A Systematic Review of the Effectiveness of Concussion Education Programs for Coaches and Parents of Youth Athletes



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
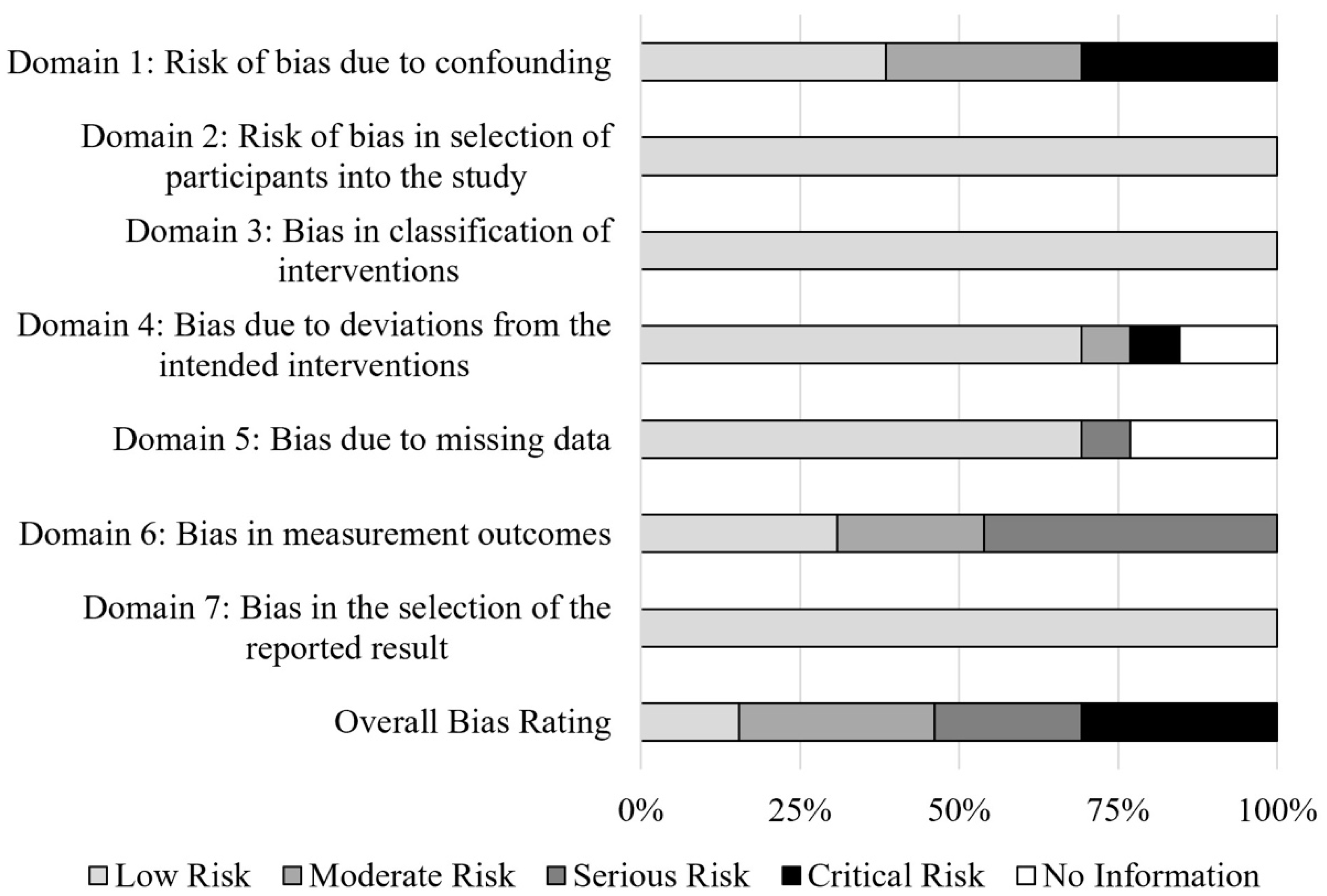
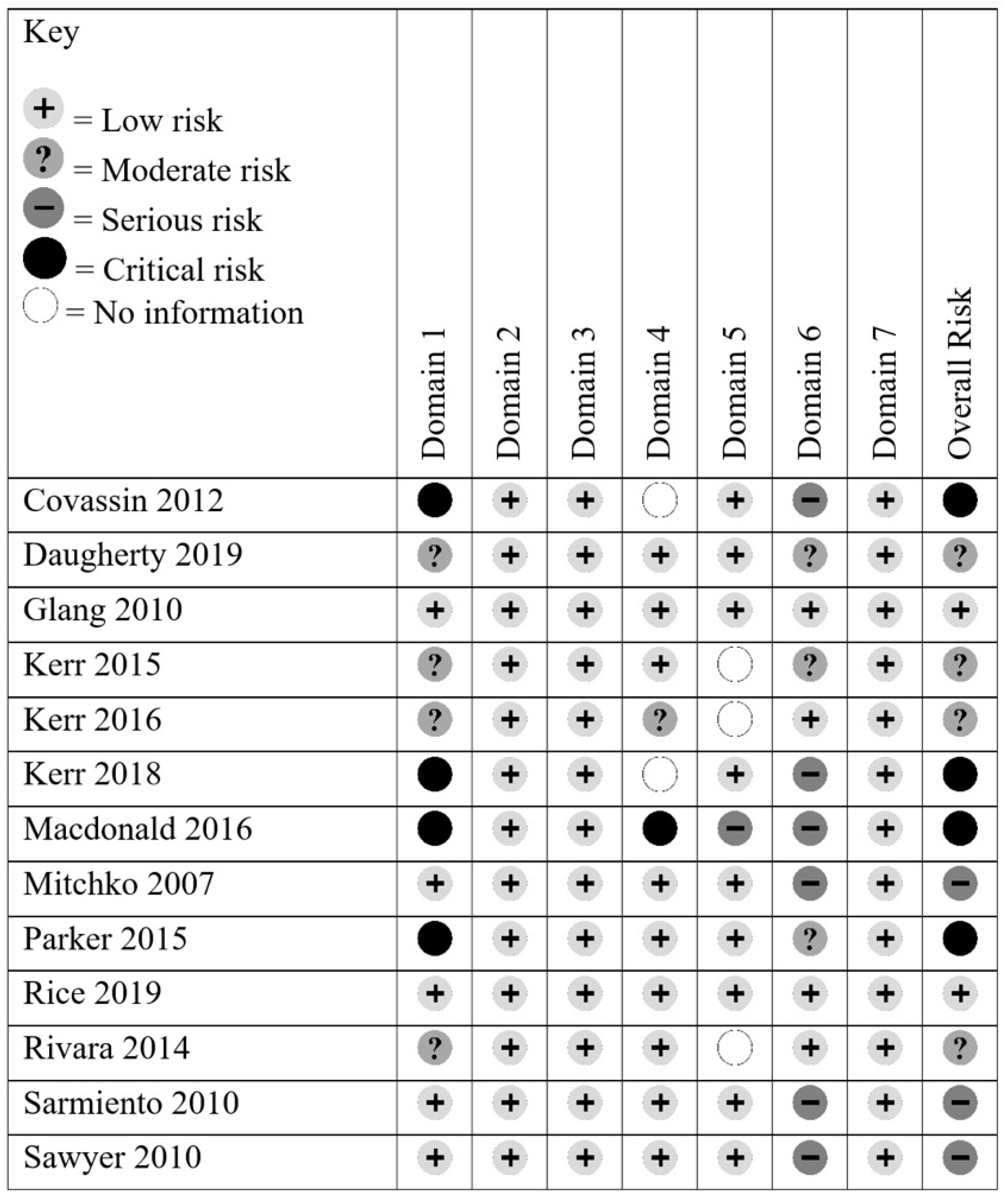
2.4. Risk of Bias
3. Results
3.1. Data Synthesis
3.2. Risk of Bias in Included Studies
3.3. Review of Programs
3.3.1. ACTive: Athletic Concussion Training™ for Coaches (ACTive™)
3.3.2. USA Football’s Heads Up Football (HUF)
3.3.3. CDC HEADS UP
3.3.4. Parent Programs
3.3.5. Comparison of Concussion Education Program Content
3.4. Evaluation of Eduction Program Materials and Implementation
3.4.1. USA Football’s Heads Up Football
3.4.2. CDC HEADS UP: Concussion in High School Sports
3.4.3. CDC HEADS UP: Concussion in Youth Sports
3.4.4. Parent Interventions
3.5. Evaluation of Eduction Program Effectiveness
3.5.1. ACTive: Athletic Concussion Training™ for Coaches (ACTive™)
3.5.2. CDC HEADS UP Concussion in Programs for Coaches
3.5.3. CDC Concussion Education Programs—Parent Outcomes
3.6. Educational Programs and Concussion Epidemiology
3.6.1. USA Football’s Heads Up Football
3.6.2. Non-Specified Programs for Coaches
4. Discussion
4.1. Program Content
4.2. Use and Implementation of Concussion Education Programs by Coaches
4.3. Influence of Education Programs on Coach Knowledge
4.4. Education Programs for Parents
4.5. Coach Concussion Education and Youth Athlete Health Outcomes
4.6. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Halstead, M.E.; Walter, K.D. Sport-Related Concussion in Children and Adolescents. Pediatrics 2010, 126, 597–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feiss, R.S.; Lutz, M.; Moody, J.R.; Pangelinan, M.M. A systematic review of coach and parent knowledge of concussion. J. Concussion 2020, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covassin, T.; Elbin, R.; Sarmiento, K. Educating coaches about concussion in sports: Evaluation of the CDC’s “Heads Up: Concussion in Youth Sports” initiative. J. Sch. Health 2012, 82, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, J.; DePadilla, L.; Sarmiento, K. Effectiveness of the US Centers for Disease Control and Prevention HEADS UP coaches’ online training as an educational intervention. Health Educ. J. 2019, 78, 784–797. [Google Scholar] [CrossRef] [PubMed]
- Glang, A.; Koester, M.; Beaver, S. Online training in sports concussion for youth sports coaches. Int. J. Sport. Sci. Coach. 2010, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, Z.; Dalton, S.; Roos, K.; Djoko, A.; Phelps, J.; Dompier, T. Comparison of Indiana High School Football Injury Rates by Inclusion of the USA Football “Heads Up Football” Player Safety Coach. Orthop. J. Sport. Med. 2016, 4, 2325967115610545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, Z.Y.; Kroshus, E.; Lee, J.G.L.; Yeargin, S.W.; Dompier, T.P. Coaches’ Implementation of the USA Football “Heads Up Football” Educational Program. Health Promot. Pract. 2018, 19, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Kerr, Z.; Yeargin, S.; McLeod, T.; Nittoli, V.; Mensch, J.; Dodge, T.; Hayden, R.; Dompier, T. Comprehensive coach education and practice contact restriction guidelines result in lower injury rates in youth American football. Orthop. J. Sport. Med. 2015, 3, 2325967115610545. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, I.; Hauber, R. Educating parents on sports-related concussions. J. Neurosci. Nurs. 2016, 48, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Mitchko, J.; Huitric, M.; Sarmiento, K.; Hayes, G.; Pruzan, M.; Sawyer, R. CDC’s approach to educating coaches about sports-related concussion. Am. J. Heal. Educ. 2007, 38, 99–103. [Google Scholar] [CrossRef]
- Parker, E.; Gilchrist, J.; Schuster, D.; Lee, R. Reach and knowledge change among coaches and other participants of the online course: “Concussion in sports: What you need to know”. J. Head Trauma Rehabil. 2015, 30, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.; Curtis, R. Parental knowledge of concussion: Evaluation of the CDC’s “Heads up to parents” educational initiative. J. Safety Res. 2019, 69, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivara, F.F.P.; Schiff, M.M.A.; Chrisman, S.P.S.; Chung, S.K.; Ellenbogen, R.G.; Herring, S.A. The Effect of Coach Education on Reporting of Concussions Among High School Athletes After Passage of a Concussion Law. Am. J. Sports Med. 2014, 42, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, K.; Mitchko, J.; Klein, C.; Wong, S. Evaluation of the Centers for Disease Control and Prevention’s concussion initiative for high school coaches: “Heads Up: Concussion in High School Sports”. J. Sch. Health 2010, 80, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, R.J.; Hamdallah, M.; White, D.; Pruzan, M.; Mitchko, J.; Huitric, M. High School Coaches’ Assessments, Intentions to Use, and Use of a Concussion Prevention Toolkit: Centers for Disease Control and Prevention’s Heads Up: Concussion in High School Sports. Health Promot. Pract. 2010, 11, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ORCAS ACTive 2011. Available online: http://www.activecoach.orcasinc.com/ (accessed on 9 January 2020).
- Center for Disease Control HEADS UP 2017. Available online: https://www.cdc.gov/headsup/index.html (accessed on 9 January 2020).
- USA Football Heads Up Football 2012. Available online: https://nfhslearn.com/home/huf_certification (accessed on 9 January 2020).
- Guskiewicz, K.M.; Bruce, S.L.; Cantu, R.C.; Michael, S.; Kelly, J.P.; McCrea, M.; Putukian, M.; Mcleod, T.C.V. National Athletic Trainers ’ Association Related Concussion. J. Athl. Train. 2004, 39, 280–297. [Google Scholar] [PubMed]
- McCrory, P.; Meeuwisse, W.; Johnston, K.; Dvorak, J.; Aubry, M.; Molloy, M.; Cantu, R. Consensus Statement on Concussion in Sport—The Third International Conference on Concussion in Sport Held in Zurich, November 2008. Phys. Sportsmed. 2009, 37, 141–159. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| References | Educational Program | Number of Participants, Participant Details | Format, Number of Sessions | Outcome Measures | Key Findings |
|---|---|---|---|---|---|
| Covassin et al., 2012 [4] | CDC HEADS UP: Concussion in Youth Sport | 340, youth sport coaches | Online survey, 6 months after receiving CDC materials | Attitudes/beliefs about concussion; post-concussion actions taken by coaches; opinion/use of CDC materials | After viewing educational materials, the majority of coaches reported viewing concussions as a serious or very serious issue and took the proper actions after an athlete was suspected of a concussion; fact sheet for coaches was the most useful material |
| Daugherty et al., 2019 [5] | CDC HEADS UP: Concussion in Youth Sport | 179,469, youth and high school sport coaches (154,807 youth, 13,043 high school, 11,619 both) | Online surveys, pre- and post-exposure to CDC HEADS UP online training | General concussion knowledge; concussion management; attitudes/beliefs about concussion; intention and self-efficacy in concussion management and prevention | Coaches showed improved knowledge scores after reviewing the material in the online program, particularly for the moderate- and high-difficulty knowledge questions; coaches felt more confident in their ability to recognize concussion symptoms in youth athletes and help an athlete with the return-to-play process; coaches reported being more likely to talk with their athletes about concussions |
| Glang et al., 2010 [6] | ACTive: Athletic Concussion Training using Interactive Video Education | 75, youth sport coaches (40 treatment, 35 control) | RCT, online survey, pre- and post-exposure to ACTive program materials | General concussion knowledge; concussion management; attitudes/beliefs about concussion; intention and self-efficacy in concussion management and prevention | Coaches who were exposed to the ACTive program materials increased their general knowledge, signs and symptoms knowledge, knowledge of misperceptions, and reported greater self-efficacy and behavioral intention to respond correctly to possible concussions |
| Kerr et al., 2016 [7] | Heads Up Football (HUF) | 6, high school football teams | Compared teams with and without the HUF programs player safety coach (PSC) component | Number of concussions | Players on teams whose staff received only the online education experienced more concussions than those whose staff received the full program including in-person training |
| Kerr et al., 2018 [8] | Heads Up Football (HUF) | 1316, football coaches | Online survey, interactions with the player safety coach, implementation of the HUF educational materials | Player safety coach on-site presence during practices; coaches rated their implementation of HUF educational program components | Player safety coach was thought to be important, but rarely seen at practice; coaches implemented most aspects of the program but some did not educate players regarding recognizing concussions |
| Kerr et al., 2015 [9] | Heads Up Football (HUF) | 15, youth football teams, players ages 8–15 (mean age = 11.7) | Compared teams with and without exposure to HUF program and a player safety coach (PSC) | Number of head impacts; number of concussions | Players on teams whose staff had been exposed to HUF training and had a PSC experienced significantly less head impacts during practice than those whose coaches had not completed the training |
| Macdonald and Hauber, 2016 [10] | CDC HEADS UP Concussion Online Training; CDC HEADS UP to School: Know Your Concussion ABCs; Know the Impact: Concussion Awareness | 29, parents of high school football players | Paper survey, post-exposure to all three educational tools | Impact of each educational tool on concussion knowledge, perception, and awareness | CDC HEADS UP Concussion Online Training had the greatest influence on concussion knowledge, perception, and awareness, but was also ranked as the most confusing; CDC HEADS UP to School: Know Your Concussion ABCs was ranked as the tool most seemingly targeted for parents; most parents had no desire to seek out more information regarding concussion after the study |
| Mitchko et al., 2007 [11] | CDC HEADS UP: Concussion in High School Sports | 500, high school coaches | Online survey | Initial evaluation of the CDC HEADS UP Concussion in High School Sports toolkit | The majority of coaches found the toolkit useful; 1/3 of coaches did not have access to concussion education materials prior to receiving the toolkit |
| Parker et al., 2015 [12] | CDC HEADS UP Concussion in Sports: What You Need to Know online course | 133,764, coaches who completed the CDC online course | Online survey, pre- and post-exposure to online educational course | General concussion knowledge; concussion management, diagnosis, and return to play | At least 86% of coaches correctly answered questions related to general knowledge, management, and return to play on the pre-test, increasing to 97.5% on the post-test; greatest improvement was seen in diagnosis as scores increased over 37% from pre- to post-test |
| Rice and Curtis, 2019 [13] | CDC HEADS UP Concussion Awareness Video and Concussion Fact Sheet for Parents | 140 parents of youth club athletes | RCT, online survey pre- and post-exposure to one of the intervention materials | General concussion knowledge; signs and symptoms of concussion, and concussion management | Parent knowledge improved similarly with both interventions; parents successfully identified most signs and symptoms, but also often identified “red herring” signs as true signs of concussion and struggled to identify mood- and sleep-related symptoms; pre-test score and receiving concussion information prior to the intervention were the strongest predictors of post-test knowledge |
| Rivara et al., 2014 [14] | Multiple modalities (written, video, PowerPoint, 6-item quiz, and in-person training) | 40, high school football and women’s soccer coaches; 778, parent–player dyads on coaches’ teams | Coach survey, parent/player phone call to report number of practices/games players participated in, if they had suffered a hit associated with concussive symptoms, their coach’s awareness of the concussion | Coach awareness of concussion; education modality coach was exposed to; number athletes playing with symptoms | Coaches using the video or quiz were 50% or 40% less likely to be aware of concussion; no difference in awareness between number of modalities coach was exposed to; 69% of athletes reported playing with concussive symptoms |
| Sarmiento et al., 2010 [15] | CDC HEADS UP: Concussion in High School Sports | 333, high school coaches | Paper survey | Use of toolkit; knowledge, attitudes, and behaviors towards concussion prevention | The booklet was most used tool; coaches, especially those who implemented multiple aspects of the toolkit, reported learning something new about concussions, regarding concussions more seriously, and changing the waythey prevent or manage concussions |
| Sawyer et al., 2010 [16] | CDC HEADS UP: Concussion in High School Sports | 497, high school coaches | Telephone survey, 2–7 weeks after receiving educational toolkit | Use of/plans to use the toolkit materials; overall opinions of the toolkit | Overall, coaches had either used or planned to use the majority of the materials in the toolkit and found it to be visually appealing and easy to use |
| Content | ACTive | USA Football’s Heads Up Football | CDC HEADS UP to Youth Sports | CDC HEADS UP to High School Sports | CDC HEADS UP to Parents | ||||
|---|---|---|---|---|---|---|---|---|---|
| Video | Written Materials | Concussion Video | Blocking/Tackling Video | Video | Written Materials | Video | Written Materials | Written Materials | |
| General Information | |||||||||
| Injury does not always occur via direct hit to head | ✓ | — | — | — | ✓ | — | — | — | — |
| Injury mechanism | ✓ | — | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| How a concussion is diagnosed | — | — | — | — | ✓ | — | — | — | — |
| Signs and Symptoms | |||||||||
| Cognitive | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Physical | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Emotional | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sleep | ✓ | ✓ | ✓ | — | — | — | ✓ | — | — |
| Loss of consciousness is not necessary for diagnosis | ✓ | — | ✓ | — | ✓ | — | ✓ | — | — |
| Concussion Management | |||||||||
| Risks of second concussion | ✓ | — | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Longer recovery time for youth athletes | ✓ | — | ✓ | — | — | — | ✓ | — | — |
| Higher risk for youth athletes | ✓ | — | ✓ | — | ✓ | — | ✓ | — | — |
| Signs emergency care is required | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Return to Play | |||||||||
| An athlete suspected of a concussion must be immediately removed from play | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| A concussed athlete must be cleared by a physician to begin the return-to-play process | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Gradual return-to-play process | ✓ | ✓ | ✓ | — | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sport-Specific Recommendations | — | — | — | ✓ | — | — | — | ✓ | — |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feiss, R.; Lutz, M.; Reiche, E.; Moody, J.; Pangelinan, M. A Systematic Review of the Effectiveness of Concussion Education Programs for Coaches and Parents of Youth Athletes. Int. J. Environ. Res. Public Health 2020, 17, 2665. https://doi.org/10.3390/ijerph17082665
Feiss R, Lutz M, Reiche E, Moody J, Pangelinan M. A Systematic Review of the Effectiveness of Concussion Education Programs for Coaches and Parents of Youth Athletes. International Journal of Environmental Research and Public Health. 2020; 17(8):2665. https://doi.org/10.3390/ijerph17082665
Chicago/Turabian StyleFeiss, Robyn, Molly Lutz, Elaine Reiche, Justin Moody, and Melissa Pangelinan. 2020. "A Systematic Review of the Effectiveness of Concussion Education Programs for Coaches and Parents of Youth Athletes" International Journal of Environmental Research and Public Health 17, no. 8: 2665. https://doi.org/10.3390/ijerph17082665