Comparing Logistic Regression Models with Alternative Machine Learning Methods to Predict the Risk of Drug Intoxication Mortality


Abstract
:1. Introduction
2. Materials and Methods
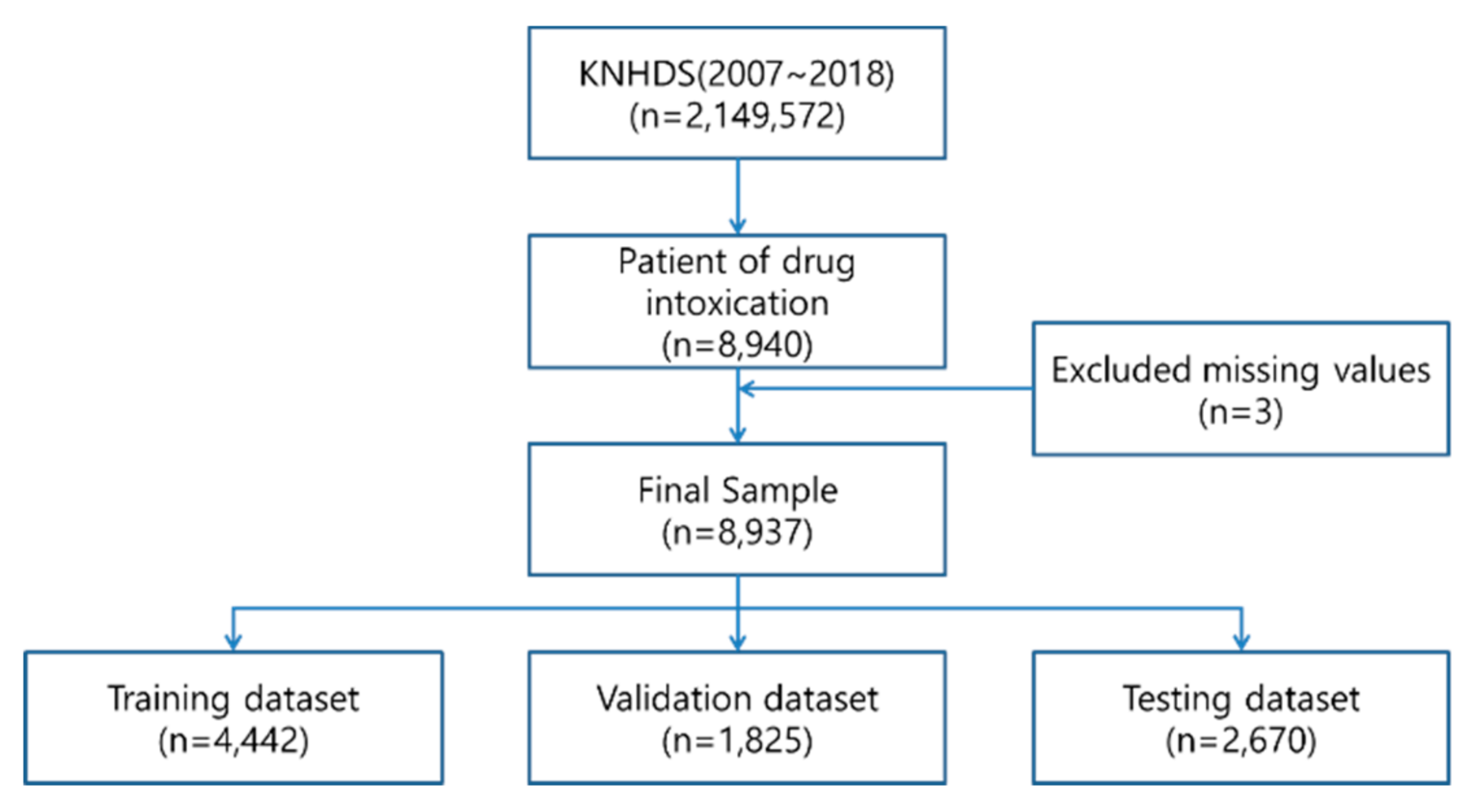
2.1. Data Set
2.2. Methods
3. Results
3.1. Statistical Analysis
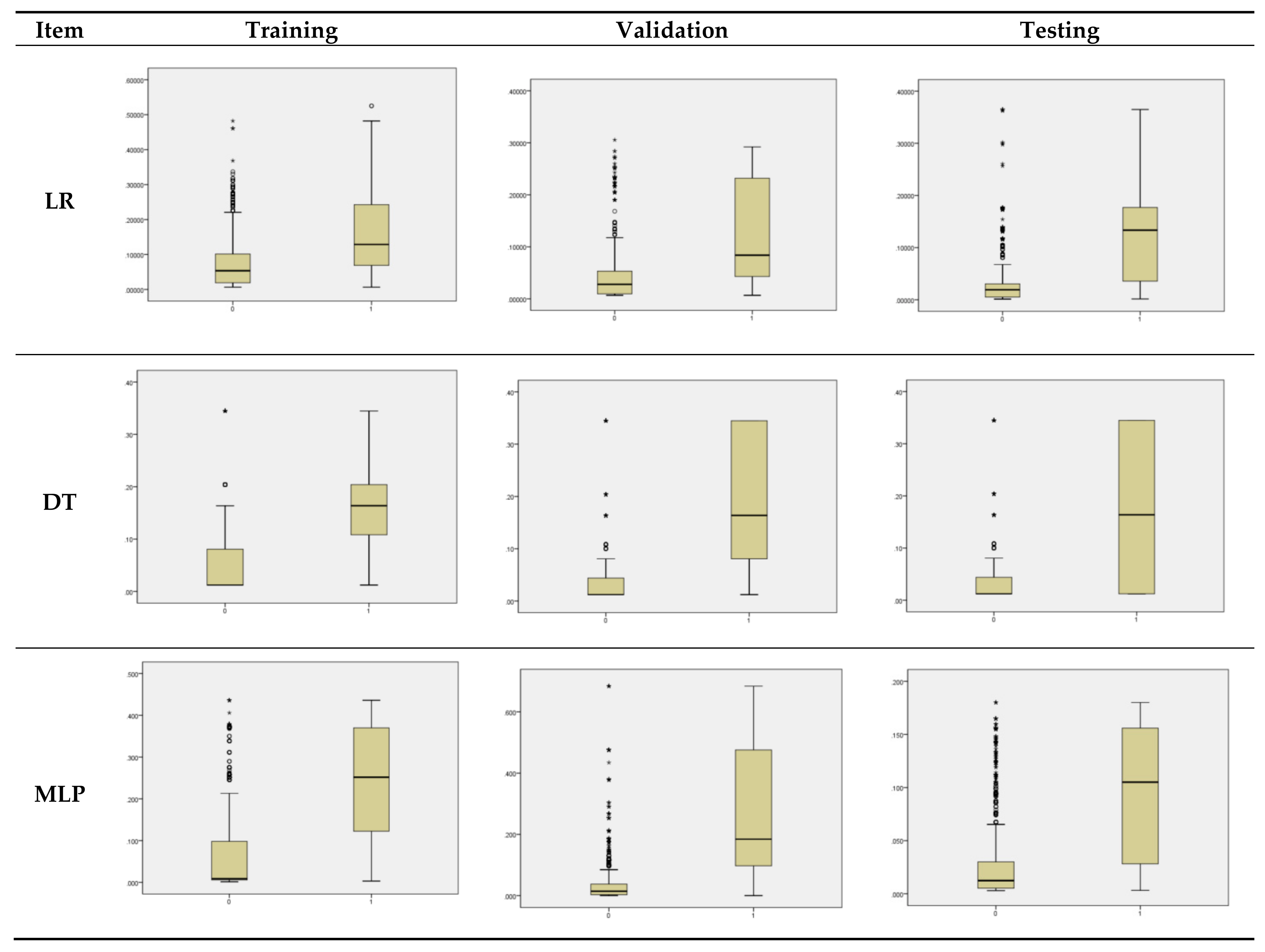
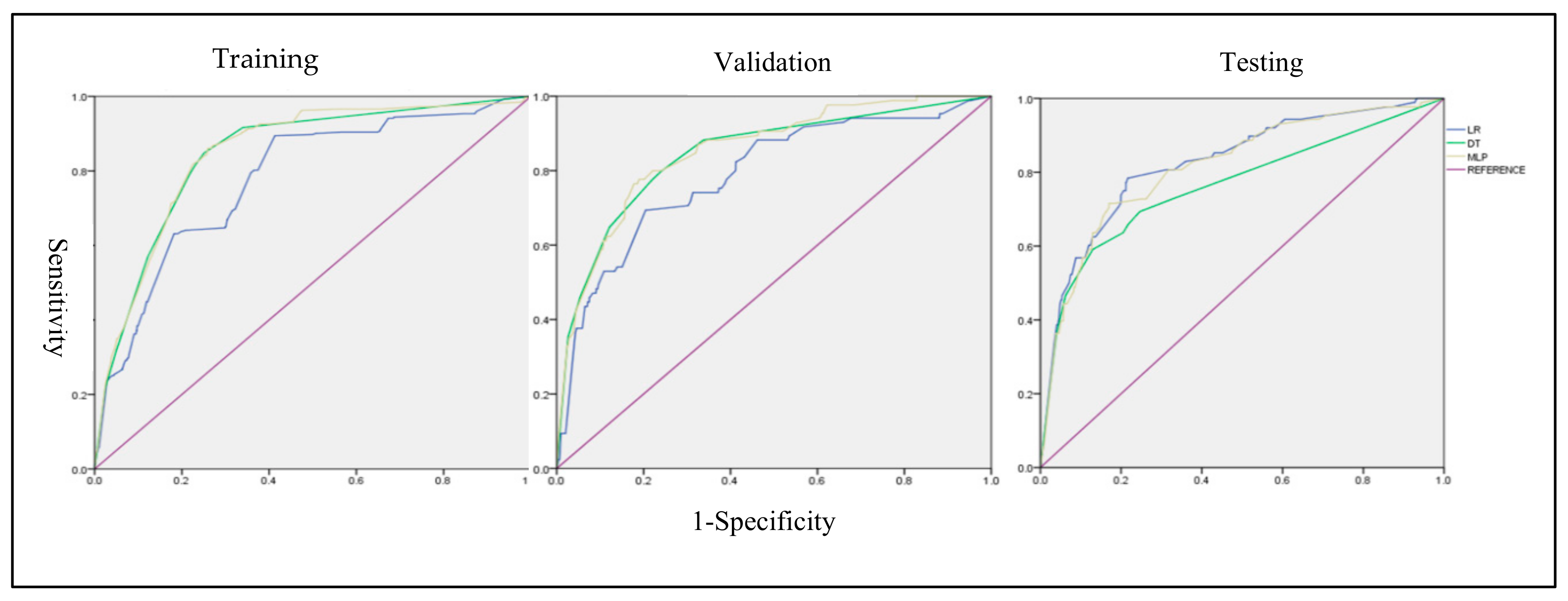
3.2. Modeling Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Han, S.T.; Lee, J.H. Comparative analysis of acute drug intoxication between 1980s and 1990s. J. Korean Soc. Emerg. Med. 1999, 10, 441–446. [Google Scholar]
- Moon, J.M.; Chun, B.J.; Cho, Y.S. The characteristics of emergency department presentations related to acute herbicide or insecticide poisoning in South Korea between 2011 and 2014. J. Toxicol. Environ. Health 2016, 79, 466–476. [Google Scholar] [CrossRef]
- Rockett, I.R.; Smith, G.S.; Caine, E.D.; Kapusta, N.D.; Hanzlick, R.L.; Larkin, G.L.; Naylor, C.P.; Nolte, K.B.; Miller, T.R.; Putnam, S.L.; et al. Confronting death from drug self-intoxication (DDSI): Prevention through a better definition. Am. J. Public Health 2014, 104, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Descamps, A.K.; Vandijck, D.M.; Buylaert, W.A.; Mostin, M.A.; Paepe, P. Characteristics and costs in adults with acute poisoning admitted to the emergency department of a university hospital in Belgium. PLoS ONE 2019, 14, e0223479. [Google Scholar] [CrossRef]
- Vermes, A.; Roelofsen, E.E.; Sabadi, G.; van den Berg, B.; de Quelerij, M.; Vulto, A.G. Intoxication with therapeutic and illicit drug substances and hospital admission to a Dutch university hospital. Neth. J. Med. 2003, 61, 168–172. [Google Scholar] [PubMed]
- Haoka, T.; Sakata, N.; Okamoto, H.; Oshiro, A.; Shimizu, T.; Naito, Y.; Onishi, S.; Morishita, Y.; Nara, S. Intentional or unintentional drug poisoning in elderly people: Retrospective observational study in a tertiary care hospital in Japan. Acute Med. Surgery 2019, 6, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Conner, K.R.; Wiegand, T.J.; Gorodetsky, R.; Schult, R.; Pizzarello, E.; Kaukeinen, K. Validation of the Poisoning Severity Score (PSS) in suicidal behavior by self-poisonin. Behav. Sci. Law 2019, 37, 240–246. [Google Scholar] [CrossRef]
- Persson, H.E.; Sjöberg, G.K.; Haines, J.A.; de Garbino, J.P. Poisoning severity score. Grading of acute poisoning. J. Toxicol. C. Toxicol. 1998, 36, 205–213. [Google Scholar] [CrossRef]
- Vasilevskis, E.E.; Kuzniewicz, M.W.; Cason, B.A.; Lane, R.K.; Dean, M.L.; Clay, T.; Rennie, D.J.; Vittinghoff, E.; Dudley, R.A. Mortality probability model III and simplified acute physiology score II: Assessing their value in predicting length of stay and comparison to APACHE IV. Chest 2009, 136, 89–101. [Google Scholar] [CrossRef] [Green Version]
- Engerstrom, L.; Nolin, T.; Mardh, C.; Sjoberg, F.; Karlstrom, G.; Fredrikson, M.; Walther, S.M. Impact of Missing Physiologic Data on Performance of the Simplified Acute Physiology Score 3 Risk-Prediction Model. Crit. Care Med. 2017, 45, 2006–2013. [Google Scholar] [CrossRef]
- Rosenthal, J.; Jacolbia, R.; Rajkomar, A.; Lee, H.; Auerbach, A. Using Tablet Computers to Increase Patient Engagement With Electronic Personal Health Records: Protocol For a Prospective, Randomized Interventional Study. J. Med. Internet Res. 2019, 18, 25. [Google Scholar]
- Rajkomar, A.; Oren, E.; Chen, K.M.; Dai, A.M.; Hajaj, N.; Liu, J.P.; Liu, X.; Sun, M.; Sundberg, P.; Yee, H.; et al. Scalable and accurate deep learning for electronic health records. Dig. Med. 2018, 1, 18. [Google Scholar] [CrossRef] [PubMed]
- Kang, I.H.; Lee, K.H.; Youk, H.; Lee, J.I.; Lee, H.Y.; Bae, K.S. Trauma and Injury Severity Score modification for predicting survival of trauma in one regional emergency medical center in Korea: Construction of Trauma and Injury Severity Score coefficient model, Hong Kong. J. Emerg. Med. 2019, 26, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Debray, T.P.; Vergouwe, Y.; Koffijberg, H.; Nieboer, D.; Steyerberg, E.W.; Moons, K.G. A new framework to enhance the interpretation of external validation studies of clinical prediction models. J. Clin. Epidemiol. 2015, 68, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Harrell, F.E. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Helmreich, J.E. Regression Modeling Strategies with Applications to Linear Models, Logistic and Ordinal Regression and Survival Analysis (2nd Edition). J. Stat. Soft. 2016, 70. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Hippisley-Cox, J.; Coupland, C. Predicting risk of emergency admission to hospital using primary care data: Derivation and validation of QAdmissions score. BMJ Open 2013, 3, e003482. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, W.; Park, R.W. A comparison of intensive care unit mortality prediction models through the use of data mining techniques. Healthc Inform. Res. 2011, 17, 232–243. [Google Scholar] [CrossRef]
- Scott, H.F.; Colborn, K. Machine learning for predicting sepsis in-hospital mortality: An important start. Acad Emerg. Med. 2016, 23, 1307. [Google Scholar] [CrossRef]
- Churpek, M.M.; Yuen, T.C.; Winslow, C.; Meltzer, D.O.; Kattan, M.W.; Edelson, D.P. Multicenter comparison of machine learning methods and conventional regression for predicting clinical deterioration on the wards. Crit. Care Med. 2016, 44, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Badriyah, T.; Briggs, J.S.; Prytherch, D.R. Decision trees for predicting risk of mortality using routinely collected data. Int. J. Soc. Hum. Sci. 2012, 6, 660–663. [Google Scholar]
- Wang, G.; Lam, K.M.; Deng, Z.; Choi, K.S. Prediction of mortality after radical cystectomy for bladder cancer by machine learning techniques. Comput. Biol. Med. 2015, 63, 124–132. [Google Scholar] [CrossRef]
- Motwani, M.; Dey, D.; Berman, D.S.; Germano, G.; Achenbach, S.; Al-Mallah H., M.; Andreini, D.; Budoff, J.M.; Cademartiri, F.; Callister, Q.T.; et al. Machine learning for prediction of all-cause mortality in patients with suspected coronary artery disease: A 5-year multicentre prospective registry analysis. Eur. Heart. J. 2016, 52, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, N.; Akbarov, A.; Kontopantelis, E.; Buchan, I.; Dunn, K.W. Mortality risk prediction in burn injury: Comparison of logistic regression with machine learning approaches. Burns 2015, 41, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Colombet, I.; Ruelland, A.; Chatellier, G.; Gueyffier, F.; Degoulet, P.; Jaulent, M.C. Models to predict cardiovascular risk: Comparison of CART, multilayer perceptron and logistic regression. Proc. AMIA Symp. 2000, 156–160, PMC2244093. [Google Scholar]
- Ross, E.G.; Shah, N.H.; Dalman, R.L.; Nead, K.T.; Cooke, J.P.; Leeper, N.J. The use of machine learning for the identification of peripheral artery disease and future mortality risk. J. Vasc. Surg. 2016, 64, 1515–1522. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Maslove, D.M.; Dubin, J.A. Personalized Mortality Prediction Driven by Electronic Medical Data and a Patient Similarity Metric. PLoS ONE 2015, 10, e0127428. [Google Scholar] [CrossRef]
- Ho, L.V.; Ledbetter, D.; Aczon, M.; Wetzel, R. The Dependence of Machine Learning on Electronic Medical Record Quality. In Proceedings of the AMIA Annual Symposium, Washinton, DC, USA, 6–8 November 2017; American Medical Informatics Association: Washinton, DC, USA, 2017; Volume 2017, p. 883. [Google Scholar]
- Tsao, H.Y.; Chan, P.Y.; Su, E.C.Y. Predicting diabetic retinopathy and identifying interpretable biomedical features using machine learning algorithms. BMC Bioinforma. 2018, 19, 195. [Google Scholar] [CrossRef] [Green Version]
- Karlık, B.; Olgaç, A.V. Performance analysis of various activation functions in generalized MLP architectures of neural networks. Inter. J. Art. Int. Exp. Sys. 2011, 1, 111–122. [Google Scholar]
- Isa, I.; Saad, Z.; Omar, S.; Osman, M.; Ahmad, K.; Sakim, H.M. Suitable MLP network activation functions for breast cancer and thyroid disease detection. In Proceedings of the IEEE, Tuban, Indonesia, 28–30 September 2010; 2010; pp. 39–44. [Google Scholar] [CrossRef]
- Moller, A. Scaled Conjugate Gradient Algorithm for Fast Supervised Learning. Neural Netw. 1993, 6, 525–533. [Google Scholar] [CrossRef]
- Khemphila, A.; Boonjing, V. Comparing performances of logistic regression, decision trees, and neural networks for classifying heart disease patients. In Proceedings of the International conference on Computer Information Systems and Industrial Management Applications (CISIM), Krakow, Poland, 8–10 October 2010; pp. 193–198. [Google Scholar] [CrossRef]
- Greene, S.L.; Dargan, P.I.; Jones, A.L. Acute poisoning: Understanding 90% of cases in a nutshell. Postgrad. Med. J. 2005, 81, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Brust, J.C. Neurologic complications of substance abuse. CONTINUUM 2014, 20, 642–656. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, Y.; Ko, Y.; Cha, E.S.; Kim, J.; Lee, W.J. Economic burden of acute pesticide poisoning in South Korea. Trop. Med. Int. Health 2012, 17, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.C.; Seo, J.Y.; Chung, J.B.; Choi, Y.M.; Choi, J.T.; You, K.C.; Ahn, M.E.; Choi, M.C.; Kim, H.K.; Kim, S.W.; et al. Clinical Review In Geriatric Trauma Patients. J. Korean Soc. Emerg. Med. 2002, 13, 1. [Google Scholar]
- Jang, S.N.; Kim, D.H. Trends in the health status of older Koreans. J. American Ger. Soc. 2010, 58, 592–598. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.M.; Kim, H.J.; Cho, Y.S.; Lee, M.G.; Jun, D.H.; Go, C.Y. Association of prescribed drug intoxication and neuropsychiatric history. J. Korean. Soc. Clin. Toxicol. 2011, 9, 77–80. [Google Scholar]
- Min, H.G.; Choi, H.S.; Kwon, O.Y.; Lee, J.S.; Hong, H.P.; Ko, Y.G. Is a psychiatric consultation necessary for the non-suicidal intentional drug ingestion patient in an emergency department. J. Korean Soc. Emerg. Med. 2010, 21, 878–886. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Items | Training | Validation | Testing | ||||
|---|---|---|---|---|---|---|---|
| Age | Under 65 | 3.333(75.0) | 62.1 *** | 1.360(74.5) | 68.5 *** | 1.878(70.3) | 67.1 *** |
| Over 65 | 1.109(25.0) | 465(25.5) | 792(29.7) | ||||
| Toxic Substance | Toxic Drug | 1.768(39.8) | 440.1 *** | 739(40.5) | 104.2 *** | 1.176(44.0) | 64.4 *** |
| Alcohol | 28(0.6) | 17(0.9) | 34(1.3) | ||||
| Hazardous Substance | 1.590(35.8) | 614(33.6) | 809(30.3) | ||||
| Other | 1.056(23.8) | 455(24.9) | 651(24.4) | ||||
| Severity (CCI) | 0 | 3.844(86.5) | 17.5 *** | 1.577(86.4) | 14.5 *** | 2.295(86.0) | 17.9 *** |
| 1 | 403(9.1) | 181(9.9) | 249(9.3) | ||||
| 2 | 114(2.6) | 44(2.4) | 73(2.7) | ||||
| 3 | 81(1.8) | 23(1.3) | 53(2.0) | ||||
| Cause of Risk | Conflict with Relatives | 666(15.0) | 11.3 ** | 192(10.5) | 13.3 ** | 317(11.9) | 13.3 ** |
| Physical Illness | 116(2.6) | 69(3.8) | 94(3.5) | ||||
| Mental Problem | 678(15.3) | 285(15.6) | 327(12.2) | ||||
| Financial Problem | 106(2.4) | 67(3.7) | 114(4.3) | ||||
| Other | 2.876(64.7) | 1.212(66.4) | 1.818(68.1) | ||||
| Intent | Unintentional | 1.657(37.3) | 123.8 *** | 699(38.3) | 25.6 *** | 1.021(38.2) | 37.3 *** |
| Intentional | 2.562(57.7) | 1.033(56.6) | 1.500(56.2) | ||||
| Missing | 223(5.) | 93(5.1) | 149(5.6) | ||||
| Total | 4.442 | 1.825 | 2.670 | ||||
| Items | Brier Score | AUC | Calibration | |
|---|---|---|---|---|
| Logistic Regression | Training | 0.06032 | 0.779 | −0.00342 |
| Validation | 0.04266 | 0.788 | 0.207416 | |
| Testing | 0.030796 | 0.827 | 0.149374 | |
| Decision Tree | Training | 0.060441 | 0.845 | 0.244034 |
| Validation | 0.042295 | 0.845 | −0.11715 | |
| Testing | 0.033615 | 0.764 | −0.49888 | |
| Multilayer Perceptron | Training | 0.059971 | 0.848 | −0.31857 |
| Validation | 0.043033 | 0.853 | −0.3938 | |
| Testing | 0.032589 | 0.816 | −0.50177 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Boo, Y. Comparing Logistic Regression Models with Alternative Machine Learning Methods to Predict the Risk of Drug Intoxication Mortality. Int. J. Environ. Res. Public Health 2020, 17, 897. https://doi.org/10.3390/ijerph17030897
Choi Y, Boo Y. Comparing Logistic Regression Models with Alternative Machine Learning Methods to Predict the Risk of Drug Intoxication Mortality. International Journal of Environmental Research and Public Health. 2020; 17(3):897. https://doi.org/10.3390/ijerph17030897
Chicago/Turabian StyleChoi, YoungJin, and YooKyung Boo. 2020. "Comparing Logistic Regression Models with Alternative Machine Learning Methods to Predict the Risk of Drug Intoxication Mortality" International Journal of Environmental Research and Public Health 17, no. 3: 897. https://doi.org/10.3390/ijerph17030897