Co-Creation with Older Adults to Improve User-Experience of a Smartphone Self-Test Application to Assess Balance Function



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
User Experience and Co-Creation in Application Design
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Prototype
2.4. Data Collection during Co-Creation Process
2.5. Data Analysis
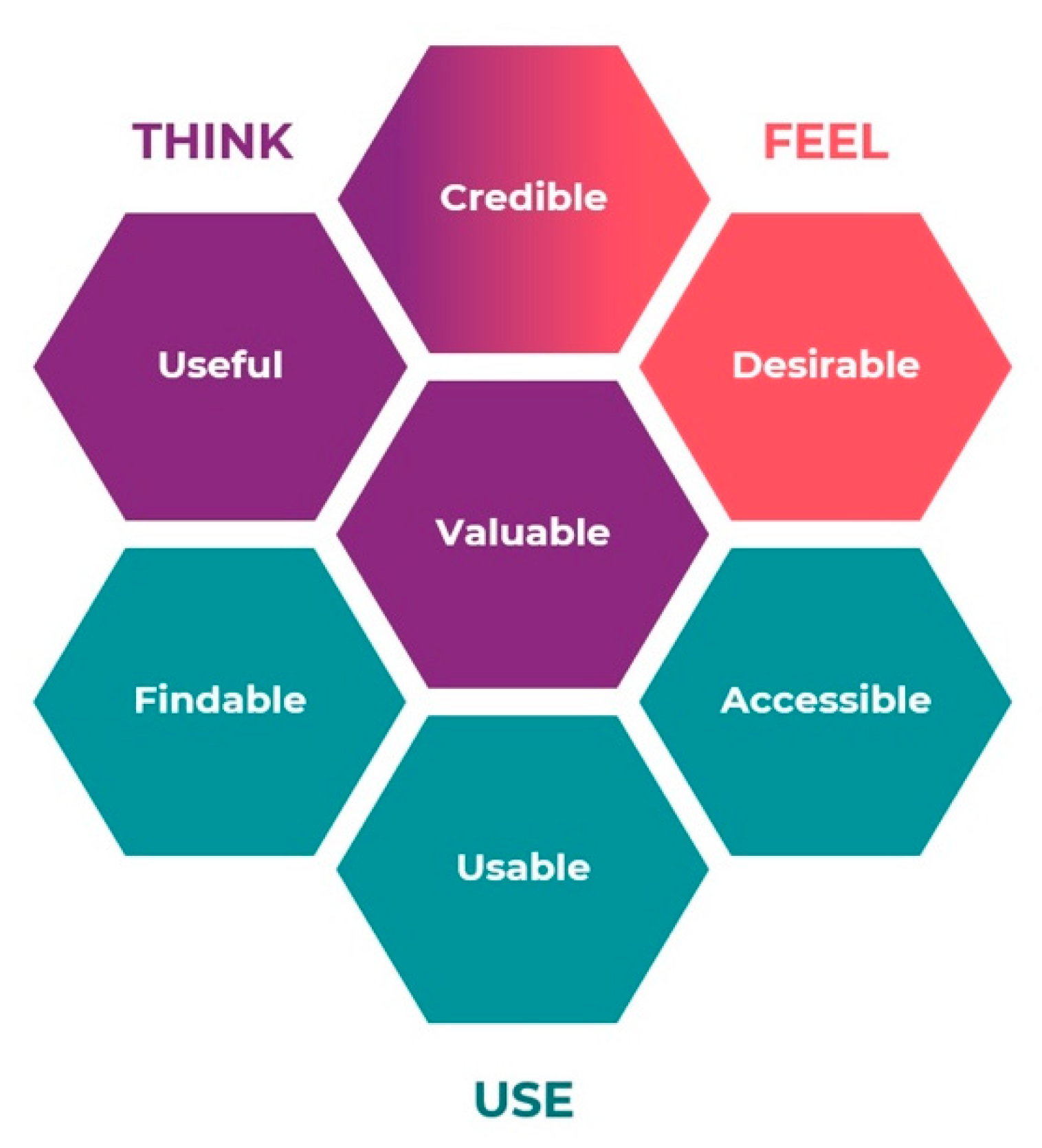
2.5.1. The Honeycomb Model
2.5.2. Analytical Procedure
2.6. Ethical Considerations
3. Results
3.1. Analysis of Co-Creation Sessions
3.1.1. Findable
“If there should be only one symbol, then it is better with the one with the feet together, as you start with that one.”Woman 5, 71 years, Session 3
“I understand that it is a trade-off between whether it becomes too extensive or clear …. that, both to get it clear and not too comprehensive, and you want to have as much as possible in there.”Woman 3, 73 years, Session 4
3.1.2. Accessible
“But it is very informative and simple. You talk clearly and slowly. My husband is very hard of hearing, and he had no problems to hear.”Woman 5, 71 years, Session 5
3.1.3. Usable
“You have to practice first, to be able to do it without instructions later.”Man 1, 76 years, Session 2
3.1.4. Desirable
“If you are looking at the entire video then, then I would have got fed up before finishing...I would have turned it off before getting to the end.”Female 2, 76 years, Session 1
“May I say one more thing, this is not a competition is it? You can post results from competitions on Facebook, but that’s something different.”Woman 2, 76 years, Session 3
3.1.5. Credible
“You know, somehow… you know subconsciously…(moves his arms to the sides as though searching support)…that you can get support against the wall.”Man 4, 82 years, Session 2 (video)
3.1.6. Useful
“I think [about results]—better or worse are based on what I did before. Have I made any improvement, or just got worse, or does it look the same? That is interesting. Or will there be a red flag, now you have… what happened to your balance?”Female 5, 71 years, Session 3
“I agree with that, that you would like to see how it [results] develops. It is exciting to follow, if it progresses or if you have been lazy. Yes, you need that push. Then it is fun as well to follow the results.”Female 6, 74 years, Session 3
3.1.7. Valuable
“But people are so different, some run to the doctor or health center for the slightest thing, others stand it to the worst, so it is very difficult to tell [if MyBalance app will help everyone] but the use of smartwatches and smartphones could be a signal that something is wrong. And it is not always…eh, that the inner feeling will alert you—then it could be beneficial with this type of signal to alert that something is wrong.”Male 4, 82 years, Session 4
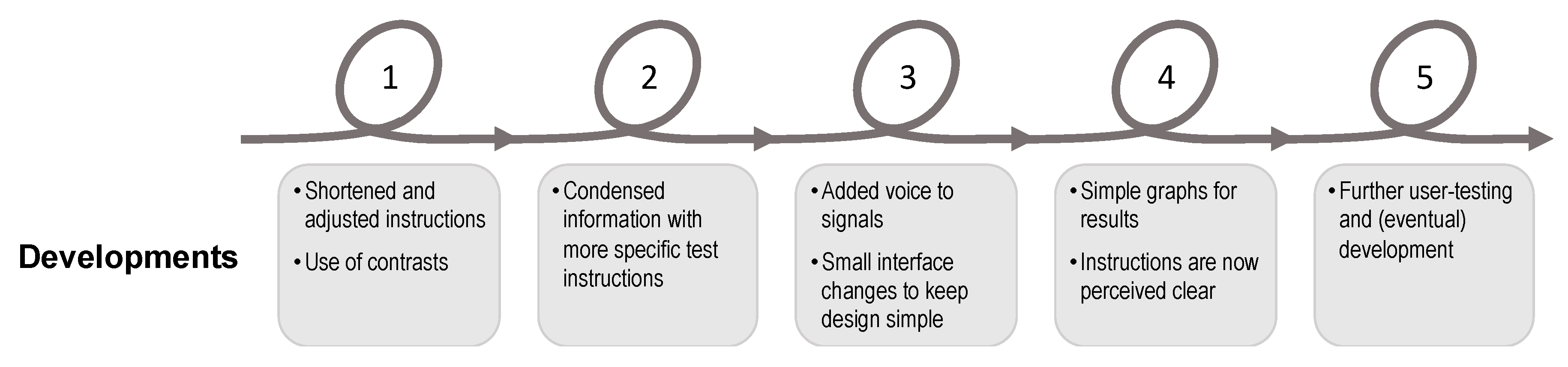
3.2. Application Development during the Co-Creation Process
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 20 March 2020).
- World Health Organization. Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 6 March 2019).
- Tinetti, M.E.; Kumar, C. The Patient Who Falls: “It’s Always a Trade-off”. JAMA 2010, 303, 258–266. [Google Scholar] [CrossRef]
- Bert, F.; Giacometti, M.; Gualano, M.R.; Siliquini, R. Smartphones and Health Promotion: A Review of the Evidence. J. Med. Syst. 2013, 38, 9995. [Google Scholar] [CrossRef]
- European Commission; Eurostat. Eurostat-Tables, Graphs and Maps Interface (TGM) Graph. Available online: https://ec.europa.eu/eurostat/tgm/graph.do?tab=graph&plugin=1&pcode=tin00083&language=en&toolbox=data (accessed on 12 December 2019).
- Internetstiftelsen. The Swedes and the Internet 2019. Available online: https://svenskarnaochinternet.se/rapporter/svenskarna-och-internet-2019/the-swedes-and-the-internet-2019-summary/ (accessed on 19 November 2019).
- DiClemente, R.; Nowara, A.; Shelton, R.; Wingood, G. Need for Innovation in Public Health Research. Am. J. Public Health 2019, 109, S117–S120. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I. Health promotion 4.0. Health Promot. Int. 2019, 34, 179–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamm, J.; Money, A.G.; Atwal, A.; Paraskevopoulos, I. Fall prevention intervention technologies: A conceptual framework and survey of the state of the art. J. Biomed. Inform. 2016, 59, 319–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, P.; Reve, E.v.h.; Daniel, F.; Casati, F.; de Bruin, E.D. Motivating and assisting physical exercise in independently living older adults: A pilot study. Int. J. Med. Inform. 2013, 82, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbaere, K.; Valenzuela, T.; Woodbury, A.; Davies, T.; Yeong, J.; Steffens, D.; Miles, L.; Pickett, L.; Zijlstra, G.; Clemson, L. Evaluating the effectiveness of a home-based exercise programme delivered through a tablet computer for preventing falls in older community-dwelling people over 2 years: Study protocol for the Standing Tall randomised controlled trial. BMJ Open 2015, 5, e009173. [Google Scholar] [CrossRef] [Green Version]
- Roeing, K.L.; Hsieh, K.L.; Sosnoff, J.J. A systematic review of balance and fall risk assessments with mobile phone technology. Arch. Gerontol. Geriatr. 2017, 73, 222–226. [Google Scholar] [CrossRef]
- Rasche, P.; Mertens, A.; Bröhl, C.; Theis, S.; Seinsch, T.; Wille, M.; Pape, H.-C.; Knobe, M. The “Aachen fall prevention App”—A Smartphone application app for the self-assessment of elderly patients at risk for ground level falls. Patient Saf. Surg. 2017, 11, 14. [Google Scholar] [CrossRef]
- Hsieh, K.L.; Fanning, J.T.; Rogers, W.A.; Wood, T.A.; Sosnoff, J.J. A Fall Risk mHealth App for Older Adults: Development and Usability Study. JMIR Aging 2018, 1, e11569. [Google Scholar] [CrossRef] [Green Version]
- Ciuti, G.; Ricotti, L.; Menciassi, A.; Dario, P. MEMS Sensor Technologies for Human Centred Applications in Healthcare, Physical Activities, Safety and Environmental Sensing: A Review on Research Activities in Italy. Sensors 2015, 15, 6441–6468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regterschot, G.R.H.; Morat, T.; Folkersma, M.; Zijlstra, W. The application of strength and power related field tests in older adults: Criteria, current status and a future perspective. Eur. Rev. Aging Phys. Act. 2015, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassenzahl, M.; Tractinsky, N. User experience—A research agenda. Behav. Inf. Technol. 2006, 25, 91–97. [Google Scholar] [CrossRef]
- Morville, P. User Experience Design. Available online: http://semanticstudios.com/user_experience_design/ (accessed on 2 September 2019).
- US Dept of Health & Human services User Experience Basics. Available online: www.usability.gov/what-and-why/user-experience.html (accessed on 19 January 2020).
- Giguere, A.; Légaré, F.; Grad, R.; Pluye, P.; Haynes, R.B.; Cauchon, M.; Rousseau, F.; Argote, J.A.; Labrecque, M. Decision boxes for clinicians to support evidence-based practice and shared decision making: The user experience. Implement. Sci. 2012, 7, 72. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.-J.; Lo, S.-Y.; Kuo, C.-L.; Wang, Y.-L.; Hsiao, H.-C. Development of an intervention tool for precision oral self-care: Personalized and evidence-based practice for patients with periodontal disease. PLoS ONE 2019, 14, e0225453. [Google Scholar] [CrossRef] [PubMed]
- Fearns, N.; Graham, K.; Johnston, G.; Service, D. Improving the user experience of patient versions of clinical guidelines: User testing of a Scottish Intercollegiate Guideline Network (SIGN) patient version. BMC Health Serv. Res. 2015, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Orr, M.; Isaacs, J.; Godbout, R.; Witmans, M.; Corkum, P. A usability study of an internet-delivered behavioural intervention tailored for children with residual insomnia symptoms after obstructive sleep apnea treatment. Internet Interv. 2019, 18, 100265. [Google Scholar] [CrossRef]
- Karagianni, K. Optimizing the UX Honeycomb—A Small Amendment to the Classic Diagram Hopefully Improves Its UX. Available online: https://uxdesign.cc/optimizing-the-ux-honeycomb-1d10cfb38097 (accessed on 18 September 2019).
- Morey, S.A.; Stuck, R.E.; Chong, A.W.; Barg-Walkow, L.H.; Mitzner, T.L.; Rogers, W.A. Mobile Health Apps: Improving Usability for Older Adult Users. Ergon. Des. Q. Human Factors Appl. 2019, 27, 4–13. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [Green Version]
- Tsertsidis, A.; Kolkowska, E.; Hedström, K. Factors influencing seniors’ acceptance of technology for ageing in place in the post-implementation stage: A literature review. Int. J. Med Inform. 2019, 129, 324–333. [Google Scholar] [CrossRef]
- Sanders, E.B.-N.; Stappers, P.J. Co-creation and the new landscapes of design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, J.; Robertson, T. (Eds.) Routledge International Handbook of Participatory Design; Routledge: New York, NY, USA, 2013; ISBN 978-0-415-69440-7. [Google Scholar]
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving Research Impact Through Co-creation in Community-Based Health Services: Literature Review and Case Study. Milbank Q. 2016, 94, 392–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F.M. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Preece, J.; Rogers, Y.; Sharp, H. Interaction Design: Beyond Human-Computer Interaction, 4th ed.; John Wiley & Sons Ldt.: Chichester, UK, 2015. [Google Scholar]
- Pettersson, B.; Wiklund, M.; Janols, R.; Lindgren, H.; Lundin-Olsson, L.; Skelton, D.A.; Sandlund, M. ‘Managing pieces of a personal puzzle’—Older people’s experiences of self-management falls prevention exercise guided by a digital program or a booklet. BMC Geriatr. 2019, 19, 43. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J. Estimating the number of subjects needed for a thinking aloud test. Int. J. Hum. Comput. Stud. 1994, 41, 385–397. [Google Scholar] [CrossRef]
- Jaspers, M.W.M. A comparison of usability methods for testing interactive health technologies: Methodological aspects and empirical evidence. Int. J. Med Inform. 2009, 78, 340–353. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lindgren, B.-M.; Lundman, B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Educ. Today 2017, 56, 29–34. [Google Scholar] [CrossRef]
- Házi, C. Re-Designing the UX Honeycomb—A Simple Way to Understand What UX Really Is. Available online: https://blog.prototypr.io/re-designing-the-ux-honeycomb-a-simple-way-to-understand-what-ux-really-is-54d0bf4387fc (accessed on 30 December 2019).
- Elo, S.; Kääriäinen, M.; Kanste, O.; Pölkki, T.; Utriainen, K.; Kyngäs, H. Qualitative Content Analysis: A Focus on Trustworthiness. SAGE Open 2014, 4, 215824401452263. [Google Scholar] [CrossRef]
- Cajita, M.I.; Hodgson, N.A.; Lam, K.W.; Yoo, S.; Han, H.-R. Facilitators of and Barriers to mHealth Adoption in Older Adults with Heart Failure. CIN Comput. Inform. Nurs. 2018, 36, 1. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, R.; Vereijken, B.; Mellone, S.; Corzani, M.; Helbostad, J.L.; Taraldsen, K. App-based Self-administrable Clinical Tests of Physical Function: Development and Usability Study. JMIR MHealth UHealth 2020, 8, e16507. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansson, L.; Wiklund, M.; Öhberg, F.; Danielsson, K.; Sandlund, M. Co-Creation with Older Adults to Improve User-Experience of a Smartphone Self-Test Application to Assess Balance Function. Int. J. Environ. Res. Public Health 2020, 17, 3768. https://doi.org/10.3390/ijerph17113768
Mansson L, Wiklund M, Öhberg F, Danielsson K, Sandlund M. Co-Creation with Older Adults to Improve User-Experience of a Smartphone Self-Test Application to Assess Balance Function. International Journal of Environmental Research and Public Health. 2020; 17(11):3768. https://doi.org/10.3390/ijerph17113768
Chicago/Turabian StyleMansson, Linda, Maria Wiklund, Fredrik Öhberg, Karin Danielsson, and Marlene Sandlund. 2020. "Co-Creation with Older Adults to Improve User-Experience of a Smartphone Self-Test Application to Assess Balance Function" International Journal of Environmental Research and Public Health 17, no. 11: 3768. https://doi.org/10.3390/ijerph17113768