Assessment of Safe Listening Intentional Behavior Toward Personal Listening Devices in Young Adults

Abstract
:1. Introduction
2. Methods
2.1. Survey
2.2. Data Analyses
3. Results
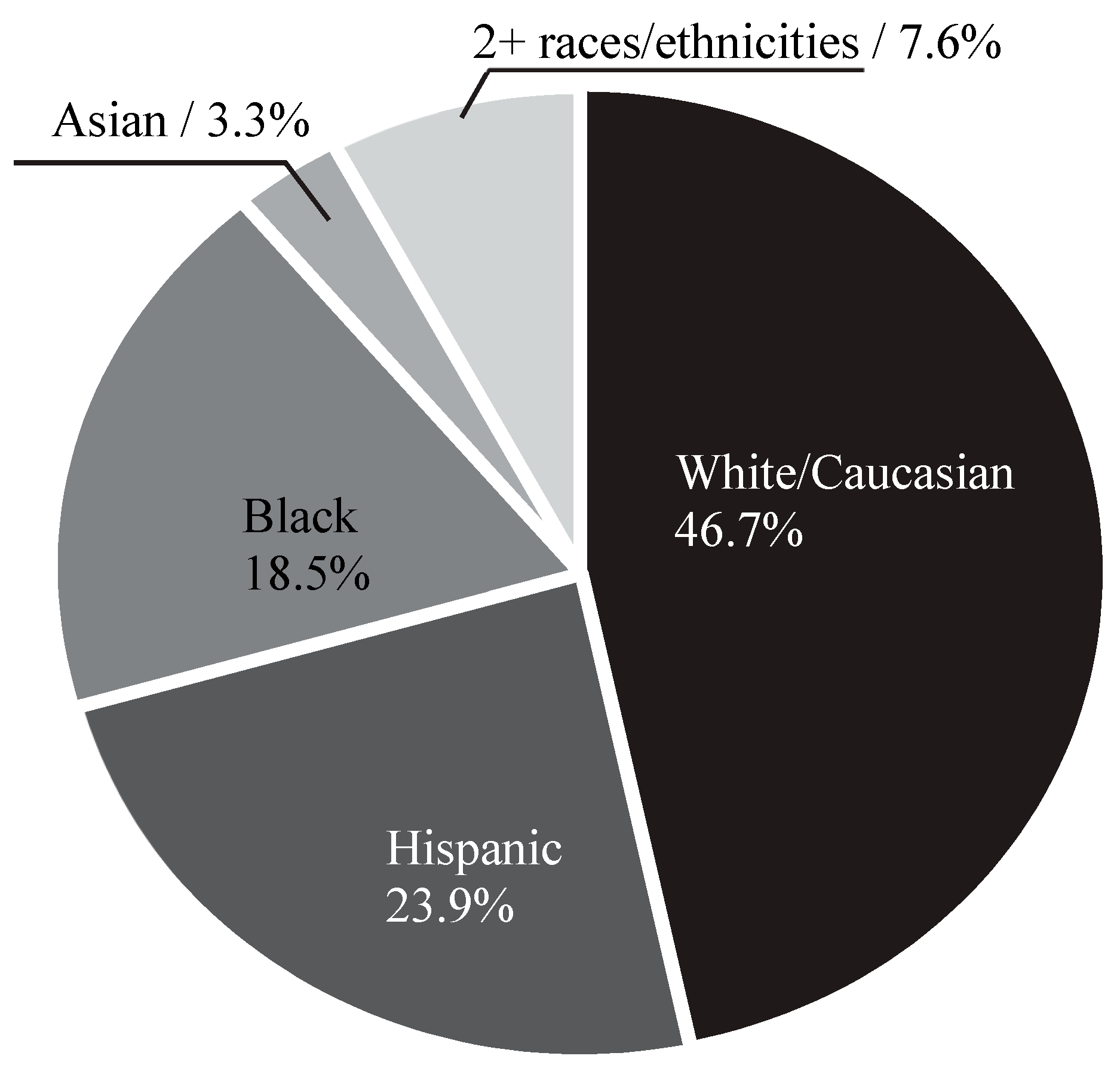
3.1. Participants
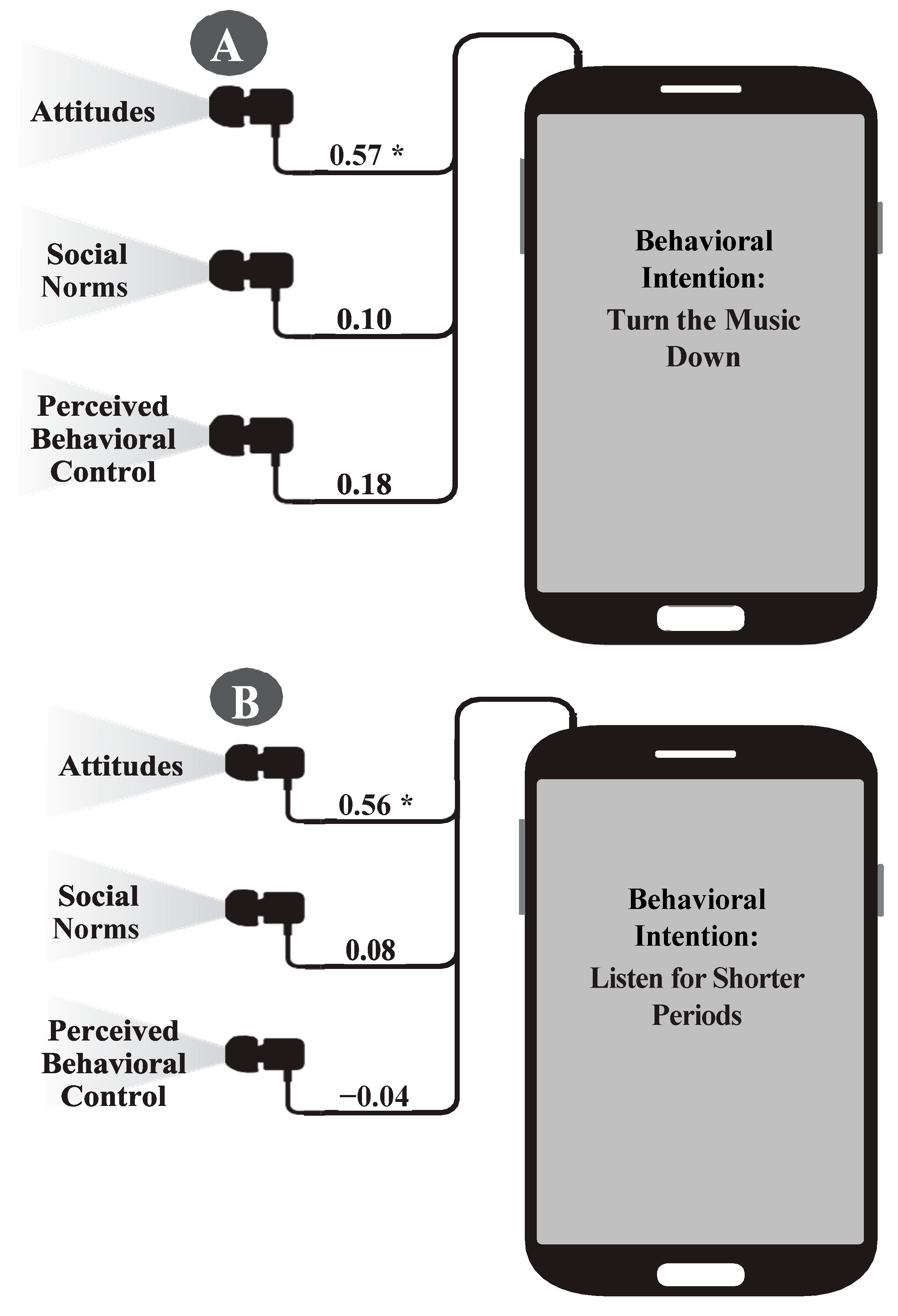
3.2. Theory of Planned Behavior
3.3. TPB Attitudes
3.4. TPB Social Norms
3.5. TPB Perceived Behavioral Control
3.6. TPB Intention
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 1.1 Billion People at Risk of Hearing Loss: WHO Highlights Serious. Threat Posed by Exposure to Recreational Noise. Available online: http://www.who.int/mediacentre/news/releases/2015/ear-care/en/ (accessed on 31 July 2019).
- Figueiredo, R.R.; de Azevedo, A.A.; de Oliveira, P.M.; Pereira, S.; Amorim, V.; Rios, A.G.; Baptista, V. Incidence of tinnitus in MP3 player users. Braz. J. Otorhinolaryngol. 2011, 77, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Le Prell, C.G.; Dell, S.; Hensley, B.N.; Hall, J.W., III; Campbell, K.C.M.; Antonelli, P.J.; Guire, K. Digital music exposure reliably induces temporary threshold shift in normal hearing human subjects. Ear Hear. 2012, 33, e44–e58. [Google Scholar] [CrossRef] [PubMed]
- Le Prell, C.G.; Spankovich, C.; Lobariñas, E.; Griffiths, S.K. Extended high-frequency thresholds in college students: effects of music player use and other recreational noise. J. Am. Acad. Audiol. 2013, 24, 725–739. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Seluakumaran, K.; Husain, R. Hearing risk associated with the usage of personal listening devices among urban high school students in Malaysia. Public Health 2013, 127, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Zhao, F.; Guderley, N.; Manchaiah, V. Daily music exposure dose and hearing problems using personal listening devices in adolescents and young adults: A systematic review. Int. J. Audiol. 2016, 55, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopal, K.V.; Mills, L.E.; Phillips, B.S.; Nandy, R. Risk assessment of recreational noise-induced hearing loss from exposure through a personal audio system-ipod touch. J. Am. Acad. Audiol. 2019, 30, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.F.; Kujawa, S.G.; Hammill, T.; Le Prell, C.; Kil, J. Temporary and permanent noise-induced threshold shifts: A review of basic and clinical observations. Otol. Neurotol. 2016, 37, 271–275. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Occupational Safety and Health (NIOSH). Occupational Noise Exposure: Revised Criteria 1998; Department of Health and Human Services: Cincinnati, OH, USA, 1998.
- Occupational Safety and Health Administration (OSHA). Noise Exposure Computation. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.95AppA (accessed on 31 July 2019).
- Gopal, K.V. Current Practices in the Assessment of Recreational Noise-Induced Hearing Loss: A Review. Make Listening Safe World Health Organization Monograph. 2017. Available online: http://www.who.int/pbd/deafness/Monograph_on_current_Practices_in_the_assessment_of_NIHL_in_recreational_settings.pdf?ua=1 (accessed on 31 July 2019).
- Rawool, V.W.; Colligon-Wayne, L.A. Auditory lifestyles and beliefs related to hearing loss among college students in the USA. Noise Health 2008, 10, 1–10. [Google Scholar] [CrossRef]
- Kumar, A.; Mathew, K.; Alexander, S.A.; Kiran, C. Output sound pressure levels of personal music systems and their effect on hearing. Noise Health 2009, 11, 132–140. [Google Scholar] [CrossRef]
- McNeill, K.; Keith, S.E.; Feder, K.; Konkle, A.T.M.; Michaud, D.S. MP3 player listening habits of 17 to 23-year-old university students. J. Acoust. Soc. Am. 2010, 128, 646–653. [Google Scholar] [CrossRef]
- Le Prell, C.G.; Hensley, B.N.; Campbell, K.C.; Hall, J.W.; Guire, K. Evidence of hearing loss in a ‘normally-hearing’ college-student population. Int. J. Audiol. 2011, 50, S21–S31. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Husain, R.; Seluakumaran, K. Evaluation of early hearing damage in personal listening device users using extended high-frequency audiometry and otoacoustic emissions. Eur. Arch. Otorhinolaryngol. 2014, 271, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Husain, R.; Seluakumaran, K. Hearing risk among young personal listening device users: Effects at high-frequency and extended high-frequency audiogram thresholds. J. Int. Adv. Otol. 2015, 11, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Kumar, U.A.; Deepashree, S.R. Personal music systems and hearing. J. Laryngol. Otol. 2016, 130, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, S.P.; Davis, A.M. Modification of otoacoustic emissions following ear-level exposure to MP3 player music. Int. J. Audiol. 2008, 47, 751–760. [Google Scholar] [CrossRef]
- Keppler, H.; Dhooge, I.; Maes, L.; Wendy, D.; Annelies, B.; Birgit, P.; Freya, S.; Bart, V. Short-term auditory effects of listening to an MP3 player. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Dumitrescu, A.L.; Wagle, M.; Dogaru, B.C.; Manolescu, B. Modeling the theory of planned behavior for intention to improve oral health behaviors: The impact of attitudes, knowledge, and current behavior. J. Oral Sci. 2011, 53, 369–377. [Google Scholar] [CrossRef]
- Cooke, R.; Dahdah, M.; Norman, P.; French, D.P. How well does the theory of planned behavior predict alcohol consumption? A systematic review and meta-analysis. Health Psychol. Rev. 2016, 10, 148–167. [Google Scholar] [CrossRef]
- Dumitrescu, A.L.; Duţă, C.; Dogaru, C.B.; Manolescu, B. Predicting undergraduates’ intentions to improve oral health behaviors: The importance of self–identity–a pilot study. Am. Dent. Hyg. Assoc. 2013, 87, 224–234. [Google Scholar]
- Widén, S.E.; Holmes, A.E.; Erlandsson, S.I. Reported hearing protection use in young adults from Sweden and the USA: Effects of attitude and gender. Int. J. Audiol. 2006, 45, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Quick, B.L.; Stephenson, M.T.; Witte, K.; Vaught, C.; Booth-Butterfield, S.; Patel, D. An examination of antecedents to coal miners’ hearing protection behaviors: A test of the theory of planned behavior. J. Saf. Res. 2008, 39, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Widén, S.E.; Holmes, A.E.; Johnson, T.; Bohlin, M.; Erlandsson, S.I. Hearing, use of hearing protection, and attitudes towards noise among young American adults. Int. J. Audiol. 2009, 48, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Widén, S.E. A suggested model for decision-making regarding hearing conservation: Towards a systems theory approach. Int. J. Audiol. 2013, 52, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Gilles, A.; Van de Heyning, P. Effectiveness of a preventive campaign for noise-induced hearing damage in adolescents. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Balanay, J.A.G.; Kearney, G.D. Attitudes toward noise, perceived hearing symptoms, and reported use of hearing protection among college students: Influence of youth culture. Noise Health 2015, 17, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Keppler, H.; Dhooge, I.; Vinck, B. Hearing in young adults. Part I: The effects of attitudes and beliefs toward noise, hearing loss, and hearing protector devices. Noise Health 2015, 17, 237–244. [Google Scholar] [CrossRef]
- Mencher, G.T.; Gerber, S.E.; McCombe, A. Audiology and Auditory Dysfunction; Allyn and Bacon: Boston, MA, USA, 1997. [Google Scholar]
- Vogel, I.; van de Looij-Jansen, P.M.; Mieloo, C.L.; Burdorf, A.; de Waart, F. Risky music-listening behaviors and associated health-risk behaviors. Pediatrics 2012, 129, 1097–1103. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Symptoms | Percentage (%) |
|---|---|
| Ringing/buzzing in ears | 32.6 |
| Ear fullness | 17.4 |
| Hearing loss/muffled hearing | 9.8 |
| Soreness of ear | 28.3 |
| Limited concentration | 21.7 |
| Decreased tolerance/annoyance to environmental sounds (hyperacusis) | 14.1 |
| More than one symptom | 38.0 |
| None of these | 39.1 |
| Response | Turning Loud Music Down | Listening to Loud Music for a Shorter Duration |
|---|---|---|
| Good | M = 5.78 (SD = 1.33) | M = 5.04 (SD = 1.48) |
| Beneficial | M = 6.11 (SD = 1.05) | M = 5.09 (SD = 1.50) |
| Positive | M = 5.64 (SD = 1.29) | M = 4.90 (SD = 1.42) |
| Negative * | M = 5.71 (SD = 1.45) | M = 5.22 (SD = 1.58) |
| Cronbach’s α | 0.86 | 0.89 |
| Overall | M = 5.81 (SD = 1.10) | M = 5.06 (SD = 1.32) |
| Response | Turning Loud Music Down | Listening to Loud Music for a Shorter Duration |
|---|---|---|
| Coworkers | M = 2.54 (SD = 1.60) | M = 2.45 (SD = 1.66) |
| Friends | M = 2.74 (SD = 1.78) | M = 2.48 (SD = 1.69) |
| Family | M = 3.71 (SD = 2.01) | M = 2.98 (SD = 1.93) |
| Cronbach’s α | 0.86 | 0.88 |
| Overall | M = 3.00 (SD = 1.59) | M = 2.63 (SD = 1.58) |
| Response | Turning Loud Music Down | Listening to Loud Music for a Shorter Duration |
|---|---|---|
| Difficult for me * | M = 5.57 (SD = 1.63) | M = 5.05 (SD = 1.65) |
| No problem | M = 6.08 (SD = 1.39) | M = 5.38 (SD = 1.62) |
| Control | M = 6.49 (SD = 1.05) | M = 6.12 (SD = 1.27) |
| Cronbach’s α | 0.66 | 0.64 |
| Overall | M = 6.04 (SD = 1.07) | M = 5.52 (SD = 1.17) |
| Response | Turning Loud Music Down | Listening to Loud Music for a Shorter Duration |
|---|---|---|
| Willingness to Engage | M = 6.04 (SD = 1.37) | M = 4.74 (SD = 1.82) |
| Recommend to Others | M = 4.62 (SD = 1.88) | M = 3.79 (SD = 1.80) |
| Actively Engage | M = 4.99 (SD = 1.88) | M = 3.79 (SD = 1.84) |
| Cronbach’s α | 0.68 | 0.82 |
| Overall | M = 5.22 (SD = 1.37) | M = 4.11 (SD = 1.57) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gopal, K.V.; Champlin, S.; Phillips, B. Assessment of Safe Listening Intentional Behavior Toward Personal Listening Devices in Young Adults. Int. J. Environ. Res. Public Health 2019, 16, 3180. https://doi.org/10.3390/ijerph16173180
Gopal KV, Champlin S, Phillips B. Assessment of Safe Listening Intentional Behavior Toward Personal Listening Devices in Young Adults. International Journal of Environmental Research and Public Health. 2019; 16(17):3180. https://doi.org/10.3390/ijerph16173180
Chicago/Turabian StyleGopal, Kamakshi V., Sara Champlin, and Bryce Phillips. 2019. "Assessment of Safe Listening Intentional Behavior Toward Personal Listening Devices in Young Adults" International Journal of Environmental Research and Public Health 16, no. 17: 3180. https://doi.org/10.3390/ijerph16173180