Addressing Cardiovascular Health Disparities in Minnesota: Establishment of a Community Steering Committee by FAITH! (Fostering African-American Improvement in Total Health)

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
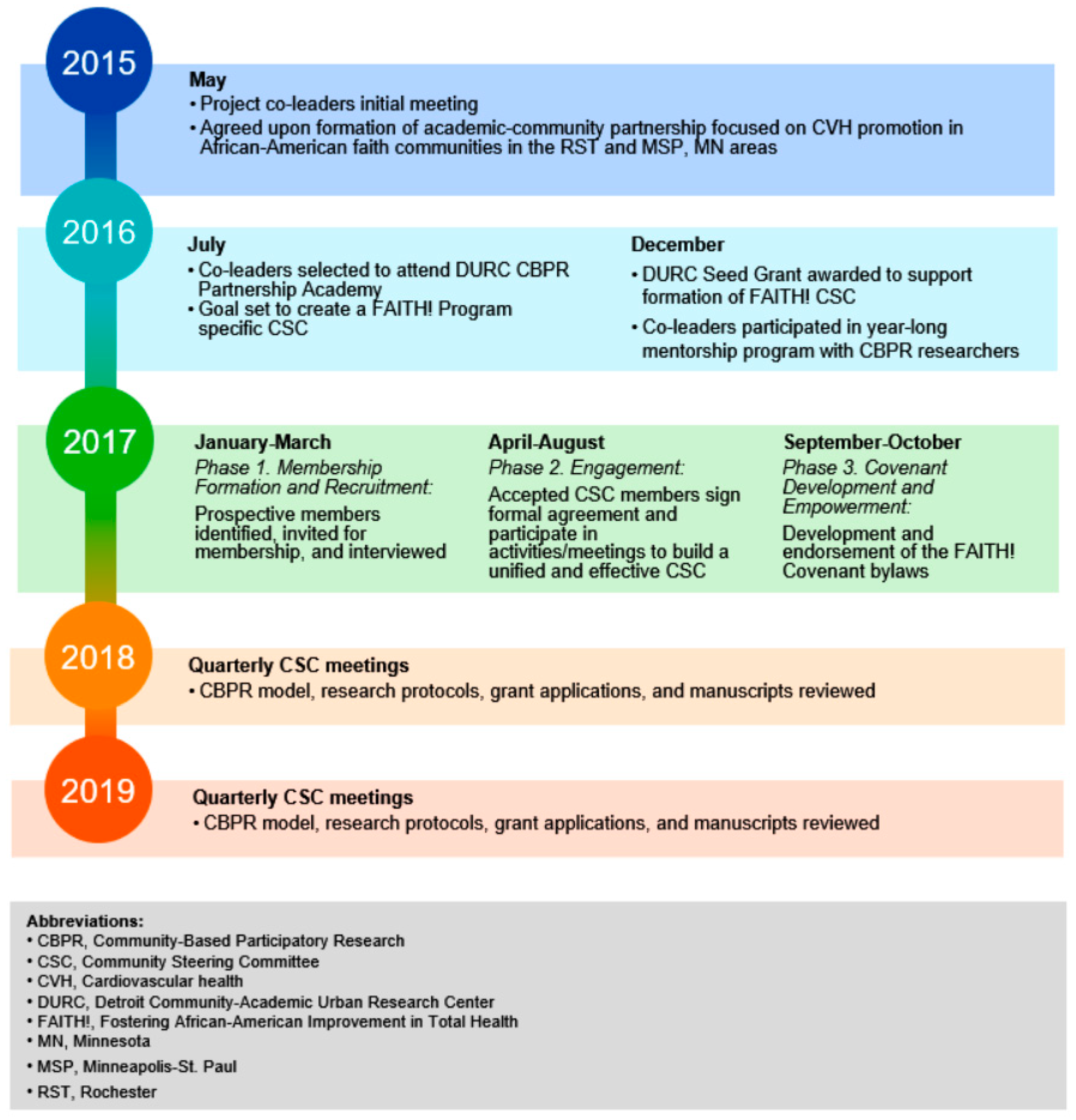
2.1. Academic-Community Partnership Development: First Steps
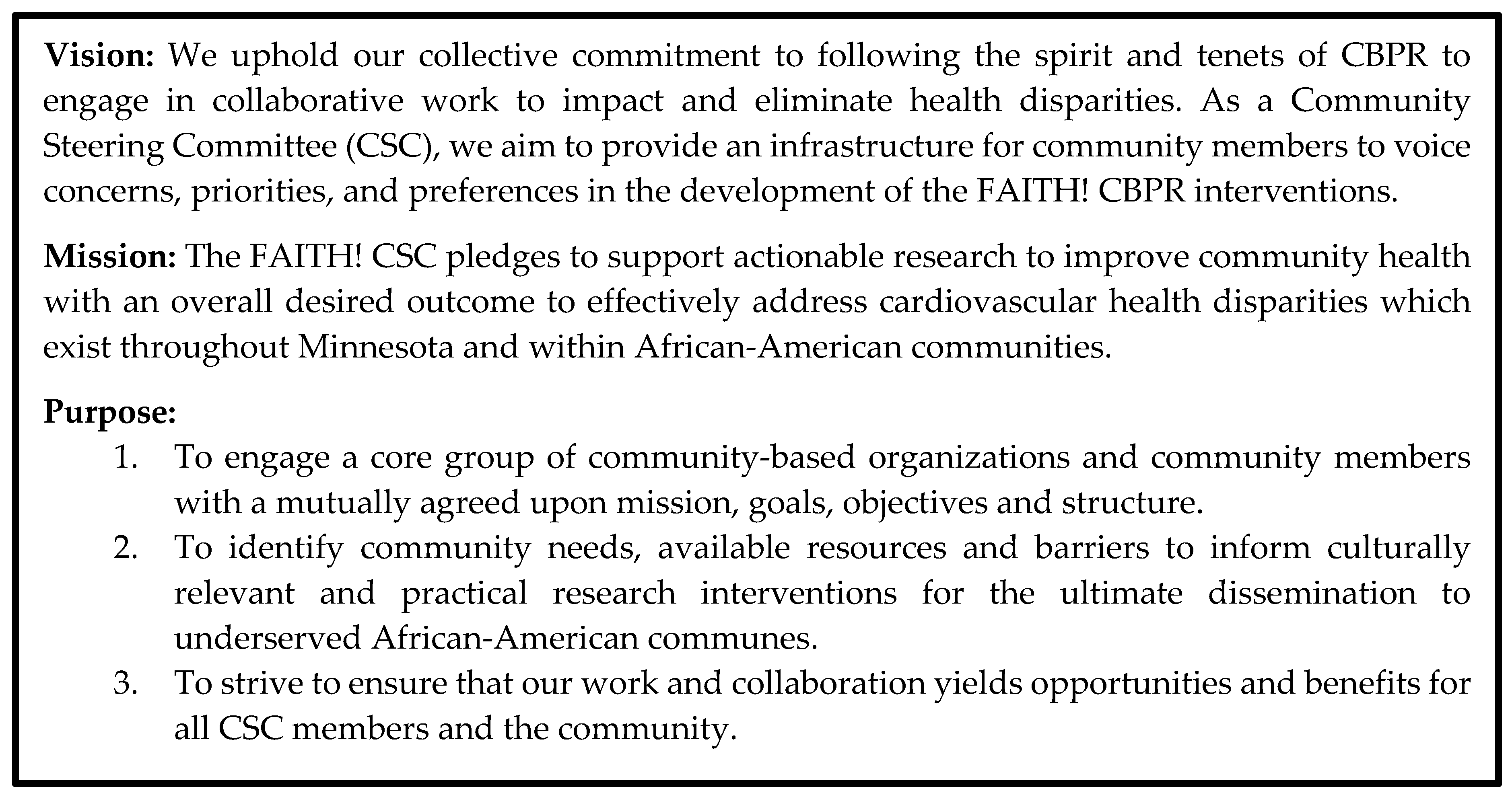
2.2. FAITH! Community Steering Committee Objectives
- Establish a CSC specific to FAITH! composed of representatives from local AA faith- and community-based organizations to provide infrastructure for community members to voice concerns, priorities, and preferences in the development of a culturally appropriate research process and intervention.
- Define a process for the formation, operation, and maintenance of the academic-community partnership and CSC using a CBPR approach through the development of a FAITH! Covenant.
2.3. Community Steering Committee Implementation Process: Three Phases
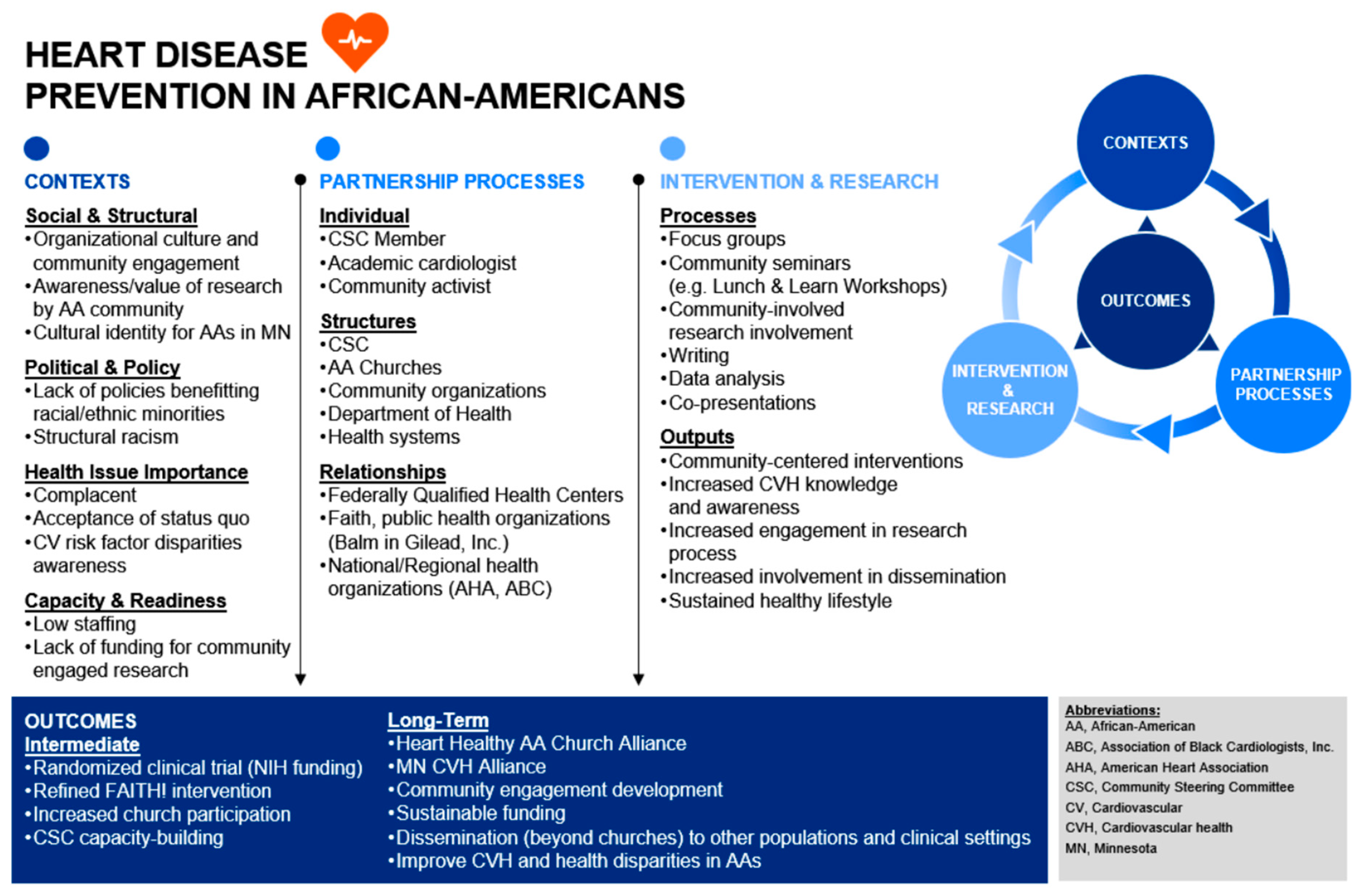
2.4. FAITH! and Community Steering Committee Conceptual Framework
3. Results
3.1. Community Steering Committee Member Evaluations
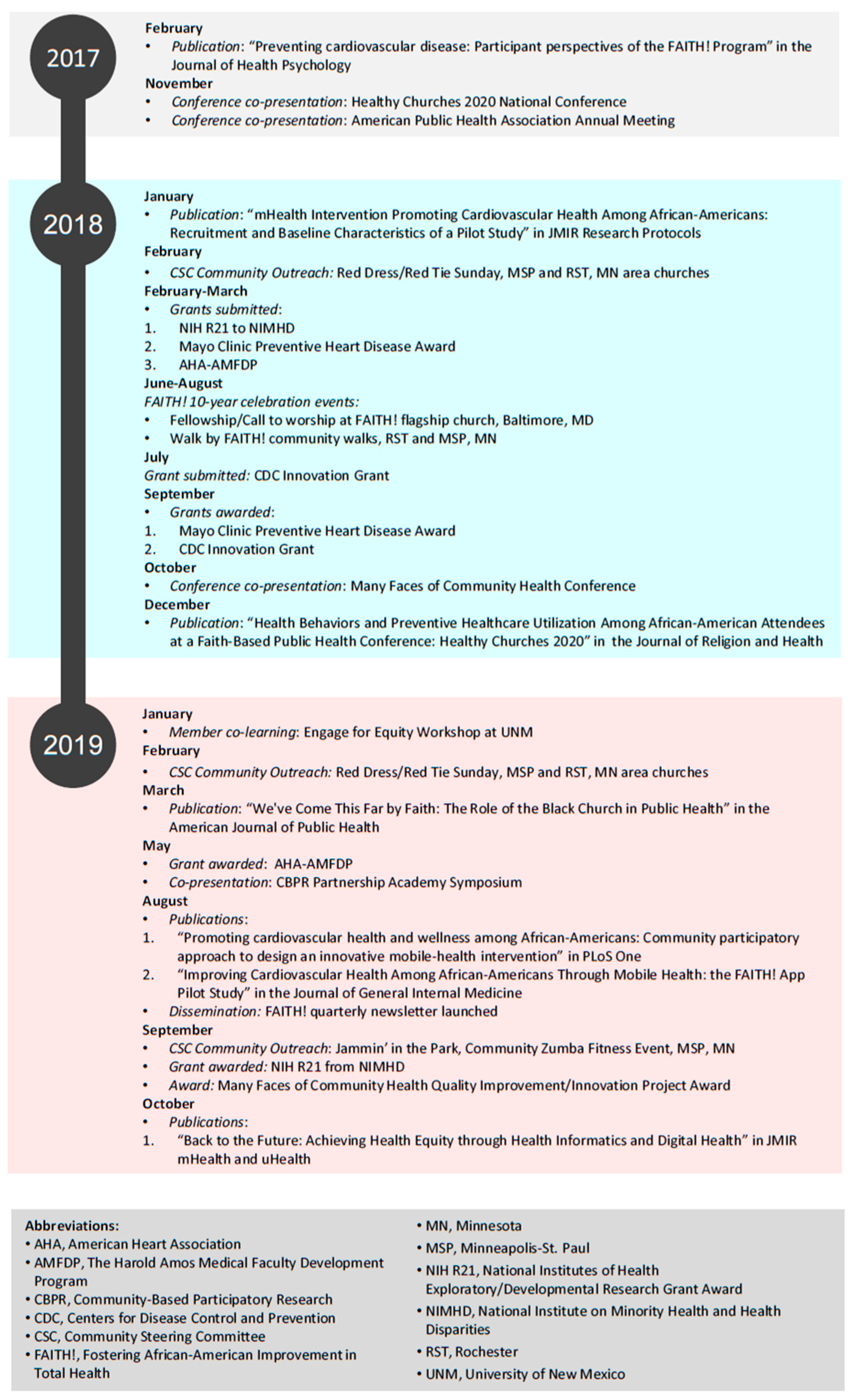
3.2. Community Steering Committee Accomplishments
4. Discussion
4.1. Lessons Learned in Forming a Community Steering Committee
4.1.1. Clarity of Purpose and Vision Is Essential
4.1.2. Group Cohesion Must Be Cultivated
4.1.3. Employ Consistent Review of CBPR Tenets with the CSC
4.1.4. Expect the Unexpected
4.2. Value of a Community Steering Committee
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Sample Letter of Mutual Intent

Letter of Mutual Intent for FAITH! (Fostering African-American Improvement in Total Health) Program Community Steering Committee
Introduction:
Desired Outcome:
Objectives:
Specific Activities and Expectations:
Summary
Community Steering Committee Member
Appendix B. FAITH! Community Steering Committee (CSC) Retreat Agenda
| Time | Agenda |
| 2:00–2:10 pm | Welcome and Introductions |
| 2:10–2:15 pm | Retreat Purpose |
| |
| |
| |
| 2:15–2:45 pm | Group Discussion: Why I joined the FAITH! CSC |
| 2:45–2:55 pm | Overview of Community-Based Participatory Research (CBPR) Key Principles |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| 2:55–3:30 pm | FAITH! Project background |
| Community-medical center partnership with African-American congregations and Mayo Clinic | |
| Goals: | |
| |
| |
| |
| 3:30–3:50 pm | Active Break |
| 3:50–4:05 pm | Breakout Session 1: Elements of a successful community meeting |
| List 5 elements of a successful and 5 elements of an unsuccessful meeting | |
| 4:05–4:20 pm | Breakout Session 2: Case story on trust-building |
| |
| |
| 4:20–4:40 pm | Questions and Answers |
| 4:40–5:00 pm | Closing Remarks and Next Steps |
| |
|
References
- Brewer, L.C.; Balls-Berry, J.E.; Dean, P.; Lackore, K.; Jenkins, S.; Hayes, S.N. Fostering African-American Improvement in Total Health (FAITH!): An Application of the American Heart Association’s Life’s Simple 7 among Midwestern African-Americans. J. Racial Ethn. Health Dispar. 2016, 4, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R.; Pu, J.; Howard, G.; Albert, M.A.; Anderson, C.A.M.; Bertoni, A.G.; Mujahid, M.S.; Palaniappan, L.; Taylor, H.A., Jr.; Willis, M.; et al. Cardiovascular Health in African Americans: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e393–e423. [Google Scholar] [CrossRef] [PubMed]
- United Health Foundation. America’s Health Rankings. Available online: https://www.americashealthrankings.org/ (accessed on 10 June 2019).
- Minnesota Department of Health. Cardiovascular Health Indicator, Measure: Heart Disease Death Rate. Available online: https://www.health.state.mn.us/diseases/cardiovascular/cardio-dashboard/heartdeathr.html (accessed on 21 May 2019).
- Ceasar, J.; Peters-Lawrence, M.H.; Mitchell, V.; Powell-Wiley, T.M. The Communication, Awareness, Relationships and Empowerment (C.A.R.E.) Model: An Effective Tool for Engaging Urban Communities in Community-Based Participatory Research. Int. J. Environ. Res. Public Health 2017, 14, 1422. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.C. Ethics in public health research: Protecting human subjects: The role of community advisory boards. Am. J. Public Health 2004, 94, 918–922. [Google Scholar] [CrossRef]
- Wallerstein, N.B.; Duran, B. Using community-based participatory research to address health disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Victor, R.G.; Lynch, K.; Li, N.; Blyler, C.; Muhammad, E.; Handler, J.; Brettler, J.; Rashid, M.; Hsu, B.; Foxx-Drew, D.; et al. A Cluster-Randomized Trial of Blood-Pressure Reduction in Black Barbershops. N. Engl. J. Med. 2018, 378, 1291–1301. [Google Scholar] [CrossRef]
- Udoh, I.C.; Chopel, A.; Minkler, M.; Smith, C.D.; Walton, S.; Grijalva, C.; Yusuf, A.; Dunbar, M. Developing and using a partnership covenant to guide a study of late HIV diagnosis. Prog. Community Health Partnersh. Res. Educ. Action 2013, 7, 403–411. [Google Scholar] [CrossRef]
- Brewer, L.C.; Jenkins, S.; Lackore, K.; Johnson, J.; Jones, C.; Cooper, L.A.; Radecki Breitkopf, C.; Hayes, S.N.; Patten, C. mHealth Intervention Promoting Cardiovascular Health Among African-Americans: Recruitment and Baseline Characteristics of a Pilot Study. JMIR Res. Protoc. 2018, 7, e31. [Google Scholar] [CrossRef]
- Buta, B.; Brewer, L.; Hamlin, D.L.; Palmer, M.W.; Bowie, J.; Gielen, A. An innovative faith-based healthy eating program: From class assignment to real-world application of PRECEDE/PROCEED. Health Promot. Pract. 2011, 12, 867–875. [Google Scholar] [CrossRef]
- Brewer, L.C.; Buta, B.; Hamlin, D.L.; Palmer, M.W.; Bowie, J.; Gielen, A. FAITH! program to improve healthy eating: From class assignment to real-world application of PRECEDE/PROCEED. In Proceedings of the American Public Health Association Annual Meeting and Expo, Philadelphia, PA, USA, 7–11 November 2009. [Google Scholar]
- Brewer, L.C.; Morrison, E.J.; Balls-Berry, J.E.; Dean, P.; Lackore, K.; Jenkins, S.; Cohen, C.; Johnson, J.; Ellis, F.; Mangum, D. Preventing cardiovascular disease: Participant perspectives of the FAITH! Program. J. Health Psychol. 2017, 24, 1710–1723. [Google Scholar] [CrossRef]
- Minnesota Compass: Demographics, Race. Available online: https://www.mncompass.org/demographics/race#7-5468-g (accessed on 23 October 2019).
- Abu-Bakr, A.; Ahmed, H.; Ojo-Fati, O.; Okuyemi, K.S. Clipper Clinic: An Academic and Community Collaborative Model to Addressing Health Disparities within Underserved Communities. J. Fam. Med. 2016, 3, 1052. [Google Scholar]
- Vidscrip. Vidscrip and Southside Community Health Services Launch Text-Message Based Program to Promote Heart Health in Local Barbershops & Beauty Salons. Available online: https://welcome.vidscrip.com/2017/02/28/vidscrip-and-southside-community-health-services-launch-text-message-based-program-to-promote-heart-health-in-local-barbershops-beauty-salons/ (accessed on 4 March 2019).
- Detroit Urban Research Center. CBPR Partnership Academy. Available online: https://www.detroiturc.org/cbpr-partnership-academy.html (accessed on 14 February 2019).
- Newman, S.D.; Andrews, J.O.; Magwood, G.S.; Jenkins, C.; Cox, M.J.; Williamson, D.C. Community advisory boards in community-based participatory research: A synthesis of best processes. Prev. Chronic Dis. 2011, 8, A70. [Google Scholar] [PubMed]
- Bandura, A. Social Foundations of Thought and Action; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Minkler, M.; Wallerstein, N. Improving health through community organization and community building. In Health Behavior and Health Education: Theory, Research, and Practice, 3rd ed.; Glanz, K., Rimer, B., Lewis, F., Eds.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 279–311. [Google Scholar]
- McCormick, J.; Alavi, S.B.; Hanham, J. The importance of context when applying social cognitive theory in organizations. In Handbook of Research on Management Ideas and Panaceas: Adaptation and Context; Edward Elgar Publishing: Cheltenham, UK, 2015; pp. 110–129. [Google Scholar]
- Israel, B.A.; Lichtenstein, R.; Lantz, P.; McGranaghan, R.; Allen, A.; Guzman, J.R.; Softley, D.; Maciak, B. The Detroit Community-Academic Urban Research Center: Development, implementation, and evaluation. J. Public Health Manag. Pract. 2001, 7, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of community-based research: Assessing partnership approaches to improve public health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Parker, E.A.; Rowe, Z.; Salvatore, A.; Minkler, M.; Lopez, J.; Butz, A.; Mosley, A.; Coates, L.; Lambert, G.; et al. Community-based participatory research: Lessons learned from the Centers for Children’s Environmental Health and Disease Prevention Research. Environ. Health Perspect. 2005, 113, 1463–1471. [Google Scholar] [CrossRef]
- Cooper, L.A.; Purnell, T.S.; Ibe, C.A.; Halbert, J.P.; Bone, L.R.; Carson, K.A.; Hickman, D.; Simmons, M.; Vachon, A.; Robb, I.; et al. Reaching for Health Equity and Social Justice in Baltimore: The Evolution of an Academic-Community Partnership and Conceptual Framework to Address Hypertension Disparities. Ethn. Dis. 2016, 26, 369–378. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.; Oetzel, J.; Duran, B.; Tafoya, G.; Belone, L.; Rae, R. What predicts outcomes in CBPR? In Community Based Participatory Research for Health: Process to Outcomes, 2nd ed.; Minkler, M., Wallerstein, N., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100 (Suppl. 1), S40–S46. [Google Scholar] [CrossRef]
- Pullins, C.T.; Seele, P.C.; White, R.O.; Willis, F.B.; Poole, K.; Albertie, M.L.; Chamie, C.; Allen, A.M.; Kelly, M.; Penheiter, S.; et al. Health Behaviors and Preventive Healthcare Utilization Among African-American Attendees at a Faith-Based Public Health Conference: Healthy Churches 2020. J. Relig. Health 2018, 57, 2538–2551. [Google Scholar] [CrossRef]
- Brewer, L.C.; Williams, D.R. We’ve Come This Far by Faith: The Role of the Black Church in Public Health. Am. J. Public Health 2019, 109, 385–386. [Google Scholar] [CrossRef]
- Brewer, L.C.; Hayes, S.N.; Caron, A.R.; Derby, D.A.; Breutzman, N.S.; Wicks, A.; Raman, J.; Smith, C.M.; Schaepe, K.S.; Sheets, R.E.; et al. Promoting cardiovascular health and wellness among African-Americans: Community participatory approach to design an innovative mobile-health intervention. PLoS ONE 2019, 14, e0218724. [Google Scholar] [CrossRef]
- Brewer, L.C.; Fortuna, K.; Jones, C.; Walker, R.; Hayes, S.N.; Patten, C.; Cooper, L.A. Back to the Future: Achieving Health Equity through Health Informatics and Digital Health. JMIR mHealth uHealth 2019. In Press. [Google Scholar] [CrossRef]
- National Institutes of Health. NIH Exploratory/Developmental Research Grant Award (R21). Available online: https://grants.nih.gov/grants/funding/r21.htm (accessed on 17 May 2019).
- Robert Wood Johnson Foundation. Harold Amos Medical Faculty Development Program (AMFDP). Available online: https://www.rwjf.org/en/library/funding-opportunities/2019/harold-amos-medical-faculty-development-program-cfa.html (accessed on 17 May 2019).
- Minnesota Department of Health. Minnesota Earns New CDC Grants to Expand Efforts Preventing Heart Disease and Diabetes. Available online: https://www.health.state.mn.us/news/pressrel/2018/heartdiabetes121318.html (accessed on 17 May 2019).
- Brewer, L.C.; Jones, C. Establishing a Community Steering Committee Through a Community-Based Participatory Approach: Lessons Learned from the FAITH! (Fostering African-American Improvement in Total Health) Program. In Proceedings of the American Public Health Association Annual Meeting and Expo, Philadelphia, PA, USA, 4–8 November 2017. [Google Scholar]
- The Balm in Gilead Healthy Churches 2020 Conference. Available online: http://healthychurches2020conference.org/ (accessed on 1 October 2019).
- Minnesota Association of Community Health Centers. Many Faces of Community Health Conference. Available online: https://manyfacesconference.org/ (accessed on 2 October 2019).
- University of New Mexico, HSC, Center for Participatory Research. CBPR Engage for Equity (2015–2020). Available online: https://cpr.unm.edu/research-projects/cbpr-project/index.html (accessed on 1 October 2019).
- Mayo Clinic Office of Health Disparities Research. High Visibility “Walk by FAITH!” Event Celebrates Intervention’s First Decade. Available online: https://healthdisparitiesresearchblog.mayo.edu/2018/09/19/high-visibility-walk-by-faith-event-celebrates-interventions-first-decade/ (accessed on 1 October 2019).
- Coughlin, S.S.; Smith, S.A. A review of community-based participatory research studies to promote physical activity among African Americans. J. Ga. Public Health Assoc. 2016, 5, 220–227. [Google Scholar] [PubMed]
- Kaiser Family Foundation. 2017 Population Distribution by Race/Ethnicity. Available online: https://www.kff.org/other/state-indicator/distribution-by-raceethnicity/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed on 13 September 2019).
- Pew Research Center. Religious Landscape Study—Blacks. Available online: https://www.pewforum.org/religious-landscape-study/racial-and-ethnic-composition/black/ (accessed on 13 September 2019).
- Edmondson, A.; Roloff, K. Leveraging Diversity through Psychological Safety. Rotman Magazine, 1 September 2009; 47–51. [Google Scholar]
- Christopher, S.; Saha, R.; Lachapelle, P.; Jennings, D.; Colclough, Y.; Cooper, C.; Cummins, C.; Eggers, M.J.; FourStar, K.; Harris, K. Applying indigenous community-based participatory research principles to partnership development in health disparities research. Fam. Community Health 2011, 34, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Michael, Y.L.; Farquhar, S.A.; Wiggins, N.; Green, M.K. Findings from a community-based participatory prevention research intervention designed to increase social capital in Latino and African American communities. J. Immigr. Minor. Health 2008, 10, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.L.; Brawner, B.; Leader, A.; Voytek, C.; Jemmott, L.S.; Frank, I. Incorporating Community Based Participatory Research Principles for the Development of a HPV Prevention Program for African American Adolescent Females and their Parents/Guardians. Am. J. Health Stud. 2012, 27, 1–7. [Google Scholar]
- Gonzalez-Guarda, R.M.; Jones, E.J.; Cohn, E.; Gillespie, G.L.; Bowen, F. Advancing nursing science through community advisory boards: Working effectively across diverse communities. Adv. Nurs. Sci. 2017, 40, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Ortega, S.; McAlvain, M.S.; Briant, K.J.; Hohl, S.; Thompson, B. Perspectives of Community Advisory Board Members in a Community-Academic Partnership. J. Health Care Poor Underserved 2018, 29, 1529–1543. [Google Scholar] [CrossRef]
- Galea, S.; Factor, S.H.; Bonner, S.; Foley, M.; Freudenberg, N.; Latka, M.; Palermo, A.G.; Vlahov, D. Collaboration among community members, local health service providers, and researchers in an urban research center in Harlem, New York. Public Health Rep. 2001, 116, 530–539. [Google Scholar] [CrossRef]
- McDavitt, B.; Bogart, L.M.; Mutchler, M.G.; Wagner, G.J.; Green, H.D., Jr.; Lawrence, S.J.; Mutepfa, K.D.; Nogg, K.A. Dissemination as Dialogue: Building Trust and Sharing Research Findings Through Community Engagement. Prev. Chronic Dis. 2016, 13, 150473. [Google Scholar] [CrossRef]
- Moreno-John, G.; Fleming, C.; Ford, M.E.; Lichtenberg, P.; Mangione, C.M.; Perez-Stable, E.J.; Tilley, B.; Washington, O.G.; Carrasquillo, O. Mentoring in community-based participatory research: The RCMAR experience. Ethn. Dis. 2007, 17, S33–S43. [Google Scholar]
- Joseph, R.P.; Keller, C.; Affuso, O.; Ainsworth, B.E. Designing Culturally Relevant Physical Activity Programs for African-American Women: A Framework for Intervention Development. J. Racial Ethn. Health Dispar. 2017, 4, 397–409. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FAITH! Community Steering Committee Member Organizations | |
|---|---|
| Community Organizations | Appetite for Change, Minneapolis, MN |
| Hue-MAN Partnership, Minneapolis, MN | |
| Samuel Simmons Consulting, Minneapolis, MN | |
| National/Regional Organizations | YMCA of the Greater Twin Cities, Minneapolis, MN |
| American Heart Association, Minnesota Division | |
| Volunteers of America, Minnesota and Wisconsin Division | |
| Thrivent Financial, Rochester, MN | |
| Faith-Based Organizations | Full Proof Ministry Church of God in Christ, Crystal, MN |
| Christ’s Church of the Jesus Hour, Rochester MN | |
| Academic Partners | Mayo Clinic Department of Cardiovascular Medicine, Rochester, MN |
| Health Systems | Mayo Clinic, Rochester, MN |
| Allina Health, Minneapolis, MN | |
| Hennepin County Medical Center, Minneapolis, MN | |
| Governmental Health Agencies | Minnesota Department of Health, St. Paul, MN |
| Health Insurance Organizations | BlueCross and BlueShield Minnesota, Eagan, MN |
| (1) Engagement Phase: Retreat (N = 8) | (2) Engagement Phase: Operating Procedures and Maintenance Meeting (N = 7) | (3) Covenant Development/ Empowerment Phase: Meeting 1 (N = 6) | (4) Covenant Development/ Empowerment Phase: Meeting 3 (N = 4) | Total (N = 25) | |
|---|---|---|---|---|---|
| I was notified of this meeting with sufficient notice | |||||
| Missing | 0 | 0 | 2 | 0 | 2 |
| True | 8 (100.0%) | 7 (100.0%) | 4 (100.0%) | 4 (100.0%) | 23 (100.0%) |
| The meeting started and ended on time | |||||
| Missing | 1 | 2 | 2 | 0 | 5 |
| True | 7 (100.0%) | 4 (80.0%) | 4 (100.0%) | 4 (100.0%) | 19 (95.0%) |
| False | 0 (0.0%) | 1 (20.0%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) |
| The meeting was worth my time | |||||
| Missing | 0 | 2 | 2 | 0 | 4 |
| True | 8 (100.0%) | 4 (80.0%) | 4 (100.0%) | 4 (100.0%) | 20 (95.2%) |
| Don’t know | 0 (0.0%) | 1 (20.0%) | 0 (0.0%) | 0 (0.0%) | 1 (4.8%) |
| Agenda | |||||
| Good | 3 (37.5%) | 4 (57.1%) | 3 (50.0%) | 0 (0.0%) | 10 (40.0%) |
| Excellent | 5 (62.5%) | 3 (42.9%) | 3 (50.0%) | 4 (100.0%) | 15 (60.0%) |
| The meeting objectives were accomplished | |||||
| Missing | 0 | 1 | 0 | 0 | 1 |
| Fair | 0 (0.0%) | 2 (33.3%) | 0 (0.0%) | 0 (0.0%) | 2 (8.3%) |
| Good | 4 (50.0%) | 1 (16.7%) | 3 (50.0%) | 0 (0.0%) | 8 (33.3%) |
| Excellent | 4 (50.0%) | 3 (50.0%) | 3 (50.0%) | 4 (100.0%) | 14 (58.3%) |
| Location of meeting | |||||
| Fair | 0 (0.0%) | 0 (0.0%) | 1 (16.7%) | 1 (25.0%) | 2 (8.0%) |
| Good | 2 (25.0%) | 3 (42.9%) | 4 (66.7%) | 3 (75.0%) | 12 (48.0%) |
| Excellent | 6 (75.0%) | 4 (57.1%) | 1 (16.7%) | 0 (0.0%) | 11 (44.0%) |
| Timing of meeting | |||||
| Fair | 1 (12.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (4.0%) |
| Good | 3 (37.5%) | 3 (42.9%) | 3 (50.0%) | 1 (25.0%) | 10 (40.0%) |
| Excellent | 4 (50.0%) | 4 (57.1%) | 3 (50.0%) | 3 (75.0%) | 14 (56.0%) |
| Quality of facilitators/presenters | |||||
| Good | 1 (12.5%) | 2 (28.6%) | 2 (33.3%) | 0 (0.0%) | 5 (20.0%) |
| Excellent | 7 (87.5%) | 5 (71.4%) | 4 (66.7%) | 4 (100.0%) | 20 (80.0%) |
| Information shared at this meeting | |||||
| Good | 2 (25.0%) | 4 (57.1%) | 2 (33.3%) | 0 (0.0%) | 8 (32.0%) |
| Excellent | 6 (75.0%) | 3 (42.9%) | 4 (66.7%) | 4 (100.0%) | 17 (68.0%) |
| The handouts | |||||
| Good | 2 (25.0%) | 3 (42.9%) | 3 (50.0%) | 0 (0.0%) | 8 (32.0%) |
| Excellent | 6 (75.0%) | 4 (57.1%) | 3 (50.0%) | 4 (100.0%) | 17 (68.0%) |
| Opportunities for participation and sharing | |||||
| Fair | 0 (0.0%) | 0 (0.0%) | 1 (16.7%) | 0 (0.0%) | 1 (4.0%) |
| Good | 2 (25.0%) | 3 (42.9%) | 2 (33.3%) | 0 (0.0%) | 7 (28.0%) |
| Excellent | 6 (75.0%) | 4 (57.1%) | 3 (50.0%) | 4 (100.0%) | 17 (68.0%) |
| The action plan or strategies developed | |||||
| Missing | 2 | 0 | 0 | 0 | 2 |
| Fair | 0 (0.0%) | 3 (42.9%) | 2 (33.3%) | 0 (0.0%) | 5 (21.7%) |
| Good | 3 (50.0%) | 3 (42.9%) | 2 (33.3%) | 0 (0.0%) | 8 (34.8%) |
| Excellent | 3 (50.0%) | 1 (14.3%) | 2 (33.3%) | 4 (100.0%) | 10 (43.5%) |
| Outline of next steps/follow-up | |||||
| Missing | 2 | 2 | 0 | 0 | 4 |
| Good | 2 (33.3%) | 3 (60.0%) | 4 (66.7%) | 0 (0.0%) | 9 (42.9%) |
| Excellent | 4 (66.7%) | 2 (40.0%) | 2 (33.3%) | 4 (100.0%) | 12 (57.1%) |
| Food served | |||||
| Good | 2 (25.0%) | 3 (42.9%) | 4 (66.7%) | 0 (0.0%) | 9 (36.0%) |
| Excellent | 6 (75.0%) | 4 (57.1%) | 2 (33.3%) | 4 (100.0%) | 16 (64.0%) |
| Survey Results | |
| Total (n = 7) | |
| The CSC is fulfilling my expectations1 | |
| Agree | 4 (57.1%) |
| Strongly agree | 3 (42.9%) |
| The CSC allows me to express my opinions and ideas1 | |
| Agree | 1 (14.3%) |
| Strongly agree | 6 (85.7%) |
| The CSC has a clear mission/vision1 | |
| Agree | 3 (42.9%) |
| Strongly agree | 4 (57.1%) |
| The CSC co-chairs are effective in leading the meetings1 | |
| Agree | 5 (71.4%) |
| Strongly agree | 2 (28.6%) |
| The CSC co-chairs are effective in leading the project as a whole1 | |
| Neutral | 1 (14.3%) |
| Agree | 3 (42.9%) |
| Strongly Agree | 3 (42.9%) |
| CSC members are easy to work with1 | |
| Agree | 3 (42.9%) |
| Strongly agree | 4 (57.1%) |
| The CSC FAITH! Covenant is clear and provides infrastructure to the group1 | |
| Neutral | 1 (14.3%) |
| Agree | 3 (42.9%) |
| Strongly agree | 3 (42.9%) |
| The number of CSC members is adequate1 | |
| Disagree | 1 (14.3%) |
| Neutral | 3 (42.9%) |
| Agree | 2 (28.6%) |
| Strongly agree | 1 (14.3%) |
| The CSC has an action plan or strategies developed1 | |
| Neutral | 1 (14.3%) |
| Agree | 2 (28.6%) |
| Strongly agree | 4 (57.1%) |
| The CSC has an outline of next steps/follow up1 | |
| Neutral | 1 (14.3%) |
| Agree | 3 (42.9%) |
| Strongly agree | 4 (57.1%) |
| The CSC is focused on improving community health1 | |
| Strongly agree | 7 (100.0%) |
| Overall, how would you rate your satisfaction with being a CSC member? 2 | |
| Satisfied | 4 (57.1%) |
| Very satisfied | 3 (42.9%) |
| Open-Ended Question Responses 3 | |
| Is there anyone (or group representative) who should be a part of the CSC? | |
| “It would be impactful for churches to commit time and staff to support and serve as advocates.” | |
| “Someone younger from a church group. Another voice outside the church leadership. Someone we are trying to serve/a participant.” | |
| What amendments do you have to the FAITH! Covenant? | |
| “Focus group participants – allowing input from a personal lens. Work more on using common language for community connections. Methods for achieving goals for personal and organizational perspectives.” | |
| Is there anything that we did this year as a CSC that should be continued in the future? | |
| “[Continue with] a future outline of meetings, projects, and the steps to prepare all presenting stuff as new knowledge for the team.” | |
| “…intermixing face to face meetings with conference calls is a good mix in managing time.” | |
| “Continue the communications about the project. Continue to think outside the box on community engagement.” | |
| “Continue to cross-check where our work connects with other similar work.” | |
| “Everything.” | |
| “[The] annual walk by FAITH!” | |
| Do you have any other comments/feedback you would like to share? | |
| “I believe in the mission and respect all the different expertise and opinions brought to the table.” | |
| “It would be good to hear more about the app and what progress is being made and how will it be introduced to address the needs of the health issues around cardiovascular health. Adding clarity of the work we are discussing at our meetings and how it is building the necessity feedback to create this service product for the community.” | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manjunath, C.; Ifelayo, O.; Jones, C.; Washington, M.; Shanedling, S.; Williams, J.; Patten, C.A.; Cooper, L.A.; Brewer, L.C. Addressing Cardiovascular Health Disparities in Minnesota: Establishment of a Community Steering Committee by FAITH! (Fostering African-American Improvement in Total Health). Int. J. Environ. Res. Public Health 2019, 16, 4144. https://doi.org/10.3390/ijerph16214144
Manjunath C, Ifelayo O, Jones C, Washington M, Shanedling S, Williams J, Patten CA, Cooper LA, Brewer LC. Addressing Cardiovascular Health Disparities in Minnesota: Establishment of a Community Steering Committee by FAITH! (Fostering African-American Improvement in Total Health). International Journal of Environmental Research and Public Health. 2019; 16(21):4144. https://doi.org/10.3390/ijerph16214144
Chicago/Turabian StyleManjunath, Chandrika, Oluwatomilona Ifelayo, Clarence Jones, Monisha Washington, Stanton Shanedling, Johnnie Williams, Christi A. Patten, Lisa A. Cooper, and LaPrincess C. Brewer. 2019. "Addressing Cardiovascular Health Disparities in Minnesota: Establishment of a Community Steering Committee by FAITH! (Fostering African-American Improvement in Total Health)" International Journal of Environmental Research and Public Health 16, no. 21: 4144. https://doi.org/10.3390/ijerph16214144