoietic Stem Cell Transplantation Setting—Impact on Physical Activity and Fatigue" International Journal of Environmental Research and Public Health 17, no. 12: 4302. https://doi.org/10.3390/ijerph17124302