Preventability of Colorectal Cancer in Saudi Arabia: Fraction of Cases Attributable to Modifiable Risk Factors in 2015–2040


Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Modifiable Risk Factors
2.2. CRC Incidence
2.3. Prevalence of Modifiable Risk Factors
2.4. Relative Risk
2.5. Calculation of PAF
2.6. Projections of Attributable CRC Cases in Saudi Arabia
3. Results
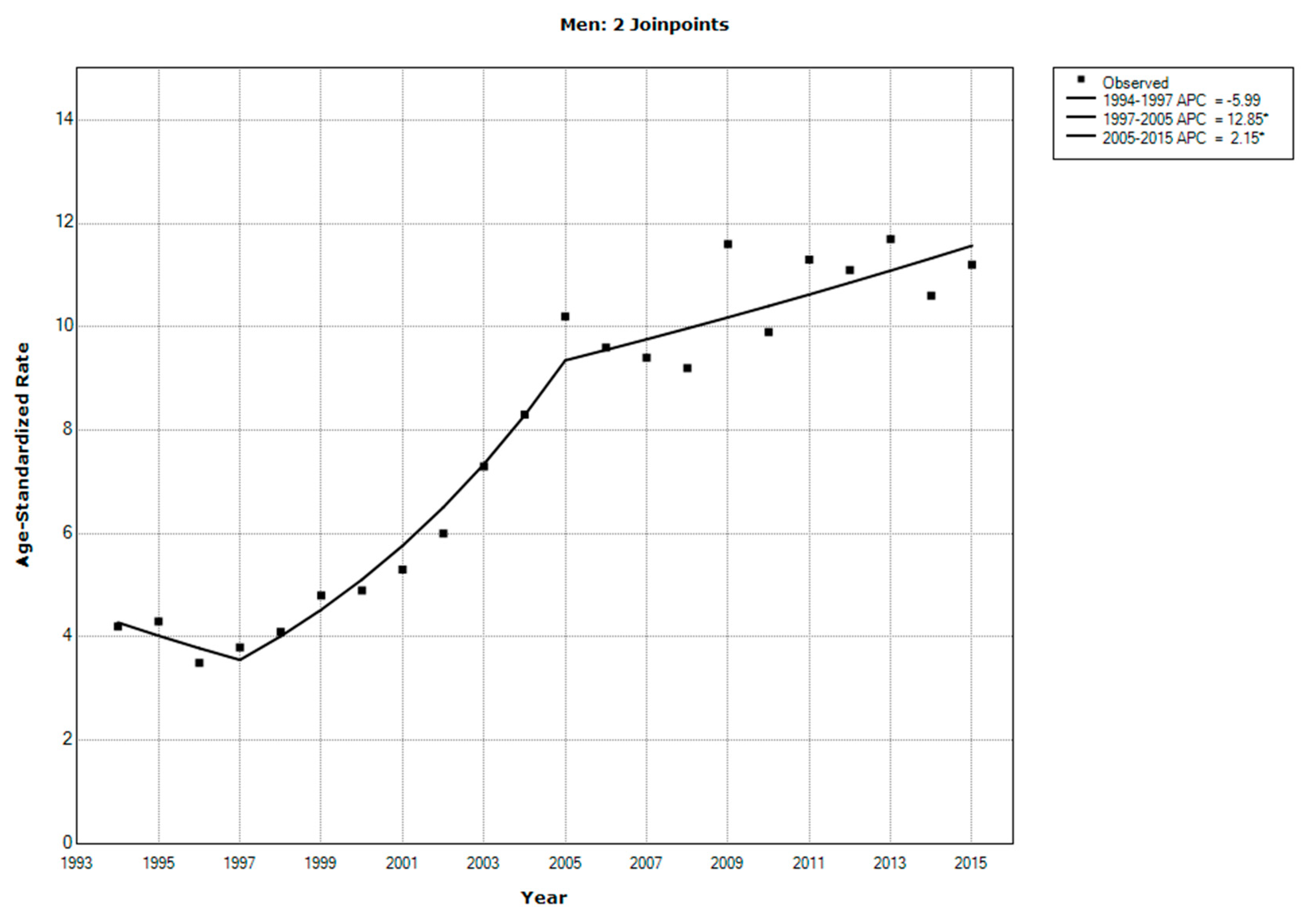
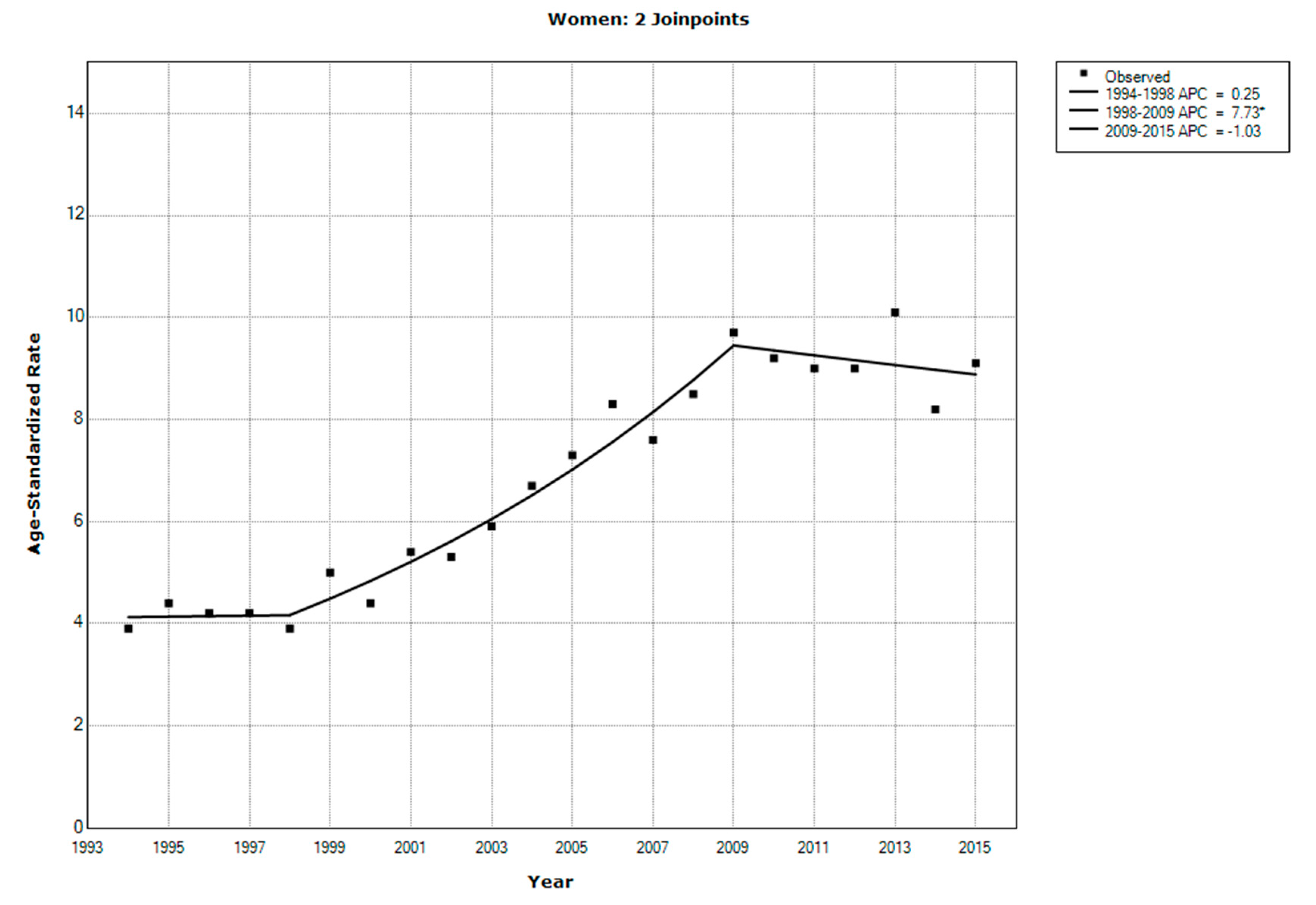
3.1. CRC Incidence
3.2. Prevalence of Risk Factors
3.3. Relative Risk Data
3.4. PAF
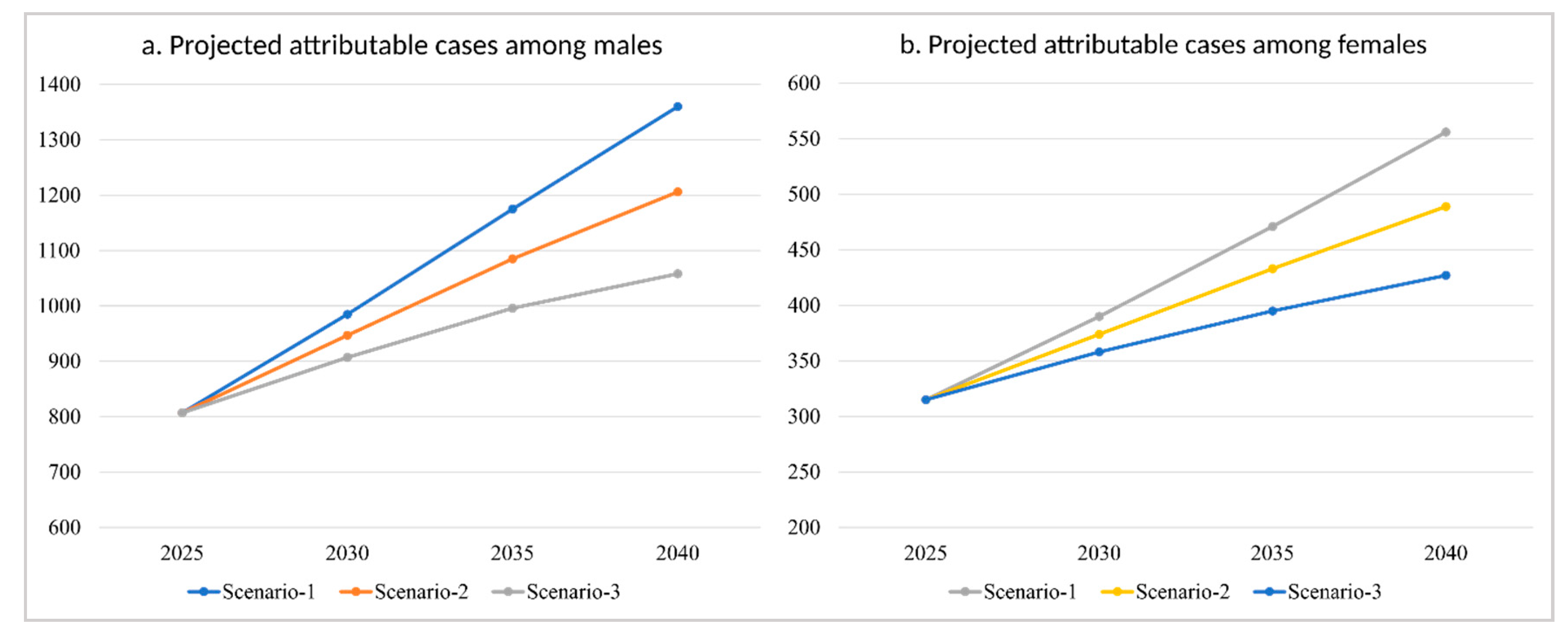
3.5. Projections
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund International: London, UK, 2018. [Google Scholar]
- Althubiti, M.A.; Nour Eldein, M.M. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med. J. 2018, 39, 1259–1262. [Google Scholar] [CrossRef] [PubMed]
- Herzallah, H.K.; Antonisamy, B.R.; Shafee, M.H.; Al-Otaibi, S.T. Temporal trends in the incidence and demographics of cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade. Saudi Med. J. 2019, 40, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Khoja, A.; Aljawadi, M.; Al-Shammari, S.A.; Bokhari, N.N.; Aldarwish, A.A.; Mardini, W.K.; Khoja, T.A. Utilization of Colorectal Cancer Screening among Saudi Elderly Population: A Study from the Saudi National Survey for Elderly Health. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 3401–3407. [Google Scholar] [CrossRef] [PubMed]
- Zubaidi, A.M.; AlSubaie, N.M.; AlHumaid, A.A.; Shaik, S.A.; AlKhayal, K.A.; AlObeed, O.A. Public awareness of colorectal cancer in Saudi Arabia: A survey of 1070 participants in Riyadh. Saudi J. Gastroenterol. 2015, 21, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Mosli, M.; Alnahdi, Y.; Alghamdi, A.; Baabdullah, M.; Hadadi, A.; Khateery, K.; Alsulami, I.; AlHoqail, A.; Almadi, M.; Jawa, H.; et al. Knowledge, attitude, and practices of primary health care physicians toward colorectal cancer screening. Saudi J. Gastroenterol. 2017, 23, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Aljumah, A.A.; Aljebreen, A.M. Policy of screening for colorectal cancer in Saudi Arabia: A prospective analysis. Saudi J. Gastroenterol. 2017, 23, 161–168. [Google Scholar] [PubMed]
- Levin, T.R.; Corley, D.A.; Jensen, C.D.; Schottinger, J.E.; Quinn, V.P.; Zauber, A.G.; Lee, J.K.; Zhao, W.K.; Udaltsova, N.; Ghai, N.R.; et al. Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology 2018, 155, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Alsanea, N.; Abduljabbar, A.S.; Alhomoud, S.; Ashari, L.H.; Hibbert, D.; Bazarbashi, S. Colorectal cancer in Saudi Arabia: Incidence, survival, demographics and implications for national policies. Ann. Saudi Med. 2015, 35, 196–202. [Google Scholar] [CrossRef]
- Ministry of Health. NCD Risk Factors Standard Report, Saudi Arabia 2004; Ministry of Health, Kingdom of Saudi Arabia: Riyadh, Saudi Arabia, 2005.
- Ministry of Health. Saudi Health Interview Survey Results; Ministry of Health: Riyadh, Saudi Arabia, 2013.
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- International Agency for Research on Cancer. List of Classifications by Cancer Sites with Sufficient or Limited Evidence in Humans, Volumes 1 to 123; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Saudi Cancer Registry. Cancer Incidence Report Saudi Arabia 2015; Saudi Health Council: Riyadh, Saudi Arabia, 2018. Available online: https://nhic.gov.sa/eServices/Documents/ESCRfinal6NOV.pdf (accessed on 26 June 2019).
- Saudi Cancer Registry. Cancer Incidence Report Saudi Arabia 2014; Saudi Health Council: Riyadh, Saudi Arabia, 2017. Available online: https://nhic.gov.sa/eServices/Documents/2014.pdf (accessed on 26 June 2019).
- Joinpoint Regression Program, 4.7.0.0; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute: Bethesda, MD, USA, 2018.
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Brown, K.F.; Rumgay, H.; Dunlop, C.; Ryan, M.; Quartly, F.; Cox, A.; Deas, A.; Elliss-Brookes, L.; Gavin, A.; Hounsome, L.; et al. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br. J. Cancer 2018, 118, 1130–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Zalabani, A.H.; Al-Hamdan, N.A.; Saeed, A.A. The prevalence of physical activity and its socioeconomic correlates in Kingdom of Saudi Arabia: A cross-sectional population-based national survey. J. Taibah Univ. Med. Sci. 2015, 10, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Liang, P.S.; Chen, T.Y.; Giovannucci, E. Cigarette smoking and colorectal cancer incidence and mortality: Systematic review and meta-analysis. Int. J. Cancer 2009, 124, 2406–2415. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Yan, Y.; Colditz, G.A.; Lee, I.M. Physical activity and colon cancer prevention: A meta-analysis. Br. J. Cancer 2009, 100, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Xue, K.; Li, F.F.; Chen, Y.W.; Zhou, Y.H.; He, J. Body mass index and the risk of cancer in women compared with men: A meta-analysis of prospective cohort studies. Eur. J. Cancer Prev. 2017, 26, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; Hayes, J.; Frampton, C.; Potter, J. Modifiable lifestyle factors that could reduce the incidence of colorectal cancer in New Zealand. N. Z. Med. J. 2016, 129, 13–20. [Google Scholar] [PubMed]
- Shield, K.D.; Parkin, D.M.; Whiteman, D.C.; Rehm, J.; Viallon, V.; Micallef, C.M.; Vineis, P.; Rushton, L.; Bray, F.; Soerjomataram, I. Population Attributable and Preventable Fractions: Cancer Risk Factor Surveillance, and Cancer Policy Projection. Curr. Epidemiol. Rep. 2016, 3, 201–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow (accessed on 21 March 2019).
- Vision 2030 National Transformation Program 2020. Available online: https://vision2030.gov.sa/en/ntp (accessed on 26 June 2019).
- Kingdom of Saudi Arabia Vision 2030. Available online: https://vision2030.gov.sa/en/ (accessed on 26 June 2019).
- Vision 2030 Quality of Life Program 2020. Available online: https://vision2030.gov.sa/en/qol (accessed on 26 June 2019).
- Naing, C.; Lai, P.K.; Mak, J.W. Immediately modifiable risk factors attributable to colorectal cancer in Malaysia. BMC Public Health 2017, 17, 637. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Prevalence (in Year 2004) | Relative Risk | Source of Relative Risk | |
|---|---|---|---|
| Men | |||
| Physical inactivity | 60.1% | 0.76 (0.71, 0.82) | [22] |
| Obesity | 28.3% | 1.38 (1.32–1.44) | [23] |
| Overweight | 37.9% | 1.17 (1.12–1.22) | [23] |
| Current smokers | 20.9% | 1.15 (1.00–1.32) | [21] |
| Former smokers | 17.0% | 1.20 (1.04–1.38) | [21] |
| Women | |||
| Physical inactivity | 72.9% | 0.79 (0.71, 0.88) | [22] |
| Obesity | 43.8% | 1.17 (1.06–1.30) | [23] |
| Overweight | 27.6% | 1.07 (1.01–1.14) | [23] |
| Current smokers | 1.2% | 1.15 (1.00–1.32) | [21] |
| Former smokers | 0.6% | 1.20 (1.04–1.38) | [21] |
| PAF (%) | Attributable Cases (2015) | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| Physical inactivity | 16.13 | 16.45 | 130 | 108 |
| Obesity | 9.71 | 6.93 | 79 | 45 |
| Overweight | 6.05 | 1.9 | 49 | 12 |
| Current smokers | 3.04 | 0.18 | 25 | 1 |
| Former smokers | 3.29 | 0.12 | 27 | 1 |
| All factors | 33.29 | 23.94 | 310 | 167 |
| Year | Projected Cases | Scenario-1 | Scenario-2 | Scenario-3 | |||
|---|---|---|---|---|---|---|---|
| PAF 1 | Attrib. Cases 1 | PAF | Attrib. Cases | PAF | Attrib. Cases | ||
| Men | |||||||
| 2025 | 2423 | 33.29% | 807 | 33.29% | 807 | 33.29% | 807 |
| 2030 | 2958 | 33.29% | 985 | 32.00% | 947 | 30.67% | 907 |
| 2035 | 3529 | 33.29% | 1175 | 30.74% | 1085 | 28.21% | 996 |
| 2040 | 4085 | 33.29% | 1360 | 29.52% | 1206 | 25.89% | 1058 |
| Women | |||||||
| 2025 | 1314 | 23.94% | 315 | 23.94% | 315 | 23.94% | 315 |
| 2030 | 1628 | 23.94% | 390 | 22.96% | 374 | 21.96% | 358 |
| 2035 | 1967 | 23.94% | 471 | 22.01% | 433 | 20.10% | 395 |
| 2040 | 2321 | 23.94% | 556 | 21.09% | 489 | 18.38% | 427 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Zalabani, A. Preventability of Colorectal Cancer in Saudi Arabia: Fraction of Cases Attributable to Modifiable Risk Factors in 2015–2040. Int. J. Environ. Res. Public Health 2020, 17, 320. https://doi.org/10.3390/ijerph17010320
Al-Zalabani A. Preventability of Colorectal Cancer in Saudi Arabia: Fraction of Cases Attributable to Modifiable Risk Factors in 2015–2040. International Journal of Environmental Research and Public Health. 2020; 17(1):320. https://doi.org/10.3390/ijerph17010320
Chicago/Turabian StyleAl-Zalabani, Abdulmohsen. 2020. "Preventability of Colorectal Cancer in Saudi Arabia: Fraction of Cases Attributable to Modifiable Risk Factors in 2015–2040" International Journal of Environmental Research and Public Health 17, no. 1: 320. https://doi.org/10.3390/ijerph17010320