Medical Students and Childhood Obesity: Health Disparity and Implication for Education


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data Collection
2.2.1. Perceived Importance of Different Roles in Reducing Childhood Obesity
2.2.2. Perceived Importance of Different Discussion Topics
2.2.3. Perceptions Related to Childhood Obesity
2.2.4. Health Disparity
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Perceptions Related to Childhood Obesity
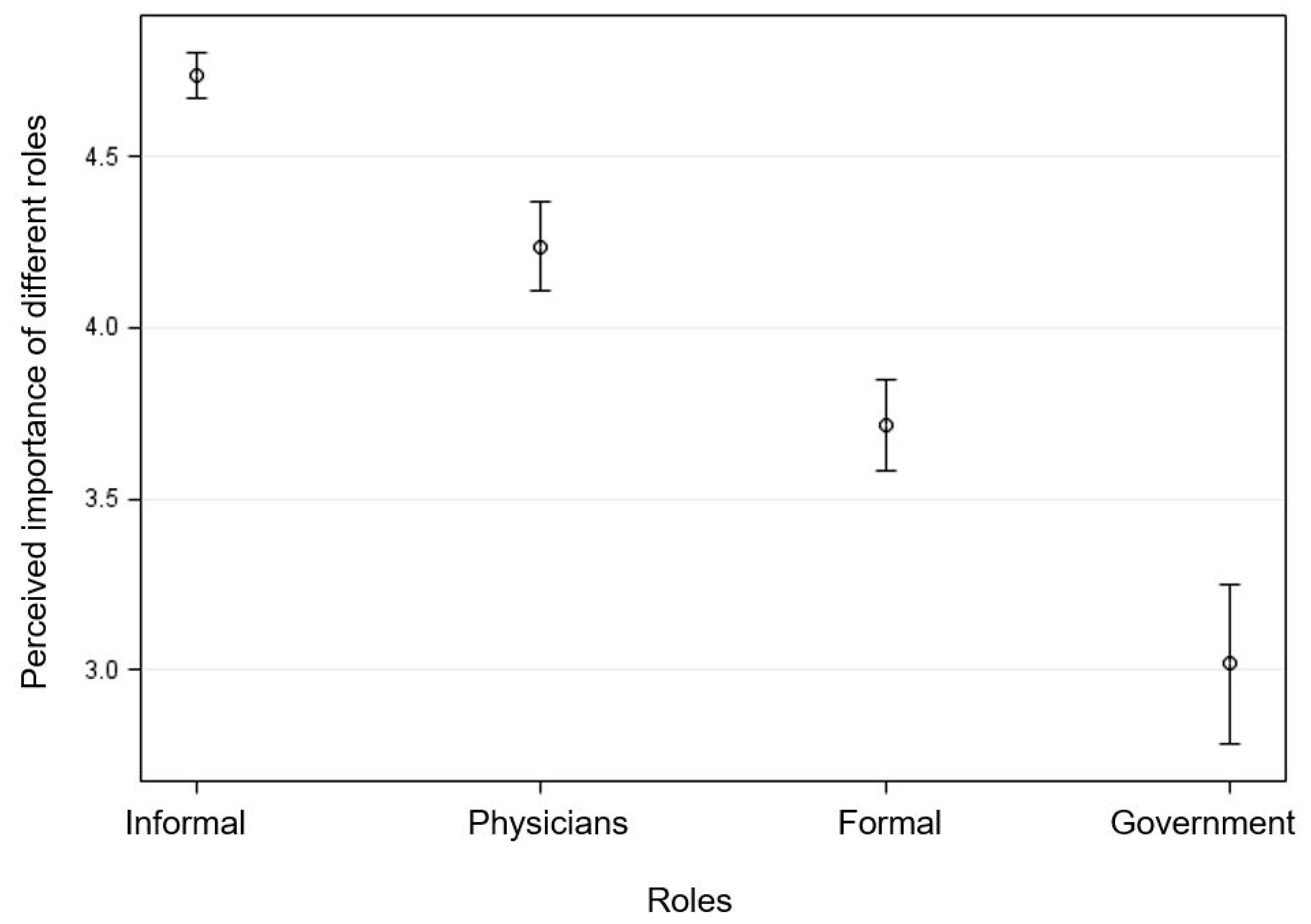
3.3. Perceived Importance of Different Roles in Reducing Childhood Obesity
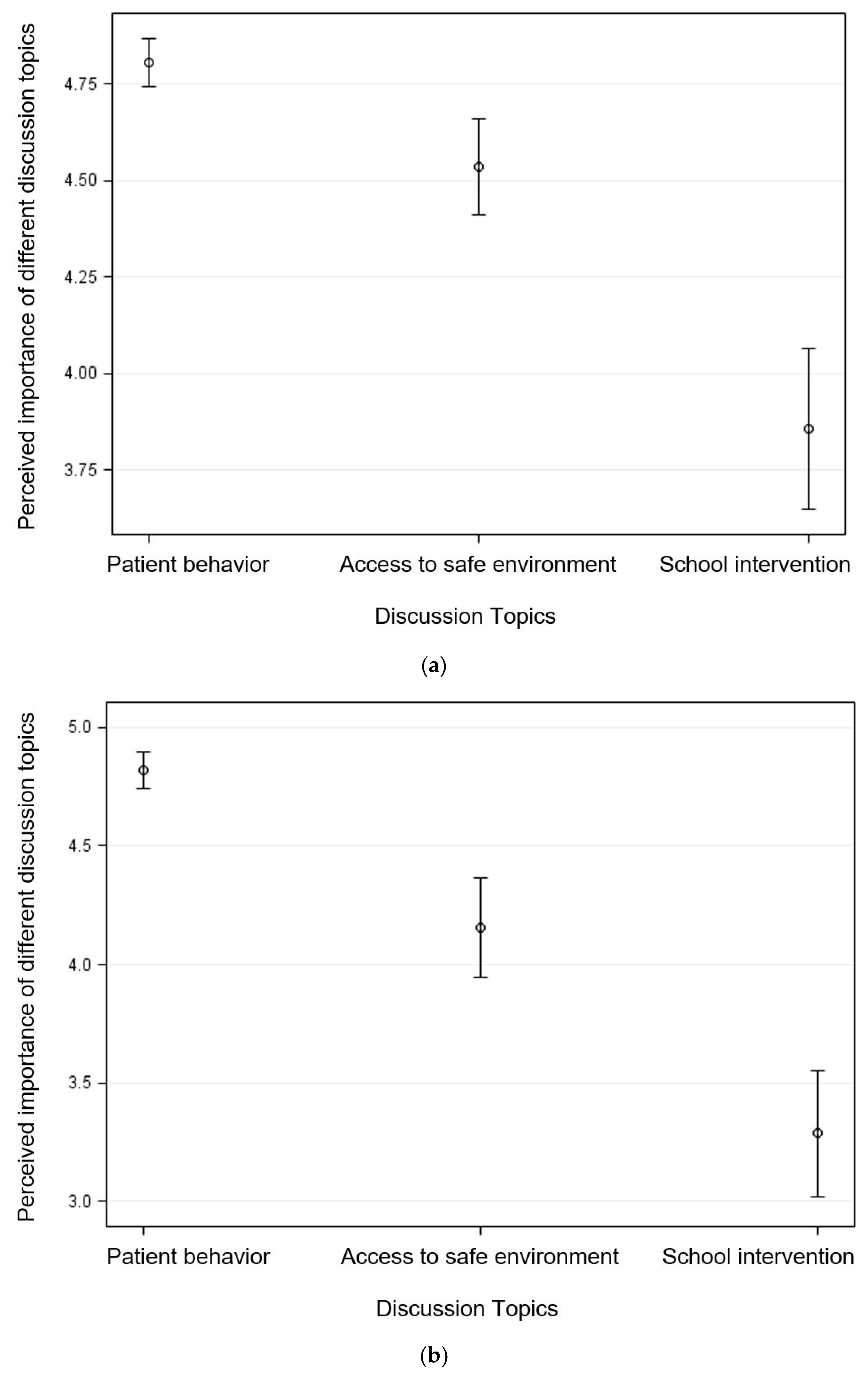
3.4. Perceived Importance of Discussing Different Topics with Child Patients and Their Parents
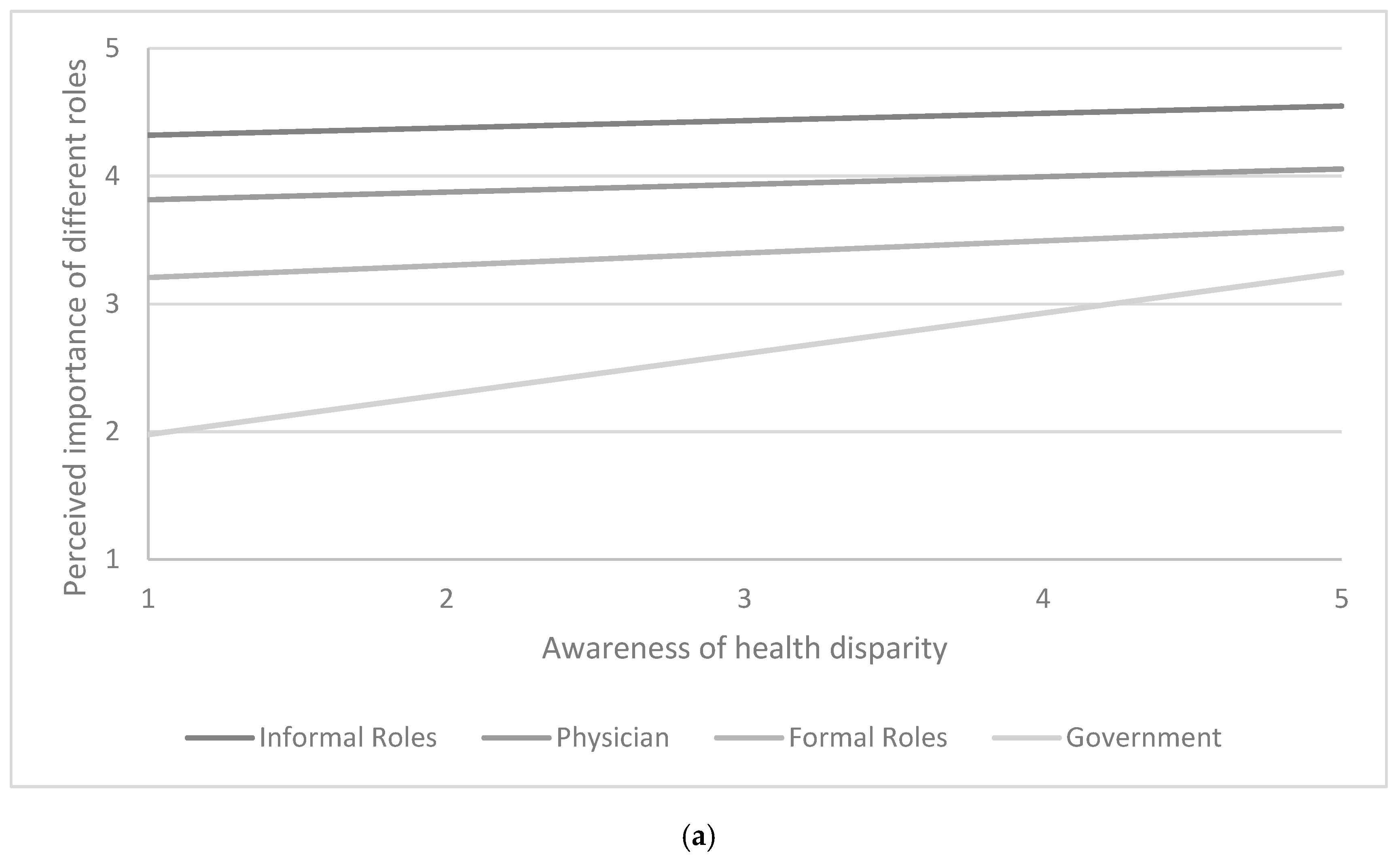
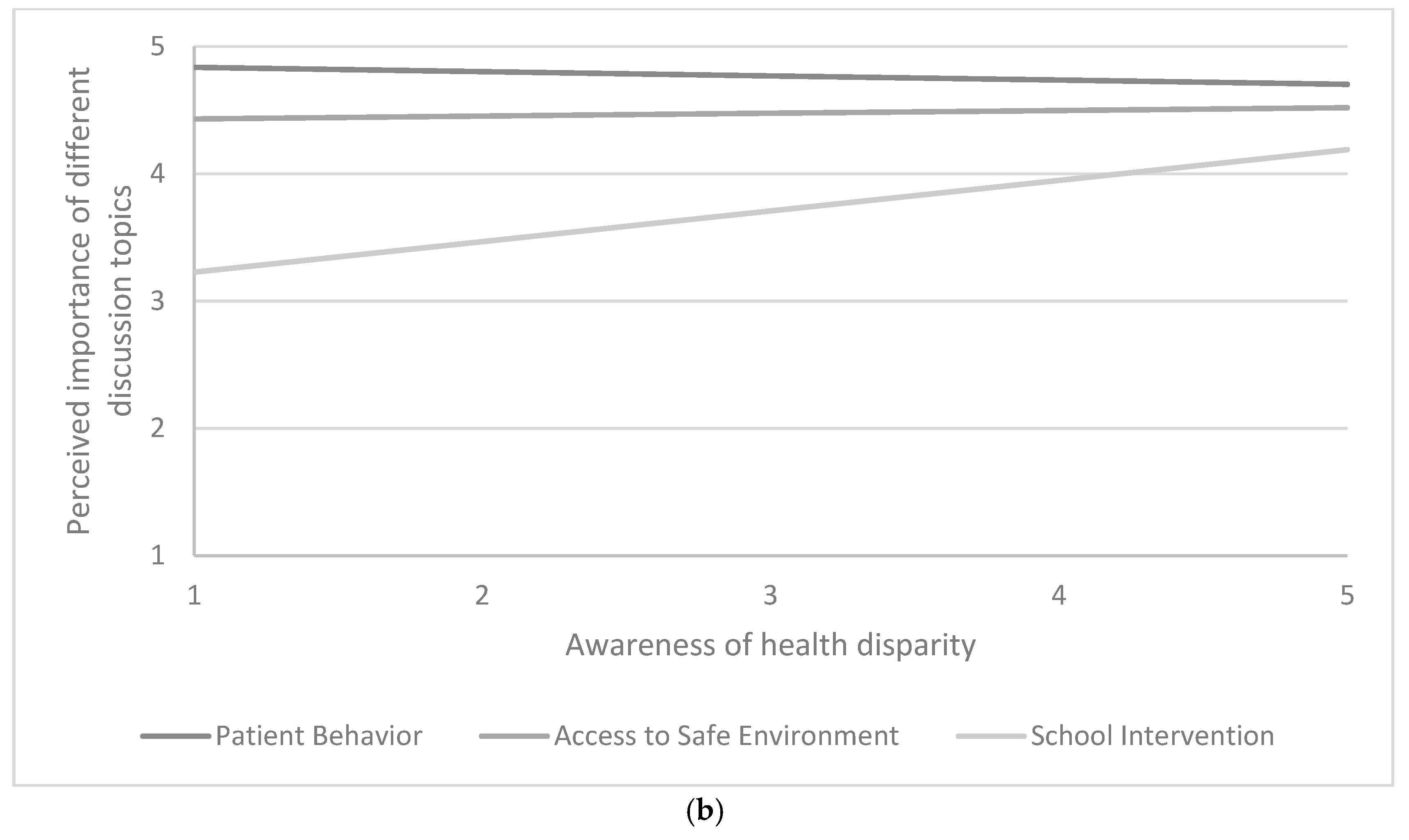
3.5. Association with Health Disparity Perception
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; NCHS Data Brief, no. 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017. Available online: https://www.cdc.gov/nchs/data/databriefs/db288.pdf (accessed on 5 November 2018).
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Committee on Nutrition. Prevention of pediatric overweight and obesity. Pediatrics 2003, 112, 424–430. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014; NCHS Data Brief, no. 219; National Center for Health Statistics: Hyattsville, MD, USA, 2015. Available online: https://www.cdc.gov/nchs/data/databriefs/db219.pdf (accessed on 5 November 2018).
- Skinner, A.C.; Skelton, J.A. Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014, 168, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Datar, A.; Chung, P.J. Changes in socioeconomic, racial/ethnic, and sex disparities in childhood obesity at school entry in the United States. JAMA Pediatr. 2015, 169, 696–697. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R.; Hassink, S.G.; Committee on Nutrition. The role of the pediatrician in primary prevention of obesity. Pediatrics 2015, 136, e275–e292. [Google Scholar] [CrossRef] [PubMed]
- Rodin, R.L.; Alexander, M.H.; Guillory, V.J.; Rogers, J. Physician counseling to prevent overweight in children and adolescents: American College of Preventive Medicine position statement. J. Public Health Manag. Pract. 2007, 13, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.M.; Gance-Cleveland, B.; Hassink, S.; Johnson, R.; Paradis, G.; Resnicow, K. Recommendations for prevention of childhood obesity. Pediatrics 2007, 120, s229–s253. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Gortmaker, S.L.; Hohman, K.H.; Horan, C.M.; Kleinman, K.P.; Mitchell, K.; Price, S.; Prosser, L.A.; Rifas-Shiman, S.L.; Gillman, M.W. A randomized controlled trial to improve primary care to prevent and manage childhood obesity: The High Five for Kids study. Arch. Pediatr. Adolesc. Med. 2011, 165, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.P.; Hamre, R.; Dietz, W.H.; Wasserman, R.C.; Slora, E.J.; Myers, E.F.; Sullivan, S.; Rockett, H.; Thoma, K.A.; Dumitru, G. Office-based motivational interviewing to prevent childhood obesity: A feasibility study. Arch. Pediatr. Adolesc. Med. 2007, 161, 495–501. [Google Scholar] [CrossRef]
- Peña, M.; Dixon, B.; Taveras, E.M. Are you talking to me? The importance of ethnicity and culture in childhood obesity prevention and management. Child. Obes. 2012, 8, 23–27. [Google Scholar] [CrossRef]
- Frintner, M.P.; Liebhart, J.L.; Lindros, J.; Baker, A.; Hassink, S.G. Are graduating pediatric residents prepared to engage in obesity prevention and treatment? Acad. Pediatr. 2016, 16, 394–400. [Google Scholar] [CrossRef]
- Cooke, N.K.; Ash, S.L.; Goodell, L.S. Medical students’ perceived educational needs to prevent and treat childhood obesity. Educ. Health 2017, 30, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Milford, E.; Morrison, K.; Teutsch, C.; Nelson, B.B.; Herman, A.; King, M.; Beucke, N. Out of the classroom and into the community: Medical students consolidate learning about health literacy through collaboration with Head Start. BMC Med. Educ. 2016, 16, 121. [Google Scholar] [CrossRef] [PubMed]
- Rosemond, T.N.; Blake, C.E.; Buff, S.M.; Blake, E.W.; Dunn, B.L.; Browne, T.; Bell, B.A.; Iachini, A.L. Sensitizing future health professionals to determinants of childhood obesity. Am. J. Prev. Med. 2016, 51, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Castillo, M.; Feinstein, R.; Tsang, J.; Fisher, M. Basic nutrition knowledge of recent medical graduates entering a pediatric residency program. Int. J. Adolesc. Med. Health 2016, 28, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Wolff, M.S.; Rhodes, E.T.; Ludwig, D.S. Training in childhood obesity management in the United States: A survey of pediatric, internal medicine-pediatrics and family medicine residency program directors. BMC Med. Educ. 2010, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F.; Butsch, W.S.; Kahan, S.; Machineni, S.; Cook, S.; Aronne, L.J. Obesity coverage on medical licensing examinations in the United States. What is being tested? Teach. Learn. Med. 2017, 29, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Heuer, C.A. The stigma of obesity: A review and update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef] [PubMed]
- Wear, D.; Aultman, J.M.; Varley, J.D.; Zarconi, J. Making fun of patients: Medical students’ perceptions and use of derogatory and cynical humor in clinical settings. Acad. Med. 2006, 81, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Luedicke, J.; Grilo, C.M. Obesity bias in training: Attitudes, beliefs, and observations among advanced trainees in professional health disciplines. Obesity 2014, 22, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Butland, B.; Jebb, S.; Kopelman, P.P.; McPherson, K.; Thomas, S.; Mardell, J.; Parry, V. Foresight. Tackling Obesities: Future Choices—Project Report; Department of Innovation, Universities and Skills: London, UK, 2007. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/287937/07-1184x-tackling-obesities-future-choices-report.pdf (accessed on 5 November 2018).
- Phelan, S.M.; Dovidio, J.F.; Puhl, R.M.; Burgess, D.J.; Nelson, D.B.; Yeazel, M.W.; Hardeman, R.; Perry, S.; van Ryn, M. Implicit and explicit weight bias in a national sample of 4,732 medical students: The medical student CHANGES study. Obesity 2014, 22, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Perman, J.A. Teaming up against childhood obesity. Bariatr. Nurs. Surg. Patient Care 2011, 6, 109–110. [Google Scholar] [CrossRef]
- More, F.G.; Sasson, L.M.; Godfrey, E.M.; Sehl, R.B. Collaboration between dietetics and dentistry: Dietetic internship in pediatric dentistry. Top. Clin. Nutr. 2005, 20, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, A.; Hart, J.; Mann, K.V.; Harkness, E.; Peters, S. Preparing medical students to facilitate lifestyle changes with obese patients: A systematic review of the literature. Acad. Med. 2012, 87, 912–923. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (95% CI 1) or Frequency (%) | p-Value 2 | ||
|---|---|---|---|---|
| Overall (n = 163) | Low Awareness of Health Disparity (n = 53) | High Awareness of Health Disparity (n = 78) | ||
| Age (years) | 25.57 (24.92, 26.22) | 26.33 (25.07, 27.59) | 25.02 (24.38, 25.65) | 0.047 * |
| Sex | ||||
| Male | 55 (43.3%) | 23 (45.1%) | 32 (42.1%) | 0.739 |
| Female | 72 (56.7%) | 28 (54.9%) | 44 (57.9%) | |
| Race | 0.012 * | |||
| White | 70 (55.6%) | 36 (70.6%) | 34 (45.3%) | |
| Asian | 33 (26.2%) | 7 (13.7%) | 26 (34.7%) | |
| Other Races | 23 (18.3%) | 8 (15.7%) | 15 (20.0%) | |
| Desired field of medicine | 0.576 | |||
| Primary care | 42 (25.8%) | 12 (22.6%) | 23 (29.5%) | |
| Specialty care | 77 (47.2%) | 27 (50.9%) | 33 (42.3%) | |
| Undecided | 44 (27.0%) | 14 (26.4%) | 22 (28.2%) | |
| Would like to work with patients under age 18 | 48 (29.4%) | 14 (26.4%) | 28 (35.9%) | 0.254 |
| Year in medical school | 0.685 | |||
| First Year | 35 (21.5%) | 10 (18.9%) | 20 (25.6%) | |
| Second Year | 73 (44.8%) | 25 (47.2%) | 34 (43.6%) | |
| Third Year | 27 (16.6%) | 9 (17.0%) | 9 (11.5%) | |
| Fourth Year | 28 (17.2%) | 9 (17.0%) | 15 (19.2%) | |
| Perceptions about | Mean (95% CI 1) or Frequency (%) | |||
|---|---|---|---|---|
| Overall (n = 163) | Low Awareness of Health disparity (n = 53) | High Awareness of Health Disparity (n = 78) | p-Value 2 | |
| Childhood obesity | ||||
| Reported that it would be likely to encounter childhood obesity in a routine medical visit | 133 (95.7%) | 49 (94.2%) | 74 (96.1%) | 0.620 |
| Reported that childhood obesity will affect more of the adolescent population | 138 (90.8%) | 49 (94.2%) | 69 (88.5%) | 0.266 |
| Agreed that childhood obesity is a family matter | 91 (68.4%) | 39 (75.0%) | 50 (64.1%) | 0.190 |
| Agreed that parents are primarily responsible for their child’s weight | 120 (90.2%) | 45 (86.5%) | 72 (92.3%) | 0.283 |
| Physicians in general | ||||
| Agreed that physicians are not trained to deal with childhood obesity | 45 (34.6%) | 25 (48.1%) | 20 (25.6%) | 0.008 * |
| Reported that physicians can be effective in childhood obesity | 90 (70.3%) | 34 (66.7%) | 56 (72.7%) | 0.463 |
| Participants as future physicians | ||||
| Prepared to treat childhood obesity | 60 (47.2%) | 29 (56.9%) | 31 (40.8%) | 0.075 |
| Would be effective in treating childhood obesity as a physician | 62 (48.8%) | 22 (43.1%) | 40 (52.6%) | 0.294 |
| Health Disparity (1–5, Higher score indicating greater agreement with the statements) | ||||
| Low-income American families lack resources to change health behaviors | 3.45 (3.29, 3.61) | 2.52 (2.37, 2.67) | 4.08 (3.97, 4.19) | <0.001 ** |
| Average Americans lack resources to change health behaviors | 2.09 (1.92, 2.25) | 1.59 (1.38, 1.79) | 2.41 (2.19, 2.63) | <0.001 ** |
| Variables | B 1 (SE 2) | ||
|---|---|---|---|
| Perceived Importance of Roles | Perceived Importance of Discussion Topics (Parents) | Perceived Importance of Discussion Topics (Child Patients) | |
| Intercept | 3.76 (0.34) ** | 4.87 (0.25) ** | 4.92 (0.31) ** |
| Roles | |||
| 1 Informal Roles | 0.51 (0.25) * | - | - |
| 2 Physicians (reference) | - | - | - |
| 3 Formal Roles | −0.65 (0.29) * | - | - |
| 4 Government | −2.09 (0.45) ** | - | - |
| Discussion Topics | |||
| 1 Patient Behavior (reference) | - | - | - |
| 2 Access to Safe Environment | - | −0.46 (0.19) * | −0.63 (0.36) |
| 3 School Intervention | - | −1.88 (0.39) ** | −1.83 (0.36) ** |
| Health Disparity Perception 3 | 0.06 (0.07) | −0.03 (0.03) | 0.004 (0.04) |
| Interaction terms | |||
| Health Disparity Perception x Role 1 | −0.003 (0.07) | - | - |
| Health Disparity Perception x Role 2 | - | - | - |
| Health Disparity Perception x Role 3 | 0.04 (0.08) | - | - |
| Health Disparity Perception x Role 4 | 0.26 (0.13) * | - | - |
| Interaction terms | |||
| Health Disparity Perception x Topic 1 | - | - | - |
| Health Disparity Perception x Topic 2 | - | 0.06 (0.05) | −0.01 (0.10) |
| Health Disparity Perception x Topic 3 | - | 0.27 (0.11) * | 0.09 (0.14) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Smith, M.L.; Kromann, L.; Ory, M.G. Medical Students and Childhood Obesity: Health Disparity and Implication for Education. Int. J. Environ. Res. Public Health 2019, 16, 2578. https://doi.org/10.3390/ijerph16142578
Lee S, Smith ML, Kromann L, Ory MG. Medical Students and Childhood Obesity: Health Disparity and Implication for Education. International Journal of Environmental Research and Public Health. 2019; 16(14):2578. https://doi.org/10.3390/ijerph16142578
Chicago/Turabian StyleLee, Shinduk, Matthew Lee Smith, Laura Kromann, and Marcia G. Ory. 2019. "Medical Students and Childhood Obesity: Health Disparity and Implication for Education" International Journal of Environmental Research and Public Health 16, no. 14: 2578. https://doi.org/10.3390/ijerph16142578