Leptospiral Culture without 5’-Fluorouracil Revealed Improved Leptospira Isolation from Febrile Patients in North-Eastern Malaysia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
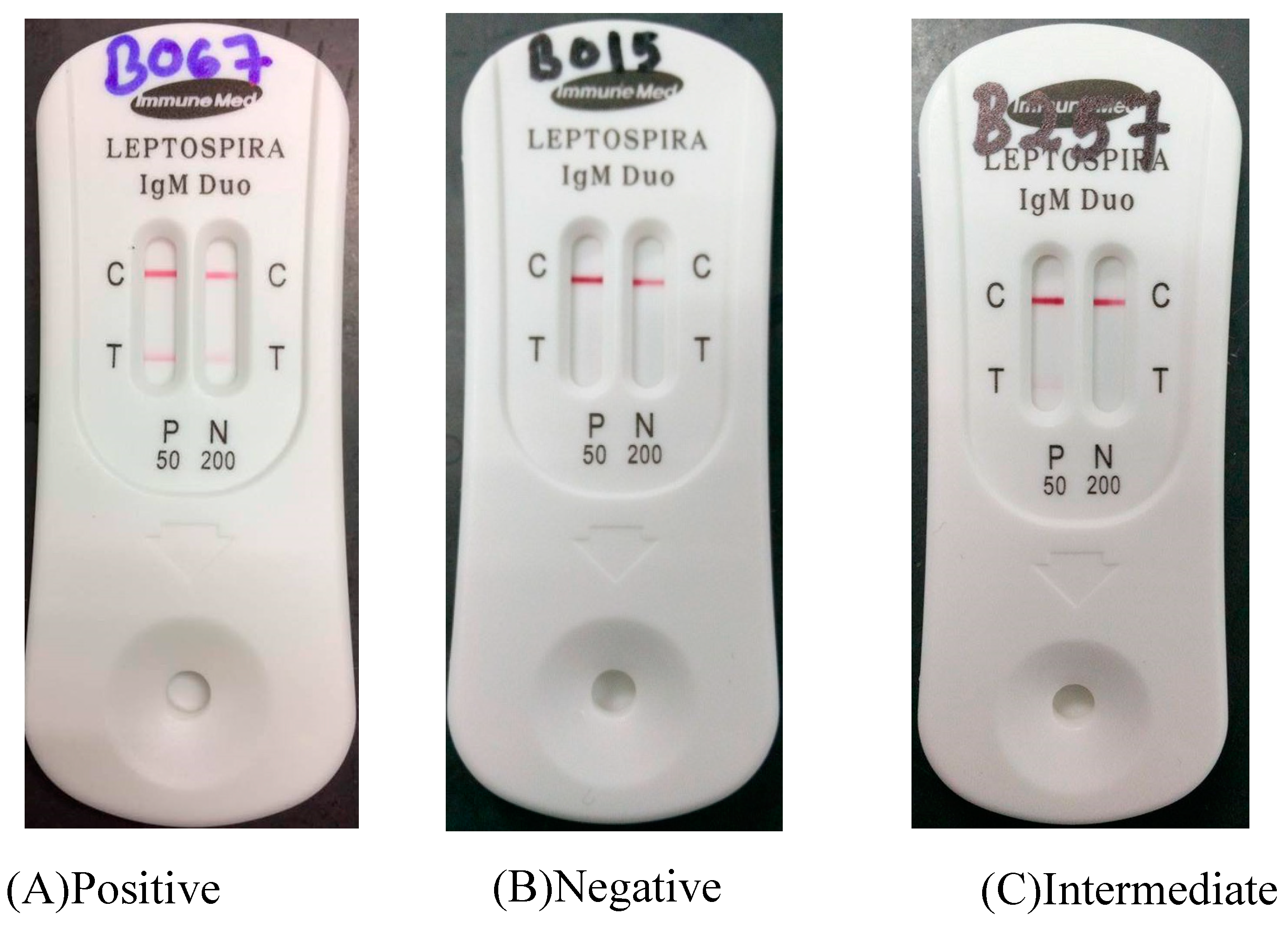
2.2. Rapid Leptospira Serology Test
2.3. Microscopic Agglutination Test
2.4. Direct Molecular Detection by Real-Time PCR
2.4.1. Extraction of Genomic DNA
2.4.2. Detection of Leptospira by Real-Time PCR
2.5. Isolation of Leptospira
2.6. Molecular Characterization of the Isolates
2.6.1. DNA Extraction
2.6.2. PCR and Visualization of Products
2.6.3. Sequencing and Sequence Analysis
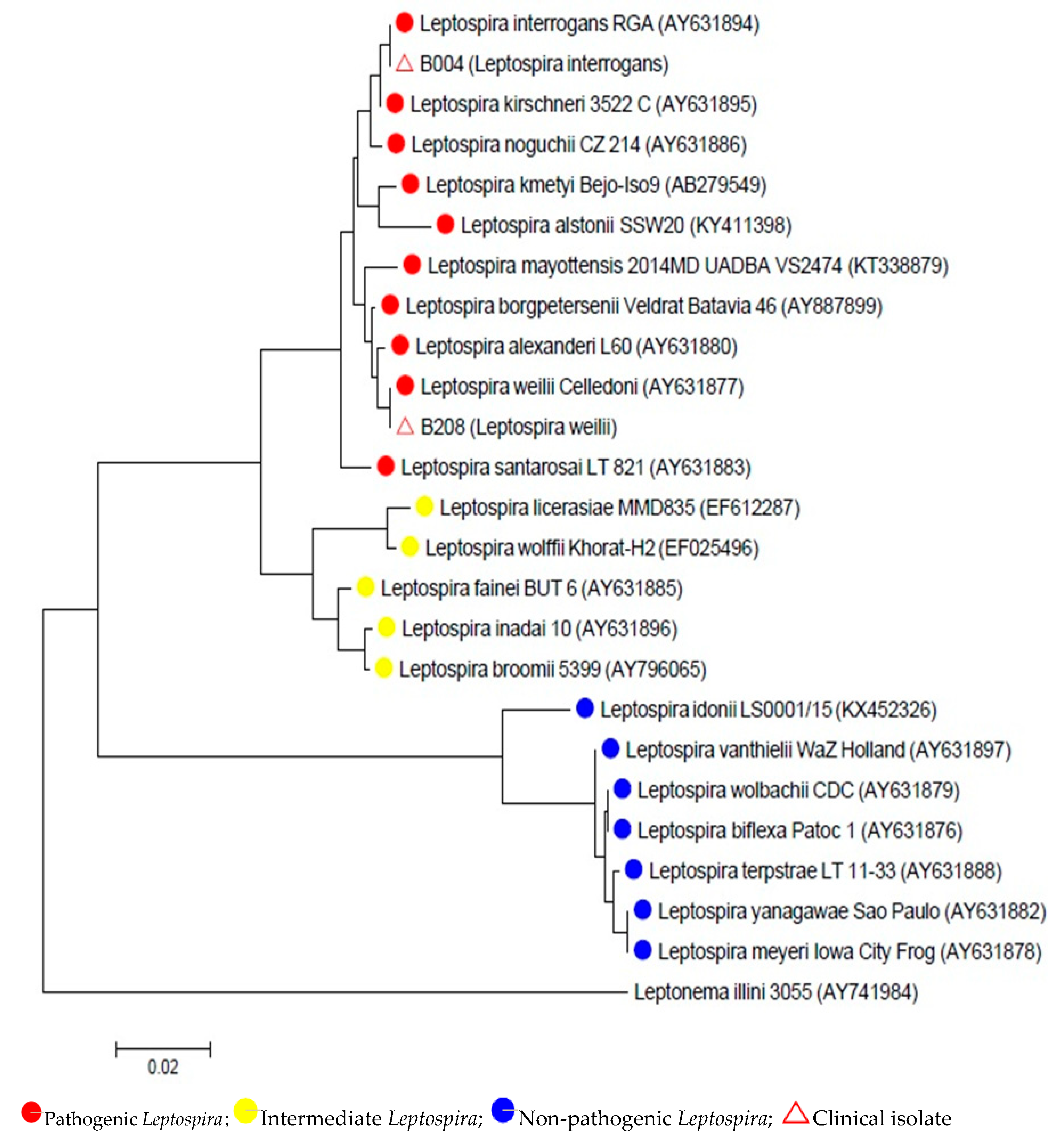
2.6.4. Phylogenetic Analysis of 16S rRNA Gene Sequences
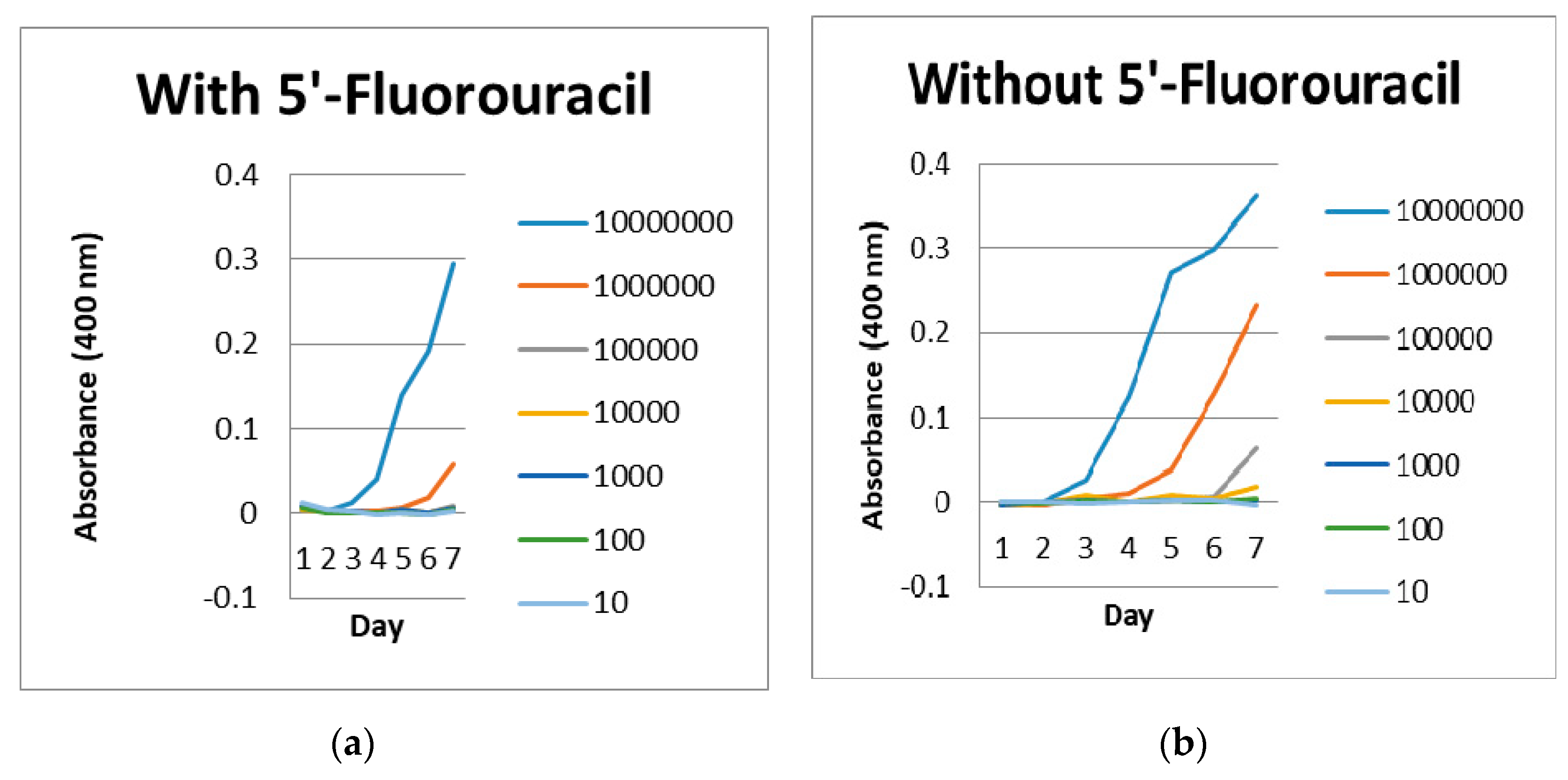
2.7. Inhibition of 5’-Fluorouracil Study
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- El, I.J.; Bahaman, A.R. A review of human leptospirosis in Malaysia. Trop. Biomed. 2004, 21, 113–119. [Google Scholar]
- Wuthiekanun, V.; Chierakul, W.; Limmathurotsakul, D.; Smythe, L.D.; Symonds, M.L.; Dohnt, M.F.; Slack, A.T.; Limpaiboon, R.; Suputtamongkol, Y.; White, N.J.; et al. Optimization of Culture of Leptospira from Humans with Leptospirosis. J. Clin. Microbiol. 2007, 45, 1363–1365. [Google Scholar] [CrossRef] [Green Version]
- Azali, M.A.; Yean Yean, C.; Harun, A.; Aminuddin Baki, N.N.; Ismail, N. Molecular Characterization of Leptospira spp. in environmental samples from north-eastern Malaysia revealed a pathogenic strain, Leptospira alstonii. J. Trop. Med. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, M.S.Z.S.; Massad, E. The impact of climate on Leptospirosis in Sao Paulo, Brazil. Int. J. Biometeorol. 2012, 56, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Adler, B.; de la Peña-Moctezuma, A. Leptospira and leptospirosis. Vet. Microbiol. 2010, 140, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Kashinkunti, M.D.; Gundikeri, S.K.; Dhananjaya, M. Acute undifferentiated febrile illness-clinical spectrum and outcome from a tertiary care teaching hospital of north Karnataka. Int. J. Biol. Med. Res. 2013, 3, 3399–3402. [Google Scholar]
- Tun, Z.M.; Moorthy, M.; Linster, M.; Su, Y.C.; Coker, R.J.; Ooi, E.E.; Low, J.G.; Smith, G.J.; Tam, C.C. Characteristics of acute febrile illness and determinants of illness recovery among adults presenting to Singapore primary care clinics. BMC Infect. Dis. 2016, 16, 612. [Google Scholar] [CrossRef] [Green Version]
- Rafizah, A.N.; Aziah, B.D.; Azwany, Y.N.; Imran, M.K.; Rusli, A.M.; Nazri, S.M.; Nabilah, I.; Asma, H.S.; Zahiruddin, W.M.; Zaliha, I. Leptospirosis in Northeastern Malaysia: Misdiagnosed or Coinfection? Int. J. Collab. Res. Intern. Med. Public Health 2012, 47, 1419–1427. [Google Scholar]
- Leelarasamee, A.; Chupaprawan, C.; Chenchittikul, M.; Udompanthurat, S. Etiologies of acute undifferentiated febrile illness in Thailand. J. Med. Assoc. Thail. 2004, 87, 464–472. [Google Scholar]
- Manocha, H.; Ghoshal, U.; Singh, S.K.; Kishore, J.; Ayyagari, A. Frequency of leptospirosis in patients of acute febrile illness in Uttar Pradesh. J. Assoc. Phys. India 2004, 52, 623–625. [Google Scholar]
- Suttinont, C.; Losuwanaluk, K.; Niwatayakul, K.; Hoontrakul, S.; Intaranongpai, W.; Silpasakorn, S.; Suwancharoen, D.; Panlar, P.; Saisongkorh, W.; Rolain, J.M.; et al. Causes of acute, undifferentiated, febrile illness in rural Thailand: Results of a prospective observational study. Ann. Trop. Med. Parasitol. 2006, 100, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Sarwankar, A.; Mulla, S. Isolation of Leptospira in suspected cases of leptospirosis: Is heparinized whole blood a better modality. Int. J. Adv. Sci. Eng. Technol. 2016, 4, 150–152. [Google Scholar]
- Boonsilp, S.; Thaipadungpanit, J.; Amornchai, P.; Wuthiekanun, V. Molecular detection and speciation of pathogenic Leptospira spp. in blood from patients with culture-negative leptospirosis. BMC Infect. Dis. 2011, 11, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Human leptospirosis: Guidance for diagnosis, surveillance and control. WHO Libr. 2003, 45, 1–109. [Google Scholar] [CrossRef]
- Ali, M.R.; Safee, A.W.; Ismail, N.H.; Sapian, R.A.; Hussin, H.M.; Ismail, N.; Yean, C.Y. Development and validation of pan-Leptospira Taqman qPCR for the detection of Leptospira spp. in clinical specimens. Mol. Cell. Probes 2018, 38, 1–6. [Google Scholar]
- Issazadeh, K.; Amirmozaffari, N.; Mehrabian, S.; Oryan, S. Assessment of Distribution Leptospira spp. in Surface Waters of Guilan Province. World J. Zool. 2009, 4, 79–84. [Google Scholar]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular Evolutionary Genetics Analysis Version 7.0 for Bigger Datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [Green Version]
- Moreno, L.Z.; Miraglia, F.; Lilenbaum, W.; Neto, J.S.; Freitas, J.C.; Morais, Z.M.; Hartskeerl, R.A.; Da Costa, B.L.; Vasconcellos, S.A.; Moreno, A.M. Profiling of Leptospira interrogans, L. santarosai, L. meyeri and L. borgpetersenii by SE-AFLP, PFGE and susceptibility testing- a continuous attempt at species and serovar differentiation. Emerg. Microbes Infect. 2016, 5, 1–7. [Google Scholar] [CrossRef]
- Chakraborty, A.; Miyahara, S.; Villanueva, S.Y.A.M.; Saito, M.; Gloriani, N.G.; Yoshida, S.-I. A novel combination of selective agents for isolation of Leptospira species. Microbiol. Immunol. 2011, 55, 494–501. [Google Scholar] [CrossRef]
- Saitou, N.; Nei, M. The neighbour-joining method: A new method for reconstructing phylogenetic trees. Mol. Biol. Evol. 1987, 4, 406–425. [Google Scholar]
- Tamura, K.; Nei, M.; Kumar, S. Prospects for inferring very large phylogenies by using the neighbor-joining method. Proc. Natl. Acad. Sci. USA 2004, 101, 11030–11035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chappel, R.J.; Goris, M.; Palmer, M.F.; Hartskeerl, R.A. Impact of proficiency testing on results of the microscopic agglutination test for diagnosis of leptospirosis. J. Clin. Microbiol. 2004, 42, 5484–5488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haake, D.A.; Levett, P.N. Leptospirosis in humans. Curr. Top. Microbiol. Immunol. 2015, 387, 65–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levett, P.N. Usefulness of serologic analysis as a predictor of the infecting serovar in patients with severe leptospirosis. Clin. Infect. Dis. 2003, 36, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Villumsen, S.; Pedersen, R.; Krogfelt, K.A.; Jensen, J.S. Expanding the Diagnostic Use of PCR in Leptospirosis: Improved Method for DNA Extraction from Blood Cultures. PLoS ONE 2010, 5, e12095. [Google Scholar] [CrossRef]
- Gonçalves, A.T.; Paiva, C.; Melo-Mota, F.; Vieira, M.L.; Carreira, T.; Nunes, M.S.; Mota-Vieira, L.; Ahmed, A.; Harstkeerl, R.A.; Hyde, K.; et al. First isolation of human Leptospira strains, Azores, Portugal. Int. J. Infect. Dis. 2010, 14. [Google Scholar] [CrossRef] [Green Version]
- Ellinghausen, H.C.; McCullough, W.G. Nutrition of Leptospira Pomona and growth of 13 other serotypes: A. Am. J. Vet. Res. 1965, 26, 39–44. [Google Scholar]
- Adler, B.; de la Peña Moctezuma, A. Leptospira and Leptospirosis, 2nd ed.; MedSci: Armadale, Australia, 1999; p. 293. [Google Scholar]
- Wuthiekanun, V.; Amornchai, P.; Paris, D.H.; Langla, S.; Thaipadunpanit, J.; Chierakul, W.; Smythe, L.D.; White, N.J.; Day, N.P.; Limmathurotsakul, D.; et al. Rapid isolation and susceptibility testing of Leptospira spp. using a new solid medium, LVW agar. Antimicrob. Agents Chemother. 2013, 57, 297–302. [Google Scholar] [CrossRef] [Green Version]
- Clarridge, J.E.; Alerts, C. Impact of 16S rRNA gene sequence analysis for identification of bacteria on clinical microbiology and infectious diseases. Clin. Microbiol. Rev. 2004, 17, 840–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, M.M.; Matsuo, M.G.; Bauab, A.R.; Vasconcelos, S.A.; Moraes, Z.M.; Baranton, G.; Saint Girons, I. A clonal subpopulation of Leptospira interrogans sensu stricto is the major cause of leptospirosis outbreaks in Brazil. J. Clin. Microbiol. 2000, 38, 450–452. [Google Scholar]
- Thaipadungpanit, J.; Wuthiekanun, V.; Chierakul, W.; Smythe, L.D.; Petkanchanapong, W.; Limpaiboon, R.; Apiwatanaporn, A.; Slack, A.T.; Suputtamongkol, Y.; White, N.J.; et al. A Dominant Clone of Leptospira interrogans Associated with an Outbreak of Human Leptospirosis in Thailand. PLoS Negl. Trop. Dis. 2007, 1, e56. [Google Scholar] [CrossRef]
- Cosate, M.R.; Sakamoto, T.; de Oliveira Mendes, T.A.; Moreira, É.C.; da Silva, C.G.; Brasil, B.S.; Oliveira, C.S.; de Azevedo, V.A.; Ortega, J.M.; Leite, R.C.; et al. Molecular typing of Leptospira interrogans serovar Hardjo isolates from leptospirosis outbreaks in Brazilian livestock. BMC Vet. Res. 2017, 13, 177. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Kaufmann, A.F.; Sulzer, K.R.; Steigerwalt, A.G.; Rogers, F.C.; Weyant, R.S. Further determination of DNA relatedness between serogroups and serovars in the family Leptospiraceae with a proposal for Leptospira alexanderi sp. nov. and four new Leptospira genomospecies. Int. J. Syst. Bacteriol. 1999, 49, 839–858. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.J.; Brown, H.E.; Tonge, J.I.; Sinnamon, C.N.; MacDonald, V.M.; Ross, C.J.; Doherty, R.L. The serological classification of 89 strains of leptospirae from North Queensland. Aust. Ann. Med. 1954, 3, 98–105. [Google Scholar] [PubMed]
- Slack, A.T.; Symonds, M.L.; Dohnt, M.F.; Corney, B.G.; Smythe, L.D. Epidemiology of Leptospira weilii serovar Topaz infections in Australia. Commun. Dis. Intell. 2007, 31, 216–222. [Google Scholar]
- Johnson, R.C.; Rogers, P. 5′-fluorouracil as a selective agent for growth of leptospirae. J. Bacteriol. 1964, 87, 422–426. [Google Scholar] [CrossRef] [Green Version]
- Turner, L.H. Leptospirosis III. Maintenance, isolation and demonstration of leptospires. Trans. R. Soc. Trop. Med. Hyg. 1970, 64, 623–646. [Google Scholar] [CrossRef]
- WHO Expert Group on Leptospirosis. Current problems in leptospirosis research. WHO Tech. Rep. Ser. 1967, 380, 1–32. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Reference Strain | Accession Number |
|---|---|
| Leptospira weilii Celledoni | AY631877 |
| Leptospira borgpeterseni Veldrat Batavia 46 | AY887899 |
| Leptospira alexanderi L60 | AY631880 |
| Leptospira santarosai LT 821 | AY631883 |
| Leptospira noguchii CZ 214 | AY631886 |
| Leptospira kirschneri 3522 C | AY631895 |
| Leptospira interrogans RGA | AY631894 |
| Leptospira vanthielii Waz Holland | AY631897 |
| Leptospira biflexa Patoc 1 | AY631876 |
| Leptospira wolbachii CDC | AY631879 |
| Leptospira terpstrae LT 11-33 | AY631888 |
| Leptospira meyeri Iowa City Frog | AY631878 |
| Leptospira yanagawae Sao Paulo | AY631882 |
| Leptonema illini 3055 | AY714984 |
| Leptospira fainei BUT 6 | AY631885 |
| Leptospira broomii 5399 | AY796065 |
| Leptospira inadai 10 | AY631896 |
| Leptospira alstonii SSW20 Leptospira idonii LS 0001/15 | KY411398 KX452326 |
| Leptospira kmetyi Bejo-Iso9 | AB279549 |
| Leptospira moyottensis 2014MD UADBA VS2474 | KT338879 |
| Leptospira licerasiae MMD835 | EF612287 |
| Leptospira wolffii Khorat-H2 | EF025496 |
| Leptospira IgM Duo Rapid (n = 109) | Microscopic Agglutination Test, Titer (n = 31) | Real-Time PCR (n = 109) |
|---|---|---|
| Intermediate (28) Positive (3) Negative (78) | 1:100 (3) 1:50 (6) Negative (22) | Positive (16) Negative (93) |
| Leptospira Concentration (cells/mL) | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5-FU | No 5-FU | 5-FU | No 5-FU | 5-FU | No 5-FU | 5-FU | No 5-FU | 5-FU | No 5-FU | 5-FU | No 5-FU | 5-FU | No 5-FU | ||
| 108 | I | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| II | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| 107 | I | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| II | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| 106 | I | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| II | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |
| 105 | I | - | - | - | - | - | - | + | + | + | + | + | + | + | + |
| II | - | - | - | - | - | - | + | + | + | + | + | + | + | + | |
| 104 | I | - | - | - | - | - | - | - | + | - | + | - | + | + | + |
| II | - | - | - | - | - | - | - | + | - | + | - | + | + | + | |
| 103 | I | - | - | - | - | - | - | - | - | - | - | - | + | + | + |
| II | - | - | - | - | - | - | - | - | - | - | - | + | + | + | |
| 102 | I | - | - | - | - | - | - | - | - | - | - | - | + | - | + |
| II | - | - | - | - | - | - | - | - | - | - | - | + | - | + | |
| 101 | I | - | - | - | - | - | - | - | - | - | - | - | + | - | + |
| II | - | - | - | - | - | - | - | - | - | - | - | + | - | + | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamad Safiee, A.W.; Mohd Ali, M.R.; Fauzi, M.H.; Muhd Besari, A.; Yean Yean, C.; Neela, V.K.; Ismail, N. Leptospiral Culture without 5’-Fluorouracil Revealed Improved Leptospira Isolation from Febrile Patients in North-Eastern Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 1307. https://doi.org/10.3390/ijerph17041307
Mohamad Safiee AW, Mohd Ali MR, Fauzi MH, Muhd Besari A, Yean Yean C, Neela VK, Ismail N. Leptospiral Culture without 5’-Fluorouracil Revealed Improved Leptospira Isolation from Febrile Patients in North-Eastern Malaysia. International Journal of Environmental Research and Public Health. 2020; 17(4):1307. https://doi.org/10.3390/ijerph17041307
Chicago/Turabian StyleMohamad Safiee, Amira Wahida, Mohammad Ridhuan Mohd Ali, Mohd Hashairi Fauzi, Alwi Muhd Besari, Chan Yean Yean, Vasantha Kumari Neela, and Nabilah Ismail. 2020. "Leptospiral Culture without 5’-Fluorouracil Revealed Improved Leptospira Isolation from Febrile Patients in North-Eastern Malaysia" International Journal of Environmental Research and Public Health 17, no. 4: 1307. https://doi.org/10.3390/ijerph17041307