Cardioprotective Effects of Honey and Its Constituent: An Evidence-Based Review of Laboratory Studies and Clinical Trials


 ,
,
Abstract
:1. Introduction
1.1. Burden of Heart Disease
1.2. Parameters of Cardiovascular Health
1.3. Honey and Its Constituents
1.4. Cardioprotective Effect of Honey
2. Methods
2.1. Literature Search
2.2. Inclusion/Exclusion Criteria
2.3. Article Selection
2.4. Data Management
2.5. Risk of Bias Assessment
3. Results
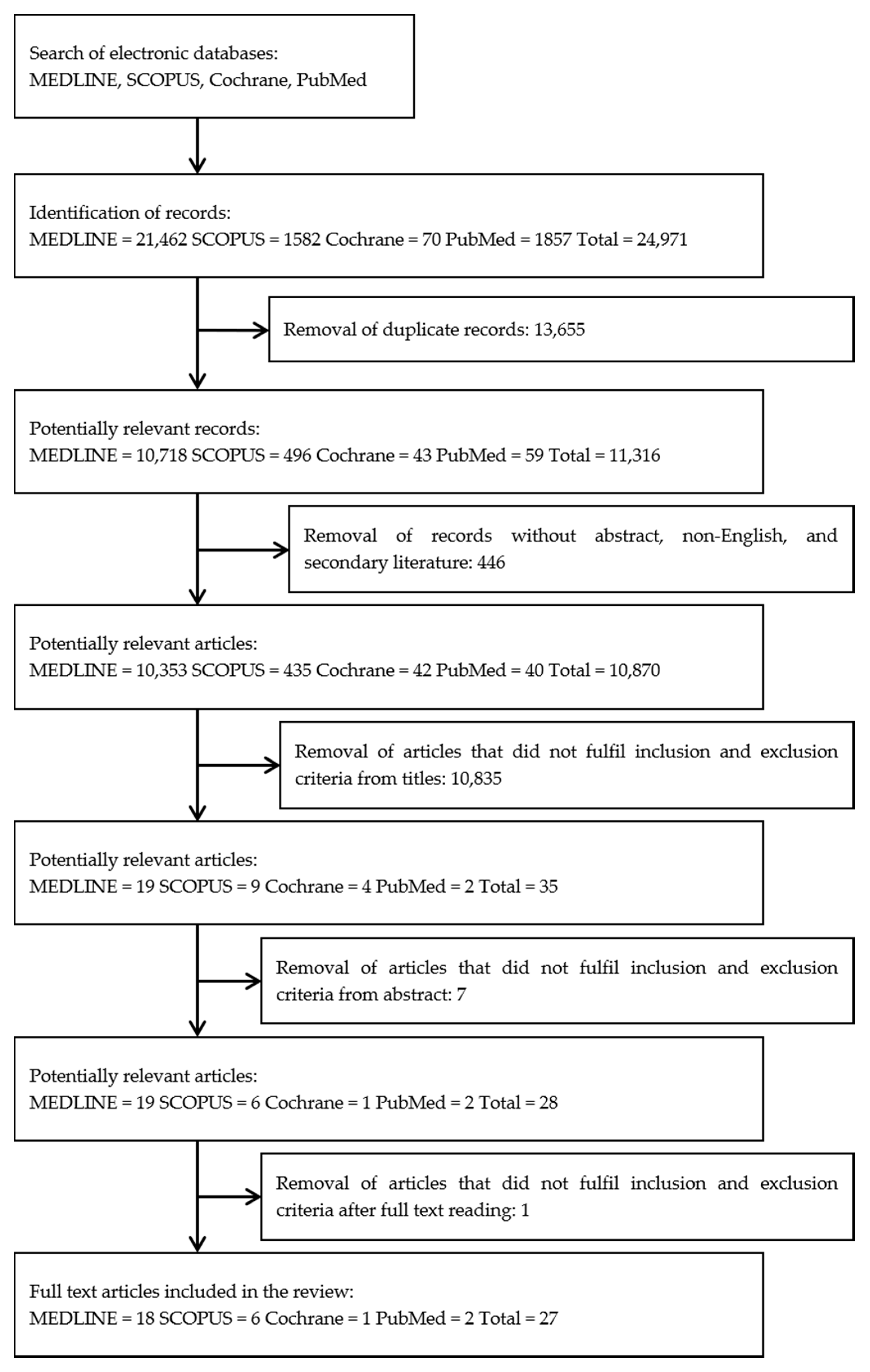
3.1. Study Selection
3.2. Study Characteristics
3.3. Clinical outcome of Honey Consumption
3.4. Honey Improves Lipid Metabolism
3.5. Honey Antioxidative Effects
3.6. Honey Prevents Free Radical Production
3.7. Honey Modulates Blood Pressure
3.8. Honey Ameliorates Cardiac Arrhythmia
3.9. Honey Reduces Myocardial Infarct Area
3.10. Honey Reduces Myocardial Injury Marker
3.11. Honey Modulates Age-Related Protein Expression
3.12. Chrysin Rescues Myocardial Injury
3.13. Chrysin Regulates Blood Pressure
3.14. Pinocembrin Ameliorates Cardiac Arrhythmia
3.15. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| ATP | Adenosine Triphosphate |
| ATR-FTIR | Attenuated Total Reflection–Fourier Transform Infra-Red |
| BMI | Body mass index |
| CK-MB | Creatine kinase MB |
| CRP | C-reactive protein |
| CVPI | Cardiovascular risk predictive index |
| DBP | Diastolic blood pressure |
| ECG | Electrocardiogram |
| GSH | Reduced glutathione |
| GPx | Glutathione peroxide |
| GRx | Glutathione reductase |
| GST | Glutathione-S-transferase |
| HDL | High-density lipoprotein |
| IKK-β | Inhibitor of nuclear factor kappa-B kinase subunit beta |
| ISO | Isoproterenol |
| LDL | Low-density protein |
| NADH | Nicotinamide adenine dinucleotide |
| NF- κβp65 | Nuclear factor kappa-light-chain-enhancer of activated B cells |
| PPAR-γ | Peroxisome proliferator-activated receptor gamma |
| RAGE | Receptor for advance glycation end products |
| ROS | Reactive oxygen species |
| SBP | Systolic blood pressure |
| cTn-1 | Serum cardiac troponin 1 |
| SOD | Superoxide dismutase |
| TBARS | Thiobarbituric acid-reactive substances |
| TC | Total cholesterol |
| TG | Total triglyceride |
| TNF-α | Tumour necrosis factor-alpha |
| VBP | Venous blood pressure |
| VEBs | Ventricular ectopic beats |
| VF | Ventricular fibrillation |
| VLDL | Very low-density lipoprotein |
| VT | Ventricular tachycardia |
References
- World Health Organization. Cardiovascular Diseases (CVDs). 2018. Available online: www.who.int/cardiovascular_diseases/en/ (accessed on 13 May 2020).
- Rezende, P.C.; Ribas, F.F.; Serrano, C.V.; Hueb, W. Clinical significance of chronic myocardial ischemia in coronary artery disease patients. J. Thorac. Dis. 2019, 11, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Arevalo, H.J.; Vadakkumpadan, F.; Guallar, E.; Jebb, A.; Malamas, P.; Wu, K.C.; Trayanova, N.A. Arrhythmia risk stratification of patients after myocardial infarction using personalized heart models. Nat. Commun. 2016, 7, 11437. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.W.; Burrington, C.M.; Lynch, D.T.; Davenport, S.K.; Johnson, A.K.; Horsman, M.J.; Chowdhry, S.; Zhang, J.; Sparks, J.D.; Tirrell, P.C. Lipid Metabolism, Oxidative Stress and Cell Death Are Regulated by PKC Delta in a Dietary Model of Nonalcoholic Steatohepatitis. PLoS ONE. 2014, 9, e85848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, H.; Kinugawa, S.; Matsushima, S. Oxidative stress and heart failure. Am. J. Physiol. Circ. Physiol. 2011, 301, H2181–H2190. [Google Scholar] [CrossRef] [Green Version]
- Maksimenko, A.V.; Vavaev, A.V. Antioxidant Enzymes as Potential Targets in Cardioprotection and Treatment of Cardiovascular Diseases. Enzyme Antioxidants: The Next Stage of Pharmacological Counterwork to the Oxidative Stress. Hear. Int. 2012, 7, 3. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxidative Med. Cell. Longev. 2017, 2017, 1–32. [Google Scholar] [CrossRef]
- Linton, M.; Yancey, P.; Davies, S.; Jerome, W.; Vickers, K.C. The Role of Lipids and Lipoproteins in Atherosclerosis; MDText.com, Inc.: South Darthmouth, MA, USA, 2000. [Google Scholar]
- Mozos, I.; Caraba, A. Electrocardiographic Predictors of Cardiovascular Mortality. Dis. Markers 2015, 2015, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Regnier, M. Cardiac troponin structure-function and the influence of hypertrophic cardiomyopathy associated mutations on modulation of contractility. Arch. Biochem. Biophys. 2016, 601, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Ásthildur, A.; Vestergaard, K.R.; Sölétormos, G.; Steffensen, R.; Goetze, J.P.; Iversen, K. Prediction of coronary heart disease or heart failure using high-sensitivity cardiac troponin T: A pilot study. Eur. J. Clin. Investig. 2018, 48, e13009. [Google Scholar]
- Patibandla, S.; Alsayouri, K. Cardiac Enzymes; StatPearls: Petersburg, FL, USA, 2020. [Google Scholar]
- Mythili, S.; Malathi, N. Diagnostic markers of acute myocardial infarction. Biomed. Rep. 2015, 3, 743–748. [Google Scholar] [CrossRef] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Hear. J. 2019, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Welsford, M.; Nikolaou, N.I.; Beygui, F.; Bossaert, L.; Ghaemmaghami, C.; Nonogi, H.; O’Connor, R.E.; Pichel, D.R.; Scott, T.; Walters, D.L.; et al. 2005 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care with treatment recommendations. Circulation 2005, 95, 112. [Google Scholar]
- Solayman, M.; Islam, A.; Paul, S.; Ali, Y.; Khalil, I.; Alam, N.; Gan, S.H. Physicochemical Properties, Minerals, Trace Elements, and Heavy Metals in Honey of Different Origins: A Comprehensive Review. Compr. Rev. Food Sci. Food Saf. 2015, 15, 219–233. [Google Scholar]
- Alvarez-Suarez, J.M.; González-Paramás, A.M.; Santos-Buelga, C.; Battino, M. Antioxidant Characterization of Native Monofloral Cuban Honeys. J. Agric. Food Chem. 2010, 58, 9817–9824. [Google Scholar] [CrossRef]
- Al-Waili, N.S.; Salom, K.; Al-Ghamdi, A.A. Honey for Wound Healing, Ulcers, and Burns; Data Supporting Its Use in Clinical Practice. Sci. World J. 2011, 11, 766–787. [Google Scholar] [CrossRef]
- Alvarez-Suarez, J.M.; Tulipani, S.; Díaz, D.; Estevez, Y.; Romandini, S.; Giampieri, F.; Damiani, E.; Astolfi, P.; Bompadre, S.; Battino, M. Antioxidant and antimicrobial capacity of several monofloral Cuban honeys and their correlation with color, polyphenol content and other chemical compounds. Food Chem. Toxicol. 2010, 48, 2490–2499. [Google Scholar] [CrossRef]
- Ahmad, A.; Alam Khan, R.; Mesaik, M.A. Anti inflammatory effect of natural honey on bovine thrombin-induced oxidative burst in phagocytes. Phytotherapy Res. 2009, 23, 801–808. [Google Scholar] [CrossRef]
- Alvarez-Suarez, J.M.; Giampieri, F.; Damiani, E.; Astolfi, P.; Fattorini, D.; Regoli, F.; Quiles, J.L.; Battino, M. Radical-scavenging Activity, Protective Effect Against Lipid Peroxidation and Mineral Contents of Monofloral Cuban Honeys. Plant Foods Hum. Nutr. 2012, 67, 31–38. [Google Scholar] [CrossRef]
- Alagwu, E.; Okwara, J.; Nneli, R.; Osim, E. Effect of honey intake on serum cholesterol, triglycerides and lipoprotein levels in albino rats and potential benefits on risks of coronary heart disease. Niger. J. Physiol. Sci. 2011, 26, 161–165. [Google Scholar]
- Afroz, R.; Tanvir, E.M.; Karim, N.; Hossain, S.; Alam, N.; Gan, S.H.; Khalil, I. Sundarban Honey Confers Protection against Isoproterenol-Induced Myocardial Infarction in Wistar Rats. BioMed Res. Int. 2016, 2016, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Miran, R.; Nabil, Z.I.; Hussein, A. Cardioactive and Vasoactive Effects of Natural Wild Honey against Cardiac Malperformance Induced by Hyperadrenergic Activity. J. Med. Food 2008, 11, 91–98. [Google Scholar] [CrossRef]
- Busserolles, J.; Gueux, E.; Rock, E.; Mazur, A.; Rayssiguier, Y. Substituting Honey for Refined Carbohydrates Protects Rats from Hypertriglyceridemic and Prooxidative Effects of Fructose. J. Nutr. 2002, 132, 3379–3382. [Google Scholar] [CrossRef] [PubMed]
- Office of Health Assessment and Translation (OHAT). Risk of Bias Assessment Process. In Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; National Institute of Environmental Health Sciences: Research Triangle, NC, USA, 2019; pp. 33–39. [Google Scholar]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (updated July 2019); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2019. [Google Scholar]
- Najafi, M.; Zahednezhad, F.; Samadzadeh, M.; Vaez, H. Zero Flow Global Ischemia-Induced Injuries in Rat Heart Are Attenuated by Natural Honey. Adv. Pharm. Bull. 2012, 2, 165–171. [Google Scholar] [PubMed]
- Vaez, H.; Samadzadeh, M.; Zahednezhad, F.; Najafi, M. Effect of post-ischemic administration of natural honey on ischemia-reperfusion induced infarct size in global ischemia model of isolated rat heart. Res. Pharm. Sci. 2012, 7, 819. [Google Scholar]
- Najafi, M.; Shaseb, E.; Ghaffary, S.; Fakhrju, A.; Eteraf Oskouei, T. Effects of chronic oral administration of natural honey on ischemia/reperfusion-induced arrhythmias in isolated rat heart. Iran. J. Basic Med. Sci. 2011, 14, 75–81. [Google Scholar]
- Eteraf-Oskouei, T.; Shaseb, E.; Ghaffary, S.; Najafi, M. Prolonged preconditioning with natural honey against myocardial infarction injuries. Pak. J. Pharm. Sci. 2013, 26, 681–686. [Google Scholar]
- Gharekhani, A.; Najafi, M.; Ghavimi, H. Acute Administration of Natural Honey Protects Isolated Heart in Normothermic Ischemia. Iran. J. Pharm. Res. IJPR 2012, 11, 1275–1284. [Google Scholar]
- Yaghoobi, N.; Al-Waili, N.; Avan, A.; Parizadeh, S.M.R.; Abasalti, Z.; Yaghoobi, Z.; Yaghoobi, F.; Esmaeili, H.; Kazemi-Bajestani, S.M.R.; Aghasizadeh, R.; et al. Natural Honey and Cardiovascular Risk Factors; Effects on Blood Glucose, Cholesterol, Triacylglycerole, CRP, and Body Weight Compared with Sucrose. Sci. World J. 2008, 8, 463–469. [Google Scholar] [CrossRef]
- Rasad, H.; Entezari, M.H.; Ghadiri, E.; Mehaki, B.; Pahlavani, N. The effect of honey consumption compared with sucrose on lipid profile in young healthy subjects (randomized clinical trial). Clin. Nutr. ESPEN 2018, 26, 8–12. [Google Scholar] [CrossRef]
- Ab Wahab, S.Z.; Hussain, N.H.N.; Zakaria, R.; Kadir, A.A.; Mohamed, N.; Tohit, N.M.; Noor, N.M.; Hassan, I.I.; Noor, N.M. Long-term effects of honey on cardiovascular parameters and anthropometric measurements of postmenopausal women. Complement. Ther. Med. 2018, 41, 154–160. [Google Scholar] [CrossRef]
- Hasenan, S.M.; Karsani, S.; Jubri, Z. Modulation of age related protein expression changes by gelam honey in cardiac mitochondrial rats. Exp. Gerontol. 2018, 113, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.; Tanvir, E.M.; Afroz, R.; Sulaiman, S.A.; Gan, S.H. Cardioprotective Effects of Tualang Honey: Amelioration of Cholesterol and Cardiac Enzymes Levels. BioMed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erejuwa, O.O.; Akpan, J.L.; Uwaezuoke, N.J.; Nwobodo, N.N.; Ezeokpo, B.C.; Erhiano, E.; Araromi, E.J.; Ude, U.N.; Abdulwahab, M.; A Sulaiman, S. Effects of Honey on Postprandial Hyperlipidemia and Oxidative Stress in Wistar Rats: Role of HMG-CoA Reductase Inhibition and Antioxidant Effect. Niger. J. Physiol. Sci. 2018, 33, 129–138. [Google Scholar] [PubMed]
- Al-Waili, N. Natural Honey Lowers Plasma Glucose, C-Reactive Protein, Homocysteine, and Blood Lipids in Healthy, Diabetic, and Hyperlipidemic Subjects: Comparison with Dextrose and Sucrose. J. Med. Food 2004, 7, 100–107. [Google Scholar] [CrossRef]
- Martina, S.J.; Ramar, L.A.P.; Silaban, M.R.I.; Luthfi, M.; Govindan, P.A.P. Antiplatelet Effectivity between Aspirin with Honey on Cardiovascular Disease Based on Bleeding Time Taken on Mice. Open Access Maced. J. Med. Sci. 2019, 7, 3416–3420. [Google Scholar]
- Cakmak-Arslan, G.; Selin, E.M.; Pinar, G.R.; Kekecoglu, M. Investigation of the Toxic Effects of Rhododendron Honey on Mouse Cardiac Muscle Tissue Lipids at Molecular Level. Kafkas Univ. Vet. Fak. Dergisi. 2020, 26, 287–294. [Google Scholar]
- Abdulrhman, M.A.; Mamdouh, N.A.; El Guindy, W.M.; Faraj, S.A.K. Effects of honey supplementation on children with idiopathic dilated cardiomyopathy: A randomized single blinded controlled study. World J. Pharm. Res. 2018, 7, 19–34. [Google Scholar]
- Wu, J.; Xun, N.; Yang, Y.; Zeng, L.; Li, Z.; Yang, W.; Liang, Y.; Tang, H.; Ma, Z. Chrysin attenuates myocardial ischemia–reperfusion injury by inhibiting myocardial inflammation. RSC Adv. 2018, 8, 13739–13746. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Xiong, J.; Zou, Q.; Wang, D.-D.; Huang, C. Chrysin attenuates interstitial fibrosis and improves cardiac function in a rat model of acute myocardial infarction. J. Mol. Histol. 2018, 49, 555–565. [Google Scholar] [CrossRef]
- Rani, N.; Bharti, S.; Bhatia, J.; Nag, T.; Ray, R.; Arya, D.S. Chrysin, a PPAR-γ agonist improves myocardial injury in diabetic rats through inhibiting AGE-RAGE mediated oxidative stress and inflammation. Chem. Interact. 2016, 250, 59–67. [Google Scholar] [CrossRef]
- Dong, F.; Zhang, J.; Zhu, S.; Lan, T.; Yang, J.; Li, L. Chrysin Alleviates Chronic Hypoxia–Induced Pulmonary Hypertension by Reducing Intracellular Calcium Concentration in Pulmonary Arterial Smooth Muscle Cells. J. Cardiovasc. Pharmacol. 2019, 74, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Veerappan, R.; Malarvili, T. Chrysin Pretreatment Improves Angiotensin System, cGMP Concentration in L-NAME Induced Hypertensive Rats. Indian J. Clin. Biochem. 2018, 34, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, T.; Zhang, C.; Wu, G.; Wan, W.; Liang, J.; Liu, X.; Liu, D.; Yang, B. Pinocembrin attenuates autonomic dysfunction and atrial fibrillation susceptibility via inhibition of the NF-κB/TNF-α pathway in a rat model of myocardial infarction. Int. Immunopharmacol. 2019, 77, 105926. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Xu, J.; Hu, W.; Yu, N.; Bai, X. Effects of Pinocembrin Pretreatment on Connexin 43 (Cx43) Protein Expression after Rat Myocardial Ischemia-Reperfusion and Cardiac Arrhythmia. Med. Sci. Monit. 2018, 24, 5008–5014. [Google Scholar] [CrossRef]
- Zhang, G.; Zhao, Z.-Y.; Hu, H.-J.; Yang, J.; Gu, G. Effect of pinocembrin pre-treatment on expressions of Cx43 protein and claudin 1 in myocardial ischemia cardiomyocytes of arrhythmic rats. Trop. J. Pharm. Res. 2018, 17, 415. [Google Scholar] [CrossRef] [Green Version]
- Kris-Etherton, P.; Eckel, R.H.; Howard, B.V.; Jeor, S.S.; Bazzarre, T.L. Lyon Diet Heart Study. Circulation 2001, 103, 1823–1825. [Google Scholar] [CrossRef] [Green Version]
- Sime, D.; Atlabachew, M.; Abshiro, M.R.; Zewde, T. Total phenols and antioxidant activities of natural honeys and propolis collected from different geographical regions of Ethiopia. Bull. Chem. Soc. Ethiop. 2015, 29, 163. [Google Scholar] [CrossRef] [Green Version]
- Dong, R.; Zheng, Y.; Xu, B. Phenolic Profiles and Antioxidant Capacities of Chinese Unifloral Honeys from Different Botanical and Geographical Sources. Food Bioprocess Technol. 2011, 6, 762–770. [Google Scholar] [CrossRef]
- Akyol, E.; Selamoglu, Z.; Dogan, H.; Akgul, H.; Unalan, A. Determining the total antioxidant status and oxidative stress indexes of honey samples obtained from different phytogeographical regions in Turkey. Fresenius Environ. Bull. 2015, 24, 1204–1208. [Google Scholar]


{kind=link}
| Honey improves Lipid Metabolism | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [41] | Normal male mice (n = 18) | Intragastric delivery of 25 or 50 mg/kg Rhododendron honey 24 h before analysis. |
| Administration of 50 mg/kg but not 25 mg/kg honey caused significant changes in the lipid molecules. | Consumption of honey causes significant toxic effects on cardiac muscle tissue lipids. |
| [38] | Wistar rats fed with high-fat diet or portable water (n = 25) | Oral delivery of 1 g/kg Nigerian honey 5 or 60 min prior to administration of high-fat diet. |
| Honey pretreatment resulted in significantly higher post-prandial HDL, cholesterol, and HMG-CoA: mevalonate while significantly lowered post-prandial LDL and cholesterol. | Pretreatment of honey has post-prandial antihyperlipidemic effect. |
| [22] | Normal adult male albino rats (n = 20) | 10% (v/v) Nigerian honey (Nigeria) added to the rat drinking water for 22 weeks. |
| Treatment of honey reduced the level of VLDL, LDL, TG, CVPI, plasma cholesterol, TC, and HDL. | Honey administration reduced risk of coronary heart disease in male albino rats. |
| [23] | Isoproterenol (ISO)-induced myocardial injury model in adult Wistar rats (n = 72) | 5 g/kg oral Sundarban honey (Bangladesh) for 6 weeks. |
| Treatment of honey restores the ISO-induced elevation of cardiac troponin, cardiac enzymes, serum lipid profile, and lipid peroxidation. | Sundarban honey confers protection against ISO-induced oxidative stress in the myocardium. |
| Honey antioxidative effects | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [25] | Fructose-induced hypertriglyceridemic and oxidation in Weaning male Wistar rats (n = 27). | 65 g/100 g oral Ceyrat honey (France) in normal rat feed for 2 weeks. |
| Treatment of honey lead to decreased TG, higher α-tocopherol level, lower plasma nitrite and nitrate concentrations, lower lipid peroxidation, and lower TBARS. | Substituting honey for refined carbohydrates protects from hypertriglyceridemia and prooxidative effects of Fructose in nutritional diet. |
| [20] | Human neutrophils or rodent peritoneal macrophages stimulated with various concentrations of bovine thrombin (0.5 to 0.0002 units/mL). | 0.03 to 15 mg/ml of six honey samples: Clover honey (America), Capilano honey (Australia), Langnease honey (Germany), Al-Shafa honey (Pakistan), Swat honey (Pakistan), Sidder honey (Pakistan). |
| Treatment of 1 mg/mL honey completely suppressed oxidative activities. | Natural honey suppression of oxidation could be extremely beneficial by attenuating the progress of cardiovascular disease. |
| Honey modulates blood pressure | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [40] | Double Ditsch Webster mice (n = 32) | High Desert® 75 mg honey oral for 12 days. |
| Treatment of honey resulted in slower bleeding time as compared to the control. | Honey has an antiplatelet effect in mice. |
| [24] | Epinephrine-induced cardiac and vasomotor dysfunction in adult male Sprague–Dawley albino rats (n = 30). | 5 g/kg intraperitoneal honey (Saint Katherine Protectorate, Southern Sinai, Egypt). |
| Treatment of honey reverses epinephrine-induced elevation of VBP, abnormalities in extrasystoles, tachyarrhythmias, bradyarrhythmia, and decreased in total antioxidant capacity. | Honey has a cardioactive and vasoactive effect that can play a crucial role as a cardioprotective agent. |
| Honey ameliorates cardiac arrhythmia | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [30] | Ischemia and reperfusion cycle myocardial injury model in male Wistar rats (n = 50–70). | 1, 2, and 4% (v/v) honey (Oskou, East Azerbaijan, Iran) added in rats drinking water for 45 days. |
| Treatment of honey reduced the number of VT, VEBs and incidence of VT, total VF incidence and duration of reversible VF following reperfusion cycle. | Long-term oral administration of honey can recover ischemic-reperfused isolated rat hearts and consequently has anti-arrhythmic activity. |
| [31] | Ischemia and reperfusion cycle myocardial injury model in male Wistar rats (n = 40–56). | 1, 2, and 3% (v/v) honey (Oskou, East Azerbaijan, Iran) added in rats drinking water for 45 days. |
| Treatment of honey reduced infarct size, VT, VEB, incidence of VT and total VF following reperfusion cycle. | Honey showed cardioprotective effects in in vivo long-term pretreatment following myocardial infarction. |
| Honey reduces myocardial infarct area | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [29] | Ischemia and reperfusion cycle myocardial injury model in male Wistar rats (n = 50–70). | 0.25%, 0.5%, 1%, and 2% (v/v) honey (Oskou, East Azerbaijan, Iran) added in rats drinking water for 45 days. |
| Treatment of honey reduced the number of single ectopic and reduced number of arrhythmias, the total number of VEBs and duration of VT, and percentage of infarct size and infarcted volume following reperfusion cycle. | Post-ischemic administration of natural honey in global ischemia showed protective effects against ischemia/reperfusion (I/R) injuries in isolated rat heart. |
| [32] | Ischemia and reperfusion cycle myocardial injury model in male Sprague-Dawley rats (n = 32–40). | 0.125%, 0.25%, 0.5%, and 1% (v/v) honey (Oskou, East Azerbaijan, Iran) added in rats drinking water for 45 days. |
| Treatment of honey reduced the number, the duration and the incidence of recorded arrhythmias, the duration and the incidence of VT and reversible VF, number of VEBs and VT and the time spent in reversible VF and VT, the duration and the incidence of reversible VF and total VF following reperfusion cycle. | The long-term administration of natural honey also caused significant cardioprotection against the myocardial infarction. |
| [37] | ISO-induced myocardial injury model in adult Wistar albino rats (n = 40) | 3 g/kg oral Tualang honey (Malaysia) for 45 days. |
| Treatment of honey reverses ISO-induced heart enlargement, elevation of cardiac troponin, cardiac enzymes, serum total cholesterol, and triglyceride, as well as decreased antioxidant activity. | Cardioprotection of Tualang honey against cardiovascular diseases. |
| Honey modulates age-related protein expression | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [36] | Young (2 months) and old (19 months) Sprague–Dawley male rats (n = 12). | 2.5 g/kg oral Gelam honey (Malaysia) for 8 months. |
| Treatment of honey restores the decreased expression of protein related to oxidative phosphorylation caused by aging such as ATP synthase, NADH dehydrogenase, and superoxide dismutase. | Gelam honey provides protective effect on cardiac tissue of aged rats by modulating age-related protein expressions. |
| Chrysin improves myocardial injury | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [43] | The left coronary artery of adult male Sprague-Dawley rats was ligated to induced acute myocardial infarction. (n = 30) | 50 mg/kg intragastric chrysin daily for 5 days. |
| Chrysin reduced artery ligation-induced infarct size, inflammatory cells in the myocardial tissue, elevation of inflammatory cytokines and elevation of cardiac marker enzymes. | Chrysin attenuates myocardial injury by inhibiting myocardial inflammation. |
| [44] | The left anterior descending coronary artery of adult male Sprague–Dawley rats was ligated to induced acute myocardial infarction. | 40 mg/kg oral for4 weeks. |
| Chrysin improves cardiac systolic function, alleviates oxidative stress, alleviates interstitial and perivascular fibrosis, reduces the expression of type I collagen, reduces the NF-KB p65 level and p-IKKβ/IKKβ ratio, reduces the expression levels of c-Fos and c-Jun, reduces ANGII-induced up-regulation of type I and type III collagen levels | Chrysin inhibits myofibroblast transformation and collagen synthesis, prevents myocardial fibrosis, and improves cardiac function. |
| [45] | Streptozotocin-induced diabetic male albino Wistar rats challenged with ISO to induce myocardial injury (n = 75). | 60 mg/kg oral chrysin for 28 days. |
| Treatment with chrysin restores the ISO-induced ventricular and myocardium damage, elevation of oxidative stress, cardiac injury markers, and apoptosis effect. | Chrysin ameliorated ISO-induced myocardial injury in diabetic rats through PPAR-γ activation. |
| Chrysin regulates blood pressure | |||||
| Ref | Experimental Model/Study Population | Honey Treatment | Outcome Measures | Result | Conclusion |
| [46] | Pulmonary hypertension was established in Sprague–Dawley rats via exposure to chronic hypoxia (n = 20) | 100-mg/kg chrysin injected via subcutaneous daily for 21 days. |
| Chrysin resulted in reversal of the hypoxia-induced RVSP and mRVP decline while attenuating right ventricular hypertrophy and increasing levels of hypoxia-related genes and proteins. | Chrysin display cardioprotective effect in hypoxia-induced pulmonary hypertension. |
| [47] | Nω-nitro-L-arginine methyl ester (L-NAME)-induced hypertension in male Wistar rats (n = 24) | 25 mg/kg oral for4 weeks. |
| Chrysin treatment reverses the L-NAME-induced elevated left ventricular functions and Ang-II while increases the cardiac HO-1 and cGMP levels. | Chrysin exerts antihypertensive effects via angiotensin system. |
| Pinocembrin ameliorates cardiac arrhythmia | |||||
| Ref | Experimental Model | Honey Treatment | Outcome Measures | Result | Conclusion |
| [48] | The left anterior descending coronary artery of adult male Sprague–Dawley rats was ligated to induced acute myocardial infarction (n = 106) | 5 mg/kg pinocembrin intravenous daily for 6 days before injection of E. coli. |
| Pinocembrin treatment significantly improved HRV, shortened atrial AL, prolonged atrial ERP, attenuated atrial fibrosis, and decreased concentrations of norepinephrine (NE), tumor necrosis factor-α (TNF-α), interleukin (IL)-1β and IL-6, increased expression of Cx43 and Cav1.2 and suppressed the phosphorylation of IκBα and p65. | Pinocembrin is protective against atrial arrhythmia. |
| [49] | The left anterior descending coronary artery of adult male Sprague–Dawley rats was ligated to induced acute myocardial infarction (n = 45) | 30 mg/kg pinocembrin intravenous 10 min before ligation. |
| Pinocembrin alleviates the surgical-induced reduction of HR, MAP, RPP, Na+-K+-ATPase activities, Ca2+-Mg2+-ATPase activities, Cx43, and Kir2.1 while attenuating the surgical-induced increase in arrhythmia index and CK-MB and cTnI levels. | Pinocembrin alleviated ventricular arrhythmia in artery ligation-induced myocardial infarction in rats. |
| [50] | Ischemia and reperfusion cycle myocardial injury model in male Sprague–Dawley rats. | 3, 10, or 30 mg/kg pinocembrin injected intravenously before ischemia. |
| Pinocembrin increases HR, MAP, RPP, Na+-K+-ATPase activities, Ca2+-Mg2+-ATPase activities, Cx43, ZO-1, and Kir2.1 while lowers the levels of CK-MB and cTnI. | Pinocembrin ameliorates ventricular arrhythmia in ischemia/reperfusion model in rats. |
| Randomized Controlled Trial | |||||
| Ref | Study Population | Honey Treatment | Outcome Measures | Result | Conclusion |
| [33] | Overweight or obese students from Mashhad University of Medical Science, Iran aged between 20 to 60 years old (n = 60). | 70 g of oral natural unprocessed honey (Iran) dissolved in 250 mL tap water for a maximum of 30 days. |
| Treatment of honey reduced the BMI, serum TG, CRP, TC, and LDL after 30 days. | Consumption of honey reduces cardiovascular risk factors in overweight and obese adults. |
| [34] | Healthy male students of Isfahan University of Medical Sciences, Isfahan, Iran (n = 60). | 70 g of oral natural honey (Iran) dissolved in 250 ml tap water for 6 weeks. |
| Treatment of honey reduced TC but increased TG and HDL after 6 weeks. | Consumption of honey reduces cardiovascular risk factors in healthy male adults. |
| [35] | Postmenopausal women visiting outpatient clinics of Hospital Universiti Sains Malaysia (n = 100). | 20 g oral Tualang honey (Malaysia) daily for 12 months. |
| Treatment with honey reduced DBP and fasting blood glucose out of all the cardiovascular outcomes measured. SBP and lipid profile remain similar to the control. | Tualang honey supplementation reduces diastolic blood pressure and fasting blood glucose. |
| [42] | Children suffering from idiopathic dilated cardiomyopathy aged between 2 to 12 years old (n = 54). | 1.2 g/kg oral Ziziphus honey (Yemen) daily for threeMonths, in addition to the standard heart failure medical therapy. |
| EF and FS increased significantly in the honey group as compared with the control group | Honey consumption resulted in significant improvement in the EF and FS in a group of children suffering from IDCM. |
| Non-Randomized Controlled Trial | |||||
| Ref | Study Population | Honey Treatment | Outcome Measures | Result | Conclusion |
| [39] | Healthy and diabetic staff from the Dubai Specialized Medical Center and Medical Research Laboratories aged between 25 to 42 years old (n = 48) | 90 g of oral natural honey (United Arab Emirates) dissolved in 250 mL drinking water for a maximum of 15 days. |
| Treatment of honey reduced level of plasma glucose, insulin, CRP, TC, LDL, and TG levels but caused elevation of HDL in healthy and diabetic subjects as early as 30 min, up to 15 days. | Consumption of honey reduces cardiovascular risk factors in healthy and diabetic adults. |
| [17] | [19] | [20] | [21] | [22] | [26] | [27] | [28] | [29] | [33] | [34] | [35] | [37] | [38] | [40] | [41] | [42] | [43] | [44] | [45] | [46] | [47] | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Numbers across groups were matched | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| Concealment of exposure allocation | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | ||
| Appropriate comparison group | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | ||
| Absence of confounding factors | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | ||
| Performance | Identical experimental condition across groups | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| Blinded outcome assessor | - | - | - | - | - | - | - | - | - | - | + | + | + | + | + | + | + | + | + | + | + | ||
| Attrition | Outcome data were complete with no exclusion from analysis | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| Detection | Appropriate exposure assessment | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| Appropriate outcome assessment | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | ||
| Reporting | All measured outcomes were reported | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| Overall risk of bias | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low | |
| [30] | [31] | [32] | [36] | [39] | ||
|---|---|---|---|---|---|---|
| Selection | Random sequence generation | + | + | + | - | + |
| Allocation concealment | + | + | + | - | - | |
| Performance | Blinding of personnel | + | + | + | - | + |
| Blinding of participants | + | + | + | - | - | |
| Detection | Blinding outcome assessments | + | + | + | + | + |
| Attrition | Incomplete outcome data | + | + | + | + | + |
| Reporting | Selective reporting | + | + | + | + | + |
| Overall risk of bias | Low | Low | Low | Moderate | Low | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bt Hj Idrus, R.; Sainik, N.Q.A.V.; Nordin, A.; Saim, A.B.; Sulaiman, N. Cardioprotective Effects of Honey and Its Constituent: An Evidence-Based Review of Laboratory Studies and Clinical Trials. Int. J. Environ. Res. Public Health 2020, 17, 3613. https://doi.org/10.3390/ijerph17103613
Bt Hj Idrus R, Sainik NQAV, Nordin A, Saim AB, Sulaiman N. Cardioprotective Effects of Honey and Its Constituent: An Evidence-Based Review of Laboratory Studies and Clinical Trials. International Journal of Environmental Research and Public Health. 2020; 17(10):3613. https://doi.org/10.3390/ijerph17103613
Chicago/Turabian StyleBt Hj Idrus, Ruszymah, Nur Qisya Afifah Veronica Sainik, Abid Nordin, Aminuddin Bin Saim, and Nadiah Sulaiman. 2020. "Cardioprotective Effects of Honey and Its Constituent: An Evidence-Based Review of Laboratory Studies and Clinical Trials" International Journal of Environmental Research and Public Health 17, no. 10: 3613. https://doi.org/10.3390/ijerph17103613