Health Impact Assessments in Spain: Have They Been Effective?

 ,
,
Abstract
:1. Background
2. Methods
- (1)
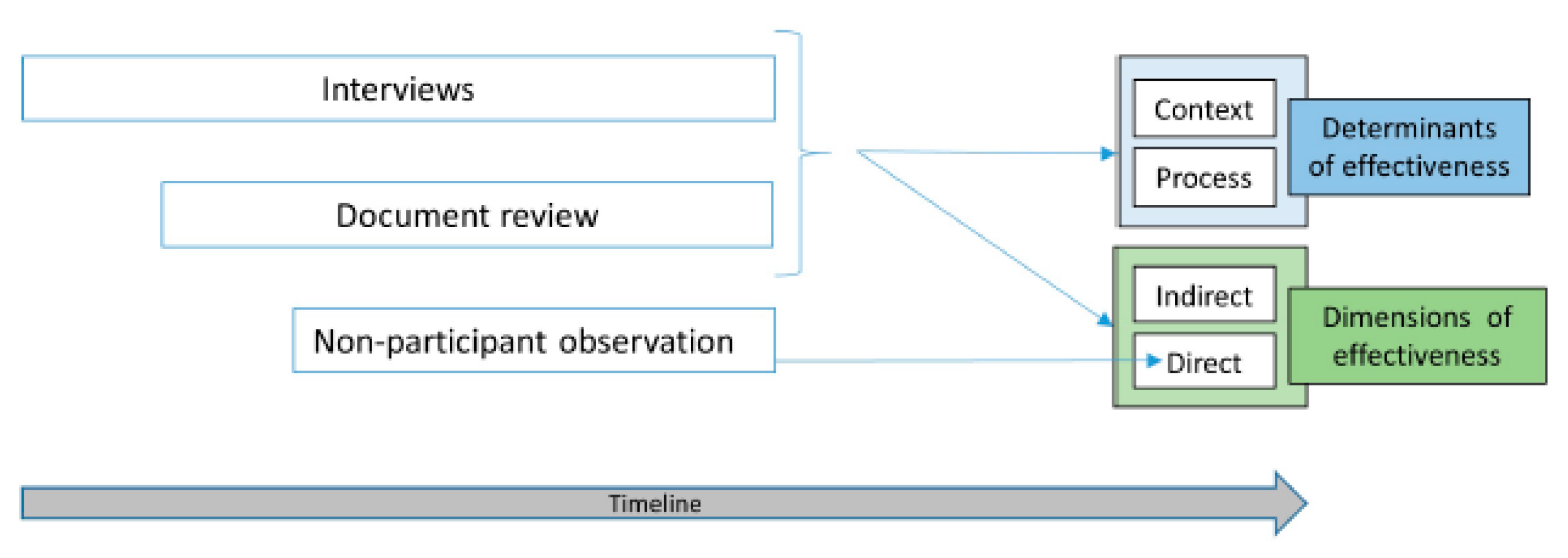
- Individual interviews with civil servants or politicians who participated in any of the HIAs or who had influence over or responsibility for decision-making in the projects are shown in Table 3. Purposive sampling was conducted, based on the intention of engaging informants from the health sector (or individuals responsible for the HIA) and from other sectors (participants in the HIA or nonparticipating decision-makers) for each HIA. Next, informants were added by snowball sampling, considering adequacy of the sample size to achieve data saturation, seeking diversity in points of view, and ensuring appropriateness of the individual (in terms of sector and role). The respondents were approached by telephone and mail. Finally, 14 interviews were carried out between October and December 2016, following a semi-structured interview guide (Supplementary Materials) based on Haigh et al.’s framework addressing both direct and indirect dimensions of HIA effectiveness and the context and process-related determinants of each HIA effectiveness. For direct effectiveness, the informants were asked how many of the recommendations of the HIA were finally carried out. For indirect effectiveness and the determinants of effectiveness, Haigh et al.’s categories related to learning and other distal impacts, as well as context and process aspects influencing HIAs effectiveness were tested. The interviews lasted approximately one hour and were conducted by the first author, who had training in interviews and focus groups. The major part of the interviews was conducted face-to-face at the respondents’ workplace. Written informed consents were obtained from all the interviewees and a processing of personal data were registered. The interviews were transcribed and manually analyzed through a thematic analysis. Haigh et al.’s categories were tested against the themes that were emerging. For each HIA, an explanatory framework about its effectiveness and its determinants was created and finally produced a list of the dimensions, categories and elements identified across the cases to compare them with each other.
- (2)
- Review of a range of different types of documents shown in Table 3 published—from 2005 to 2017 in English, Catalan or Spanish—and nonpublished. Search terms were related to the interventions denominations and the search databases were institutional websites, documentation centers, scientific meetings reports, social media and online press. The criterion for including the documents was that they contained descriptions, analysis or interpretation of the HIAs under analysis or related to the projects associated with the HIAs. Relevant information about the dimensions not fully covered by the interviews was collected. In addition, the document review provided a situated knowledge about each HIA context, that contributed to improve the analysis of interviews.
- (3)
- Nonparticipant observation in two settings (Bilbao and Barceloneta) where the HIAs were carried out, seeking to access information related to the impact of the recommendations of the HIA that we failed to obtain from the in-depth interviews. Observations, based on structured checking lists, were held in December 2016 by both the first and second authors in the case of Bilbao and by the first author in the case of Barceloneta. In the case of Bilbao, the places and features along the neighborhood that were built or modified by the regeneration project, such as the new elevators, the speed reduction elements, the new park, the accessibility improvements in the civic center, were observed. In the case of Barceloneta, features in the intervened blocks—such as elevators and renewed fronts—were checked.
3. Results
“As well as finally producing a series of recommendations, there was another objective, namely, learning and skills development and the handling of the tool […] certainly, this second objective was achieved to a greater extent than that related to the recommendations themselves”.
“We learnt that public health should abandon its traditional role of health authority in the context of intersectoral work”Health sector HIA promoter, Bay of Pasaia HIA
“Urban projects used to be developed from purely urban perspective. If we seek to improve people’s quality of life, we should take a more comprehensive approach, considering equity, equality, and gender criteria, and all the better if we think about this before the project”Environmental sector technician, Vitoria-Gasteiz HIA
“The HIA provided a new focus, which had not been considered until now, and was useful for establishing collaborations with certain sectors, such as urban planning”Health sector HIA promoter, Vitoria-Gasteiz HIA
“Now there is a greater involvement of the public health authority in the community, as an entity that can collaborate in certain fields, and that has something to say”Health sector HIA promoter, Bay of Pasaia HIA
“If this HIA was seen to be effective in some way, it was at the regional government level, when it came to encouraging, [and] teaching by showing the intervention to loads of people. In this sense, it did have an impact; I think, in fact, it had a big impact”Health sector technician, Bilbao HIA
“We worked under the framework of the health plan; one of its objectives was to reduce inequalities in health through interventions that evaluated the impact of non-health interventions on health equality. This was ideal”Health sector technician, Bilbao HIA
“It seemed to us that there was insufficient institutional support and political commitment [...]. Commitment is about assuming that failure is part of the process and a prerequisite for future success. So, I think that there is a long way to go at this level, even though it is included in the health plan...”Health sector HIA promoter, Bay of Pasaia HIA
“In the public administration, the organizational structure is very hierarchical, with very distinct levels, and we are very used to working vertically, and when we have to work horizontally, we find it difficult. We need to speak the same language and have a shared vision and common goals from the outset. This is about working by project rather than by management body”Participation sector technician, Barceloneta HIA
“The economic crisis [...], changes in political leadership at the local and regional levels [...] made the process difficult. They disrupted things and delayed us a lot, because they extended the time frame; we had to raise the question of the HIA with the various urban planning promoters and decision-makers all over again”.
“Every meeting [achieved] with the institutions was a victory, because they felt judged in some way [...]. The course of these projects was so complex and contentious, that it hampered transparency between the agents involved [...]. Moreover, it caused a wave of mistrust and skepticism among community about everything proposed by the government that made it difficult to be brought over discussion, reflection, participation”Health sector HIA promoter, Bay of Pasaia HIA
“[The lack of a formal agreement] made the follow-up difficult given the changes in political leadership and meant that the follow through on the recommendations was based on the good personal relationships established”Health sector HIA promoter, Alcalá de Guadaíra HIA
“We disguised it as a research project to soften its image compared to what an HIA is expected to do, namely, empower, enable real participation, etc. so that they would let us do it [...] it was more technical than political in nature”Health sector technician conducting Bilbao HIA
“It’s not clear to me that here people who shop in supermarkets have a poorer health than those who shop in local shops. I am not convinced that the evidence generated in the United Kingdom is generalizable to our setting”Health sector technician conducting Bilbao HIA
“It is essential to analyze and understand your context; if you don’t know it well enough, it’s going to be difficult to explain and manage future problems or difficulties, and it’s unlikely that the HIA will be effective”Health sector HIA promoter, Bay of Pasaia HIA
“In an HIA, we need to take into account time frames, in urban planning [...] interests converge, there is a need for time for all the procedures, legislative requirements [...] and it’s subject to twists and turns. Changes that considerably complicate matters and that can seriously slow the process. This translates into long waits and uncertainty for the community. HIA must bear in mind this impact on citizens and, at the same time, should adapt its own development to those circumstances”Health Sector HIA promoter, Bay of Pasaia HIA
“We must manage to develop efficient and practical tools that provide substantive knowledge and added value to the process that already exists, that are easy to use, such as evidence summaries [...] enabling integration of the HIA into procedures that are already carried out or health issues into other consultation procedures”Health sector technician conducting Alcalá de Guadaíra HIA
“I think that if we don’t establish a mutual understanding with decision-makers and obtain their commitment, the HIA might be completed, but the process would be much more tortuous and the implementation of the recommendations more difficult”Health sector HIA promoter, Bay of Pasaia HIA
“It is important that decision-makers are present, since this ensures that what has been drafted can be carried over to the design of the project”Environmental sector technician, Vitoria-Gasteiz HIA
“We executed the plan, made the investment, they commissioned a different plan and there we left it. Perhaps we failed to create strong enough links with the units at the municipal level responsible for implementing this type of policy for there to be follow through on these recommendations, beyond this specific project”Participation sector technician, Barceloneta HIA
“It was an interesting insight into how people see health impacts. They made proposals beyond the two specific interventions, which have also recently been accepted and budgeted for; in this sense, participation has been essential”Health sector HIA promoter, Bay of Pasaia HIA
“Thanks to the HIA, people have learnt about the characteristics of the projects, the positions of different parties [...]. No one changed their opinion, but they did improve their understanding other points of view”Health sector technician conducting Bay of Pasaia HIA
“[Monitoring on the ground] is what little by little may consolidate these intersectoral relationships and rebuild relationships where there have been tensions, because if not, we came, we asked questions and that’s it. Here we are and the health sector is presenting issues playing a role in the citizens’ everyday life. After two years, we want to know if there has been any change since that experience”Health sector HIA promoter, Bay of Pasaia HIA
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Commission on the Reduction of Social Inequalities in Health in Spain. Moving Forward Equity. A Proposal of Policies and Interventions to Reduce Social Inequalities in Health in Spain. Directorate General for Public Health and Foreign Health Ministry of Health, Social Policy and Equality, 2010. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/promocion/desigualdadSalud/docs/Moving_Forward_Equity.pdf (accessed on 23 April 2020).
- Marmot, M. Health equity in England: The Marmot review 10 years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I.; Gleicher, D. Governance for Health in the 21st Century; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Shankardass, K.; Solar, O.; Murphy, K.; Freiler, A.; Bobbili, S.; Bayoumi, A.; O’Campo, P. Health in All Policies: A Snapshot for Ontario, Results of A Realist-Informed Scoping Review of the Literature; Centre for Research on Inner City Health: Toronto, ON, Canada, 2011. [Google Scholar]
- Lawless, A.; Lane, A.; Lewis, F.-A.; Baum, F.; Harris, P. Social determinants of health and local government: Understanding and uptake of ideas in two Australian states. Aust. N. Z. J. Public Health 2016, 41, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Leeuw, E.; Kickbusch, I.; Palmer, N.; Spanswick, L. European Healthy Cities come to terms with health network governance. Heal. Promot. Int. 2015, 30, i32–i44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias, M.; Martí-Costa, M.; Subirats, J.; Tomàs, M. (Eds.) Políticas urbanas en España. Grandes Ciudades, Actores y Gobiernos; Icaria: Barcelona, Spain, 2011. [Google Scholar]
- Gutiérrez, A. Incidencia de la participación en las políticas de regeneración urbana en Cataluña: Actores, ciudadanía y desigual poder local. In Proceedings of the XIII Coloquio Internacional de Geocrítica, El control del Espacio y los Espacios de Control, Barcelona, Spain, 5–10 May 2014. [Google Scholar]
- Guglielmin, M.; Muntaner, C.; O’Campo, P.; Shankardass, K. A scoping review of the implementation of health in all policies at the local level. Heal. Policy 2018, 122, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Elliott, E.; Harrop, E.; Williams, G.H. Contesting the Science: Public Health Knowledge and Action in Controversial Land-Use Developments. In Risk Communication and Public Health; Oxford University Press (OUP): Glasgow, UK, 2010; pp. 181–196. [Google Scholar]
- World Health Organization. Health Organization. Health Impact Assessment—Main concepts and suggested approach. In Gothenburg Consensus Paper; European Centre for Health Police, WHO Regional Office for Europe: Brussels, Belgium, 2011. [Google Scholar]
- Delany, T.; Harris, P.; Williams, C.; Harris, E.; Baum, F.; Lawless, A.; Wildgoose, D.; Haigh, F.; MacDougall, C.; Broderick, D.; et al. Health Impact Assessment in New South Wales & Health in All Policies in South Australia: Differences, similarities and connections. BMC Public Health 2014, 14, 699. [Google Scholar] [CrossRef] [Green Version]
- Scott-Samuel, A.; Birley, M.; Ardern, K. The Merseyside Guidelines for Health Impact Assessment, 2nd ed.; International Health Impact Assessment Consortium: Liverpool, UK, 2001. [Google Scholar]
- Harris-Roxas, B.; Harris, E. The impact and effectiveness of health impact assessment: A conceptual framework. Environ. Impact Assess. Rev. 2013, 42, 51–59. [Google Scholar] [CrossRef]
- Krieger, G.R.; Utzinger, J.; Winkler, M.S.; Divall, M.J.; Phillips, S.; Balge, M.Z.; Singer, B.H. Barbarians at the gate: Storming the Gothenburg consensus. Lancet 2010, 375, 2129–2131. [Google Scholar] [CrossRef]
- Elliott, E.; Francis, S. Making effective links to decision-making: Key challenges for health impact assessment. Environ. Impact Assess. Rev. 2005, 25, 747–757. [Google Scholar] [CrossRef]
- Haigh, F.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Harris, P.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.; Spickett, J.; et al. The effectiveness of health impact assessment in influencing decision-making in Australia and New Zealand 2005–2009. BMC Public Health 2013, 13, 1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parry, J.; Kemm, J. Criteria for use in the evaluation of health impact assessments. Public Health 2005, 119, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Wismar, M.; Blau, J.; Ernst, K.; Figueras, J. The Effectiveness of Health Impact Assessment: Scope and limitations of Supporting Decision-Making in Europe; Observatory on Health Systems and Policies, World Health Organization: Copenhagen, Denmark, 2007. [Google Scholar]
- Harris, P.; Sainsbury, P.; Kemp, L. The fit between health impact assessment and public policy: Practice meets theory. Soc. Sci. Med. 2014, 108, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haigh, F.; Harris, E.; Harris, P.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.; et al. What makes health impact assessments successful? Factors contributing to effectiveness in Australia and New Zealand. BMC Public Heath 2015, 15, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law 33/2011, of October 4, on General Public Health. BOE Number 240. Available online: https://www.boe.es/eli/es/l/2011/10/04/33 (accessed on 23 April 2020).
- Bacigalupe, A.; Esnaola, S.; Calderón, C.; Zuazagoitia, J.; Aldasoro, E. Health impact assessment of an urban regeneration project: Opportunities and challenges in the context of a southern European city. J. Epidemiology Community Heath 2009, 64, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Morteruel, M.; Díez, E. Health Impact Assessment of Buildings Rehabilitation Measures in a Neighbourhood of Barcelona. 2011. Available online: http://si.easp.es/eis2011/wp-content/uploads/2011/04/HIA11_Book_of_abstracts.pdf (accessed on 23 April 2020).
- Venegas-Sánchez, J.; Rivadeneyra-Sicilia, A.; Bolívar-Muñoz, J.; Fernandez, L.A.L.; Martin-Olmedo, P.; Fernández-Ajuria, A.; Daponte-Codina, A.; Ruiz-Fernández, J.; Purroy, C.A. Evaluación del impacto en la salud del proyecto de reurbanización de la calle San Fernando en Alcalá de Guadaíra (Sevilla). Gac. Sanit. 2013, 27, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano, E.; Larrañaga, I.; Morteruel, M.; De Ros, M.D.B.; Basterrechea, M.; Martinez, D.; Aldasoro, E.; Bacigalupe, A. Urban regeneration as population health intervention: A health impact assessment in the Bay of Pasaia (Spain). Int. J. Equity Health 2016, 15, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez, F.; Estibalez, J.J. Health Impact Assessment of the Tunnelling of the Railroad in Vitoria-Gasteiz, Spain. 2011. Available online: http://si.easp.es/eis2011/wp-content/uploads/2011/04/HIA11_Book_of_abstracts.pdf (accessed on 23 April 2020).
- Departamento de Salud, Gobierno Vasco. Políticas de Salud para Euskadi. 2013–2020. Vitoria-Gasteiz: Departamento de Salud, Gobierno Vasco. 2013. Available online: https://www.euskadi.eus/contenidos/informacion/plan_salud_2013_2020/es_def/adjuntos/plan_salud_2013_2020-web%2012_03_2018.pdf (accessed on 23 April 2020).
- Esnaola, S.; Bacigalupe, A.; Calderón, C.; Zuazagoitia, J.; Aldasoro, E. Evaluación del Impacto en la Salud del Plan de Reforma Integral de Uretamendi-Betolaza y Circunvalación; Departamento de Sanidad y Consumo: Vitoria-Gasteiz, Spain, 2008. [Google Scholar]
- Diagnóstico, Perfil y Plan de Desarrollo de la Salud de Vitoria-Gasteiz. 2007-2009. Departamento de Salud y Consumo. Ayuntamiento de Vitoria-Gasteiz. Available online: https://www.vitoria-gasteiz.org/docs/wb021/contenidosEstaticos/adjuntos/es/52/87/5287.pdf (accessed on 23 April 2020).
- Law 2/2004, of June 4, on the Improvement of Neighborhoods, Urban Areas and Towns Requiring Special Attention. DOGC, No. 4151.
- Decree 169/2014 of 9 December Establishing the Health Impact Assessment Procedure of the Autonomous Community of Andalusia. BOJA, No. 243.
- Serrano, E.; Larrañaga, I.; Tolosana, E.S.; Baixas, M.D.; Basterrechea, M.; Conde, F.; Aldasoro, E. Evaluación del impacto en salud de intervenciones de regeneración en la bahía de Pasaia: Percepciones de la población afectada. Gac. Sanit. 2014, 28, 442–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano, E.; Larrañaga, I.; Morteruel, M.; De Ros, M.D.B.; Basterrechea, M.; Martinez, D.; Aldasoro, E.; Bacigalupe, A. Evaluación del Impacto en la Salud de dos Intervenciones de Regeneración en la Bahía de Pasaia. Vitoria-Gasteiz: Departamento de Salud del Gobierno Vasco. Available online: http://www.euskadi.eus/contenidos/informacion/publicaciones_departamento/es_def/adjuntos/salud_publica/eval_impacto_salud_bahia_pasaia.pdf (accessed on 23 April 2020).
- Dannenberg, A.L. Effectiveness of Health Impact Assessments: A Synthesis of Data from Five Impact Evaluation Reports. Prev. Chronic Dis. 2016, 13, 150559. [Google Scholar] [CrossRef] [PubMed]
- Rhodus, J.; Fulk, F.; Autrey, B.; O’Shea, S.; Roth, A. A Review of Health Impact Assessments in the U.S.: Current State-of-Science, Best Practices, and Areas for Improvement; US Environmental Protection Agency, Office of Research and Development: Cincinnati, OH, USA, 2013.
- Bourcier, E.; Charbonneau, D.; Cahill, C.; Dannenberg, A.L. An Evaluation of Health Impact Assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davenport, C.; Mathers, J.; Parry, J. Use of health impact assessment in incorporating health considerations in decision making. J. Epidemiol. Community Health 2006, 60, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spickett, J.; Katscherian, D.; Brown, H.; Rumchev, K. Health Impact Assessment: Improving Its Effectiveness in the Enhancement of Health and Well-Being. Int. J. Environ. Res. Public Health 2015, 12, 3847–3852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQueen, D.; Wismar, M.; Lin, V.; Jones, C.M.; Davies, M. (Eds.) Intersectoral Governance for Health in All Policies. Structures, Actions and Experiences; World Health Organization: Copenhagen, Denmark, 2012. [Google Scholar]


{kind=link}
| UBC (Bilbao) HIA | Vitoria-Gasteiz HIA | Barceloneta HIA | Alcalá de Guadaíra HIA | Bay of Pasaia HIA | |
|---|---|---|---|---|---|
| Project framework | Comprehensive reform plan for the neighborhood Uretamendi-Betolaza bypass (Bilbao) | Construction works associated with an urban masterplan involving burying the railway tracks underground as they pass through the city | Comprehensive intervention plan (neighborhood law) for the Barceloneta neighborhood (Barcelona) | Regeneration measures (with in the “Plan Urban” project) for the San Miguel neighborhood in Alcalá de Guadaíra | Masterplan for redevelopment of the Bay of Pasaia |
| Year | 2005–2006 | 2007 | 2008–2009 | 2010 | 2012–2013 |
| Interventions analyzed | -Improvements in access within the neighborhood and to the rest of the city accessibility -Redevelopment of various areas in the neighborhood and creation of green spaces | -Construction of new structures and development of services -Planning of uses for the space gained | -A comprehensive housing rehabilitation program | -Improvements in access to the neighborhood -Redevelopment of a street | -Construction of a new wholesale fish market, freeing up ground-level space -No action being taken to regenerate an abandoned area |
| Determinants of Effectiveness (Haigh et al., 2015) | Present? | ||
|---|---|---|---|
| Yes | Yes, Partially | No | |
| Decision-making context | |||
| Alignment of the project and HIA values | Alignment of all values | Alignment of some values | No alignment of values |
| Alignment of the project and HIA formal objectives | Alignment of all objectives | Alignment of some objectives | No alignment of objectives |
| A suitable stage of planning of the project in order to make recommendations | The project is well defined: it is easy to make recommendations | The project is poorly defined: it is difficult to make recommendations | The project is not defined: no recommendations can be made |
| Key elements for the HIA | |||
| Based on available evidence and knowledge | Availability of several types of evidence, knowledge and skills necessary for the HIA | Lack of certain types of evidence, knowledge or skills necessary for the HIA | Complete lack of evidence, knowledge or skills for the HIA |
| Economic resources | Sufficient economic resources to fully the execute the HIA | Limited economic resources, constraining the execution of the HIA | No economic resources to execute the HIA |
| Procedures | |||
| Participation of key agents in decision-making | Participation of key agents in the steering committee throughout the process | Limited participation of key agents in the process | No participation of key agents |
| Community participation | Community representation in the HIA steering committee or extensive community participation | No community representation in the HIA steering committee and limited community participation | No community participation |
| Transparency and accountability in the HIA | Full process transparency between authorities and towards the community and a plan to follow-up on recommendations | Limited process transparency and/or follow-up of recommendations without an established plan | No transparency or follow-up |
| HIA | Interviews Role in HIA | Main Contributions to Results | Document Review | Main Contributions to Results | Nonparticipant Observation | Main Contributions to Results | |
|---|---|---|---|---|---|---|---|
| Role in HIA | Professional Position When HIA (Current Position, If Different) | ||||||
| Bilbao | 1.Health sector technician conducting HIA | 1. Public Health technician at the autonomous government (University lecturer) | -Evidence to verify the direct and indirect HIA effectiveness and its determinants | -Health Plan of the Basque Country [28] -HIA-related scientific articles and institutional reports [23,29] -Historical documents -News articles -Social platforms websites | -Evidence to verify the contextual and process-related determinants of HIA effectiveness | -Work carried out on the regeneration plan in accordance with the HIA recommendations | -Evidence to verify the direct HIA effectiveness |
| Vitoria-Gasteiz | 1.Health sector HIA promoter 2.Environmental sector HIA technician | 1. Head of Public Health Department at the local level 2. Environmental Health technician at the local level | -Evidence to verify the indirect HIA effectiveness and its determinants | -Health Plan of Vitoria-Gasteiz [30] -HIA-related documents and institutional reports [27] | -Evidence to verify the contextual and process-related determinants of HIA effectiveness | - | - |
| Barceloneta | 1.Health sector HIA promoter 2.City Development sector HIA participant 3. Citizen Participation sector HIA participant | 1. Public Health technician at the local level 2. City Development technician (Municipal District Manager) 3. Citizen Participation technician (Director of a Municipal District Department) | -Evidence to verify the direct and indirect HIA effectiveness and its determinants | -HIA-related scientific documents and institutional reports [24] -Neighborhoods Plan documents -Autonomous Neighborhoods Law [31] -Historical documents -News articles -Social platforms websites | -Evidence to verify the contextual and process-related determinants of HIA effectiveness | -Work carried out on the regeneration plan in accordance with the HIA recommendations | -Evidence to verify the direct HIA effectiveness |
| Alcalá de Guadaíra | 1. Health sector HIA promoter 2. Health sector technician conducting HIA | 1. Director of Public Health institution at the autonomous government (Public Health consultant) 2. Public health technician at the autonomous government (University lecturer) | -Evidence to verify the direct and indirect HIA effectiveness and its determinants | -HIA-related scientific articles and institutional reports [25] -Regeneration Plan documents -Autonomous HIA legislation [32] -News articles | -Evidence to verify the contextual and process-related determinants of HIA effectiveness | - | - |
| Bahía de Pasaia | 1. Health sector HIA promoter 2. Health sector technician conducting HIA | 1. Deputy Director of Public Health at the autonomous government 2. Public Health technician at the autonomous government | -Evidence to verify the direct and indirect HIA effectiveness and its determinants | -Health Plan of the Basque Country [28] -HIA-related scientific articles and institutional reports [26,33,34] -Historical documents -News articles -Social platforms websites | -Evidence to verify the contextual and process-related determinants of HIA effectiveness | - | - |
| Bilbao HIA | Vitoria-Gasteiz HIA | Barceloneta HIA | Alcalá de Guadaíra HIA | Bay of Pasaia HIA | |
|---|---|---|---|---|---|
| DIRECT EFFECTIVENESS | |||||
| Total number of recommendations adopted | 5/23 (21.7%) | . | 5/8 (62.5%) | 11/19 (57.9%) | 3/26 (11.5%) |
| Additional to the projects | 1/7 (14.3%) | . | 2/3 (66.6%) | 2/4 (50%) | 2/11 (18.2%) |
| Regarding the design of the projects | 4/7 (57.1%) | . | 3/5 (60%) | 2/3 (66.6%) | 1/14 (7.1%) |
| Regarding the construction work phase | ? | . | . | 7/12 (58.3%) | 0/1 (0%) |
| Changes in social determinants of health | |||||
| Physical environment/housing | +++ | . | + | . | ++ |
| Employability, social inclusion and cohesion | ? | . | . | ++ | ? |
| INDIRECT EFFECTIVENESS | |||||
| Learning | |||||
| Conceptual | ✓ | ✓✓ | ✓ | ✓✓ | ✓ |
| Technical | ✓ | ✓ | ✓ | ✓ | ✓ |
| Social | . | ✓✓ | ✓ | ✓ | ✓✓ |
| Strengthening of intersectoral action | . | ✓ | ✓ | ✓ | ✓✓ |
| Impact on other actions | ✓ | . | ✓ | ✓✓ | ✓ |
| Other indirect impacts | ✓ | . | . | ✓ | ✓✓ |
| Determinants of the Effectiveness of the HIAs | Bilbao | Vitoria-Gasteiz | Barceloneta | Alcalá de Guadaíra | Bahía de Pasaia | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Present? | DE | IE | Present? | DE | IE | Present? | DE | IE | Present? | DE | IE | Present? | DE | IE | ||
| CONTEXT | Institutional context for the HIA | |||||||||||||||
| Institutionalization of the social model of health | Yes | Yes | Yes | Yes | Yes | |||||||||||
| Political commitment to the HIA | No | Yes | No | No | No | |||||||||||
| Socio-political and economic context | ||||||||||||||||
| Economic crisis | No | / | / | Yes | No | / | / | Yes | Yes | |||||||
| Electoral situation | No | / | / | No | / | / | No | / | / | Yes | Yes | |||||
| Social and institutional conflicts | Yes | No | / | / | Yes | Yes | Yes | |||||||||
| Decision-making context | ||||||||||||||||
| Understanding between the stakeholders | No | Yes | Yes | Yes | No | |||||||||||
| Formal agreement on the HIA | Yes | Yes | No | No | No | |||||||||||
| Alignment with HIA values | No | Yes | Partial | Partial | No | |||||||||||
| Alignment with HIA objectives | No | Yes | Partial | Partial | Partial | |||||||||||
| Good timing for the HIA | Yes | Partial | Yes | Yes | Yes | |||||||||||
| PROCESS | Key elements of the HIA | |||||||||||||||
| Evidence and knowledge available | Yes | Partial | Partial | Yes | Yes | |||||||||||
| Sufficient resources for the HIA | Yes | Yes | Partial | Partial | Yes | |||||||||||
| Flexibility and adaptability of the HIA | Yes | Yes | Yes | Yes | Yes | |||||||||||
| Procedures | ||||||||||||||||
| Involvement and participation of key agents | Partial | Yes | Yes | Yes | Partial | |||||||||||
| Community participation | Yes | No | Partial | Yes | Yes | |||||||||||
| Transparency and accountability | Partial | Partial | Partial | Partial | Partial | |||||||||||
| INDIVIDUAL DIMENSION (CROSS-CUTTING) | ||||||||||||||||
| Individual agency and proactiveness | Yes | Yes | Yes | Yes | Yes | |||||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morteruel, M.; Bacigalupe, A.; Aldasoro, E.; Larrañaga, I.; Serrano, E. Health Impact Assessments in Spain: Have They Been Effective? Int. J. Environ. Res. Public Health 2020, 17, 2959. https://doi.org/10.3390/ijerph17082959
Morteruel M, Bacigalupe A, Aldasoro E, Larrañaga I, Serrano E. Health Impact Assessments in Spain: Have They Been Effective? International Journal of Environmental Research and Public Health. 2020; 17(8):2959. https://doi.org/10.3390/ijerph17082959
Chicago/Turabian StyleMorteruel, Maite, Amaia Bacigalupe, Elena Aldasoro, Isabel Larrañaga, and Elena Serrano. 2020. "Health Impact Assessments in Spain: Have They Been Effective?" International Journal of Environmental Research and Public Health 17, no. 8: 2959. https://doi.org/10.3390/ijerph17082959