Risk of Dementia in Patients with Leptospirosis: A Nationwide Cohort Analysis


Abstract
:1. Background
2. Materials and Methods
2.1. Data Sources
2.2. Study Participants
2.3. Statistical Analysis
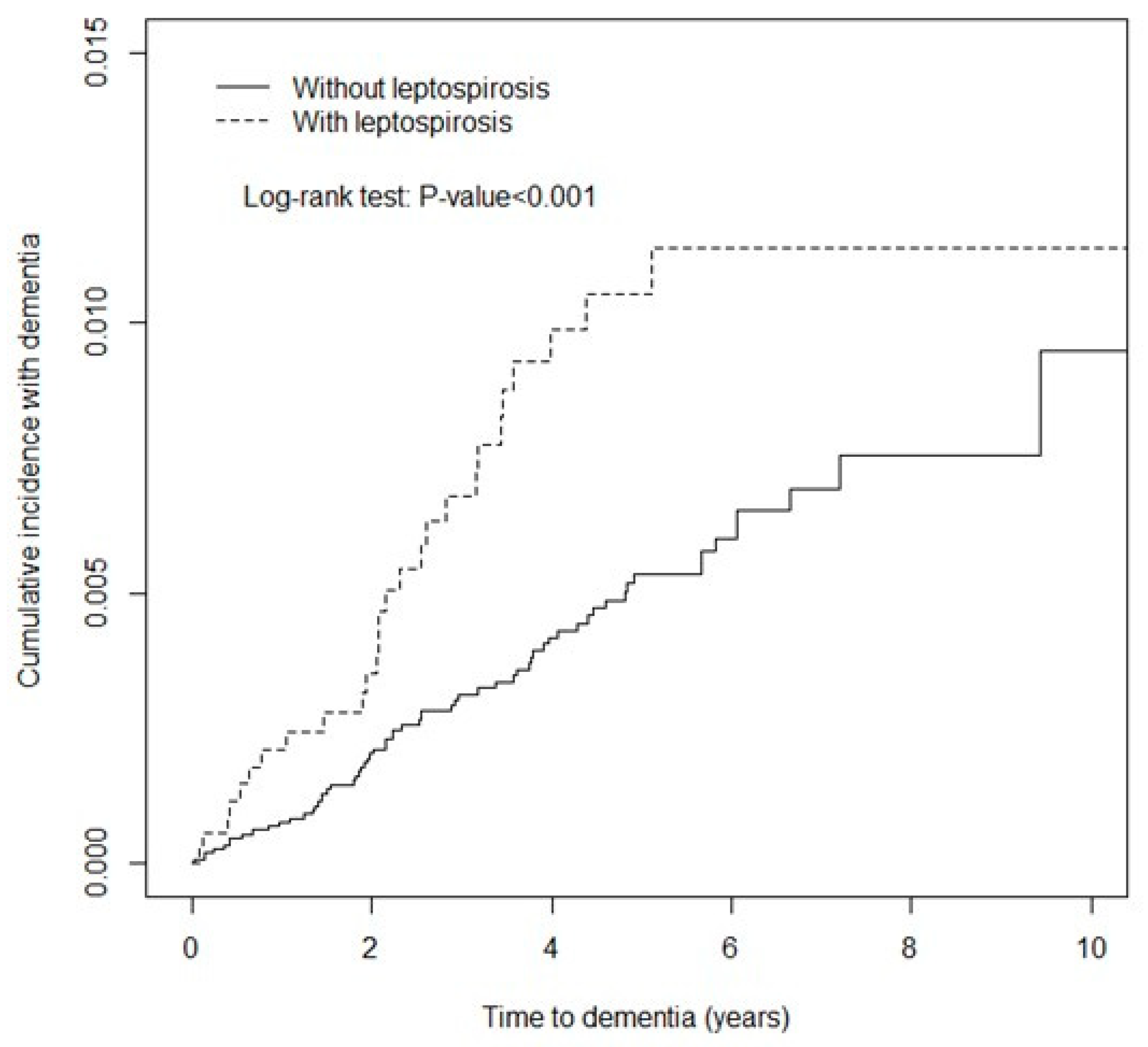
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| NHI | National Health Insurance |
| NHIRD | National Health Insurance Research Database |
| ICD-9-CM | Ninth Revision, Clinical Modification |
| HRs | hazard ratios |
| CIs | confidence intervals |
References
- Levett, P.N. Leptospirosis. Clin. Microbiol. Rev. 2001, 14, 296–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, A.I.; Reis, M.G.; Dourado, C.M.; Johnson, W.D., Jr.; Riley, L.W.; Salvador Leptospirosis Study Group. Urban epidemic of severe leptospirosis in Brazil. Lancet 1999, 354, 820–825. [Google Scholar] [CrossRef]
- Katz, A.R.; Ansdell, V.E.; Effler, P.V.; Middleton, C.R.; Sasaki, D.M. Assessment of the clinical presentation and treatment of 353 cases of laboratory-confirmed leptospirosis in Hawaii, 1974–1998. Clin. Infect. Dis. 2001, 33, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Faine, S.; Adler, B.; Bolin, C.; Perolat, P. Leptospira and Leptospirosis, 2nd ed.; Melbourne Vic: Melbourne, Australia, 1999; p. 295. [Google Scholar]
- Alzheimer’s Association. 2013 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2013, 9, 208–245. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Jolley, D. The incidence of dementia: A meta-analysis. Neurology 1998, 51, 728–733. [Google Scholar] [CrossRef]
- Goodman, R.A.; Lochner, K.A.; Thambisetty, M.; Wingo, T.S.; Posner, S.F.; Ling, S.M. Prevalence of dementia subtypes in United States Medicare fee-for-service beneficiaries, 2011–2013. Alzheimer’s Dement. 2017, 13, 28–37. [Google Scholar] [CrossRef]
- Bennett, S.; Grant, M.M.; Aldred, S. Oxidative stress in vascular dementia and Alzheimer’s disease: A common pathology. J. Alzheimer’s Dis. 2009, 17, 245–257. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; DeCarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the american heart association/american stroke association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef]
- Sun, X.; He, G.; Qing, H.; Zhou, W.; Dobie, F.; Cai, F.; Staufenbiel, M.; Huang, L.E.; Song, W. Hypoxia facilitates Alzheimer’s disease pathogenesis by up-regulating BACE1 gene expression. Proc. Natl. Acad. Sci. USA 2006, 103, 18727–18732. [Google Scholar] [CrossRef]
- Chung, W.S.; Chu, Y.H.; Lin, C.L.; Kao, C.H. Increased risk of acute coronary syndrome among leptospirosis patients: A nationwide cohort analysis. Int. J. Cardiol. 2015, 184, 576–580. [Google Scholar] [CrossRef]
- Database N.H.I.R. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 18 April 2018).
- Chen, Y.C.; Yeh, H.Y.; Wu, J.C.; Haschler, I.; Chen, T.J.; Wetter, T. Taiwan’s National Health Insurance Research Database: Administrative health care database as study object in bibliometrics. Scientometrics 2011, 86, 16. [Google Scholar] [CrossRef]
- Chuang, Y.W.; Yu, M.C.; Lin, C.L.; Yu, T.M.; Shu, K.H.; Huang, S.T.; Kao, C.H. Risk of peripheral arterial occlusive disease in patients with rheumatoid arthritis. A nationwide population-based cohort study. Thromb. Haemost. 2016, 115, 439–445. [Google Scholar] [CrossRef]
- Wang, C.C.; Chang, C.T.; Lin, C.L.; Huang, B.R.; Kao, C.H. Spinal cord injury is associated with an increased risk of atrial fibrillation: A population-based cohort study. Heart Rhythm 2016, 13, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Y.; Hsu, P.Y.; Pan, M.J.; Wu, M.S.; Lee, C.H.; Yu, C.C.; Hung, C.C.; Yang, C.W. Clinical distinction and evaluation of leptospirosis in Taiwan—A case-control study. J. Nephrol. 2005, 18, 45–53. [Google Scholar] [PubMed]
- Pourhoseingholi, M.A.; Baghestani, A.R.; Vahedi, M. How to control confounding effects by statistical analysis. Gastroenterol. Hepatol. Bed Bench 2012, 5, 79–83. [Google Scholar] [PubMed]
- Jansen, A.; Stark, K.; Schneider, T.; Schöneberg, I. Sex differences in clinical leptospirosis in Germany: 1997–2005. Clin. Infect. Dis. 2007, 44, e69–e72. [Google Scholar] [CrossRef] [PubMed]
- Cagliero, J.; Villanueva, S.; Matsui, M. Leptospirosis Pathophysiology: Into the Storm of Cytokines. Front. Cell. Infect. Microbiol. 2018, 8, 204. [Google Scholar] [CrossRef] [Green Version]
- Barage, S.H.; Sonawane, K.D. Amyloid cascade hypothesis: Pathogenesis and therapeutic strategies in Alzheimer’s disease. Neuropeptides 2015, 52, 1–18. [Google Scholar] [CrossRef]
- Bishop, G.M.; Robinson, S.R. The amyloid hypothesis: Let sleeping dogmas lie? Neurobiol. Aging 2002, 23, 1101–1105. [Google Scholar] [CrossRef]
- de la Torre, J.C. Alzheimer disease as a vascular disorder: Nosological evidence. Stroke 2002, 33, 1152–1162. [Google Scholar] [CrossRef]
- Moir, R.D.; Lathe, R.; Tanzi, R.E. The antimicrobial protection hypothesis of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 1602–1614. [Google Scholar] [CrossRef]
- Davis, D.G.; Schmitt, F.A.; Wekstein, D.R.; Markesbery, W.R. Alzheimer neuropathologic alterations in aged cognitively normal subjects. J. Neuropathol. Exp. Neurol. 1999, 58, 376–388. [Google Scholar] [CrossRef] [PubMed]
- Terry, R.D.; Masliah, E.; Salmon, D.P.; Butters, N.; DeTeresa, R.; Hill, R.; Hansen, L.A.; Katzman, R. Physical basis of cognitive alterations in Alzheimer’s disease: Synapse loss is the major correlate of cognitive impairment. Ann. Neurol. 1991, 30, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Aisen, P.S.; Ferris, S.H.; Saumier, D.; Duong, A.; Haine, D.; Garceau, D.; Suhy, J.; Oh, J.; Lau, W.; et al. Effect of tramiprosate in patients with mild-to-moderate Alzheimer’s disease: Exploratory analyses of the MRI sub-group of the Alphase study. J. Nutr. Health Aging 2009, 13, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Imbimbo, B.P.; Giardina, G.A. gamma-secretase inhibitors and modulators for the treatment of Alzheimer’s disease: Disappointments and hopes. Curr. Top. Med. Chem. 2011, 11, 1555–1570. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, V.T. Alzheimer’s dementia begins as a disease of small blood vessels, damaged by oxidative-induced inflammation and dysregulated amyloid metabolism: Implications for early detection and therapy. FASEB J. 2011, 25, 5–13. [Google Scholar] [CrossRef]
- Cline, E.N.; Bicca, M.A.; Viola, K.L.; Klein, W.L. The Amyloid-beta Oligomer Hypothesis: Beginning of the Third Decade. J. Alzheimer’s Dis. 2018, 64, S567–S610. [Google Scholar] [CrossRef]
- Caruso, G.; Distefano, D.A.; Parlascino, P.; Fresta, C.G.; Lazzarino, G.; Lunte, S.M.; Nicoletti, V.G. Receptor-mediated toxicity of human amylin fragment aggregated by short- and long-term incubations with copper ions. Mol. Cell. Biochem. 2017, 425, 85–93. [Google Scholar] [CrossRef]
- Julien, C.; Tomberlin, C.; Roberts, C.M.; Akram, A.; Stein, G.H.; Silverman, M.A.; Link, C.D. In vivo induction of membrane damage by beta-amyloid peptide oligomers. Acta Neuropathol. Commun. 2018, 6, 131. [Google Scholar] [CrossRef]
- Torrisi, S.A.; Geraci, F.; Tropea, M.R.; Grasso, M.; Caruso, G.; Fidilio, A.; Musso, N.; Sanfilippo, G.; Tascedda, F.; Palmeri, A.; et al. Fluoxetine and Vortioxetine Reverse Depressive-Like Phenotype and Memory Deficits Induced by Abeta1–42 Oligomers in Mice: A Key Role of Transforming Growth Factor-beta1. Front. Pharmacol. 2019, 10, 693. [Google Scholar] [CrossRef]
- Fratiglioni, L.; Winblad, B.; von Strauss, E. Prevention of Alzheimer’s disease and dementia. Major findings from the Kungsholmen Project. Physiol. Behav. 2007, 92, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Launer, L.J.; Ross, G.W.; Petrovitch, H.; Masaki, K.; Foley, D.; White, L.R.; Havlik, R.J. Midlife blood pressure and dementia: The Honolulu-Asia aging study. Neurobiol. Aging 2000, 21, 49–55. [Google Scholar] [CrossRef]
- Hofman, A.; Ott, A.; Breteler, M.M.; Bots, M.L.; Slooter, A.J.; van Harskamp, F.; van Duijn, C.N.; Van Broeckhoven, C.; Grobbee, D.E. Atherosclerosis, apolipoprotein E, and prevalence of dementia and Alzheimer’s disease in the Rotterdam Study. Lancet 1997, 349, 151–154. [Google Scholar] [CrossRef]
- Haake, D.A.; Levett, P.N. Leptospirosis in humans. Curr. Top. Microbiol. Immunol. 2015, 387, 65–97. [Google Scholar] [PubMed]
- Taylor, A.J.; Paris, D.H.; Newton, P.N. A Systematic Review of the Mortality from Untreated Leptospirosis. PLoS Negl. Trop. Dis. 2015, 9, e0003866. [Google Scholar] [CrossRef] [PubMed]
- Limmathurotsakul, D.; Turner, E.L.; Wuthiekanun, V.; Thaipadungpanit, J.; Suputtamongkol, Y.; Chierakul, W.; Smythe, L.D.; Day, N.P.; Cooper, B.; Peacock, S.J. Fool’s gold: Why imperfect reference tests are undermining the evaluation of novel diagnostics: A reevaluation of 5 diagnostic tests for leptospirosis. Clin. Infect. Dis. 2012, 55, 322–331. [Google Scholar] [CrossRef]
- Reller, M.E.; Wunder, E.A., Jr.; Miles, J.J.; Flom, J.E.; Mayorga, O.; Woods, C.W.; Ko, A.I.; Dumler, J.S.; Matute, A.J. Unsuspected leptospirosis is a cause of acute febrile illness in Nicaragua. PLoS Negl. Trop. Dis. 2014, 8, e2941. [Google Scholar] [CrossRef] [PubMed]
- Monahan, A.M.; Miller, I.S.; Nally, J.E. Leptospirosis: Risks during recreational activities. J. Appl. Microbiol. 2009, 107, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Chiu, W.C.; Tsan, Y.T.; Tsai, S.L.; Chang, C.J.; Wang, J.D.; Chen, P.C.; Health Data Analysis in Taiwan (hDATa) Research Group. Hepatitis C viral infection and the risk of dementia. Eur. J. Neurol. 2014, 21, 1068-e59. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.S.; Yang, T.Y.; Shen, W.C.; Lin, C.L.; Lin, M.C.; Kao, C.H. Association between Helicobacter pylori infection and dementia. J. Clin. Neurosci. 2014, 21, 1355–1358. [Google Scholar] [CrossRef] [PubMed]
- Barnes, L.L.; Capuano, A.W.; Aiello, A.E.; Turner, A.D.; Yolken, R.H.; Torrey, E.F.; Bennett, D.A. Cytomegalovirus infection and risk of Alzheimer disease in older black and white individuals. J. Infect. Dis. 2015, 211, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Huang, W.S.; Muo, C.H.; Kao, C.H. Increased risk of dementia among chronic osteomyelitis patients. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Kao, L.T.; Sheu, J.J.; Lin, H.C.; Tsai, M.C.; Chung, S.D. Association between sepsis and dementia. J. Clin. Neurosci. 2015, 22, 1430–1433. [Google Scholar] [CrossRef] [PubMed]
- Miklossy, J. Alzheimer’s disease—A neurospirochetosis. Analysis of the evidence following Koch’s and Hill’s criteria. J. Neuroinflamm. 2011, 8, 90. [Google Scholar] [CrossRef] [PubMed]
- Itzhaki, R.F. Herpes simplex virus type 1 and Alzheimer’s disease: Increasing evidence for a major role of the virus. Front. Aging Neurosci. 2014, 6, 202. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, N.S.; Chung, C.H.; Lin, F.H.; Chiang, C.P.; Yeh, C.B.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Yeh, H.W.; et al. Anti-herpetic Medications and Reduced Risk of Dementia in Patients with Herpes Simplex Virus Infections—A Nationwide, Population-Based Cohort Study in Taiwan. Neurotherapeutics 2018, 15, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Jafarinejad, H.; Moghoofei, M.; Mostafaei, S.; Salimian, J.; Jamalkandi, S.A.; Ahmadi, A. Worldwide prevalence of viral infection in AECOPD patients: A meta-analysis. Microb. Pathog. 2017, 113, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Knapp, S. Diabetes and infection: Is there a link?—A mini-review. Gerontology 2013, 59, 99–104. [Google Scholar] [CrossRef]
- Liao, Y.T.; Hsieh, M.H.; Yang, Y.H.; Wang, Y.C.; Tsai, C.S.; Chen, V.C.; Gossop, M. Association between depression and enterovirus infection: A nationwide population-based cohort study. Medicine 2017, 96, e5983. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Leptospirosis (n = 3766) | Control (n = 15,064) | p-value | |
|---|---|---|---|---|
| Sex | ||||
| Female | 1185 (31.5) | 4740 (31.5) | 0.99 | |
| Male | 2581 (68.5) | 10,324 (68.5) | ||
| Age, mean | Mean (SD) | 52.4 (16.3) | 52.0 (16.5) | 0.20 |
| Age groups (years) | ≤49 | 1127 (45.2) | 6804 (45.2) | 0.99 |
| 50–64 | 1127 (29.9) | 4508 (29.9) | ||
| ≥65 | 938 (24.9) | 3752 (24.9) | ||
| Comorbidity | ||||
| Diabetes | 570 (15.1) | 827 (5.5) | <0.001 | |
| Hypertension | 824 (21.9) | 1444 (9.6) | <0.001 | |
| Head injury | 236 (6.3) | 503 (3.3) | <0.001 | |
| Depression | 70 (1.9) | 88 (0.6) | <0.001 | |
| Stroke | 301 (8.0) | 596 (4.0) | <0.001 | |
| COPD | 206 (5.5) | 393 (2.6) | <0.001 |
| Variable | Leptospirosis | Control | Crude HR* (95% CI) | Adjusted HR† (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| No. of dementia | PY | Rate# | No. of dementia | PY | Rate# | |||
| All | 27 | 13,989 | 1.93 | 65 | 64,400 | 1.01 | 1.91 (1.71, 2.13) | 1.89 (1.72, 2.08) |
| Sex | ||||||||
| Female | 12 | 4447 | 2.70 | 22 | 20,138 | 1.09 | 2.47 (2.06, 2.96) | 2.69 (2.29, 3.15) |
| Male | 15 | 9542 | 1.57 | 43 | 44,262 | 0.97 | 1.62 (1.41, 1.86) | 1.54 (1.36, 1.74) |
| Age (years) | ||||||||
| ≤65 | 3 | 11,074 | 0.27 | 5 | 48,961 | 0.10 | 2.65 (2.32, 3.03) | 1.53 (1.34, 1.73) |
| >65 | 24 | 2915 | 8.23 | 60 | 15,439 | 3.89 | 2.12 (1.74, 2.58) | 1.73 (1.42, 2.10) |
| Comorbidity‡ | ||||||||
| No | 4 | 9145 | 0.44 | 29 | 55,001 | 0.53 | 0.84 (0.29, 2.38) | 1.23 (1.06, 1.43) |
| Yes | 23 | 4844 | 4.75 | 36 | 9399 | 3.83 | 1.23 (0.73, 2.07) | 2.06 (1.70, 2.50) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-H.; Chen, P.-C.; Wang, Y.-C.; Lin, C.-L.; Lee, F.-Y.; Wu, C.-C.; Chang, K.-H. Risk of Dementia in Patients with Leptospirosis: A Nationwide Cohort Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3168. https://doi.org/10.3390/ijerph16173168
Chiu C-H, Chen P-C, Wang Y-C, Lin C-L, Lee F-Y, Wu C-C, Chang K-H. Risk of Dementia in Patients with Leptospirosis: A Nationwide Cohort Analysis. International Journal of Environmental Research and Public Health. 2019; 16(17):3168. https://doi.org/10.3390/ijerph16173168
Chicago/Turabian StyleChiu, Chun-Hsiang, Po-Chung Chen, Ying-Chuan Wang, Cheng-Li Lin, Feng-You Lee, Chia-Chang Wu, and Kuang-Hsi Chang. 2019. "Risk of Dementia in Patients with Leptospirosis: A Nationwide Cohort Analysis" International Journal of Environmental Research and Public Health 16, no. 17: 3168. https://doi.org/10.3390/ijerph16173168