High Level of Physical Activity Reduces the Risk of Renal Progression in Hypertensive Patients


Abstract
:1. Introduction
2. Materials and Methods
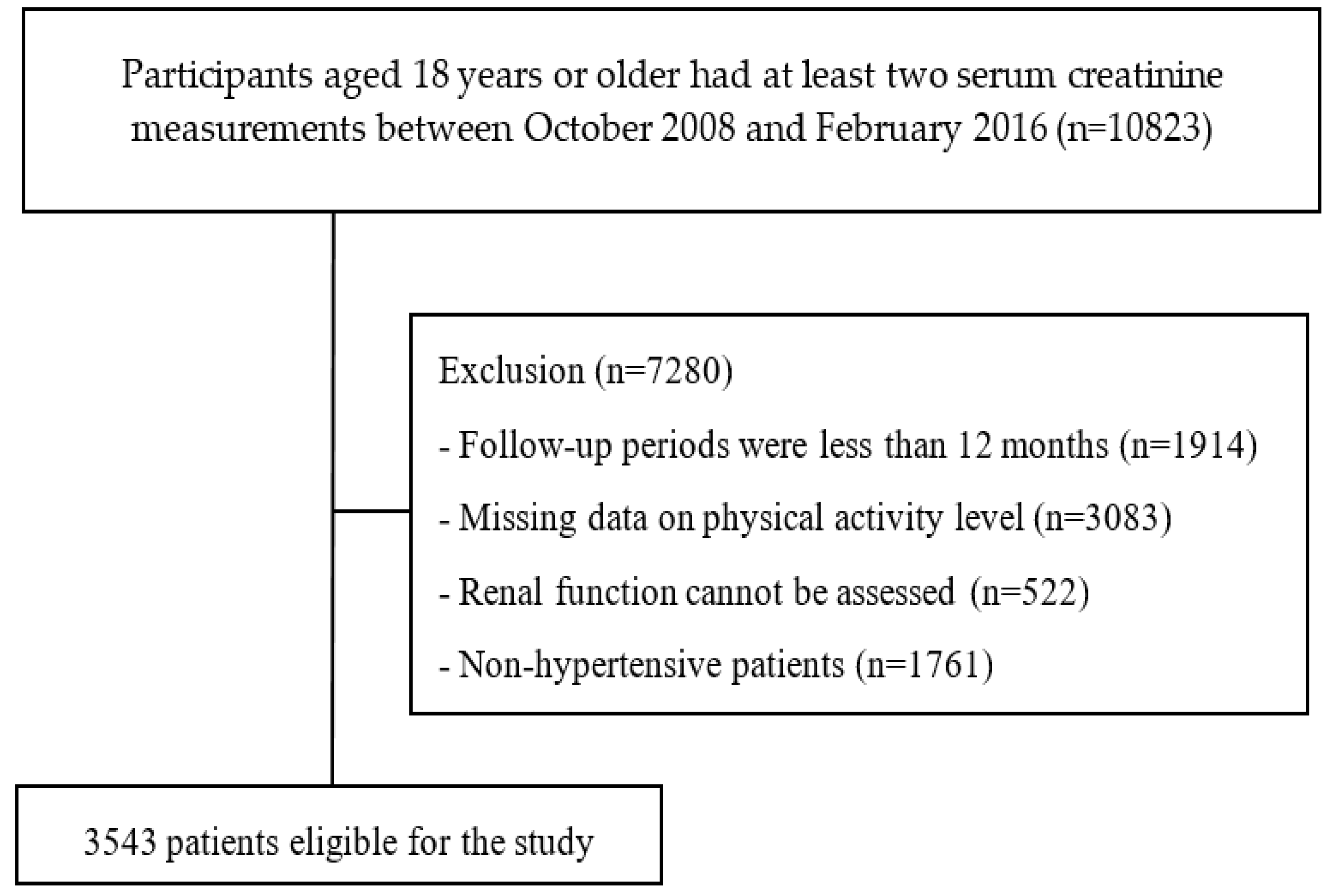
2.1. Study Population
2.2. Study Variables and Definitions
2.3. Physical Activities Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Whelton, P.K. Epidemiology of hypertension. Lancet 1994, 344, 101–106. [Google Scholar] [CrossRef]
- Horowitz, B.; Miskulin, D.; Zager, P. Epidemiology of Hypertension in CKD. Adv. Chronic Kidney Dis. 2015, 22, 88–95. [Google Scholar] [CrossRef]
- Tsai, W.C.; Wu, H.Y.; Peng, Y.S.; Yang, J.Y.; Chen, H.Y.; Chiu, Y.L.; Hsu, S.P.; Ko, M.J.; Pai, M.F.; Tu, Y.K.; et al. Association of Intensive Blood Pressure Control and Kidney Disease Progression in Nondiabetic Patients with Chronic Kidney Disease: A Systematic Review and Meta-analysis. JAMA Int. Med. 2017, 177, 792–799. [Google Scholar] [CrossRef]
- Ku, E.; Lee, B.J.; Wei, J.; Weir, M.R. Hypertension in CKD: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 74, 120–131. [Google Scholar] [CrossRef] [Green Version]
- U.S. Renal Data System. USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; USRDS: Bethesda, MD, USA, 2013.
- National Health Research Institutes. Annual Report on Kidney Disease in Taiwan; National Health Research Institutes: Zhunan, Taiwan, 2017.
- Bidani, A.K.; Griffin, K.A. Pathophysiology of hypertensive renal damage: Implications for therapy. Hypertension 2004, 44, 595–601. [Google Scholar] [CrossRef] [Green Version]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Howden, E.J.; Coombes, J.S.; Strand, H.; Douglas, B.; Campbell, K.L.; Isbel, N.M. Exercise Training in CKD: Efficacy, Adherence, and Safety. Am. J. Kidney Dis. 2015, 56, 583–591. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity and Adults-Recommended Levels of Physical Activity for Adults Aged 18–64 Years. Available online: https://www.who.int/dietphysicalactivity/factsheet_adults/en/ (accessed on 19 January 2020).
- National Kidney Foundation. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am. J. Kidney Dis. 2005, 45, S1–S154. [Google Scholar]
- Painter, P.; Roshanravan, B. The association of physical activity and physical function with clinical outcomes in adults with chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2013, 22, 615–623. [Google Scholar] [CrossRef]
- Hu, G.; Eriksson, J.; Barengo, N.C.; Lakka, T.A.; Valle, T.T.; Nissinen, A.; Jousilahti, P.; Tuomilehto, J. Occupational, commuting, and leisure-time physical activity in relation to total and cardiovascular mortality among Finnish subjects with type 2 diabetes. Circulation 2004, 110, 666–673. [Google Scholar] [CrossRef] [Green Version]
- Mayer-Davis, E.J.; D’Agostino, R., Jr.; Karter, A.J.; Haffner, S.M.; Rewers, M.J.; Saad, M.; Bergman, R.N. Intensity and amount of physical activity in relation to insulin sensitivity: The Insulin Resistance Atherosclerosis Study. JAMA 1998, 279, 669–674. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar]
- Levey, A.S.; Coresh, J.; Bolton, K.; Culleton, B.; Harvey, K.S.; Ikizler, T.A.; Johnson, C.A.; Kausz, A.; Kimmel, P.L.; Kusek, J.; et al. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Chen, L.I.; Guh, J.Y.; Wu, K.D.; Chen, Y.M.; Kuo, M.C.; Hwang, S.J.; Chen, T.H.; Chen, H.C. Modification of diet in renal disease (MDRD) study and CKD epidemiology collaboration (CKD-EPI) equations for Taiwanese adults. PLoS ONE 2014, 9, e99645. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Vupputuri, S.; Sandler, D.P. Lifestyle risk factors and chronic kidney disease. Ann. Epidemiol. 2003, 13, 712–720. [Google Scholar] [CrossRef]
- Bauman, A.; Bull, F.; Chey, T.; Craig, C.L.; Ainsworth, B.E.; Sallis, J.F.; Bowles, H.R.; Hagstromer, M.; Sjostrom, M.; Pratt, M. The International Prevalence Study on Physical Activity: Results from 20 countries. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 1–11. [Google Scholar] [CrossRef]
- Oyeyemi, A.L.; Oyeyemi, A.Y.; Adegoke, B.O.; Oyetoke, F.O.; Aliyu, H.N.; Aliyu, S.U.; Rufai, A.A. The Short International Physical Activity Questionnaire: Cross-cultural adaptation, validation and reliability of the Hausa language version in Nigeria. BMC Med. Res. Methodol. 2011, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Liou, Y.M.; Jwo, C.J.; Yao, K.G.; Chiang, L.C.; Huang, L.H. Selection of appropriate Chinese terms to represent intensity and types of physical activity terms for use in the Taiwan version of IPAQ. J. Nurs. Res. 2008, 16, 252–263. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Jette, M.; Sidney, K.; Blumchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- International Physical Activity Questionnaires (IPAQ). IPAQ Scoring Protocol. Available online: http://www.ipaq.ki.se (accessed on 12 January 2020).
- Bharakhada, N.; Yates, T.; Davies, M.J.; Wilmot, E.G.; Edwardson, C.; Henson, J.; Webb, D.; Khunti, K. Association of sitting time and physical activity with CKD: A cross-sectional study in family practices. Am. J. Kidney Dis. 2012, 60, 583–590. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Zelle, D.M.; Klaassen, G.; van Adrichem, E.; Bakker, S.J.; Corpeleijn, E.; Navis, G. Physical inactivity: A risk factor and target for intervention in renal care. Nat. Rev. Nephrol. 2017, 13, 152–168. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Cmaj 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Neufer, P.D.; Bamman, M.M.; Muoio, D.M.; Bouchard, C.; Cooper, D.M.; Goodpaster, B.H.; Booth, F.W.; Kohrt, W.M.; Gerszten, R.E.; Mattson, M.P.; et al. Understanding the Cellular and Molecular Mechanisms of Physical Activity-Induced Health Benefits. Cell Metab. 2015, 22, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Ruegsegger, G.N.; Booth, F.W. Health Benefits of Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Nunan, D.; Mahtani, K.R.; Roberts, N.; Heneghan, C. Physical activity for the prevention and treatment of major chronic disease: An overview of systematic reviews. Syst. Rev. 2013, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Chang, P.Y.; Chien, L.N.; Lin, Y.F.; Wu, M.S.; Chiu, W.T.; Chiou, H.Y. Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine 2016, 95, 1–7. [Google Scholar] [CrossRef]
- Sabolic, I.; Asif, A.R.; Budach, W.E.; Wanke, C.; Bahn, A.; Burckhardt, G. Gender differences in kidney function. Pflugers Archiv: Eur. J. Physiol. 2007, 455, 397–429. [Google Scholar] [CrossRef]
- Iseki, K. Gender differences in chronic kidney disease. Kidney Int. 2008, 74, 415–417. [Google Scholar] [CrossRef] [Green Version]
- Silbiger, S.R.; Neugarten, J. The impact of gender on the progression of chronic renal disease. Am. J. Kidney Dis. 1995, 25, 515–533. [Google Scholar] [CrossRef]
- Reckelhoff, J.F.; Samson, W.K. Sex and gender differences in cardiovascular, renal and metabolic diseases. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R1057–R1059. [Google Scholar] [CrossRef] [Green Version]
- Taylor, D. Physical activity is medicine for older adults. Postgrad. Med. J. 2014, 90, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Tak, E.; Kuiper, R.; Chorus, A.; Hopman-Rock, M. Prevention of onset and progression of basic ADL disability by physical activity in community dwelling older adults: A meta-analysis. Ageing Res. Rev. 2013, 12, 329–338. [Google Scholar] [CrossRef]
- Spittaels, H.; Van Cauwenberghe, E.; Verbestel, V.; De Meester, F.; van Dyck, D.; Verloigne, M.; Haerens, L.; Deforche, B.; Cardon, G.; De Bourdeaudhuij, I. Objectively measured sedentary time and physical activity time across the lifespan: A cross-sectional study in four age groups. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Najafi, I.; Attari, F.; Islami, F.; Shakeri, R.; Malekzadeh, F.; Salahi, R.; Gharavi, M.Y.; Hosseini, M.; Broumand, B.; Haghighi, A.N.; et al. Renal function and risk factors of moderate to severe chronic kidney disease in Golestan Province, northeast of Iran. PLoS ONE 2010, 5, e14216. [Google Scholar] [CrossRef] [Green Version]
- Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S. Uric acid and incident kidney disease in the community. J. Am. Soc. Nephrol. 2008, 19, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Fandler-Hofler, S.; Enzinger, C.; Kneihsl, M.; Pinter, D.; Eppinger, S.; Obermayer-Pietsch, B.; Goritschan, A.; Hafner-Giessauf, H.; Rosenkranz, A.R.; Fazekas, F.; et al. Early renal dysfunction and fibroblast growth factor-23 in patients with small vessel disease-related stroke. Sci. Rep. 2019, 9, 15410. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Available online: https://www.who.int/ncds/surveillance/steps/resources/GPAQ_Analysis_Guide.pdf (accessed on 19 February 2020).


{kind=link}
| Characteristic | Overall | Renal Non-Progression | Renal Progression | p-Value |
|---|---|---|---|---|
| (n = 3543) | (n = 2470) | (n = 1073) | ||
| Sex, % | 0.052 | |||
| Female | 1500 (42.34) | 1019 (41.26) | 481 (44.83) | |
| Male | 2043 (57.66) | 1451 (58.74) | 592 (55.17) | |
| Age (years), mean ± SD | 63.32 ± 12.29 | 63.02 ± 12.21 | 63.99 ± 12.45 | 0.031 |
| Comorbidities, % | ||||
| CKD | 2771 (78.21) | 1755 (71.05) | 1016 (94.69) | <0.001 |
| Diabetes mellitus | 1642 (46.34) | 1069 (43.28) | 573 (53.40) | <0.001 |
| Dyslipidemia | 1428 (40.30) | 992 (40.16) | 436 (40.63) | 0.821 |
| Stroke | 330 (9.31) | 206 (8.34) | 124 (11.56) | 0.003 |
| Gout | 1005 (28.37) | 596 (24.13) | 409 (38.12) | <0.001 |
| Physical examination, mean ± SD | ||||
| Serum creatinine (mg/dL) | 1.58 ± 1.22 | 1.29 ± 0.98 | 2.25 ± 1.44 | <0.001 |
| Baseline eGFR (mL/min per 1.73 m2) | 52.70 ± 24.66 | 59.27 ± 22.43 | 37.57 ± 22.86 | <0.001 |
| Height (cm) | 161.39 ± 8.28 | 161.71 ± 8.32 | 160.65 ± 8.12 | <0.001 |
| Weight (kg) | 67.58 ± 12.91 | 68.03 ± 13.03 | 66.55 ± 12.58 | 0.002 |
| BMI (kg/m2) | 25.87 ± 4.11 | 25.93 ± 4.10 | 25.73 ± 4.14 | 0.181 |
| Fasting glucose (mg/dL) | 115.63 ± 36.33 | 113.54 ± 33.92 | 120.32 ± 40.87 | <0.001 |
| SBP (mmHg) | 133.88 ± 16.70 | 133.07 ± 16.64 | 135.73 ± 16.70 | <0.001 |
| DBP (mmHg) | 77.33 ± 11.61 | 77.63 ± 11.35 | 76.62 ± 12.17 | 0.022 |
| Total cholesterol (mg/dL) | 181.91 ± 38.58 | 181.45 ± 37.02 | 182.96 ± 41.88 | 0.332 |
| Lifestyle, % | ||||
| Cigarette smoking | 919 (25.95) | 630 (25.51) | 289 (26.96) | 0.387 |
| Alcohol consumption | 423 (11.94) | 304 (12.31) | 119 (11.09) | 0.332 |
| Sitting Time (HR/per day), mean ± SD | 242.84 ± 136.91 | 241.90 ± 137.36 | 244.53 ± 136.20 | 0.717 |
| Levels of Physical Activity, % | <0.001 | |||
| Low | 2235 (63.08) | 1519 (61.50) | 716 (66.73) | |
| Moderate | 926 (26.14) | 653 (26.44) | 273 (25.44) | |
| High | 382 (10.78) | 298 (12.06) | 84 (7.83) | |
| Characteristic | Low | Moderate | High | p-Value |
|---|---|---|---|---|
| n = 2235 | n = 926 | n = 382 | ||
| Sex, % | <0.001 | |||
| Female | 1021 (45.68) | 380 (41.04) | 99 (25.92) | |
| Male | 1214 (54.32) | 546 (58.96) | 283 (74.08) | |
| Age (years), mean ± SD | 63.29 ± 12.70 | 64.19 ± 11.33 | 61.34 ± 11.86 | <0.001 |
| Comorbidities, % | ||||
| CKD | 1765 (78.97) | 725 (78.29) | 281 (73.56) | 0.061 |
| Diabetes mellitus | 1085 (48.55) | 404 (43.63) | 153 (40.05) | 0.001 |
| Dyslipidemia | 881 (39.42) | 375 (40.50) | 172 (45.03) | 0.118 |
| Stroke | 214 (9.57) | 83 (8.96) | 33 (8.64) | 0.771 |
| Gout | 619 (27.70) | 262 (28.29) | 124 (32.46) | 0.161 |
| Physical examination, mean ± SD | ||||
| Serum creatinine (mg/dL) | 1.63 ± 1.28 | 1.52 ± 1.16 | 1.46 ± 1.02 | 0.010 |
| Baseline eGFR (mL/min per 1.73 m2) | 51.89 ± 25.26 | 53.31 ± 23.77 | 55.90 ± 22.97 | 0.009 |
| Height (cm) | 161.14 ± 8.34 | 161.23 ± 8.17 | 163.16 ± 7.96 | <0.001 |
| Weight (kg) | 67.66 ± 13.31 | 66.64 ± 11.87 | 69.37 ± 12.84 | 0.002 |
| BMI (kg/m2) | 25.98 ± 4.26 | 25.58 ± 3.85 | 25.96 ± 3.80 | 0.044 |
| Fasting glucose (mg/dL) | 116.90 ± 38.76 | 114.31 ± 32.27 | 111.53 ± 30.44 | 0.016 |
| SBP (mmHg) | 133.94 ± 16.82 | 133.81 ± 16.63 | 133.67 ± 16.18 | 0.948 |
| DBP (mmHg) | 77.18 ± 11.35 | 77.61 ± 12.22 | 77.51 ± 11.58 | 0.609 |
| Total cholesterol (mg/dL) | 181.97 ± 39.65 | 182.32 ± 38.26 | 180.59 ± 32.74 | 0.777 |
| Lifestyle, % | ||||
| Cigarette smoking | 561 (25.10) | 237 (25.62) | 121 (31.68) | 0.025 |
| Alcohol consumption | 261 (11.68) | 102 (11.02) | 60 (15.71) | 0.048 |
| Sitting time, mean ± SD | 246.43 ± 139.73 | 240.75 ± 135.73 | 232.71 ± 127.43 | 0.396 |
| Variable | Crude Odds Ratio (95% CI) | Adjusted Odds Ratio (95% CI) |
|---|---|---|
| Levels of Physical Activity | ||
| High | Reference | Reference |
| Moderate | 1.48 (1.12–1.96) | 1.39 (1.01–1.90) |
| Low | 1.67 (1.29–2.16) | 1.39 (1.04–1.86) |
| Sex | ||
| Male | Reference | Reference |
| Female | 1.16 (1.00–1.33) | 1.16 (1.00–1.33) |
| Age (years) | 1.01 (1.00–1.01) | 1.00 (0.99–1.00) |
| Comorbidities, % | ||
| CKD | 7.26 (5.48–9.61) | 3.87 (2.86–5.24) |
| Diabetes mellitus | 1.50 (1.30–1.73) | 1.75 (1.48–2.08) |
| Dyslipidemia | 1.02 (0.88–1.18) | 1.01 (0.85–1.19) |
| Stroke | 1.44 (1.14–1.82) | 1.30 (1.00–1.70) |
| Gout | 1.94 (1.66–2.26) | 1.47 (1.23–1.77) |
| BMI (kg/m2) | 0.99 (0.97–1.01) | 0.99 (0.97–1.01) |
| Serum creatinine (mg/dL) | 2.05 (1.90–2.21) | 2.00 (1.83–2.18) |
| Cigarette smoking | 1.08 (0.92–1.27) | 1.09 (0.88–1.35) |
| Alcohol consumption | 0.87 (0.71–1.11) | 0.98 (0.76–1.28) |
| Subgroups | High | Moderate Odds Ratio (95% CI) | Low Odds Ratio (95% CI) | p for Trend |
|---|---|---|---|---|
| Male | Reference | 1.45 (0.99–2.12) | 1.56 (1.10–2.20) | <0.020 |
| Female | Reference | 1.20 (0.63–1.87) | 1.09 (0.67–2.12) | 0.866 |
| Age ≥ 60 | Reference | 1.50 (1.02–2.21) | 1.54 (1.08–2.22) | 0.052 |
| Age < 60 | Reference | 1.52 (0.87–2.64) | 1.51 (0.92–2.48) | 0.191 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, P.-Y.; Lyu, S.-Y.; Lin, Y.-F.; Huang, C.-C. High Level of Physical Activity Reduces the Risk of Renal Progression in Hypertensive Patients. Int. J. Environ. Res. Public Health 2020, 17, 1669. https://doi.org/10.3390/ijerph17051669
Chang P-Y, Lyu S-Y, Lin Y-F, Huang C-C. High Level of Physical Activity Reduces the Risk of Renal Progression in Hypertensive Patients. International Journal of Environmental Research and Public Health. 2020; 17(5):1669. https://doi.org/10.3390/ijerph17051669
Chicago/Turabian StyleChang, Po-Ya, Shu-Yu Lyu, Yuh-Feng Lin, and Chun-Ching Huang. 2020. "High Level of Physical Activity Reduces the Risk of Renal Progression in Hypertensive Patients" International Journal of Environmental Research and Public Health 17, no. 5: 1669. https://doi.org/10.3390/ijerph17051669