Using Gamification and Social Incentives to Increase Physical Activity and Related Social Cognition among Undergraduate Students in Shanghai, China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
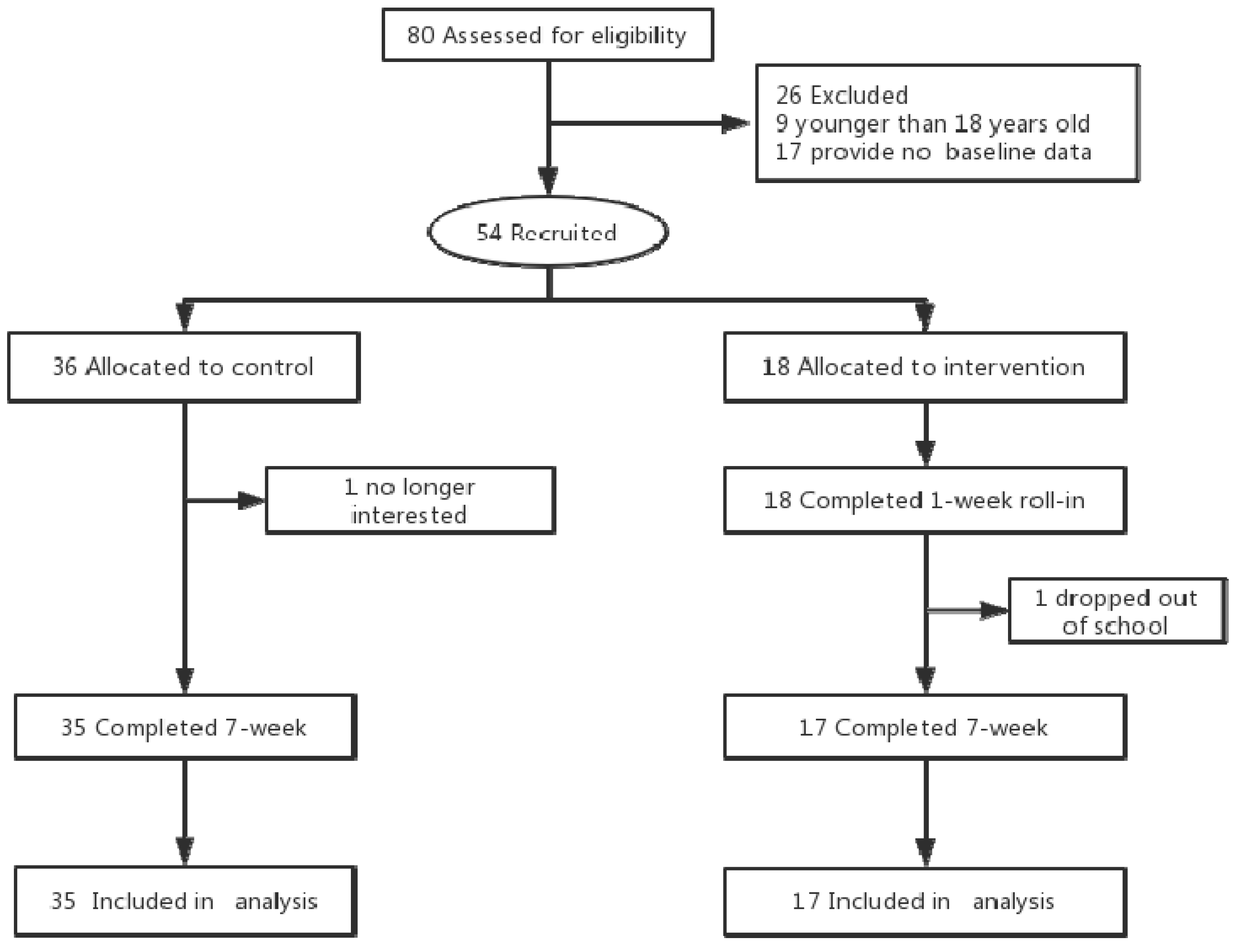
2.2. Recruitment and Participants
2.3. Power Analysis
2.4. Baseline Measures and Goal Setting
2.5. Intervention
2.5.1. Designs to Enhance Social Incentives
- Daily Report within Teams: The subjects were required to report their DPAD of the prior day and whether they had met their goals in their team WeChat group before 15:00 every day.
- Peer Support: Praising teammates who achieved their DPAD goals and encouraging those who did not within their team WeChat group every day were also required. Criticism and ridicule, which might cause negative reactions, were not allowed.
- Accountability: The leader of each team was endowed with the responsibility to remind their teammates and send peer support (PS) in the BIG INTERVENTION GROUP once all the teammates had reported and interacted before 15:00 every day.
- Team Punishment: The team that sent PS later than 15:00 the most times during the week would receive a punishment during the weekend.
- Team discussion: Educational materials about PA were posted by the investigators in each WeChat group on every Friday. The participants were guided to read it and discuss their gains, as well as the advantages and barriers of promoting PA within groups.
- Competition and Reward: A team competition was held to stimulate the subjects to engage in teamwork, and all the subjects acted as raters to ensure participation. The team that got the highest score was rewarded with a virtual certificate.
2.5.2. Designs to Enhance Gamification
- Points: Every team was endowed with 100 points for 1 week. Each day, if they failed to send PS before 15:00, 10 points were deducted. If any member was absent in the team discussion, 30 points were deducted. This design was based on the following three psychological principles: individuals tend to be more motivated by losses than gains [43], behavior is often better sustained by variable than by constant reinforcement [44], and individuals tend to be more motivated for aspirational behavior around temporal landmarks, such as the beginning of the week (the fresh start effect) [45].
- Ranking: The ranking by the final points of each team for every week was announced in the BIG INTERVENTION GROUP on every Sunday.
- Punishment: The team at the bottom of the ranking was required to perform a talent show in the BIG INTERVENTION GROUP (posting a voice message of a song or standup comedy or a video of a dance performance were all acceptable). Utilizing such performance as the mode of punishment could urge participants to follow the rules and avoid embarrassment, and it could also lighten up the atmosphere, thus improving compliance.
- Rewards: At the end of the intervention, each member of the team that accumulated the highest points was rewarded with a diploma and a small prize, such as a mug or a notebook.
2.6. Outcome Measures
2.6.1. Physical Activity (PA)
2.6.2. Daily Physical Activity Duration (DPAD)
2.6.3. Theory of Planned Behavior Constructs
- 7.
- Subjective norms were measured with 3 items (Cronbach alpha = 0.834), scored from 1 (extremely disagree) to 7 (extremely agree): (a) ‘‘Most people who are important to me approve of my DPAD goal”; (b). “Most people like me will meet my DPAD goal”; and (c). “Most people who are important to me think that I should try to meet my DPAD goal”.
- 8.
- Perceived behavior control was measured with 3 items (Cronbach alpha = 0.912), scored from 1 (extremely disagree) to 7 (extremely agree): (a) “I am confident that I can meet my DPAD Goal”; (b). “Whether or not I meet my DPAD Goal” is up to me; and (c). “I have the ability to meet my DPAD Goal”.
- 9.
- Intention was measured with 3 items (Cronbach alpha = 0.941), scored from 1 (extremely disagree) to 7 (extremely agree): (a) “I intend to meet my DPAD Goal”; (b). “I will make an effort to meet my DPAD Goal”; and (c). “I plan to meet my DPAD Goal”.
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Intervention Effects on the Baseline (T0) to Post-Test (T1) Changes in the TPB Constructs.
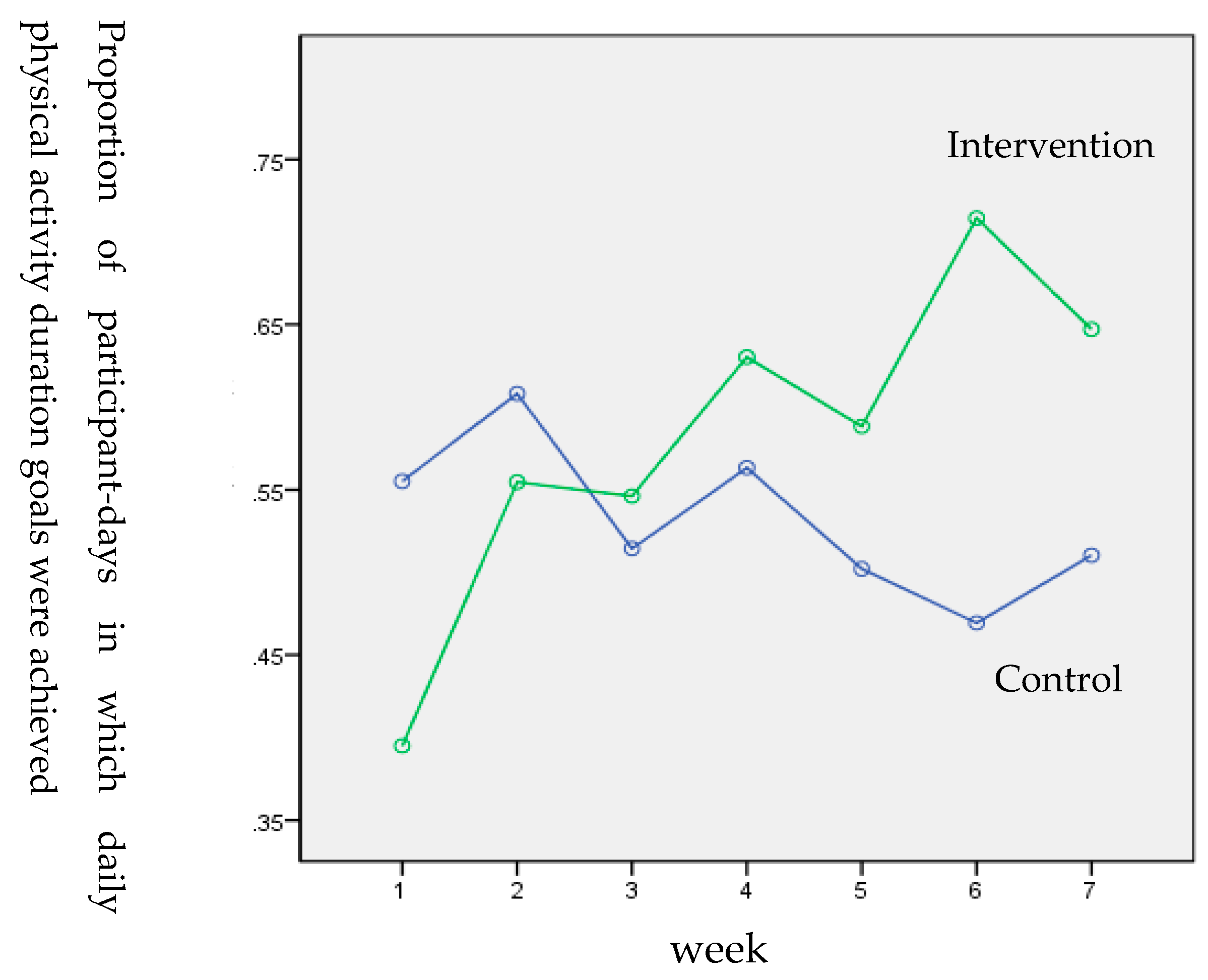
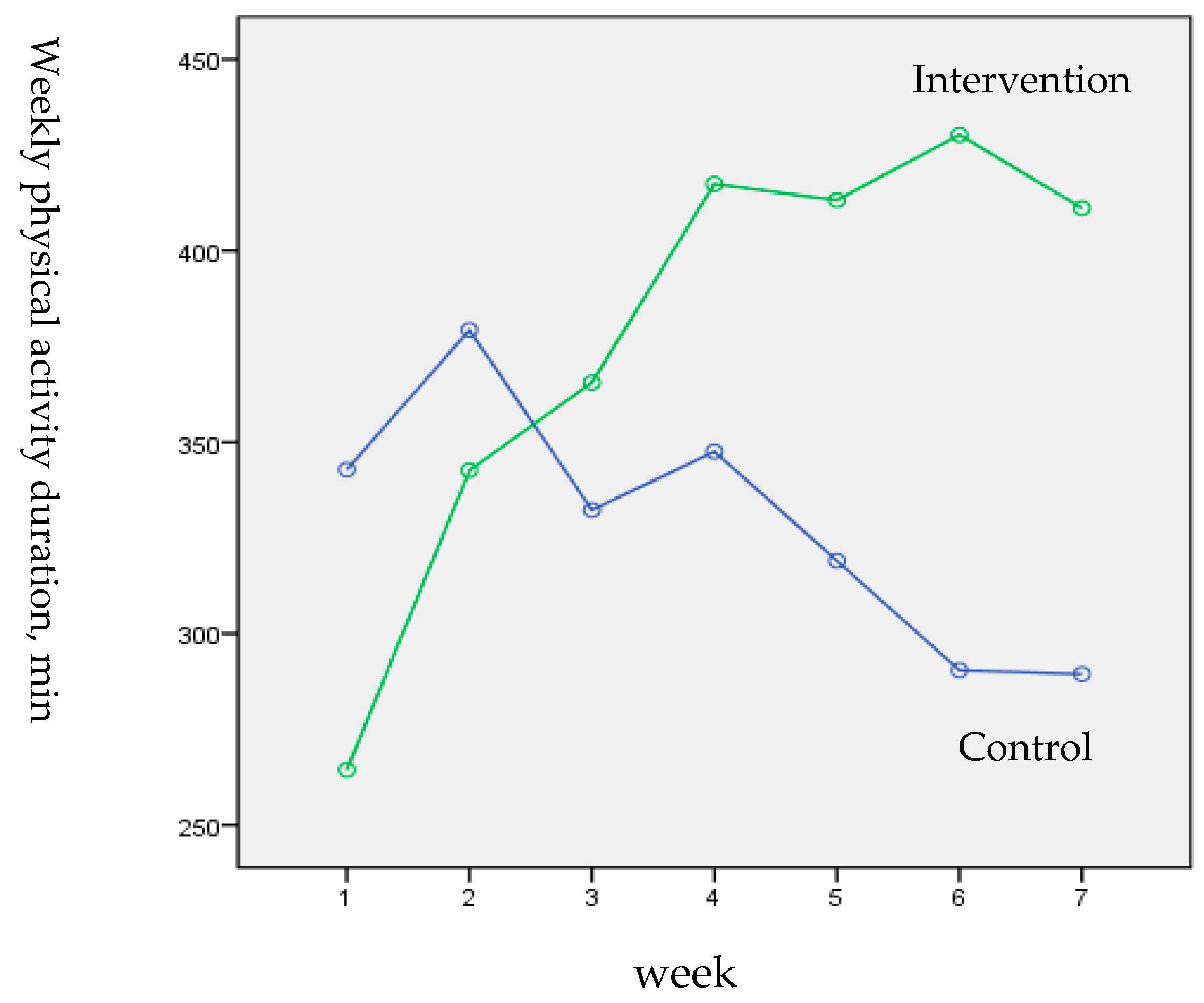
3.3. Intervention Effects on Baseline (T0) to Post-test (T1) Changes in Physical Activity Measures
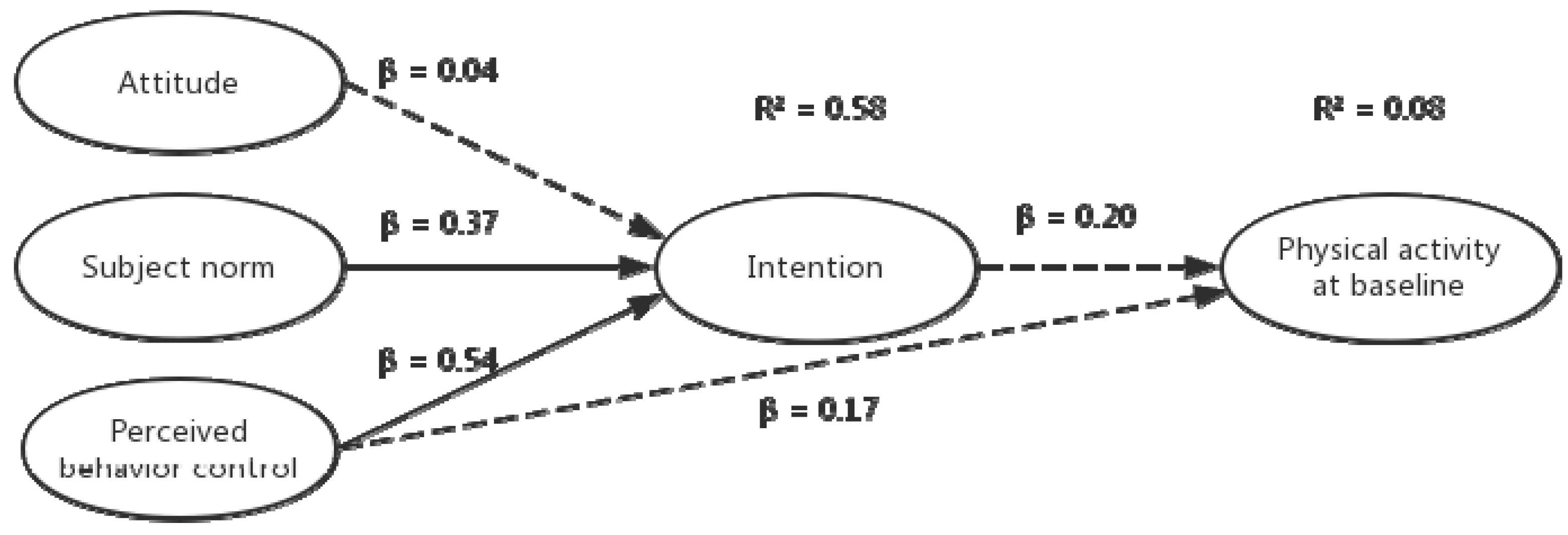
3.4. Prediction of PA by TPB Constructs
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kesaniemi, Y.K.; Danforth, E.J.; Jensen, M.D.; Kopelman, P.G.; Lefebvre, P.; Reeder, B.A. Dose-response issues concerning physical activity and health: An evidence-based symposium. Med. Sci. Sports Exerc. 2001, 33, S351–S358. [Google Scholar] [PubMed]
- Dankel, S.J.; Loenneke, J.P.; Loprinzi, P.D. Health Outcomes in Relation to Physical Activity Status, Overweight/Obesity, and History of Overweight/Obesity: A Review of the WATCH Paradigm. Sports Med. 2017, 47, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010; pp. 23–28. [Google Scholar]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.K.; Page, A.S.; Falconer, C.; Cooper, A.R. Longitudinal changes in sedentary time and physical activity during adolescence. Int. J. Behav. Nutr. Phys. 2015, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Keating, X.D.; Guan, J.; Piñero, J.C.; Bridges, D.M. A Meta-Analysis of College Students’ Physical Activity Behaviors. J. Am. Coll. Health 2005, 54, 116–126. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K.; Kassean, H.K.; Tsala Tsala, J.P.; Sychareun, V.; Müller-Riemenschneider, F. Physical inactivity and associated factors among university students in 23 low-, middle- and high-income countries. Int. J. Public Health 2015, 60, 539–549. [Google Scholar] [CrossRef]
- Zhang, X.; Song, Y.; Yang, T.B.; Zhang, B.; Dong, B.; Ma, J. Analysis of current situation of physical activity and influencing factors in Chinese primary and middle school students in 2010. Chin. J. Prev. Med. 2012, 46, 781–788. [Google Scholar]
- Wu, X.; Tao, S.; Zhang, Y.; Zhang, S.; Tao, F. Low Physical Activity and High Screen Time Can Increase the Risks of Mental Health Problems and Poor Sleep Quality among Chinese College Students. PLoS ONE 2015, 10, e119607. [Google Scholar] [CrossRef]
- Xu, X.; Pu, Y.; Sharma, M.; Rao, Y.; Cai, Y.; Zhao, Y. Predicting Physical Activity and Healthy Nutrition Behaviors Using Social Cognitive Theory: Cross-Sectional Survey among Undergraduate Students in Chongqing, China. Int. J. Environ. Res. Public Health 2017, 14, 1346. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.L.; Michie, S.; Dale, J.; Stallard, N.; French, D.P. The effects of a brief intervention to promote walking on Theory of Planned Behavior constructs: A cluster randomized controlled trial in general practice. Patient Educ. Couns. 2015, 98, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Gulley, T.; Boggs, D. Time Perspective and the Theory of Planned Behavior: Moderate Predictors of Physical Activity Among Central Appalachian Adolescents. J. Pediatr. Health Care 2014, 28, e41–e47. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Lubans, D.R.; Penfold, C.M.; Courneya, K.S. Testing the utility of three social-cognitive models for predicting objective and self-report physical activity in adults with type 2 diabetes. Br. J. Health Psychol. 2014, 19, 329–346. [Google Scholar] [CrossRef] [PubMed]
- Rebar, A.L.; Maher, J.P.; Doerksen, S.E.; Elavsky, S.; Conroy, D.E. Intention–behavior gap is wider for walking and moderate physical activity than for vigorous physical activity in university students. J. Sci. Med. Sport 2016, 19, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, Y. An extended version of the theory of planned behaviour: The role of self-efficacy and past behaviour in predicting the physical activity of Chinese adolescents. J. Sports Sci. 2016, 34, 587–597. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Darabi, F.; Kaveh, M.H.; Majlessi, F.; Khalaj Abadi Farahani, F.; Yaseri, M.; Shojaeizadeh, D. Effect of theory-based intervention to promote physical activity among adolescent girls: A randomized control trial. Electron. Physician 2017, 9, 4238–4247. [Google Scholar] [CrossRef]
- Jemmott, J.B.; Jemmott, L.S.; Ngwane, Z.; Zhang, J.; Heeren, G.A.; Icard, L.D.; O’Leary, A.; Mtose, X.; Teitelman, A.; Carty, C. Theory-based behavioral intervention increases self-reported physical activity in South African men: A cluster-randomized controlled trial. Prev. Med. 2014, 64, 114–120. [Google Scholar] [CrossRef] [Green Version]
- McIntosh, J.R.D.; Jay, S.; Hadden, N.; Whittaker, P.J. Do E-health interventions improve physical activity in young people: A systematic review. Public Health 2017, 148, 140–148. [Google Scholar] [CrossRef]
- Bright, P.; Hambly, K. Patients Using an Online Forum for Reporting Progress When Engaging With a Six-Week Exercise Program for Knee Conditioning: Feasibility Study. JMIR Rehabil. Assist. Technol. 2018, 5, e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, N.; Campo, S.; Yang, J.; Janz, K.F.; Snetselaar, L.G.; Eckler, P. Effects of Social Support About Physical Activity on Social Networking Sites: Applying the Theory of Planned Behavior. Health Commun. 2015, 30, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Kelders, S.M.; Sommers-Spijkerman, M.; Goldberg, J. Investigating the Direct Impact of a Gamified Versus Nongamified Well-Being Intervention: An Exploratory Experiment. J. Med. Internet Res. 2018, 20, e247. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, D.N.; Brown, J.D.; Tate, D.F.; Devellis, R.F.; Zimmer, C.; Ammerman, A.S. The Role of Companionship, Esteem, and Informational Support In Explaining Physical Activity Among Young Women In an Online Social Network Intervention. J. Behav. Med. 2014, 37, 955–966. [Google Scholar] [CrossRef]
- Miller, A.S.; Cafazzo, J.A.; Seto, E. A game plan: Gamification design principles in mHealth applications for chronic disease management. Health Inform. J. 2014, 22, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Menna, B.; Noelle, O.; Hugo, V.W.; Parisa, E.; Matt, J.; Ann, J. Gamification and Adherence to Web-Based Mental Health Interventions: A Systematic Review. JMIR Ment. Health 2016, 3, e39. [Google Scholar] [Green Version]
- Mohan, D.; Schell, J.; Angus, D.C. Not thinking clearly? Play a game, seriously! JAMA 2016, 316, 1867–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.S.; Benjamin, E.J.; Volpp, K.G.; Fox, C.S.; Small, D.S.; Massaro, J.M.; Lee, J.J.; Hilbert, V.; Valentino, M.; Taylor, D.H.; et al. Effect of a Game-Based Intervention Designed to Enhance Social Incentives to Increase Physical Activity Among Families. JAMA Intern. Med. 2017, 177, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.A. Beat the Street: A Pilot Evaluation of a Community-Wide Gamification-Based Physical Activity Intervention. Games Health J. 2018, 7, 208–212. [Google Scholar] [CrossRef]
- Corepal, R.; Best, P.; O’Neill, R.; Tully, M.A.; Edwards, M.; Jago, R.; Miller, S.J.; Kee, F.; Hunter, R.F. Exploring the use of a gamified intervention for encouraging physical activity in adolescents: A qualitative longitudinal study in Northern Ireland. BMJ Open 2018, 8, e19663. [Google Scholar]
- Sailer, M.; Hense, J.U.; Mayr, S.K.; Mandl, H. How gamification motivates: An experimental study of the effects of specific game design elements on psychological need satisfaction. Comput. Hum. Behav. 2017, 69, 371–380. [Google Scholar] [CrossRef]
- Asch, D.A.; Rosin, R. Engineering Social Incentives for Health. N. Engl. J. Med. 2016, 375, 2511–2513. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; Asch, D.A.; Rosin, R.; Small, D.S.; Bellamy, S.L.; Eberbach, K.; Walters, K.J.; Haff, N.; Lee, S.M.; Wesby, L. Individual Versus Team-Based Financial Incentives to Increase Physical Activity: A Randomized, Controlled Trial. J. Gen. Intern. Med. 2016, 31, 746–754. [Google Scholar] [CrossRef] [Green Version]
- Kurtzman, G.W.; Day, S.C.; Small, D.S.; Lynch, M.; Zhu, J.; Wang, W.; Rareshide, C.A.L.; Patel, M.S. Social Incentives and Gamification to Promote Weight Loss: The LOSE IT Randomized, Controlled Trial. J. Gen. Intern. Med. 2018, 33, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Lister, C.; West, J.H.; Cannon, B.; Sax, T.; Brodegard, D. Just a Fad? Gamification in Health and Fitness Apps. JMIR Serious Games 2014, 2, e9. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.A.; Lumsden, J.; Rivas, C.; Steed, L.; Edwards, L.A.; Thiyagarajan, A.; Sohanpal, R.; Caton, H.; Griffiths, C.J.; Munafò, M.R. Gamification for health promotion: Systematic review of behaviour change techniques in smartphone apps. BMJ Open 2016, 6, e12447. [Google Scholar] [CrossRef] [PubMed]
- Tencent Released Its Financial Report of the First Half Year in 2018. Available online: http://tech.qq.com/a/20180815/054575.htm (accessed on 15 August 2018).
- Rhodes, R.E.; Kaos, M.D.; Beauchamp, M.R.; Bursick, S.K.; Latimer-Cheung, A.E.; Hernandez, H.; Warburton, D.E.R.; Ye, Z.; Nicholas Graham, T.C. Effects of home-based exergaming on child social cognition and subsequent prediction of behavior. Scand. J. Med. Sci. Sports 2018, 28, 2234–2242. [Google Scholar] [CrossRef]
- Rogers, T.; Milkman, K.L.; Volpp, K.G. Commitment devices: Using initiatives to change behavior. JAMA 2014, 311, 2065–2066. [Google Scholar] [CrossRef]
- Ariely, D.; Wertenbroch, K. Procrastination, deadlines, and performance: Self-control by precommitment. Psychol. Sci. 2010, 13, 219–224. [Google Scholar] [CrossRef]
- Leinonen, A.M.; Pyky, R.; Ahola, R.; Kangas, M.; Siirtola, P.; Luoto, T.; Enwald, H.; Ikaheimo, T.M.; Roning, J.; Keinanen-Kiukaanniemi, S.; et al. Feasibility of Gamified Mobile Service Aimed at Physical Activation in Young Men: Population-Based Randomized Controlled Study (MOPO). JMIR mHealth uHealth 2017, 5, e146. [Google Scholar] [CrossRef] [Green Version]
- Divisón Garrote, J.A.; Escobar, C.C. Framing financial incentives to increase physical activity among overweight and obese adults. Ann. Intern. Med. 2016, 165, 385–394. [Google Scholar]
- Tina, W. The Behavior of Organisms: An Experimental Analysis; Appleton Century Crofts: New York, NJ, USA, 1938; Volume 186, pp. 43–50. [Google Scholar]
- Dai, H.; Milkman, K.L.; Riis, J. The Fresh Start Effect: Temporal Landmarks Motivate Aspirational Behavior. Soc. Sci. Electron. Publ. 2013, 60, 2563–2582. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajzen, I. From Intentions to Actions: A Theory of Planned Behavior; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Rubin, D.B. Multiple imputation for nonresponse in surveys. J. Mark. Res. 2009, 137, 180. [Google Scholar]
- Heeren, G.A.; Jemmott, J.B.; Marange, C.S.; Rumosa Gwaze, A.; Batidzirai, J.M.; Ngwane, Z.; Mandeya, A.; Tyler, J.C. Health-Promotion Intervention Increases Self-Reported Physical Activity in Sub-Saharan African University Students: A Randomized Controlled Pilot Study. Behav. Med. 2018, 44, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Lauer, E.E.; Jackson, A.W.; Martin, S.B.; Morrow, J.J.R. Meeting USDHHS Physical Activity Guidelines and Health Outcomes. Int. J. Exerc. Sci. 2017, 10, 121. [Google Scholar] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef]
- Nascimento-Ferreira, M.V.; Acf, D.M.; Toazza Oliveira, P.V.; Rendo-Urteaga, T.; Gracia-Marco, L.; Clm, F.; Moreno, L.A.; Carvalho, H.B. Assessment of physical activity intensity and duration in the paediatric population: Evidence to support an a priori hypothesis and sample size in the agreement between subjective and objective methods. Obes. Rev. 2018, 19, 810–824. [Google Scholar] [CrossRef]
- Weiss, T.W.; Slater, C.H.; Green, L.W.; Kennedy, V.C.; Albright, D.L.; Wun, C.C. The validity of single-item, self-assessment questions as measures of adult physical activity. J. Clin. Epidemiol. 1990, 43, 1123–1129. [Google Scholar] [CrossRef]
- Cavallo, D.N.; Tate, D.F.; Ward, D.S.; Devellis, R.F.; Thayer, L.M.; Ammerman, A.S. Social support for physical activity-role of Facebook with and without structured intervention. Transl. Behav. Med. 2014, 4, 346–354. [Google Scholar] [CrossRef]
- Epton, T.; Norman, P.; Dadzie, A.S.; Harris, P.R.; Webb, T.L.; Sheeran, P.; Julious, S.A.; Ciravegna, F.; Brennan, A.; Meier, P.S.; et al. A theory-based online health behaviour intervention for new university students (U@Uni): Results from a randomised controlled trial. BMC Public Health 2014, 14, 563. [Google Scholar] [CrossRef] [PubMed]
- Sriramatr, S.; Berry, T.; Spence, J. An internet-based intervention for promoting and maintaining physical activity in Thai university-aged females. J. Sci. Med. Sport 2014, 38, 430–439. [Google Scholar] [CrossRef]
- Clark, B.K.; Winkler, E.; Healy, G.N.; Gardiner, P.G.; Dunstan, D.W.; Owen, N.; Reeves, M.M. Adults’ Past-Day Recall of Sedentary Time. Med. Sci. Sports Exerc. 2013, 45, 1198–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, B.K.; Pavey, T.G.; Lim, R.F.; Gomersall, S.R.; Brown, W.J. Past-day recall of sedentary time: Validity of a self-reported measure of sedentary time in a university population. J. Sci. Med. Sport 2016, 19, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Milton, K.; Bull, F.C.; Bauman, A. Reliability and validity testing of a single-item physical activity measure. Brit. J. Sport Med. 2011, 45, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.M.; Mailing, L.J.; Niemiro, G.M.; Moore, R.; Cook, M.D.; White, B.A.; Holscher, H.D.; Woods, J.A. Exercise Alters Gut Microbiota Composition and Function in Lean and Obese Humans. Med. Sci. Sports Exerc. 2018, 50, 747–757. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Weekly PA Duration (min) | Percentage of Goal Greater than the Baseline |
|---|---|
| 150~ | 0~10% |
| 120~149 | 10~20% |
| 90~119 | 20~30% |
| 60~79 | 30~40% |
| 30~59 | 40~60% |
| ~30 | 60~80% |
| Variable | Intervention Group (n = 17) | Control Group (n = 35) | p |
|---|---|---|---|
| Demographics | |||
| Age, mean (SD), y | 20.76 (1.97) | 20.74 (2.33) | 0.958 |
| Female, No. (%) | 9 (52.94) | 18 (51.43) | 0.768 |
| Baseline Measures | |||
| BMI, mean (SD), kg/m2 | 21.71 (2.50) | 21.36 (2.63) | 0.649 |
| Physical Activity Measures | |||
| DPAD, mean (SD), min | 36.39 (27.26) | 48.98 (22.10) | 0.760 |
| DPAD increase from the baseline to the goal, mean (SD), min | 25.86 (11.37) | 30.59 (14.29) | 0.823 |
| days doing VPA per week, mean (SD), d | 2.24 (1.35) | 2.94 (1.63) | 0.118 |
| VPA time per day, mean (SD), min | 26.18 (14.42) | 26.57 (15.38) | 0.784 |
| VPA time per week, mean (SD), min | 72.65 (50.93) | 89.71 (64.99) | 0.549 |
| days doing MPA per week, mean (SD), d | 2.88 (1.45) | 3.03 (2.15) | 0.890 |
| MPA time per day, mean (SD), min | 31.47 (18.61) | 31.71 (19.78) | 0.676 |
| MPA time per week, mean (SD), min | 87.35 (50.50) | 113.71 (105.04) | 0.821 |
| Days Walking>10min per week, mean (SD), d | 6.53 (0.72) | 5.94 (1.21) | 0.113 |
| Walk time per day, mean (SD), min | 47.94 (28.23) | 43.14 (37.26) | 0.192 |
| Walk time per week, mean (SD), min | 306.18 (181.52) | 267.71 (259.72) | 0.050 |
| Sitting time per week, mean (SD), min | 3306.47 (590.62) | 3455.80 (870.82) | 0.553 |
| Physical activity total score, mean (SD) | 1940.97 (813.28) | 2056.03(1323.26) | 0.585 |
| TPB Construct Measures | |||
| Attitude, mean (SD) | 5.51 (1.28) | 5.53 (0.99) | 0.969 |
| Subjective norms, mean (SD) | 5.27 (1.09) | 5.58 (1.02) | 0.346 |
| Perceived behavioral control, mean (SD) | 5.97 (0.96) | 5.98 (1.06) | 0.921 |
| Intention, mean (SD) | 5.65 (0.89) | 5.99 (1.19) | 0.129 |
| Variable | Intervention group (N = 17) | Control group (N =3 5) | P |
|---|---|---|---|
| Attitude, mean (SD) | 0.55 (1.11) | −0.13 (1.08) | 0.023 |
| Subjective norms, mean (SD) | 0.82 (1.13) | −0.17 (1.23) | 0.006 |
| Perceived behavioral control, mean (SD) | 0.28 (0.90) | −0.35 (0.97) | 0.011 |
| Intention, mean (SD) | 0.80 (0.83) | −0.40 (1.23) | 0.000 |
| Variable | Intervention Group (n = 17) | Control Group (n = 35) | p |
|---|---|---|---|
| days doing VPA per week, mean (SD), d | 2.29 (1.11) | 0.66 (1.80) | 0.000 |
| VPA time per day, mean (SD), min | 12.94 (13.92) | 2.71 (12.14) | 0.019 |
| VPA time per week, mean (SD), min | 105.59 (77.43) | 18.14 (56.10) | 0.000 |
| days doing MPA per week, mean (SD), d | 1.41 (1.27) | 0.09 (1.82) | 0.012 |
| MPA time per day, mean (SD), min | 13.24 (22.63) | −2.14 (16.51) | 0.013 |
| MPA time per week, mean (SD), min | 101.47 (75.74) | −3.57 (72.28) | 0.000 |
| Days Walking>10 min per week, mean (SD), d | 0.47 (0.71) | 0.91 (1.22) | 0.256 |
| Walk time per day, mean (SD), min | 6.47 (20.37) | 7.00 (34.30) | 0.735 |
| Walk time per week, mean (SD), min | 74.71 (124.09) | 70.00 (225.87) | 0.937 |
| Sitting time per week, mean (SD), min | −420.00 (410.41) | 0.20 (544.05) | 0.005 |
| Physical activity total score, mean (SD) | 1497.12 (640.62) | 361.86 (974.64) | 0.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mo, D.; Xiang, M.; Luo, M.; Dong, Y.; Fang, Y.; Zhang, S.; Zhang, Z.; Liang, H. Using Gamification and Social Incentives to Increase Physical Activity and Related Social Cognition among Undergraduate Students in Shanghai, China. Int. J. Environ. Res. Public Health 2019, 16, 858. https://doi.org/10.3390/ijerph16050858
Mo D, Xiang M, Luo M, Dong Y, Fang Y, Zhang S, Zhang Z, Liang H. Using Gamification and Social Incentives to Increase Physical Activity and Related Social Cognition among Undergraduate Students in Shanghai, China. International Journal of Environmental Research and Public Health. 2019; 16(5):858. https://doi.org/10.3390/ijerph16050858
Chicago/Turabian StyleMo, Dandan, Mi Xiang, Mengyun Luo, Yuanyuan Dong, Yue Fang, Shunxing Zhang, Zhiruo Zhang, and Huigang Liang. 2019. "Using Gamification and Social Incentives to Increase Physical Activity and Related Social Cognition among Undergraduate Students in Shanghai, China" International Journal of Environmental Research and Public Health 16, no. 5: 858. https://doi.org/10.3390/ijerph16050858