Digital Undergraduate Education in Dentistry: A Systematic Review



Abstract
:1. Introduction
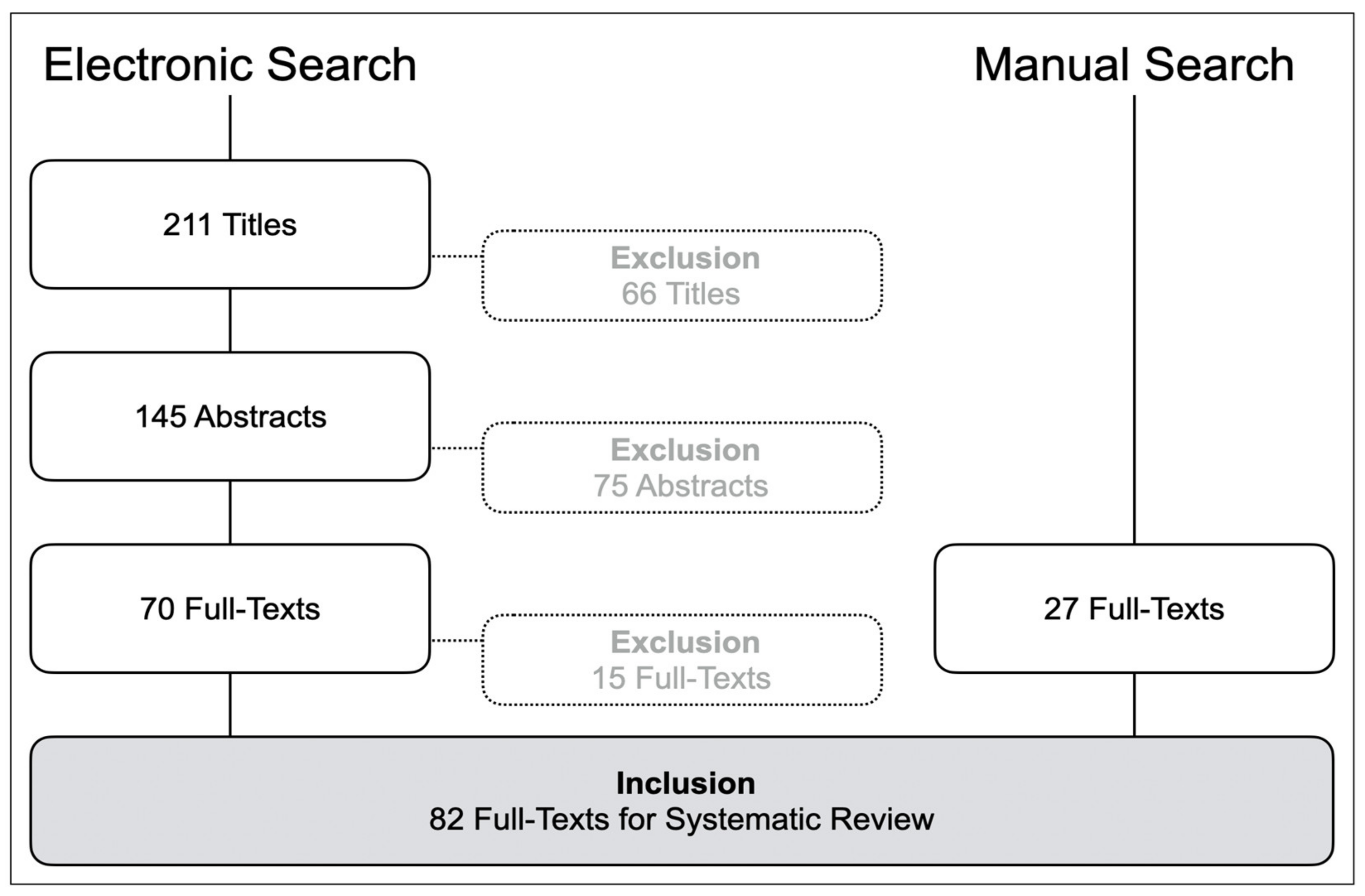
2. Materials and Methods
3. Results
- Web-based knowledge transfer/e-learning (22 studies);
- Digital surface mapping (20 studies);
- Dental simulator motor skills including IOS (23 studies);
- 3D printing and prototyping (2 studies);
- Digital radiography (5 studies); and
- Surveys related to the penetration and acceptance of digital education (10 studies).
3.1. Web-Based Knowledge Transfer/e-Learning
3.2. Digital Surface Mapping
3.3. Dental Simulator Motor Skills Including Intraoral Optical Scanning

{kind=link}
| Study (Year) | Study Design | Theory / Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Quinn et al. 2003 [65] | RCT | P | 20 | Compared students’ performance in preparing class I amalgam cavity on a VR-based training unit; test group had virtual real-time feedback and software evaluation, control group had clinical instructor available during preparation. Anonymous scoring by 2 faculties, criteria: outline form, retention form, smoothness, cavity depth and cavity margin angulation. Questionnaire feed-back in test group. | Similar results for retention and wall angulation, while outline form, smoothness and cavity depth scored better in control. Test group assessed software as superior for immediate feed-back, self-paced learning, consistency of evaluation, encouraging independent work and more thorough assessment, while conventional training was superior for increasing confidence in cavity preparation. VR-based training should be used as adjunct but not replacing conventional training methods. |
| Jasinevicius et al. 2004 [64] | CT | P | 28 | Compared students’ performance in amalgam and crown preparations on typodont teeth either with a contemporary non-computer-assisted simulation system (CS), or with a virtual reality computer-assisted simulation system (VR). Both groups were provided with presentations describing preparations, CS group received handouts, VR group had preparation criteria available on the computer. Student-faculty (S-F) interaction time was logged. | Preparation quality did not differ between CS and VR. CS required 2.8 h, VR 0.5 h S-F. CS received five times more instructional time from faculty than VR. |
| LeBlanc et al. 2004 [60] | RCT | P | 68 | Compared students’ technical skills in preclinical operative dentistry after standard traditional laboratory-based instructions (over 110 h) and additional virtual reality simulator-enhanced training (test group with 20 students) Simulator (DentSim, DenX) provided real-time feedback, training conducted during 6–10 h in 3 blocks over 8 months. | While all students improved in the 4 tests during the year, test students tended to better scores in the final exam. Virtual reality simulators can be implemented in the traditional training of future dentists. |
| Rees et al. 2007 [54] | CT | P | 16 | Evaluated simulator training (DentSim, DenX) by undergraduate students for Class I and II preparations (time, marks, number of evaluations), students spent 6 h cutting an unlimited number of Class I cavities and Class II cavities; feedback by questionnaire. | Class I preparations obtained a mean mark of 66.8, preparation time was 12.5 min, with 6.7 evaluations; Class II had a mark of 26.5, time 18 min, with 7.0 evaluations. Class II was more difficult to cut. Students appreciated easy change of teeth, working at their own pace and examine the cavity in a cross-section. |
| Welk et al. 2008 [55] | OT | P/T | 80 | Evaluated students’ performance in operative dentistry after training with computer-assisted dental simulator (DentSim, DenX), feedback by questionnaire. | Students indicated high interest in simulator training, high acceptance and response to additional elective training time in the computer assisted simulation lab. The shift in curriculum and instructional goals has to be optimized continuously. |
| Urbankova et al. 2010 [58] | RCT | P | 75 | Evaluated adjunctive computerized dental simulator (CDS; DentSim) training (8 h) in operative dentistry (Class I and II preparations): either before (n = 26) or after 1st exam (n = 13); control group (n = 36) with traditional preclinical dental training alone (110 h). | CDS-trained students performed better than control in the 1st and 2nd exam, no difference between pre-exam and post-exam groups. In the 3rd exam (end of the year) CDS group had higher, but not significantly different scores than control. |
| Pohlenz et al. 2010 [57] | CT | P | 53 | Evaluated VR training (Voxel-Man) for virtual apicoectomy; questionnaire about simulated force feedback, spatial 3D perception, resolution and integration of further pathologic conditions. | 92.7% recommended the virtual simulation as additional modality in dental education, 81.1% reported the simulated force feedback as good or very good, 86.8% evaluated 3D spatial perception as good or very good; 100% recommended integration of further pathologies. |
| Gottlieb et al. 2011 [59] | CT | T | 202 | Evaluated VR simulation training (DentSim, Image Navigation Ltd.) in operative preparations and restorations, 60 h VR training, laboratory course was reduced to 234 h (instead of traditional 304h). 13 experienced faculties assessed 97 non-VR students (1st year, control) and 105 students with 1 semester VR experience (test); survey about students’ abilities in ergonomics, confidence level, performance, preparation, and self-assessment. | Faculty expected greater psychomotor skills and ability to prepare teeth in VR, abilities were lower than anticipated but numerically higher than in non-VR students. Faculty members perceived students’ ergonomics in the test group better than in control. |
| Ben-Gal et al. 2011 [56] | CT | P | 33 | Evaluated use of VR simulator (IDEA Dental) for dental instruction, self-practice, and student evaluation. 21 experienced dental educators, 12 randomly selected experienced dental students (5th year) performed 5 drilling tasks using the simulator, feed-back by questionnaire. | Both groups found that the simulator could provide significant benefits in teaching and self-learning of manual dental skills. |
| Ben-Gal et al. 2013 [63] | CT | P | 106 | Evaluated potential of VR training simulator (IDEA Dental) to assess manual dexterity in 63 dental students, 28 dentists, 14 non-dentists, performed virtual drilling tasks in different geometric shapes: time to completion, accuracy, number of trials to successful completion, score provided by the simulator. | Simulator scoring algorithm showed high reliability in all parameters and was able to differentiate between non-professionals and dental students or non-professionals and dentists. |
| Lee & Gallucci 2013 [73] | CT | P | 30 | Compared digital (IOS) to conventional impression for single implant restorations, evaluated efficiency, difficulty and students’ preference. | Mean total treatment time, preparation time and working time were significantly longer for conventional than for IOS; conventional impressions were assessed as more difficult than IOS; 60% preferred IOS, 7% conventional, 33% either techniques |
| Kikuchi et al. 2013 [62] | RCT | P | 43 | Compared VR simulator (DentSim) training with or without instructor feedback for preparation of porcelain fused to metal (PFM) crown preparation. 43 students (5th year). randomly divided into: 1. VR group with instructor’s feedback (DSF; n = 15); 2. VR without instructor’s feedback (DS; n = 15); 3. neither VR simulator training nor faculty feedback (NDS; n = 13); preparation time and scores of 4 crown preparations (1week for 4 weeks). | DSF and DS had significantly higher total scores than NDS. Similar results in DSF and DS, but shortened preparation time with instructors’ feed-back (DSF) at early stages. |
| Douglas et al. 2014 [69] | CT | P | 50 | Compared students’ performance in traditional waxing vs. computer-aided crown designing (IOS with CEREC 3D, Sirona Dental Systems), faculty grading of occlusal contacts and anatomic form, feed-back by questionnaire. | Similar gradings for wax design (79.1) and crown design (78.3); more occlusal contacts with CAD; students enjoyed designing a full contour crown using CAD and required less time with CAD. Students recognized limits of CAD technology in representing anatomic contours and excursive occlusion compared to conventional wax techniques. |
| Wang et al. 2015 [66] | CT | P | 20 | Compared VR simulator (iDental with Phanotm Omni, SensAble Tech. Inc.) in novice group (graduate students with less than 3 years clinical practice experience) and resident group (with 3–0 years clinical practice); assessment of caries removal, pulp chamber opening, time and amount of removed healthy/unhealthy tissue; feed-back by a questionnaire. | No differences in time and amount of tissue removal between groups; residents spend slightly more time than students; both groups suggested improvements in spatial registration precision, more realistic model with material properties and force feedback of different tissues, improvement of the depth of the virtual space. |
| Schwindling et al. 2015 [68] | CT | P | 56 | Evaluated a CAD/CAM hands-on course (test) compared to video-supported lecture only (control); written exam about cast digitizing and zirconia crown designing. | Test group performed significantly better than controls (16.8/20 vs. 12.5/20 correct answers); interest of students in CAD/CAM was higher after hands-on course. |
| Kattadiyil et al. 2015 [75] | CCS | P | 15 | Compared clinical treatment outcomes, patient satisfaction, and dental student preferences for digital (AvaDent, two appointments) and conventional (five appointments) complete dentures (CD) in 15 patients, 15 dental students fabricated two sets of CDs for each patient. Faculty and patient ratings, patient and student preferences, perceptions, treatment time was analyzed. | Digital process was equally effective and more time-efficient than conventional; faculty scored digital better than conventional dentures; patients and students preferred digital dentures. |
| Zitzmann et al. 2017 [72] | RCT | P | 50 | Investigated performance (time recording) and perception (questionnaire feedback) of IOS and conventional implant impression after video teaching. | Students rated conventional impressions as more difficult (VAS 46) than IOS (VAS 70), with greater patient-friendliness of IOS (VAS 83) compared to conventional impressions (VAS 36); 76% preferred digital, 88% felt most effective with IOS; total work time of all steps was significantly shorter with 301 sec. for IOS and 723 sec. for conventional impressions. |
| Wegner et al. 2017 [70] | OT | P | 108 | Evaluated students’ perception (questionnaire feedback) of IOS (Lava Cos Training, 3M Espe), scanning of 3 typodont tooth preparations. | 63.9% positive opinion, 60.2% considered scanning process as manageable, 55.6% profited from magnified view of their preparation to understand chamfer finish lines. |
| Marti et al. 2017 [74] | RCT | P | 25 | Analyzed time to instruct IOS (DS; LAVA C.O.S. digital impression system) and conventional impression technique (CI; polyvinyl siloxane) with video lecture, investigator led demonstration, and independent impression exercise: time recording and questionnaire about familiarity and student’s expectations. | Teaching DS required significantly more time than CI for video lecture (16 vs. 10 min), demonstration time (9 vs 5 min) and impression time (18 vs. 9 min). Initially students were more familiar with CI (3.96) than DS (1.96) technique. After instructions and practice, CI technique proved significantly easier than expected. Manageability of DS was not influenced by the instruction and practice experience. 96% expressed an expectation that DS will become their predominant impression technique. |
| de Boer et al. 2019 [67] | RCT | P | 126 | Investigated skill transfer between various levels of force feedback (FFB) using Simodont dental trainer (Moog) for cross-figure preparations as manual dexterity exercise. Assessment of students’ satisfaction by questionnaire. | Longer practice time was correlated with test performance: students passing at different FFB levels had mean of 300h, those passing in one FFB level had 271 h, failing students had 224 h. Skill transfer from one level of FFB to another was feasible with sufficient training. |
| Schott et al. 2019 [71] | OT | P | 31 | Evaluated dental students’ perception of IOS compared to conventional alginate impression; survey after basic training and self-practicing. | 77% (24) students were overall “very” or “rather satisfied" with the handling of IOS; 58% preferred IOS from the dentist’s perspective, no significant difference from the patient’s perspective but reduced comfort related to the impression tray. |
| Murbay et al. 2020 [61] | RCT | P | 32 | Incorporated VR with Moog Simodont dental trainer in preclinical training; students performed an occlusal preparation on typodont teeth and had previous exposure to VR (group 1) or no VR exposure (group 2); assessment was conducted (satisfactory / unsatisfactory) by manual approach or digital (Magic 19.01 64-bit). | VR use improved preparation significantly with 75% (12/16) satisfactory preparations in group 1 and 44% (7/16) in group 2. Manual and digital evaluation methods did not differ significantly. |
| Murrell et al. 2019 [76] | OT | P | 288 | Evaluated completion of posterior crown planning with or without presenting the situation to the patient by intraoral camera use; 51 students completed 198 surveys, 35 faculty members with 64 surveys, 202 patient surveys, survey was voluntary and camera use optional. | Positive perception of intraoral camera use by students and patients, while faculty was neutral; significantly higher completion rate when intraoral camera was used. |
3.4. 3D Rapid Prototyping
3.5. Digital Radiography
3.6. Surveys Related to the Penetration and Acceptance of Digital Education
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fernandez, M.A.; Nimmo, A.; Behar-Horenstein, L.S. Digital Denture Fabrication in Pre- and Postdoctoral Education: A Survey of U.S. Dental Schools. J. Prosthodont. 2016, 25, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Prager, M.C.; Liss, H. Assessment of Digital Workflow in Predoctoral Education and Patient Care in North American Dental Schools. J. Dent. Educ. 2019. [Google Scholar] [CrossRef]
- Joda, T.; Lenherr, P.; Dedem, P.; Kovaltschuk, I.; Bragger, U.; Zitzmann, N.U. Time efficiency, difficulty, and operator’s preference comparing digital and conventional implant impressions: A randomized controlled trial. Clin. Oral Implant. Res. 2017, 28, 1318–1323. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Ferrari, M.; Bragger, U.; Zitzmann, N.U. Patient Reported Outcome Measures (PROMs) of posterior single-implant crowns using digital workflows: A randomized controlled trial with a three-year follow-up. Clin. Oral Implant. Res. 2018, 29, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Muhlemann, S.; Sandrini, G.; Ioannidis, A.; Jung, R.E.; Hammerle, C.H.F. The use of digital technologies in dental practices in Switzerland: A cross-sectional survey. Swiss Dent. J. 2019, 129, 700–707. [Google Scholar]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Goodacre, C.J. Digital Learning Resources for Prosthodontic Education: The Perspectives of a Long-Term Dental Educator Regarding 4 Key Factors. J. Prosthodont. 2018, 27, 791–797. [Google Scholar] [CrossRef]
- De Boer, I.R.; Wesselink, P.R.; Vervoorn, J.M. The creation of virtual teeth with and without tooth pathology for a virtual learning environment in dental education. Eur. J. Dent. Educ. 2013, 17, 191–197. [Google Scholar] [CrossRef]
- Joda, T.; Gallucci, G.O.; Wismeijer, D.; Zitzmann, N.U. Augmented and virtual reality in dental medicine: A systematic review. Comput. Biol. Med. 2019, 108, 93–100. [Google Scholar] [CrossRef]
- Towers, A.; Field, J.; Stokes, C.; Maddock, S.; Martin, N. A scoping review of the use and application of virtual reality in pre-clinical dental education. Br. Dent. J. 2019, 226, 358–366. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Komolpis, R.; Johnson, R.A. Web-based orthodontic instruction and assessment. J. Dent. Educ. 2002, 66, 650–658. [Google Scholar] [PubMed]
- Bains, M.; Reynolds, P.A.; McDonald, F.; Sherriff, M. Effectiveness and acceptability of face-to-face, blended and e-learning: A randomised trial of orthodontic undergraduates. Eur. J. Dent. Educ. 2011, 15, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.F.; Hendricson, W.D. Evaluation of a 3-D interactive tooth atlas by dental students in dental anatomy and endodontics courses. J. Dent. Educ. 2010, 74, 110–122. [Google Scholar] [PubMed]
- Mitov, G.; Dillschneider, T.; Abed, M.R.; Hohenberg, G.; Pospiech, P. Introducing and evaluating MorphoDent, a Web-based learning program in dental morphology. J. Dent. Educ. 2010, 74, 1133–1139. [Google Scholar] [PubMed]
- Curnier, F. Teaching dentistry by means of virtual reality—The Geneva project. Int. J. Comput. Dent. 2010, 13, 251–263. [Google Scholar]
- Kingsley, K.V.; Kingsley, K. A case study for teaching information literacy skills. BMC Med. Educ. 2009, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, S.M.; Gadbury-Amyot, C.C. Using Twitter for Teaching and Learning in an Oral and Maxillofacial Radiology Course. J. Dent. Educ. 2016, 80, 149–155. [Google Scholar]
- Vuchkova, J.; Maybury, T.; Farah, C.S. Digital interactive learning of oral radiographic anatomy. Eur. J. Dent. Educ. 2012, 16, e79–e87. [Google Scholar] [CrossRef]
- Schultze-Mosgau, S.; Zielinski, T.; Lochner, J. Web-based, virtual course units as a didactic concept for medical teaching. Med. Teach. 2004, 26, 336–342. [Google Scholar] [CrossRef]
- Qi, S.; Yan, Y.; Li, R.; Hu, J. The impact of active versus passive use of 3D technology: A study of dental students at Wuhan University, China. J. Dent. Educ. 2013, 77, 1536–1542. [Google Scholar] [PubMed]
- Reissmann, D.R.; Sierwald, I.; Berger, F.; Heydecke, G. A model of blended learning in a preclinical course in prosthetic dentistry. J. Dent. Educ. 2015, 79, 157–165. [Google Scholar] [PubMed]
- Alves, L.S.; de Oliveira, R.S.; Nora, A.D.; Cuozzo Lemos, L.F.; Rodrigues, J.A.; Zenkner, J.E.A. Dental Students’ Performance in Detecting In Vitro Occlusal Carious Lesions Using ICDAS with E-Learning and Digital Learning Strategies. J. Dent. Educ. 2018, 82, 1077–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luz, P.B.; Stringhini, C.H.; Otto, B.R.; Port, A.L.; Zaleski, V.; Oliveira, R.S.; Pereira, J.T.; Lussi, A.; Rodrigues, J.A. Performance of undergraduate dental students on ICDAS clinical caries detection after different learning strategies. Eur. J. Dent. Educ. 2015, 19, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.H.; Zhong, J.; Phillips, C.; Koroluk, L.D. Self-Directed Digital Learning: When Do Dental Students Study? J. Dent. Educ. 2018, 82, 373–378. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proenca, L.; Rua, J.; Delgado, A.; Joao Mendes, J. Cloud-based collaboration and productivity tools to enhance self-perception and self-evaluation in senior dental students: A pilot study. Eur. J. Dent. Educ. 2019, 23, e53–e58. [Google Scholar] [CrossRef] [Green Version]
- Boynton, J.R.; Johnson, L.A.; Nainar, S.M.; Hu, J.C. Portable digital video instruction in predoctoral education of child behavior management. J. Dent. Educ. 2007, 71, 545–549. [Google Scholar]
- Weaver, J.M.; Lu, M.; McCloskey, K.L.; Herndon, E.S.; Tanaka, W. Digital multimedia instruction enhances teaching oral and maxillofacial suturing. J. Calif. Dent. Assoc. 2009, 37, 859–862. [Google Scholar]
- Smith, W.; Rafeek, R.; Marchan, S.; Paryag, A. The use of video-clips as a teaching aide. Eur. J. Dent. Educ. 2012, 16, 91–96. [Google Scholar] [CrossRef]
- Schittek Janda, M.; Mattheos, N.; Nattestad, A.; Wagner, A.; Nebel, D.; Farbom, C.; Le, D.H.; Attstrom, R. Simulation of patient encounters using a virtual patient in periodontology instruction of dental students: Design, usability, and learning effect in history-taking skills. Eur. J. Dent. Educ. 2004, 8, 111–119. [Google Scholar] [CrossRef]
- Reynolds, P.A.; Harper, J.; Dunne, S.; Cox, M.; Myint, Y.K. Portable digital assistants (PDAs) in dentistry: Part II—Pilot study of PDA use in the dental clinic. Br. Dent. J. 2007, 202, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyorala, E.; Maenpaa, S.; Heinonen, L.; Folger, D.; Masalin, T.; Hervonen, H. The art of note taking with mobile devices in medical education. BMC Med. Educ. 2019, 19, 96. [Google Scholar] [CrossRef] [PubMed]
- Mahrous, A.; Schneider, G.B.; Holloway, J.A.; Dawson, D.V. Enhancing Student Learning in Removable Partial Denture Design by Using Virtual Three-Dimensional Models Versus Traditional Two-Dimensional Drawings: A Comparative Study. J. Prosthodont. 2019, 28, 927–933. [Google Scholar] [CrossRef]
- Callan, R.S.; Haywood, V.B.; Cooper, J.R.; Furness, A.R.; Looney, S.W. The Validity of Using E4D Compare’s “% Comparison” to Assess Crown Preparations in Preclinical Dental Education. J. Dent. Educ. 2015, 79, 1445–1451. [Google Scholar] [PubMed]
- Esser, C.; Kerschbaum, T.; Winkelmann, V.; Krage, T.; Faber, F.J. A comparison of the visual and technical assessment of preparations made by dental students. Eur. J. Dent. Educ. 2006, 10, 157–161. [Google Scholar] [CrossRef]
- Greany, T.J.; Yassin, A.; Lewis, K.C. Developing an All-Digital Workflow for Dental Skills Assessment: Part I, Visual Inspection Exhibits Low Precision and Accuracy. J. Dent. Educ. 2019, 83, 1304–1313. [Google Scholar] [CrossRef]
- Hamil, L.M.; Mennito, A.S.; Renne, W.G.; Vuthiganon, J. Dental students’ opinions of preparation assessment with E4D compare software versus traditional methods. J. Dent. Educ. 2014, 78, 1424–1431. [Google Scholar]
- Kateeb, E.T.; Kamal, M.S.; Kadamani, A.M.; Abu Hantash, R.O.; Abu Arqoub, M.M. Utilising an innovative digital software to grade pre-clinical crown preparation exercise. Eur. J. Dent. Educ. 2017, 21, 220–227. [Google Scholar] [CrossRef]
- Kozarovska, A.; Larsson, C. Implementation of a digital preparation validation tool in dental skills laboratory training. Eur. J. Dent. Educ. 2018, 22, 115–121. [Google Scholar] [CrossRef]
- Kunkel, T.C.; Engelmeier, R.L.; Shah, N.H. A comparison of crown preparation grading via PrepCheck versus grading by dental school instructors. Int. J. Comput. Dent. 2018, 21, 305–311. [Google Scholar]
- Liu, L.; Li, J.; Yuan, S.; Wang, T.; Chu, F.; Lu, X.; Hu, J.; Wang, C.; Yan, B.; Wang, L. Evaluating the effectiveness of a preclinical practice of tooth preparation using digital training system: A randomised controlled trial. Eur. J. Dent. Educ. 2018, 22, e679–e686. [Google Scholar] [CrossRef]
- Mays, K.A.; Crisp, H.A.; Vos, P. Utilizing CAD/CAM to Measure Total Occlusal Convergence of Preclinical Dental Students’ Crown Preparations. J. Dent. Educ. 2016, 80, 100–107. [Google Scholar]
- Miyazono, S.; Shinozaki, Y.; Sato, H.; Isshi, K.; Yamashita, J. Use of Digital Technology to Improve Objective and Reliable Assessment in Dental Student Simulation Laboratories. J. Dent. Educ. 2019, 83, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Park, C.F.; Sheinbaum, J.M.; Tamada, Y.; Chandiramani, R.; Lian, L.; Lee, C.; Da Silva, J.; Ishikawa-Nagai, S. Dental Students’ Perceptions of Digital Assessment Software for Preclinical Tooth Preparation Exercises. J. Dent. Educ. 2017, 81, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Gratton, D.G.; Kwon, S.R.; Blanchette, D.; Aquilino, S.A. Impact of Digital Tooth Preparation Evaluation Technology on Preclinical Dental Students’ Technical and Self-Evaluation Skills. J. Dent. Educ. 2016, 80, 91–99. [Google Scholar] [PubMed]
- Gratton, D.G.; Kwon, S.R.; Blanchette, D.R.; Aquilino, S.A. Performance of two different digital evaluation systems used for assessing pre-clinical dental students’ prosthodontic technical skills. Eur. J. Dent. Educ. 2017, 21, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.R.; Restrepo-Kennedy, N.; Dawson, D.V.; Hernandez, M.; Denehy, G.; Blanchette, D.; Gratton, D.G.; Aquilino, S.A.; Armstrong, S.R. Dental anatomy grading: Comparison between conventional visual and a novel digital assessment technique. J. Dent. Educ. 2014, 78, 1655–1662. [Google Scholar]
- Garrett, P.H.; Faraone, K.L.; Patzelt, S.B.; Keaser, M.L. Comparison of Dental Students’ Self-Directed, Faculty, and Software-Based Assessments of Dental Anatomy Wax-Ups: A Retrospective Study. J. Dent. Educ. 2015, 79, 1437–1444. [Google Scholar]
- Mays, K.A.; Levine, E. Dental students’ self-assessment of operative preparations using CAD/CAM: A preliminary analysis. J. Dent. Educ. 2014, 78, 1673–1680. [Google Scholar]
- Sly, M.M.; Barros, J.A.; Streckfus, C.F.; Arriaga, D.M.; Patel, S.A. Grading Class I Preparations in Preclinical Dental Education: E4D Compare Software vs. the Traditional Standard. J. Dent. Educ. 2017, 81, 1457–1462. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Kobayashi, H.; Lee, S.R.; Ohyama, H. The Role of Digital 3D Scanned Models in Dental Students’ Self-Assessments in Preclinical Operative Dentistry. J. Dent. Educ. 2018, 82, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.A.; Simon, B.; Toth, Z.; Vag, J. Evaluating the efficiency of the Dental Teacher system as a digital preclinical teaching tool. Eur. J. Dent. Educ. 2018, 22, e619–e623. [Google Scholar] [CrossRef] [PubMed]
- Wolgin, M.; Grabowski, S.; Elhadad, S.; Frank, W.; Kielbassa, A.M. Comparison of a prepCheck-supported self-assessment concept with conventional faculty supervision in a pre-clinical simulation environment. Eur. J. Dent. Educ. 2018, 22, e522–e529. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.S.; Jenkins, S.M.; James, T.; Dummer, P.M.; Bryant, S.; Hayes, S.J.; Oliver, S.; Stone, D.; Fenton, C. An initial evaluation of virtual reality simulation in teaching pre-clinical operative dentistry in a UK setting. Eur. J. Prosthodont. Restor. Dent. 2007, 15, 89–92. [Google Scholar]
- Welk, A.; Maggio, M.P.; Simon, J.F.; Scarbecz, M.; Harrison, J.A.; Wicks, R.A.; Gilpatrick, R.O. Computer-assisted learning and simulation lab with 40 DentSim units. Int. J. Comput. Dent. 2008, 11, 17–40. [Google Scholar]
- Gal, G.B.; Weiss, E.I.; Gafni, N.; Ziv, A. Preliminary assessment of faculty and student perception of a haptic virtual reality simulator for training dental manual dexterity. J. Dent. Educ. 2011, 75, 496–504. [Google Scholar]
- Pohlenz, P.; Grobe, A.; Petersik, A.; von Sternberg, N.; Pflesser, B.; Pommert, A.; Hohne, K.H.; Tiede, U.; Springer, I.; Heiland, M. Virtual dental surgery as a new educational tool in dental school. J. Cranio-Maxillofac. Surg. 2010, 38, 560–564. [Google Scholar] [CrossRef]
- Urbankova, A. Impact of computerized dental simulation training on preclinical operative dentistry examination scores. J. Dent. Educ. 2010, 74, 402–409. [Google Scholar]
- Gottlieb, R.; Lanning, S.K.; Gunsolley, J.C.; Buchanan, J.A. Faculty impressions of dental students’ performance with and without virtual reality simulation. J. Dent. Educ. 2011, 75, 1443–1451. [Google Scholar]
- LeBlanc, V.R.; Urbankova, A.; Hadavi, F.; Lichtenthal, R.M. A preliminary study in using virtual reality to train dental students. J. Dent. Educ. 2004, 68, 378–383. [Google Scholar]
- Murbay, S.; Neelakantan, P.; Chang, J.W.W.; Yeung, S. Evaluation of the introduction of a dental virtual simulator on the performance of undergraduate dental students in the pre-clinical operative dentistry course. Eur. J. Dent. Educ. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, H.; Ikeda, M.; Araki, K. Evaluation of a virtual reality simulation system for porcelain fused to metal crown preparation at Tokyo Medical and Dental University. J. Dent. Educ. 2013, 77, 782–792. [Google Scholar]
- Ben-Gal, G.; Weiss, E.I.; Gafni, N.; Ziv, A. Testing manual dexterity using a virtual reality simulator: Reliability and validity. Eur. J. Dent. Educ. 2013, 17, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Jasinevicius, T.R.; Landers, M.; Nelson, S.; Urbankova, A. An evaluation of two dental simulation systems: Virtual reality versus contemporary non-computer-assisted. J. Dent. Educ. 2004, 68, 1151–1162. [Google Scholar] [PubMed]
- Quinn, F.; Keogh, P.; McDonald, A.; Hussey, D. A study comparing the effectiveness of conventional training and virtual reality simulation in the skills acquisition of junior dental students. Eur. J. Dent. Educ. 2003, 7, 164–169. [Google Scholar] [CrossRef]
- Wang, D.; Zhao, S.; Li, T.; Zhang, Y.; Wang, X. Preliminary evaluation of a virtual reality dental simulation system on drilling operation. Biomed. Mater. Eng. 2015, 26 (Suppl. 1), S747–S756. [Google Scholar] [CrossRef] [Green Version]
- de Boer, I.R.; Lagerweij, M.D.; Wesselink, P.R.; Vervoorn, J.M. The Effect of Variations in Force Feedback in a Virtual Reality Environment on the Performance and Satisfaction of Dental Students. Simul. Healthc. 2019, 14, 169–174. [Google Scholar] [CrossRef]
- Schwindling, F.S.; Deisenhofer, U.K.; Porsche, M.; Rammelsberg, P.; Kappel, S.; Stober, T. Establishing CAD/CAM in Preclinical Dental Education: Evaluation of a Hands-On Module. J. Dent. Educ. 2015, 79, 1215–1221. [Google Scholar]
- Douglas, R.D.; Hopp, C.D.; Augustin, M.A. Dental students’ preferences and performance in crown design: Conventional wax-added versus CAD. J. Dent. Educ. 2014, 78, 1663–1672. [Google Scholar]
- Wegner, K.; Michel, K.; Seelbach, P.H.; Wostmann, B. A questionnaire on the use of digital denture impressions in a preclinical setting. Int. J. Comput. Dent. 2017, 20, 177–192. [Google Scholar]
- Schott, T.C.; Arsalan, R.; Weimer, K. Students’ perspectives on the use of digital versus conventional dental impression techniques in orthodontics. BMC Med. Educ. 2019, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Kovaltschuk, I.; Lenherr, P.; Dedem, P.; Joda, T. Dental Students’ Perceptions of Digital and Conventional Impression Techniques: A Randomized Controlled Trial. J. Dent. Educ. 2017, 81, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Marti, A.M.; Harris, B.T.; Metz, M.J.; Morton, D.; Scarfe, W.C.; Metz, C.J.; Lin, W.S. Comparison of digital scanning and polyvinyl siloxane impression techniques by dental students: Instructional efficiency and attitudes towards technology. Eur. J. Dent. Educ. 2017, 21, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J. Prosthet. Dent. 2015, 114, 818–825. [Google Scholar] [CrossRef]
- Murrell, M.; Marchini, L.; Blanchette, D.; Ashida, S. Intraoral Camera Use in a Dental School Clinic: Evaluations by Faculty, Students, and Patients. J. Dent. Educ. 2019, 83, 1339–1344. [Google Scholar] [CrossRef]
- Soares, P.V.; de Almeida Milito, G.; Pereira, F.A.; Reis, B.R.; Soares, C.J.; de Sousa Menezes, M.; de Freitas Santos-Filho, P.C. Rapid prototyping and 3D-virtual models for operative dentistry education in Brazil. J. Dent. Educ. 2013, 77, 358–363. [Google Scholar]
- Kroger, E.; Dekiff, M.; Dirksen, D. 3D printed simulation models based on real patient situations for hands-on practice. Eur. J. Dent. Educ. 2017, 21, e119–e125. [Google Scholar] [CrossRef]
- Mileman, P.A.; van den Hout, W.B.; Sanderink, G.C. Randomized controlled trial of a computer-assisted learning program to improve caries detection from bitewing radiographs. Dentomaxillofac. Radiol. 2003, 32, 116–123. [Google Scholar] [CrossRef]
- Minston, W.; Li, G.; Wennberg, R.; Nasstrom, K.; Shi, X.Q. Comparison of diagnostic performance on approximal caries detection among Swedish and Chinese senior dental students using analogue and digital radiographs. Swed. Dent. J. 2013, 37, 79–85. [Google Scholar]
- Busanello, F.H.; da Silveira, P.F.; Liedke, G.S.; Arus, N.A.; Vizzotto, M.B.; Silveira, H.E.; Silveira, H.L. Evaluation of a digital learning object (DLO) to support the learning process in radiographic dental diagnosis. Eur. J. Dent. Educ. 2015, 19, 222–228. [Google Scholar] [CrossRef]
- Kratz, R.J.; Nguyen, C.T.; Walton, J.N.; MacDonald, D. Dental Students’ Interpretations of Digital Panoramic Radiographs on Completely Edentate Patients. J. Dent. Educ. 2018, 82, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, A.; Kirkevang, L.L. Students’ attitudes to digital radiography and measurement accuracy of two digital systems in connection with root canal treatment. Eur. J. Dent. Educ. 2004, 8, 167–171. [Google Scholar] [CrossRef]
- Jathanna, V.R.; Jathanna, R.V.; Jathanna, R. The awareness and attitudes of students of one Indian dental school toward information technology and its use to improve patient care. Educ. Health (Abingdon) 2014, 27, 293–296. [Google Scholar] [CrossRef] [PubMed]
- McCann, A.L.; Schneiderman, E.D.; Hinton, R.J. E-teaching and learning preferences of dental and dental hygiene students. J. Dent. Educ. 2010, 74, 65–78. [Google Scholar] [PubMed]
- Ren, Q.; Wang, Y.; Zheng, Q.; Ye, L.; Zhou, X.D.; Zhang, L.L. Survey of student attitudes towards digital simulation technologies at a dental school in China. Eur. J. Dent. Educ. 2017, 21, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.S.; Roberts, E.P.; Reynolds, S.; Stein, A.F. Dental Students’ Use of Student-Managed Google Docs and Other Technologies in Collaborative Learning. J. Dent. Educ. 2019, 83, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarfe, W.C.; Potter, B.J.; Farman, A.G. Effects of instruction on the knowledge, attitudes and beliefs of dental students towards digital radiography. Dentomaxillofac. Radiol. 1996, 25, 103–108. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Hariri, N.H.; Jahangiri, L. Student’s Perception of the Impact of E-learning on Dental Education. J. Contemp. Dent. Pract. 2019, 20, 616–621. [Google Scholar] [CrossRef]
- Chatham, C.; Spencer, M.H.; Wood, D.J.; Johnson, A. The introduction of digital dental technology into BDS curricula. Br. Dent. J. 2014, 217, 639–642. [Google Scholar] [CrossRef]
- Brownstein, S.A.; Murad, A.; Hunt, R.J. Implementation of new technologies in U.S. dental school curricula. J. Dent. Educ. 2015, 79, 259–264. [Google Scholar]
- Bhardwaj, A.; Nagandla, K.; Swe, K.M.; Abas, A.B. Academic Staff Perspectives Towards Adoption of E-learning at Melaka Manipal Medical College: Has E-learning Redefined our Teaching Model? Kathmandu Univ. Med. J. (KUMJ) 2015, 13, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020. [Google Scholar] [CrossRef] [Green Version]
- Greany, T.J.; Yassin, A.; Lewis, K.C. Developing an All-Digital Workflow for Dental Skills Assessment: Part II, Surface Analysis, Benchmarking, and Grading. J. Dent. Educ. 2019, 83, 1314–1322. [Google Scholar] [CrossRef]

| Study (Year) | Study Design | Theory/Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Komolpis et al. 2002 [12] | RCT | P | 99 | Compared effectiveness (exam scores and time spent) in clinical orthodontic diagnosis in test group (50 students with web-based digital records) and control group (49 students provided with traditional records) with study models, panoramic and cephalometric radiograph, facial and intraoral photographs. | Test and control group performed similar in the exam with no difference in test time; positive feedback about the web-based learning module, students benefit from convenient access to study material on the computer without time constrictions. |
| Schultze-Mosgau et al. 2004 [20] | OT | T | 82 | Evaluated a web-based course with a concluding online examination. Feed-back by questionnaire. | Course gradings excellent or good were given for accessibility independent of time (89%), for access independent of location (83%), for objectification of knowledge transfer (67%), and for use of videos for surgical techniques (91%). |
| Schittek Janda et al. 2004 [30] | RCT | P | 39 | Compared the effect of a web-based virtual learning environment (VLE) on students’ performance in history interview. Both groups underwent standard instruction in professional behavior, history taking, clinical decision making and treatment planning. Test group worked with the virtual periodontal patient for 1 week prior to their first patient contact; control group was first allowed to use the virtual patient after their first patient contact. Time spent, type and order of questions and professional behavior were analyzed. | Test group asked more relevant questions, spent more time on patient issues, and performed a more complete history interview than control. The use of the virtual patient and the process of writing questions in working with the virtual patient stimulated students to organize their knowledge and resulted in more confident behavior towards the patient. |
| Boynton et al. 2006 [27] | CS | P | 108 | Explored students’ behaviors management in pediatric dentistry using portable video instructions; test group: 11 students reviewing video lecture material on a portable device (iPod) supplementing conventional pediatric behavior management lecture; additional 6 students (intermediate) used audio versions or video on the computer; control group: 91 students without digital learning material; exam on student comprehension. | Test group performed significantly better on the examination (mean 9.3) than control (7.9) or intermediate group (7.8); portable format was preferred. |
| Reynolds et al. 2007 [31] | CS | P | 12 | Investigated students’ educational use of portable digital assistants (PDA) to access a Virtual Learning Environment in a primary dentalcare clinic and at home; cross over trial with 6 students with / 6 without for 12 weeks. | PDA was frequently used for online education; over 90% wanted PDA as part of their dental kit. |
| Kingsley et al. 2009 [17] | CS | P | 78 | Examined students’ ability to use web-based online technologies to find recently published online citations and to answer clinically relevant questions (oral pathogens and immunology course); technology skills analyzed: ability to locate online library resources, understand how information is organized within the library system, access online databases, interpret and evaluate research materials within the context of a specific discipline; students were provided with a review article of vaccines against caries from 2001. | 100% of students had correct responses to the content-specific or technology-independent portions; 46% had correct responses to the information literacy or technology-dependent portions; as web-based technologies grow more prevalent in the digital era, information literacy and technology-dependent, applied research assignments should be integrated into graduate-level curricula. |
| Weaver et al. 2009 [28] | RCT | P | 12 | Evaluated performance in intraoral suturing after digital multimedia instruction; control group: written information; test group: plus teaching tool; suturing performed on a model situation, evaluated by 10 grading criteria. | Test group performed better than control; video addressed common mistakes made by novice students, improved long-term understanding of the basic suture principles. |
| Wright et al. 2009 [14] | OT | T | 235 | Determined whether dental students used an interactive DVD-tooth atlas as a study aid and perceived the 3D interactive tooth atlas as a value-added learning experience. | 14% students downloaded the DVD voluntarily prior to adding atlas-related exam questions as incentives; after adding incentives 43% downloaded the material; financial concerns and overly sophisticated content were deemed responsible for the low acceptance. |
| Curnier 2010 [16] | OT | P | 26 | Assessed VR integration into teaching of dental anatomy, feedback by questionnaire | 70% of the students were satisfied/very satisfied with IT integration in the curriculum. |
| Bains et al. 2010 [13] | RCT | T | 90 | Compared effectiveness and attitudes toward e-learning (EL, online tutorial without teacher), face-to-face learning (F2FL, led by teacher) and blended learning (BL) subdivided in BL1 (EL first then F2FL) and BL2 (F2FL first then EL) among 4th year students. Groups received cephalometric tutorial in the allocated mode, answered an MCQ (Multiple Choice Questionnaire). | F2FL and BL resulted in similar test results; EL alone was less effective. BL was the most and F2FL was the least accepted method, EL was significantly less preferred, the order B1 or 2 had no effect. |
| Mitov et al. 2010 [15] | CS | T | 36 | Testing an e-learning software (morphoDent) to prepare for an anatomy exam. 3D models with description and x-rays of permanent human teeth were available for viewing and interaction on the learning platform. Practical dental morphology exam was compared to virtual tooth anatomy exam. Evaluation of students’ perceptions in a questionnaire. | Similar exam scores in traditional and online exam. Majority felt the software helped them learning dental morphology, despite of difficulties in operating the program. |
| Vuchkova et al. 2012 [19] | CS | P | 88 | Evaluated interactive digital versus conventional radiology textbook (course radiographic anatomy), outcome was radiographic interpretation test and survey feedback. | 95% perceived positive enhancement of learning and interpretation. |
| Smith et al. 2012 [29] | OT | P | 26 | Compared the use of online video-clips with traditional live demonstrations with one-to-one supervision; students exam scores before and after the video introduction were compared. Feed-back by questionnaire. | 76% preferred video-clips to live demonstrations, 57% reviewed DVD at home; 57% felt one-to-one supervision more effective developing their competence in tooth preparation. |
| Qi et al. 2013 [21] | RCT | P | 95 | Comparison of active versus passive approaches in using 3D virtual scenes in dental implant cases. Students were exposed to educational materials about implant restoration on three types of webpages: traditional 2D (group 1); active-controlling 3D (group 2); passive-controlling 3D (group 3). After reviewing their webpages, students were asked to complete a posttest to assess the relative quality of information acquisition. Before study exposure, students performed a standardized test of spatial ability (mental rotations test, MRT). | Posttest scores were highest in group 3 (passive control) and lowest in group 2 (active control). Higher MRT scores were associated with better posttest performances in all three groups. Individuals with low spatial ability did not benefit from 3D interactive virtual reality, while passive control produced higher learning effects compared to active control. |
| Reissmann et al. 2015 [22] | OT | T | 71 | Creation of a blended learning model; e-learning modules covered fundamental principles, additional information, and learning tests (tests were repeated until passed and the next video sequence unlocked); modules comprised (i) tooth preparation, placement of post and core, and provisional crown; (ii) with preparation, manufacturing and insertion of a FDP (Fixed Dental Prosthesis). Students rated the course on a questionnaire, comparison to previous courses without e-learning. | Significantly higher satisfaction among students enrolled in the e-learning modules compared to the years prior to integration of the e-learning tests. Results suggest that instructor-based practical demonstrations in preclinical courses in prosthetic dentistry could be successfully replaced by e-learning applications provided that course content is structured according to specific predefined learning goals and procedures. |
| Luz et al. 2015 [24] | RCT | P | 39 | Evaluated the effect of a digital learning tool on students’ caries detection in 12 pediatric patients (3.4 per student) using ICDAS (International Caries Detection & Assessment System) (1264 dental surfaces). 2 weeks after first exam students were split into 3 training groups: Group 1: ICDAS e-learning program; group 2: plus digital learning tool; group 3: no learning strategy; students reassessed the same patients 2 weeks, and results compared. | After training group 1 and 2 had improved with significantly higher sensitivity; group 2 showed significant increase in sensitivity at the D2 and D3 thresholds as a result of the digital learning tool. |
| Gonzales et al. 2016 [18] | OT | T | 40 | Implementation social media (Twitter) in a dental radiology course and evaluated students’ use and perception by a questionnaire. | 95% (38) had not used Twitter prior to the course; 53% (21) created an account during the course to view radiographic examples and stay informed; overall Twitter had a positive impact with improved accessibility to the instructor. |
| Jackson et al. 2018 [25] | OT | P | 80 | Evaluated dental students study patterns using self-directed web-based learning modules with scheduled self-study time instead of lectures; web-based module access (date and time) was recorded for four courses in the growth & development curriculum; scheduled access time was 8 am to 5 pm. | Frequency of module access (at least once) varied among the four courses (10–64%); only three students had > 20% of their total accesses taking place during designated self-study times. For all courses the proportion of module access was significantly higher 0–2 days before an exam compared to 3–7 or >7 days before final exam; no association between module access during scheduled times and course performance. |
| Alves et al. 2018 [23] | RCT | P | 64 | Evaluated the effect of a digital learning tool on students’ caries detection in 80 teeth using ICDAS; Group 1 (21 students): ICDAS e-learning program; group 2 (22 students): plus digital learning tool; group 3 (21 students): no training; reassessment of the 80 teeth 2 weeks after training. | After training group 1 and 2 had improved with significantly higher sensitivity and specificity; group 3 had increased sensitivity at the D2 thresholds; ICDAS e-learning with or without digital learning tool improved occlusal caries detection. |
| Botelho et al. 2019 [26] | OT | T | 40 | Surveyed dental students’ perception of cloud-based practice records (documenting clinical progression) compared to traditional paper record. | Cloud based records were rated significantly better in terms of usefulness, ease of use, and learning, satisfaction. |
| Pyörälä et al. 2019 [32] | OT | T | 176 | Investigated perception of mobile devices for study use among 124 medical, 52 dental students provided with iPads and followed from 1st to 5th year; feed-back by questionnaire. | Note taking was the most frequent application of the mobile device in the 1st–5th year; students personalized digital learning materials by making comments, underlining, marking images and drawings. Students retrieved their notes anytime when studying for examinations and treating patients in clinical practice. |
| Mahrous et al. 2019 [33] | RCT | P | 77 | Compared virtual 3D casts with 2D paper-based exercise in planning removable partial denture design; group 1 (n = 39) planned RPD in Kennedy class IV in virtual 3D and Kennedy class II in traditional 2D format, group 2 (=38) planned class IV traditional and class II virtual; survey lines and undercut positions were drawn on virtual 3D casts or given in written descriptions (2D); students planned design (with rests, clasp type, retention location, guide plane) was scored; feed-back by questionnaire. | Similar scores for 3D and 2D exercises; majority favored virtual 3D casts because of improved understanding of relevant parameters and spatial visualization. Currently, physical casts are still required to practice surveying and drawing on the cast. |
| Study (Year) | Study Design | Theory/Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Esser et al. 2006 [35] | CS | P | 36 | Compared conventional visual examination by faculty with digital analysis (“Prep Assistant”) of students’ preparation of a central incisor for a metal-ceramic crown; preparations were scanned; before the exam preparation, students had received theoretical and practical exercises. | Digital measuring technique was superior for convergence angle, occlusal reduction and width of shoulder; low correlation between visual and digital was observed for the assessments of chamfer, path of insertion, width of bevel and basic form; calibration of evaluators benefit from digital analysis tool. |
| Hamil et al. 2014 [37] | OT | P | 81 | Evaluated dental students’ opinion about a new grading software program (E4D Compare with surface mapping technology) for their self-assessment and as faculty-grading tool in a preclinical course to evaluate crown preparations. Software was introduced (one-hour lecture and three-hour hands-on laboratory session) and applied for self-assessment during one semester; questionnaire about students’ perception. | Students preferred digital grading system over traditional hand-grading 95% reported on feedback inconsistencies among different faculty members, 72% reported on inconsistencies from the examiner; 85% agreed or strongly agreed that E4D Compare provided more consistent grading than faculty; 79% responded that the software provided more feedback, 90% found the software helping them to understand their deficiencies; 89% agreed or strongly agreed that E4D Compare grading helped them be better clinicians. |
| Mays et al. 2014 [49] | CT | P | 25 | Compared students’ visual self-assessment, students’ digital (CAD/CAM) self-assessment, faculty visual assessment, and faculty digital assessment. Students prepared mesial-occlusal amalgam cavity, used standardized grading sheets for visual self-assessment, scanned their preparation, used design tool of Cerec software for digital self-assessment. | Moderate agreement between faculty visual and digital evaluation for occlusal and proximal shape, orientation and definition; poor agreement between student visual and digital evaluation for occlusal shape, and fair for proximal shape, orientation and definition; slight to poor agreement between students visual and faculty visual evaluation, and digital assessment did not improve student/faculty agreement. |
| Kwon et al. 2014 [47] | OT | P | 60 | Compared conventional visual faculty grading of wax-ups to digital assessment in dental anatomy course; 30 faculty wax-ups, 15 student wax-ups and 15 dentoform teeth; visual grading was performed by two experienced faculty members, digital grading by one operator, both gradings were repeated after 1 week; maxillary 1st molar wax-up (from faculty) with highest scores from visual grading was used as master model for digital grading. | Modest intra-rater reliability for visual scoring with similar rating between the two trials (0.7); low inter-rater agreement between the two faculty raters; digital grading showed high intra-rater agreement for the repeated assessment (ICC 0.9); modest correlation between visual and digital grading. |
| Garrett et al. 2015 [48] | CCS | P | 57 | Evaluated E4D software (Planmeca) to assess incisor and molar wax-ups of 57 students, who used digital images for self-assessment, and compare to faculty members; based on five assessment criteria (arch alignment, proximal contacts, proximal contour and embrasures, facial contour, lingual contour) and applying 300, 400, and 500 μm level of tolerance in E4D. | Students’ self-assessment of the maxillary incisor wax-up was higher than faculty and E4D300, but lower than E4D 400 and 500. For the molar wax-up, self-assessment was not different to faculty, but higher than E4D300. E4D500 evaluations were sig. superior than other assessments. |
| Callan et al. 2015 [34] | CCS | P | 82 | Validated E4D software (Planmeca) to assess molar crown preparation of 82 students and compare to calibrated faculty members based on four criteria (occlusal reduction, proximal reduction, facial/lingual reduction, margins and draw). Agreement in rankings between faculty scores and E4D Compare scores was measured with Spearman’s correlation coefficient (SCC) at five different tolerance levels (0.1–0.5 mm). | SCC values for practical exams varied between 0.20 and 0.56. None of the upper 95% confidence limits reached the for strong correlation. SCC values indicated only weak to moderate agreement in ranks between practical exam scores and scores obtained with E4D Compare. When ranked from lowest to highest, the results from the conventional grading by the faculty did not correlate within an acceptable range to E4D Compare software data. |
| Mays et al. 2016 [42] | CCS | P | 50 | Validated E4D software (Planmeca) to assess occlusal convergence (TOC) of 50 molar crown preparations from students and compared to traditional faculty assessment. | Digital software could distinguish differences in TOC, which were grouped as minimum taper (mean 11°), moderate (mean 23°), or excessive (mean 47°). Digital TOC evaluation was more objective compared to faculty visual scoring. |
| Gratton et al. 2016 [45] | RCT | P | 80 | Compared effect of access to digital systems in addition to conventional preparation instructions; CEREC prepCheck (n = 20), E4D Compare (n=20), and control without access to digital system (n = 40); incisor and molar crown preparations were assessed by the students, by 3 faculties and by E4D Compare at 0.30 mm tolerance. | All groups had similar preparation scores. Visual and digital assessment scores showed modest correlation. |
| Gratton et al. 2017 [46] | RCT | P | 79 | Compared digital systems Compare (n = 42) and prepCheck (n = 37) as additional evaluation tool assessing their crown preparations (maxillary central incisor and mandibular molar); all preparations were graded by faculty Compare and prepCheck; feed-back with post-course questionnaire. | Both groups had similar technical scores; both systems had modest correlation with faculty scores and strong correlation with each other. 55.3% of students felt unfavorable about learning digital evaluation protocols, while 62.3% felt favorable about the integration of the tools into the curriculum. |
| Park et al. 2017 [44] | OT | P | 36 | Evaluated prepCheck for self-assessment, students performed ceramo-metal crown preparation (maxillary molar during formative exercise, mandibular molar during summative exam); five learning tools were used for assessments: reduction, margin width, surface finish, taper, undercut; tools were rated for usefulness, user-friendliness, and frequency of use (scale from 1 = lowest to 5 = highest). Faculty members graded tooth preparations as pass (P), marginal-pass (MP), or fail (F). | Tools assessing undercut and taper received highest scores for usefulness, user-friendliness, and frequency of use. Students’ performance was 38.8% P, 30.6% MP and 30.6% F. Failing students had the highest score (4.4) on usefulness. |
| Kateeb et al. 2017 [38] | OT | P | 96 | Compared digital assessment software of students’ crown preparation with traditional visual inspection; four examiners; sample of 20 preparations were reassessed for intra-rater reliability. | Intra-rater reliability (ICC) was 0.73–0.78 and 0.99 for the digital grading system; inter-rater reliability among the four examiners was good (0.76); agreement between examiners and digital ratings were low to moderate; digital grading was more consistent. |
| Sly et al. 2017 [50] | OT | P | 98 | Compared E4D software (Planmeca) to assess students intracoronal Class I preparation with traditional visual inspection; four examiners. | Similar results for grading of isthmus width and remaining marginal ridge, while pulpal floor depth was assessed more precisely with visual inspection; results indicate that software has limitations for intracoronal cavity assessment but offers a self-assessment tool to improve psychomotor skills with independent and immediate feedback. |
| Kunkel et al. 2018 [40] | OT | P | 69 | Compared prepCheck with visual faculty assessment of taper in students’ crown preparation of typodont teeth, 10 experienced course instructors. | Instructor gradings were overrated compared to digital prepCheck grades, prepCheck facilitates evaluation instantly and exactly by students and examiners. |
| Kozarovska & Larsson 2018 [39] | RCT | P | 57 | Evaluated a digital preparation validation tool (PVT) for students’ self-assessment of crown preparation (tooth 11 and 21); group A (“prep-and-scan” self-assessed and scanned three preparations; group B (“best-of-three”) self-assessed the three attempts, chose the best for scanning; questionnaire about students’ and teachers’ experiences with PVT. | Group A showed an increase in agreement of self-assessment and feedback from PVT, while group B showed low level agreement with PVT. Bucco-incisal reduction, reduction of the tuberculum surface and presence of undercuts were difficult to correctly identify by the students. Questionnaire feedback revealed need for PVT to develop skills, to ease assessment, while critical aspects were PVT’s time efficiency and the need for verbal feedback. Teachers observed the PVT as a motivation during skills laboratory training, while verbal feedback were still deemed necessary. |
| Wolgin et al. 2018 [53] | RCT | P | 47 | Investigated digital self-assessment concept (prepCheck software) for students in the phantom course preparing a three surface (MOD) class II amalgam cavity; intervention group (IG): compared a 3D image of their preparation against master preparation with PrepCheck; control group (CG): received verbal feedback from supervisor based on pre-defined criteria. | Test and control groups performed similar and self-assessment learning tool was deemed equivalent to conventional supervision. |
| Lee et al. 2018 [51] | OT | P | 69 | Compared students’ self-assessment (conventional and digital with Cerec software) with assessment (conventional and digital) by faculty members for class II amalgam preparations (C2AP) and Class III composite preparations (C3CP). | Students overestimated their performance (positive S-F gap) in both the C2AP and C3CP preparation exercises in conventional (11% and 5%) and digital assessments (8% and 2%); in conventional assessments, preclinical performance was negatively correlated with student-faculty gap (r = −0.47, p < 0.001); particularly students in the bottom quartile sig. improved their self-assessment accuracy using digital self-assessments over conventional assessments. |
| Nagy et al. 2018 [52] | RCT | P | 36 | Investigated the effect of a digital feedback (test group) for mesio-occlusal onlay preparation by a 3D visualization of the cavity (Dental Teacher software, KaVo), while verbal feedback from supervisor was given to control group. Following feedbacks, 2nd corrective preparations were conducted and improvements measured. Parameters: occlusal cavity depth (OD), approximal depth (AD), extent of cusp reduction on the mesiobuccal cusp (CR), width of shoulder preparation around the mesiobuccal cusp (SW), cavity width at two different points in the occlusal box (OW). | Test group improved in all parameter and showed significantly smaller deviations of mean OD, AD and mean SW; in control group, parameter deviations were similar during 1st and 2nd preparation. |
| Liu et al. 2018 [41] | RCT | P | 66 | Evaluated the effectiveness of preclinical training on ceramic crown preparation using digital training system compared with traditional training method; test group: trained with digital method with Online Peer-Review System (OPRS) and Real-time Dental Training and Evaluation System (RDTES); control group: traditional method with instructor demonstration and evaluation; central incisor crown preparation. | Five of 15 assessed items were significantly better in test group; 96.97% of test students agreed or strongly agreed that using digital training system could better improve the practical ability than traditional method. |
| Greany et al. 2019 [36] | OT | P | 67 | Compared conventional visual faculty inspection of wax-ups to digital assessment; six examiners evaluated 67 students’ wax-ups of maxillary first molar, reevaluation after 1 week; scan with IOS, STL files imported to free available open source data cloud comparison utility (Cloud Compare.org), digital evaluation by two examiners. | Visual inspection had low inter-examiner precision (ICC 0.332) and accuracy; intra-examiner precision for reevaluation was low; inter-examiner precision of digital exam was high (ICC 0.866) with high accuracy. |
| Miyazone et al. 2019 [43] | OT | P | 100 | Compared prepCheck with visual faculty assessment of students’ crown preparation of typodont teeth (mandibular first molar as crown abutment, maxillary 2nd premolar and 2nd molar as FDP abutments), assess inter- and intra-grader agreement of five experienced examiners conducting visual and digital exam; scoring repeated three times; parameters for crown abutments: axial tissue removal, margin width, undercut, occlusal reduction, cusp tips, occlusal anatomy; for FDP abutments: path of insertion. | Intra-grader agreement was better with prepCheck than visual assessment for all parameters except cusp tip and occlusal anatomy; inter-grader agreement for path of insertion was questionable with visual, but good with digital assessment. Inter-grader disagreement was greater in visual than digital assessment. Overestimation of tooth reduction in visual grading was eliminated by digital analysis. |
| Study (Year) | Study Design | Theory/Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Soares et al. 2013 [77] | OT | T | 40 | Cavity preparation was taught with conventional teaching materials with 2D schematic illustration and photographs. New didactic material with virtual 3D (videos of the preparations) and magnified nylon prototyped models was introduced. Evaluation by questionnaire. | Improvement of teaching quality when combining 3D virtual technology with real models. |
| Kröger et al. 2016 [78] | OT | P | 22 | 3D printed simulation models based on real patient situations were used for hands-on practice. Models simulated realistic tooth positions and wide variability of dental cases and procedures. Students removed a crown from tooth 16, detected and removed caries, did a build-up filling and crown preparation within 3 h. Students’ feedback on a VAS questionnaire. | Students evaluated models based on real patient situations as good training possibilities. The lack of gingiva was disturbing. |
| Study (Year) | Study Design | Theory/Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Mileman et al. 2003 [79] | RCT | P | 67 | Investigated computer-assisted learning (CAL) calibration program to improves dental students’ accuracy in dentin caries detection from bitewing radiographs; experimental (n = 33) group: used CAL with feedback for self-calibration control (n = 34) group. | CAL improved students’ diagnostic performance; true positive ratio (sensitivity) for caries detection was significantly higher in test 76.3% than control with 66.9%, while false positive ratio (specificity) was similar (28.1 and 28.7%); diagnostic odds ratio was sig. higher in test (12.4) than in control (8.8). |
| Wenzel et al. 2004 [83] | RCT | P | 31 | Compared 2 digital systems (RVG-ui CCD sensor, Digora PSP plate system) for radiographic examination; after education in digital radiography one student group started with CCD, one with PSP and both completed endodontic treatment of single-rooted extracted tooth; groups switched radiography system and treated a 2nd tooth. True tooth length (TTL) and root filling length (RFL) were measured with the software and compared to manual measurement; feed-back questionnaire after each treatment. | Using CCD sensor required less time than PSP; positioning the tooth was easier with PSP plate; positive attitudes towards digital radiography; lengths measured on the digital images from both digital systems were slightly larger than true tooth lengths with no difference in ratio TTL/RFL between systems. |
| Minston et al. 2013 [80] | CT | P | 20 | Investigated students’ diagnostic performance on approximal caries detection with analog and digital radiographs from 46 extracted human premolars and molars, compared diagnostic accuracy; teeth were sectioned and histopathologically analyzed (gold standard) | Students ability for caries detection was poor, no difference between analog and digital radiographs. |
| Busanello et al. 2015 [81] | CCS | P | 62 | Evaluated digital learning object to improve skills in diagnosing radiographic dental changes (Visual Basic Application software); test group used the digital tool, control group: conventional imaging diagnosis course; diagnosis test after 3 weeks. | Test group performed significantly better, females were better than males. |
| Kratz et al. 2018 [82] | CT | P | 169 | Evaluated students’ ability to identify positional errors (tongue position, head rotation, chin position) in panoramic radiographs of edentulous patients, students in 2nd year (n = 84) and 3rd–4th year (n = 85) | 2nd year students identified significantly more positional errors than 3rd and 4th students. Students were more experienced at identifying radiographic findings compared to positional errors. |
| Study (Year) | Study Design | Theory/Practice | Participants | Materials and Methods | Results |
|---|---|---|---|---|---|
| Scarfe et al. 1996 [88] | OT | T | 277 | Investigated the effects of instructions in intraoral digital radiology on dental students’ knowledge, attitudes and beliefs; 174 from a university with formal instruction on digital dental radiography, and 103 from a university without instructions. | Students with instructions knew significantly more than students without; 93% wanted digital radiology to be included in the dental curriculum. |
| McCann et al. 2010 [85] | OT | T | 366 | Surveyed student’s (dental and dental hygiene) preferences for e-teaching and learning, using an online questionnaire in 2008 related to computer experience, use and effectiveness of e-resources, preferences for various environments, need for standardization, and preferred modes of communication. | 64% preferred printed text over digital and 74% wanted e-materials to supplement but not replace lectures; 71% preferred buying traditional textbooks, 11% preferred electronic versions; among e-resources virtual microscopy (69%), digital skull atlas (68%), and digital tooth atlas (64%) were reported as most effective; e-materials would enhance learning, in particular e-lectures (59%), clinical videos (54%), and podcasts (45%). E-resources should not replace interactions with faculty; students wanted lectures and clinical procedures recorded. |
| Jathanna et al. 2014 [84] | OT | T | 186 | Surveyed the perception of Indian dental students toward usefulness of digital technologies in improving dental practice, willingness to use digital and electronic technologies, perceived obstacles to use digital and electronic technologies in dental care setups, and their attitudes toward internet privacy issues. | Students indicated that digital technology increases patient satisfaction and practice efficiency, improves record quality, doctor-doctor communication, case diagnosis and treatment planning; obstacles to the wide adoption of these technologies were cost and dentists’ lack of knowledge and comfort with technology. |
| Chatham et al. 2014 [90] | OT | T | 11 | Surveyed the penetration of digital technologies in UK dental schools (11/16 responded). | 45% did not teach digital technologies (36% because it was not part of the curriculum, or in 95% due to the lack of technical expertise or support); half of those teaching digital technologies did so with lectures or demonstrations, the other half allowed practical involvement. |
| Brownstein et al. 2015 [91] | OT | T | 33 | Surveyed the penetration of emerging dental technologies into the curricula at US dental schools (62 eligible schools were contacted); academic Deans answered 19 questions related to 12 dental topics); 19 schools had <100 students/class; 14 had >100 students. | Highest penetration was in preclinical didactic courses (62%) and lowest was in preclinical laboratory (36%); most common specific technologies were digital radiography (85%) and rotary endodontics (81%), least common were CAD/CAM denture fabrication (20%) and hard tissue lasers (24%); the bigger the class sizes (>100 students) and the older the school, the lower the incorporation of newer technologies. |
| Bhardwaj et al. 2015 [92] | OT | T | 54 | Surveyed faculties’ opinion (15 dental, 42 medical faculty members in Melaka, Malaysia) toward the existing e-learning activities, and to analyze the extent of adopting and integration of e-learning into their traditional teaching methods; questionnaire with socio-demographic profile, skills and aptitude on the use of computer, knowledge and use of existing e-learning technology (e.g., MOODLE), experiences and attitudes towards e-learning, faculty opinion on novel e-learning techniques, and initiatives to be adopted for optimization of existing e-learning facilities. | 65.4% of faculty was positive towards e-learning; formal training required to support e-learning that enables smooth transition of the faculty from traditional teaching into blended approach; traditional instructor centered teaching is shifting to learner centered model facilitating students to control their own learning. Popular e-learning education tools: Virtual Learning Environment systems such as WebCT™. |
| Ren et al. 2017 [86] | OT | T | 389 | Questionnaire assessed students’ attitudes towards digital simulation technologies and teaching methods, how students compare digital technologies with traditional training methods; four categories: digital microscope, virtual pathology slides, digital radiology, virtual simulation training. | Most students accepted digital technologies as stimulating tool for self-learning; digital X-ray images were used to study oral radiology and preferred to conventional X-rays. Dental simulation training was most preferred technology (54.6%), 16.7% preferred digital microscopy, 15.0% virtual pathology slides, 13.7% digital x-ray images. 76% used the virtual simulation training machine to study oral clinical skills; 61% felt that the simulator would be a useful addition to current pre-clinical training; 66% felt that the simulator provided a realistic virtual environment. |
| Roberts et al. 2019 [87] | OT | T | 282 (in 2015) 129 (in 2017) | Surveyed the use of student-managed online technologies in collaborative e-learning; comparison of web-based applications and other study methods (survey in 2015 focused on Google Doc/survey in 2017 focused on all e-learning technologies). | Significant decrease in Google Docs overall usage in 2017 (95%) compared to 2015 (99%), but significantly increased frequency of use in all courses from 36% (2015) to 71.6% (2017). The use of textbooks dropped significantly from 25% (2015) to 15% (2017). Only 4% reported that textbooks were worth the cost. 52% would not use textbooks to study even when placed at disposal. In 2017 52% spent study time with social media (Twitter or Facebook), 66% “sometimes” questioned the validity of information posted by others in collaborative documents. To collaboratively study with peers, Google Docs and personal contacts were the top choices in 2017. |
| Prager & Liss 2019 [2] | OT | T | 54 | Surveyed the extent of teaching digital modalities and use for patient care in dental schools (54 out of 76 dental schools in U.S. and Canada responded) in February 2019. | 93% used CAD/CAM digital scanning, IOS was performed exclusively in 55%, extraoral model scan was used as sole technique in 8%, intra- and extraoral scanning in 37% of the schools. IOS was applied for crowns (100%), inlays/onlays (77%), implant crowns (52%), fixed partial denture (34%), complete denture (2%), but none of the schools indicated to use IOS always for crowns. 59% had a digital workflow established to deliver same-day restorations. 34% had at least 10% of faculty proficient in IOS, 66% had 10% or less. |
| Turkyilmaz et al. 2019 [89] | OT | T | 255 | Surveyed students’ perception of e-learning impact on dental education, response rate of 22.6% (255 out of 1130 electronically distributed 14-question surveys to 2nd–4th year students). | 48.6% preferred traditional lecture mixed with online learning, 18.4% online classes only, 18.0% traditional lecture style only; greatest impact on learning had YouTube, Bone Box, and Google. 60% spent between 1 and >4 h per day on electronic resources for academic performance. E-learning had a significant perceived effect on didactic and clinical understanding. Students observed that faculties estimated <50 years of age were more likely to incorporate e-learning into courses and more likely to use social media for communication. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zitzmann, N.U.; Matthisson, L.; Ohla, H.; Joda, T. Digital Undergraduate Education in Dentistry: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3269. https://doi.org/10.3390/ijerph17093269
Zitzmann NU, Matthisson L, Ohla H, Joda T. Digital Undergraduate Education in Dentistry: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(9):3269. https://doi.org/10.3390/ijerph17093269
Chicago/Turabian StyleZitzmann, Nicola U., Lea Matthisson, Harald Ohla, and Tim Joda. 2020. "Digital Undergraduate Education in Dentistry: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 9: 3269. https://doi.org/10.3390/ijerph17093269
APA StyleZitzmann, N. U., Matthisson, L., Ohla, H., & Joda, T. (2020). Digital Undergraduate Education in Dentistry: A Systematic Review. International Journal of Environmental Research and Public Health, 17(9), 3269. https://doi.org/10.3390/ijerph17093269