Effects of Extreme Temperatures on Mortality and Hospitalization in Ho Chi Minh City, Vietnam

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Source and Quality
2.3. Definition of a Heat Wave
2.4. Statistical Model
Log (Yt) = α + β1 * Tt,l + β2 * HW + β3 * DOW + β4 * NCS (Time, 7 df/year)
3. Results
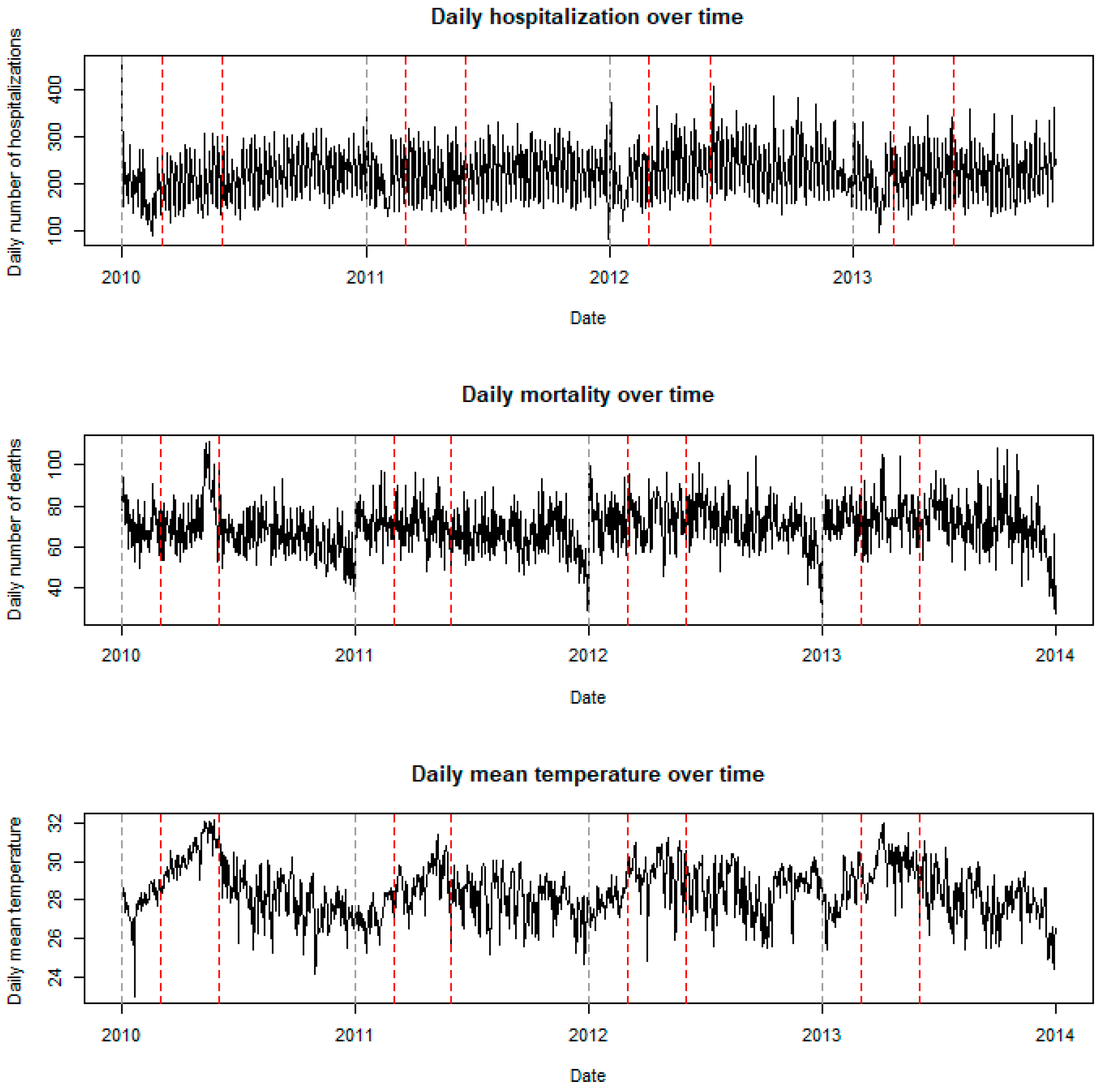
3.1. Descriptive Statistics
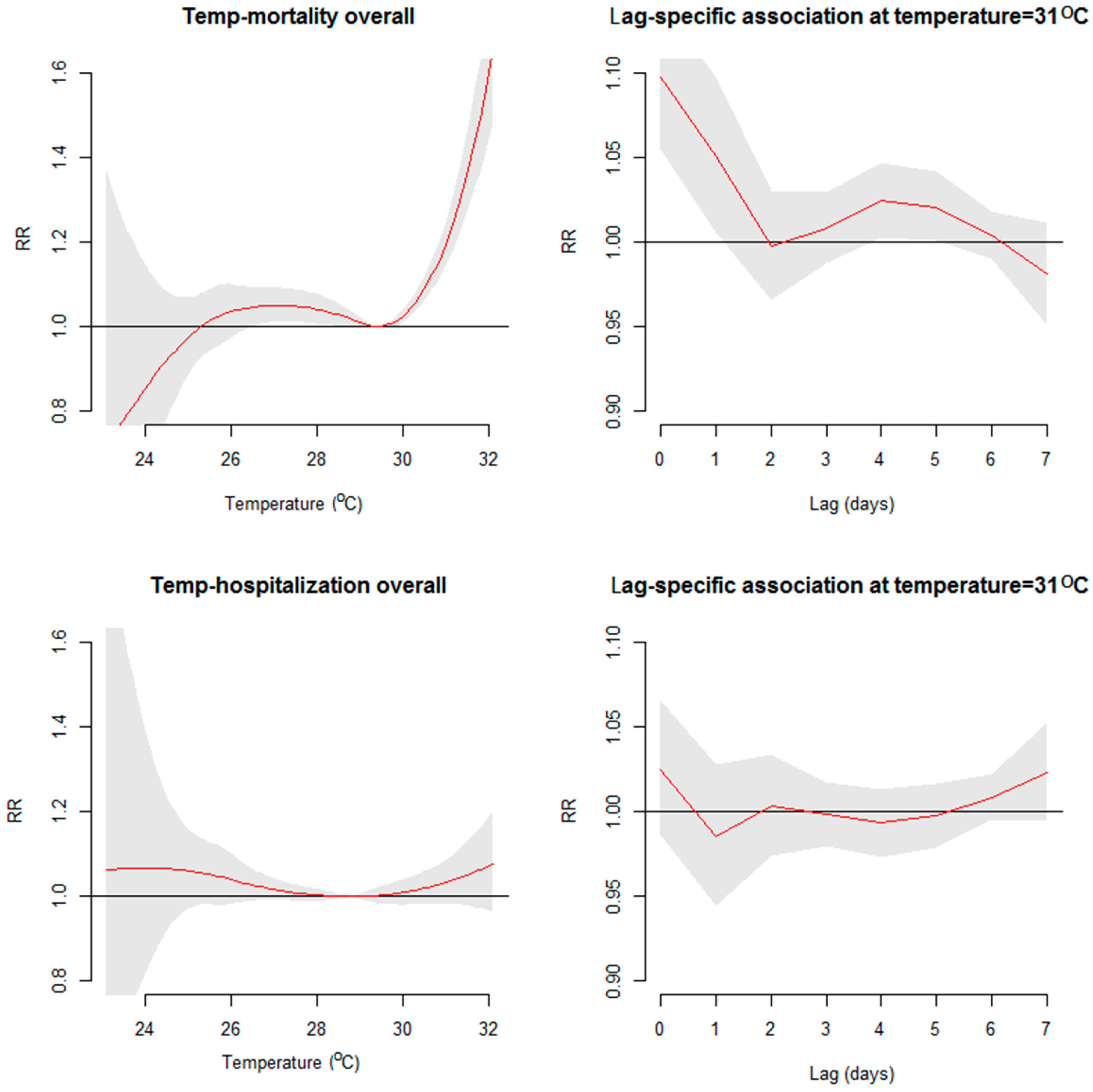
3.2. The Short-Term Relationship between Temperature and Health Outcomes
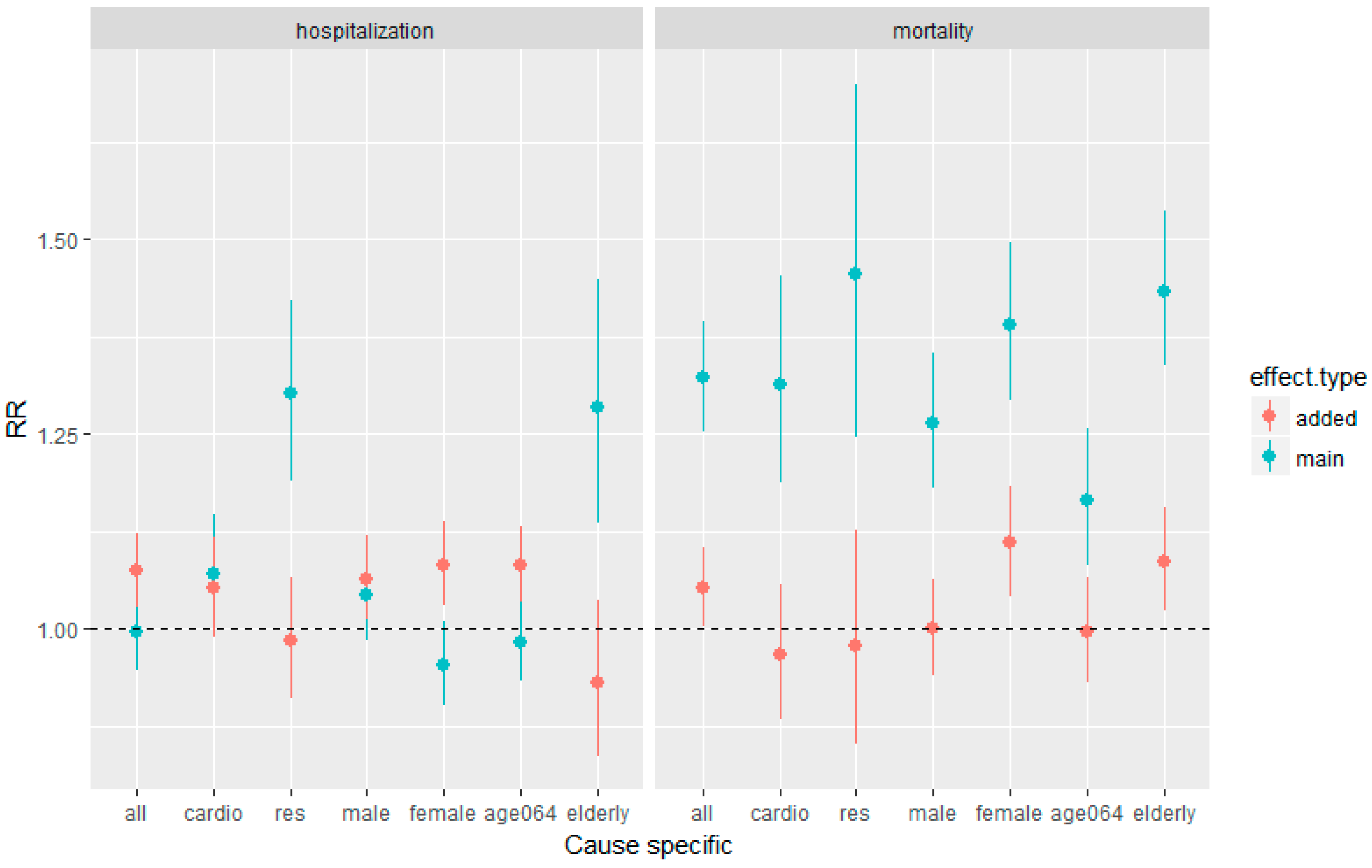
3.3. Comparability of the Temperature Effects on Mortality and Hospitalization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barros, V.R.; Field, C.B.; Dokken, K.J.; March, M.D.; Mastrandrea, T.E.; Bilir, M.; Chatterjee, K.L.; Ebi, Y.O.; Estrada, J.C.; et al. Climate Change 2014: Impacts, Adaptation and Vulnerablity. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Hondula, D.M.; Barnett, A.G. Heat-related morbidity in Brisbane, Australia: spatial variation and area-level predictors. Environ. Health Perspect. 2014, 122, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; Accetta, G.; Desario, M.; D’Ipolliti, A.; Marino, C.; Baccini, M.; Biggeri, A.; Anderson, H.R.; Katsouyanni, K.; Ballester, F.; et al. High temperature and hospitalizations for cardiovascular and respiratory causes in 12 European cities. Am. J. Respir. Crit. Care Med. 2009, 179, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Phung, D.; Guo, Y.; Thai, P.; Rutherford, S.; Wang, X.; Nguyen, M.; Do, C.M.; Nguyen, N.H.; Alam, N.; Chu, C. The effects of high temperature on cardiovascular admissions in the most populous tropical city in Vietnam. Environ. Pollut. 2015, 208, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Amstrong, B.; Li, S.; Tawatsupa, B.; Tobias, A.; Laviqne, E.; Coelho, M.d.Z.S.; Leone, M.; Pan, X.; et al. Global variation in the effects of ambient temperature on mortality: A systematic evaluation. Epidemiology 2014, 25, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Laviqne, E.; Anobetti, A.; Swartz, J.; Tobias, A.; Tong, S.; Rocklov, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambian temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Huang, C.; Barnett, A.G.; Wang, X.; Tong, S. Effects of extreme temperatures on years of life lost for cardiovascular deaths: A time-series study in Brisbane, Australia. Circulation 2012, 5, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, L.; Wang, J.; Huang, J.; Lu, S. Cardiovascular mortality associated with low and high temperatures: Determinants of inter-region vulnerability in China. Int. J. Environ. Res. Public Health 2015, 12, 5918–5933. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Hansen, A.; Liu, Q.; Liu, X.; Tong, M.X.; Sun, Y.; Cameron, S.; Hanson-Easay, S.; Han, G.S.; Williams, C.; et al. Association between dengue fever incidence and meteorological factors in Guangzhou, China, 2005–2014. Environ. Res. 2017, 153, 17–26. [Google Scholar] [CrossRef]
- Phung, D.; Huang, C.; Rutherford, S.; Chu, C.; Wang, X.; Nguyen, M.; Nguyen, N.H.; Manh, C.D.; Nguyen, T.H. Association between climate factors and diarrhoea in a Mekong Delta area. Int. J. Biometeorol. 2015, 59, 1321–1331. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Chu, C.; Nguyen, H.L.; Nguyen, H.T.; Manh, C.D.; Rutherford, S.; Phung, D. Temporal and spatial analysis of hand, foot, and mouth disease in relation to climate factors: A study in the Mekong Delta region. Vietnam. Sci. Total Environ. 2017, 581, 766–772. [Google Scholar] [CrossRef]
- Milazzo, A.; Giles, L.C.; Zhang, Y.; Koehler, A.P.; Hiller, J.E.; Bi, P. The effect of temperature on different Salmonella serotypes during warm seasons in a Mediterranean climate city, Adelaide, Australia. Epidemiol. Infect. 2016, 144, 1231–1240. [Google Scholar] [CrossRef]
- Yang, D.; Xu, C.; Wang, J.; Zhao, Y. Spatiotemporal epidemic characteristics and risk factor analysis of malaria n Yunnan Province, China. BMC Public Health 2017, 17, 66. [Google Scholar] [CrossRef] [PubMed]
- Ebi, K.L.; Exuzides, K.A.; Lau, E.; Kelsh, M.; Barnston, A. Weather changes associated with hospitalizations for cardiovascular diseases and stroke in California, 1983–1998. Int. J. Biometeorol. 2004, 49, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Samet, J.M.; Patz, J.A. Hospital admission for heart disease: The effects of temperature and humidity. Epidemiology 2004, 15, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Bayentin, L.; Adlouni, S.E.; Ouarda, T.B.; Gosselin, P.; Doyon, B.; Chebana, F. Spatial variability of climate effects on ischemic heart disease hospitalization rates for the period 1989–2006 in Quebec, Canada. Int. J. Health Geogr. 2010, 9, 5. [Google Scholar] [CrossRef]
- Turner, L.R.; Barnett, A.G.; Connell, D.; Tong, S. Ambient temperature and cardiorespiratory morbidity: A systematic review and meta-analysis. Epidemiology 2012, 23, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Phung, D.; Guo, Y.; Nguyen, H.T.L.; Rutherford, S.; Baum, S.; Chu, C. High temperature and risk of hospitalizations, and effect modifying potential of socio-economic conditions: A multi-province study in the tropical Mekong Delta Region. Environ. Int. 2016, 92, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Konken, P.J.; Piver, W.T.; Ye, F.; Elixhauser, A.; Olsen, L.M.; Portier, C.J. Temperature, air pollution, and hospitalization for cardiovascular diseases among elderly people in Denver. Environ. Health Perspect. 2003, 111, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Luo, M.; Walker, R.J.; Liu, X.; Hwang, S.A.; Chinery, R. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diaseas. Epidemiology 2009, 20, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Kovats, R.S.; Edwards, S.J.; Hajat, S.; Armstrong, B.G.; Ebi, K.L.; Menne, B.; Grp, C. The effect of temperature on food poisoning: A time-series analysis of salmonellosis in ten European countries. Epidemiol. Infect. 2004, 132, 443–453. [Google Scholar] [CrossRef]
- Linares, C.; Diaz, J. Impacts of high temperature on hospital admissions: Comparative analysis with previous studies about mortality (Madrid). Eur. J. Public Health 2008, 18, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Gronlund, C.J.; Zanobetti, A.; Schwartz, J.D.; Wellenius, G.A.; O’Neill, M.S. Heat, heat waves, and hospital admissions among the elderly in the United States, 1992–2006. Environ. Health Perspect. 2014, 122, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, G.; Hajat, S.; Fadda, E.; Buja, A.; Fedeli, U.; Spolaore, P. Contrasting patterns of hospital admissions and mortality during heat waves: Are deaths from circulatory disease a real excess or an artifact? Med. Hypotheses 2006, 66, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Hosking, J.; Jones, R.; Percival, T.; Turner, N.; Ameratunga, S. Climate change: The implications for children health in Australasia. J. Paediatr. Child Health 2010, 47, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Viet Nam: Ha Noi and Ho Chi Minh City Power Grid Development Sector Project. Available online: https://www.adb.org/sites/default/files/linked-documents/46391-001-ieeab-04.pdf (accessed on 1 November 2018).
- Guo, Y.; Li, S.; Chen, D.; Williams, G.; Tong, S. Projecting future temperature-related mortality in three largest Australian cities. Environ. Pollut. 2016, 208, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Dang, T.N.; Seposo, X.T.; Duc, N.H.C.; Thang, T.B.; An, D.D.; Hang, L.T.M.; Long, T.T.; Loan, B.T.H.; Honda, Y. Characterizing the relationship between temperature and mortality in tropical and subtropical cities: A distributed lag non-linear model analysis in Hue, Viet Nam, 2009–2013. Glob. Health Act. 2016, 9, 28738. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.R.; Ngoan, L.T.; Hung, D.V.; Huong Tu, N.T.; Mai, A.L.; Ivers, R.Q.; Huong, H.T. Evaluation of the Vietnamese A6 mortality reporting system: Injury as a cause of death. Inj. Prev. 2012, 18, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Hung, D.V.; Hoang, T.H.; Mai Anh, L.; Tu Nguyen, T.H.; Le Tran, N. Evaluation of the Vietnamese A6 Mortality Reporting System: All-Cause Mortality. Asia Pac. J. Public Health 2015, 27, 733–742. [Google Scholar] [CrossRef]
- The National Oceanic and Atmospheric Administration’s National Climate Data Center. Global Summary of the Day. 2015. Available online: http://www.ncdc.noaa.gov/ (accessed on 1 January 2015).
- Tong, S.; FitzGerald, G.; Wang, X.Y.; Aitken, P.; Tippett, V.; Chen, D.; Wang, X.; Guo, Y. Exploration of the health risk-based definition for heatwave: A. multi-city study. Environ. Res. 2015, 142, 696–702. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Cheng, J.; Hu, W.; Tong, S. Heatwave and health events: A systematic evaluation of different temperature indicators, heatwave intensities and durations. Sci. Total Environ. 2018, 630, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.K.; Ho, T.J.; Wang, Y.C. Mortality risk associated with temperature and prolonged temperature extremes in elderly populations in Taiwan. Environ. Res. 2011, 111, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Lao, X.; Rutherford, S.; Xu, Y.; Xu, X.; Lin, H.; Liu, T.; Luo, Y.; Xiao, J.; Hu, M.; et al. The effect of heat waves on mortality and effect modifiers in four communities of Guangdong Province, China. Sci. Total Environ. 2014, 482, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed lag linear and non-linear models in R.: The package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med. Res. Methodol. 2013, 13, 1. [Google Scholar] [CrossRef]
- Semenza, J.C.; McCullough, J.E.; Flanders, W.D.; McGeehin, M.A.; Lumpkin, J.R. Excess hospital admissions during the July 1995 heat wave in Chicago. Am. J. Prev. Med. 1999, 16, 269–277. [Google Scholar] [CrossRef]
- Kovats, R.S.; Hajat, S.; Wilkinson, P. Contrasting patterns of mortality and hospital admissions during hot weather and heat waves in Greater London, UK. Occup. Environ. Med. 2004, 61, 893–898. [Google Scholar] [CrossRef] [Green Version]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic factors in heat wave related deaths: A meta-analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Bi, P. Morbidity and mortality during heatwaves in metropolitan Adelaide. Med. J. Aust. 2007, 187, 662–665. [Google Scholar] [PubMed]
- Giegi, G.; Pistelli, F.; Sherrill, D.L.; Maio, S.; Baldacci, S.; Carrozzi, L. Definition, epidemiology and natural history of COPD. Eur. Respir. J. 2007, 30, 993–1013. [Google Scholar] [Green Version]
- Sprung, C.L. Heat stroke: Modern appraoch to an accident disease. Chest 1980, 77, 461–462. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | Standard Deviation | Minimum | Percentile | Maximum | ||
|---|---|---|---|---|---|---|---|
| 25% | 50% | 75% | |||||
| Maximum temperature (°C) | 33.8 | 1.8 | 24.5 | 32.7 | 34 | 35 | 39 |
| Average temperature (°C) | 28.4 | 1.3 | 23.0 | 27.5 | 28.4 | 29.4 | 32.1 |
| Minimum temperature (°C) | 25.4 | 1.4 | 20.0 | 24.5 | 25.4 | 26.3 | 29.8 |
| Average relative humidity (%) | 74.1 | 7.2 | 52 | 70 | 74 | 79 | 94 |
| Mortality data # | |||||||
| All-cause | 70 | 11.5 | 26 | 62 | 70 | 77 | 111 |
| Cardiovascular disease | 15 | 4.3 | 3 | 12 | 15 | 18 | 34 |
| Respiratory disease | 6.0 | 2.6 | 0 | 4 | 6 | 8 | 16 |
| Male | 38 | 7.3 | 13 | 33 | 38 | 43 | 64 |
| Female | 32 | 7.1 | 10 | 27 | 31 | 36 | 59 |
| 0–14 years old | 1 | 1.0 | 0 | 0 | 1 | 2 | 5 |
| 15–64 years old | 28 | 5.8 | 6 | 24 | 28 | 32 | 46 |
| ≥65 years old | 41 | 8.6 | 14 | 25 | 40 | 46 | 71 |
| Hospitalization data # | |||||||
| All-cause | 222 | 52.3 | 83 | 175.8 | 224 | 258 | 456 |
| Cardiovascular disease | 42 | 9.3 | 18 | 35 | 42 | 48 | 76 |
| Respiratory disease | 25 | 7.1 | 7 | 20 | 24 | 30 | 49 |
| Male | 107 | 25.2 | 36 | 87 | 105 | 123 | 239 |
| Female | 115 | 29.4 | 26 | 89 | 116 | 136 | 220 |
| 0–14 years old | 11 | 3.7 | 1 | 8 | 10 | 13 | 24 |
| 15–64 years old | 56 | 15.1 | 19 | 44 | 55 | 66 | 112 |
| ≥65 years old | 155 | 38.3 | 52 | 123 | 155 | 182 | 327 |
| Heat Wave Definition (Threshold, Duration) | Start–End Date | Duration (Days) | Intensity (°C) Median (Range) |
|---|---|---|---|
| 97th percentile, 2 days | 24/4–26/4/2010 | 2 | 31.2 (31.07–31.25) |
| 5/5–21/5/2010 | 16 | 31.75 (30.95–32.1) | |
| 23/5–27/5/2010 | 4 | 31.125 (30.925–32.125) | |
| 30/5–2/6/2010 | 3 | 31.23 (31.025–31.3) | |
| 31/3–6/4/2013 | 6 | 31.4 (30.9–32) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, T.N.; Honda, Y.; Van Do, D.; Pham, A.L.T.; Chu, C.; Huang, C.; Phung, D. Effects of Extreme Temperatures on Mortality and Hospitalization in Ho Chi Minh City, Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 432. https://doi.org/10.3390/ijerph16030432
Dang TN, Honda Y, Van Do D, Pham ALT, Chu C, Huang C, Phung D. Effects of Extreme Temperatures on Mortality and Hospitalization in Ho Chi Minh City, Vietnam. International Journal of Environmental Research and Public Health. 2019; 16(3):432. https://doi.org/10.3390/ijerph16030432
Chicago/Turabian StyleDang, Tran Ngoc, Yasushi Honda, Dung Van Do, Anh Lan Thi Pham, Cordia Chu, Cunrui Huang, and Dung Phung. 2019. "Effects of Extreme Temperatures on Mortality and Hospitalization in Ho Chi Minh City, Vietnam" International Journal of Environmental Research and Public Health 16, no. 3: 432. https://doi.org/10.3390/ijerph16030432