Treatment and Cost of Hepatocellular Carcinoma: A Population-Based Cohort Study in Taiwan

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Study Design and Population
2.3. Study Variables
2.4. Health Services Utilization and Costs
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
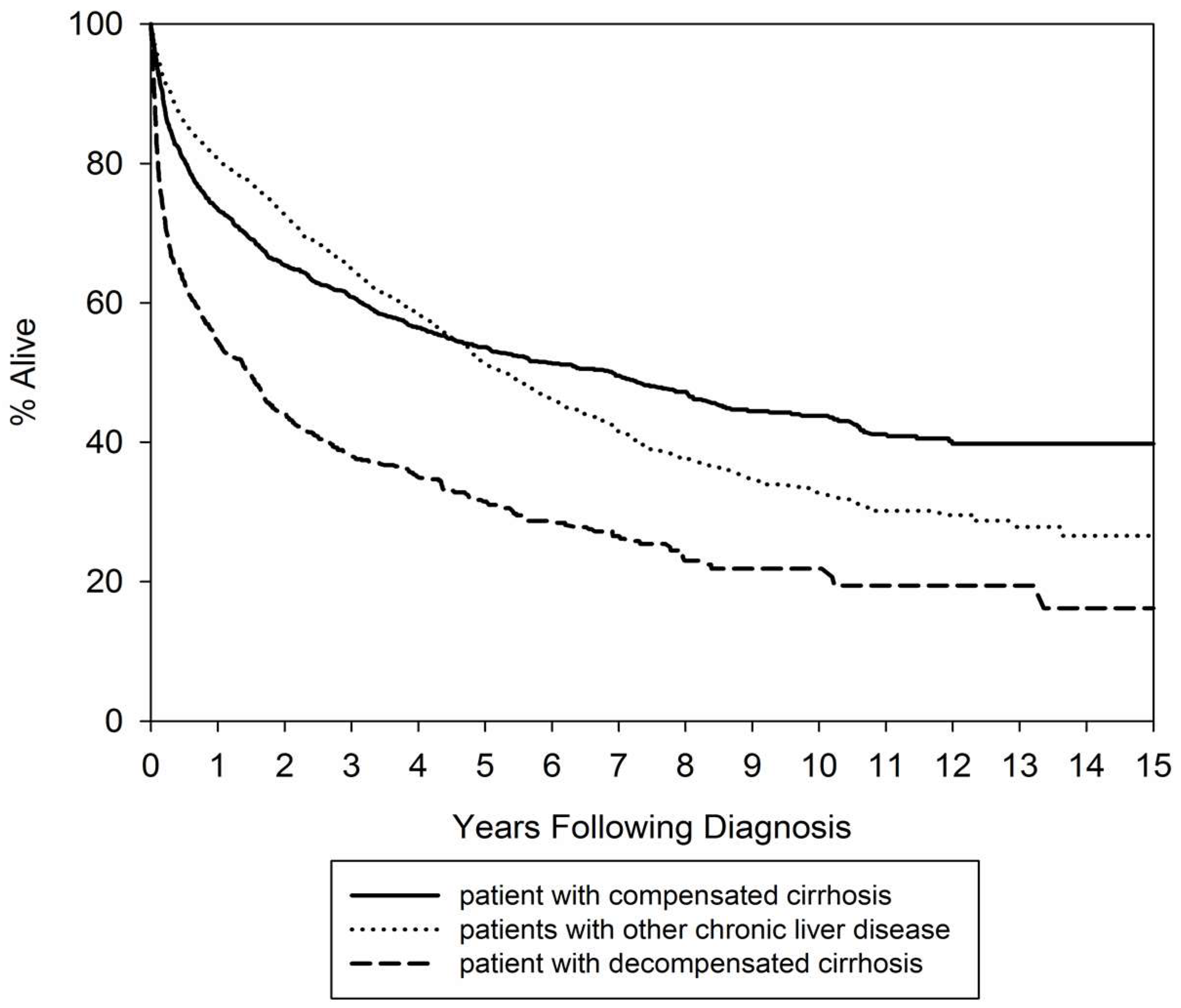
3.2. Survival Outcomes
3.3. Health Service Utilization
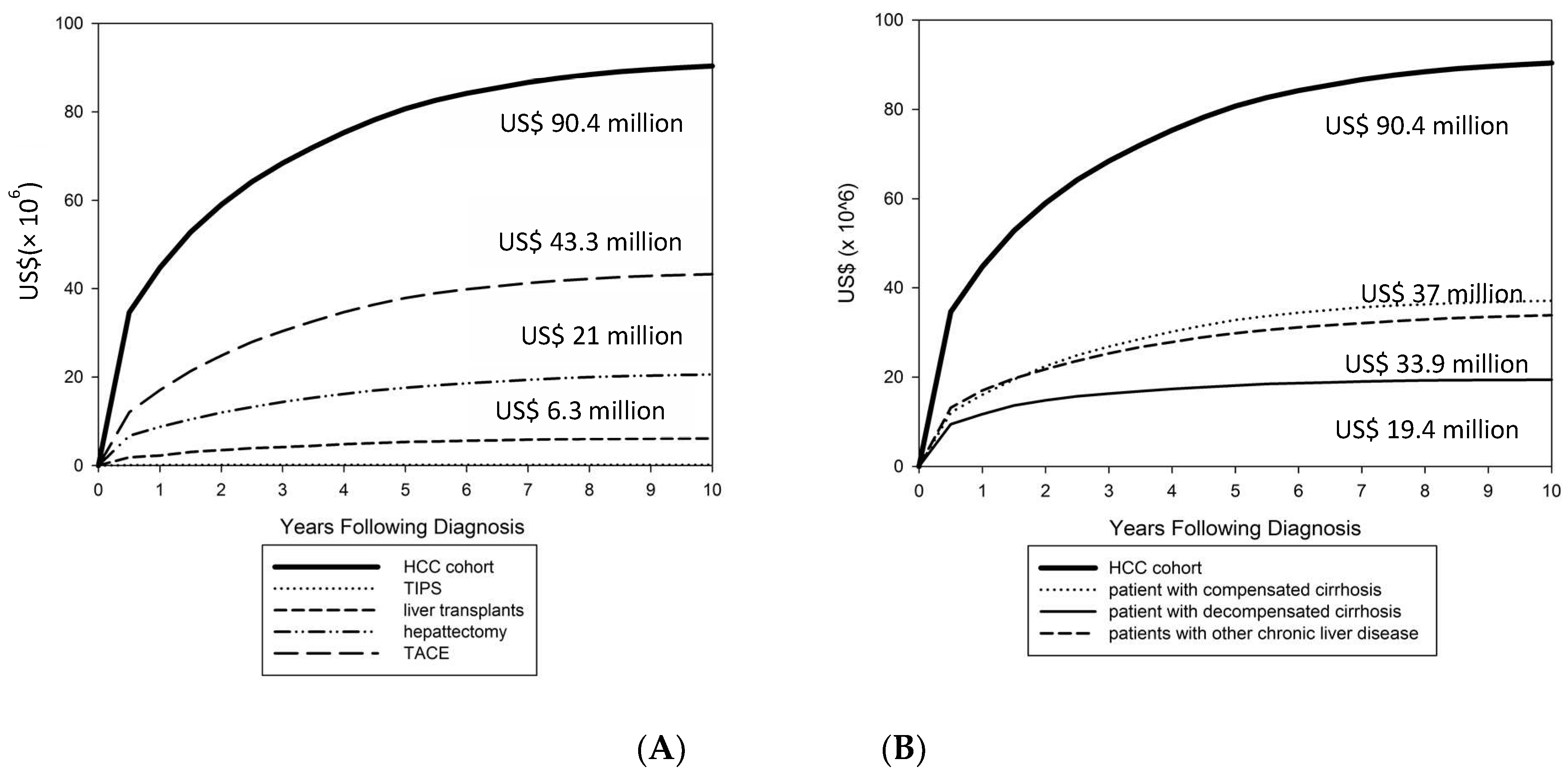
3.4. Total Cost for Caring for Hepatocellular Carcinoma Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012, 142, 1264–1273. [Google Scholar] [CrossRef]
- Sartorius, K.; Sartorius, B.; Aldous, C.; Govender, P.S.; Madiba, T.E. Global and country underestimation of hepatocellular carcinoma (HCC) in 2012 and its implications. Cancer Epidemiol. 2015, 39, 284–290. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127, S35–S50. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.C.; Wu, J.C.; Yen, S.H.; Lan, C.F.; Wu, S.L. The lifetime cost of hepatocellular carcinoma: A claims data analysis from a medical centre in Taiwan. Appl. Health Econ. Health Policy 2008, 6, 55–65. [Google Scholar] [CrossRef]
- Colombo, G.L.; Camma, C.; Attili, A.F.; Ganga, R.; Gaeta, G.B.; Brancaccio, G.; Franzini, J.M.; Volpe, M.; Turchetti, G. Patterns of treatment and costs of intermediate and advanced hepatocellular carcinoma management in four Italian centers. Ther. Clin. Risk Manag. 2015, 11, 1603–1612. [Google Scholar] [CrossRef]
- Thein, H.H.; Isaranuwatchai, W.; Campitelli, M.A.; Feld, J.J.; Yoshida, E.; Sherman, M.; Hoch, J.S.; Peacock, S.; Krahn, M.D.; Earle, C.C. Health care costs associated with hepatocellular carcinoma: A population-based study. Hepatology 2013, 58, 1375–1384. [Google Scholar] [CrossRef] [Green Version]
- Lang, K.; Danchenko, N.; Gondek, K.; Shah, S.; Thompson, D. The burden of illness associated with hepatocellular carcinoma in the United States. J. Hepatol. 2009, 50, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.J.; Yang, Y.W.; You, S.L.; Lai, M.S.; Chen, C.J. Thirty-year outcomes of the national hepatitis B immunization program in Taiwan. JAMA 2013, 310, 974–976. [Google Scholar] [CrossRef]
- Huang, Y.T.; Jen, C.L.; Yang, H.I.; Lee, M.H.; Su, J.; Lu, S.N.; Iloeje, U.H.; Chen, C.J. Lifetime risk and sex difference of hepatocellular carcinoma among patients with chronic hepatitis B and C. J. Clin. Oncol. 2011, 29, 3643–3650. [Google Scholar] [CrossRef]
- Chiang, C.J.; Yang, Y.W.; Chen, J.D.; You, S.L.; Yang, H.I.; Lee, M.H.; Lai, M.S.; Chen, C.J. Significant reduction in end-stage liver diseases burden through the national viral hepatitis therapy program in Taiwan. Hepatology 2015, 61, 1154–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longitudinal Health Insurance Database (LHID) 2000. National Health Insurance Research Database in Taiwan. Available online: http://nhird.nhri.org.tw/en/Data_Subsets.html (accessed on 26 April 2016).
- Cheng, C.L.; Chien, H.C.; Lee, C.H.; Lin, S.J.; Yang, Y.H. Validity of in-hospital mortality data among patients with acute myocardial infarction or stroke in National Health Insurance Research Database in Taiwan. Int. J. Cardiol. 2015, 201, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.Y.; Wang, S.N.; Wang, S.C.; Chuang, S.C.; Chen, C.M.; Lee, K.T. Preoperative transarterial chemoembolization and resection for hepatocellular carcinoma: A nationwide Taiwan database analysis of long-term outcome predictors. J. Surg. Oncol. 2014, 109, 487–493. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Fidelman, N.; Kwan, S.W.; LaBerge, J.M.; Gordon, R.L.; Ring, E.J.; Kerlan, R.K., Jr. The transjugular intrahepatic portosystemic shunt: An update. AJR. Am. J. Roentgenol. 2012, 199, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Directorate-General of Budget, Accounting and Statistics, Executive Yuan, Taiwan. Consumer Price Index Query. Available online: http://estat.dgbas.gov.tw/cpi_curv/cpi_curv.asp (accessed on 2 December 2016).
- Diehr, P.; Yanez, D.; Ash, A.; Hornbrook, M.; Lin, D.Y. Methods for analyzing health care utilization and costs. Annu. Rev. Public Health 1999, 20, 125–144. [Google Scholar] [CrossRef]
- Chang, I.C.; Huang, S.F.; Chen, P.J.; Chen, C.L.; Chen, C.L.; Wu, C.C.; Tsai, C.C.; Lee, P.H.; Chen, M.F.; Lee, C.M.; et al. The Hepatitis Viral Status in Patients with Hepatocellular Carcinoma: A Study of 3843 Patients From Taiwan Liver Cancer Network. Medicine 2016, 95, e3284. [Google Scholar] [CrossRef]
- Gagnon, Y.M.; Levy, A.R.; Iloeje, U.H.; Briggs, A.H. Treatment costs in Canada of health conditions resulting from chronic hepatitis B infection. J. Clin. Gastroenterol. 2004, 38, S179–S186. [Google Scholar] [CrossRef]
- White, L.A.; Menzin, J.; Korn, J.R.; Friedman, M.; Lang, K.; Ray, S. Medical care costs and survival associated with hepatocellular carcinoma among the elderly. Clin. Gastroenterol. Hepatol. 2012, 10, 547–554. [Google Scholar] [CrossRef]
- 2016 Statistics of Causes of Death. Ministry of Health and Welfare, Taiwan. Available online: http://www.mohw.gov.tw/lp-3327-2.html (accessed on 7 July 2017).
- Burak, K.W.; Kneteman, N.M. An evidence-based multidisciplinary approach to the management of hepatocellular carcinoma (HCC): The Alberta HCC algorithm. Can J. Gastroenterol. 2010, 24, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.J.; Chen, H.H.; Chen, C.L.; Fann, J.C.; Chen, S.L.; Chiu, S.Y.; Lin, Y.M.; Liao, C.S.; Chang, H.C.; Lin, Y.S.; et al. Cost-effectiveness analysis of population-based screening of hepatocellular carcinoma: Comparing ultrasonography with two-stage screening. World J. Gastroenterol. 2016, 22, 3460–3470. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.T.; Crowley, S.; Sheu, J.C. Cost-effectiveness analysis of a two-stage screening intervention for hepatocellular carcinoma in Taiwan. J. Formos Med. Assoc. 2010, 109, 39–55. [Google Scholar] [CrossRef]
- Falade-Nwulia, O.; Suarez-Cuervo, C.; Nelson, D.R.; Fried, M.W.; Segal, J.B.; Sulkowski, M.S. Oral Direct-Acting Agent Therapy for Hepatitis C Virus Infection: A Systematic Review. Ann. Int. Med. 2017, 166, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Chen, C.L. Living donor liver transplantation for hepatocellular carcinoma achieves better outcomes. Hepatobiliary Surg. Nutr. 2016, 5, 415–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Russell, M.C. Complications following hepatectomy. Surg. Oncol. Clin. North Am. 2015, 24, 73–96. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Tobe, R.G.; Inagaki, Y.; Kokudo, N.; Hasegawa, K.; Sugawara, Y.; Tang, W. The management of hepatocellular carcinoma around the world: A comparison of guidelines from 2001 to 2011. Liver Int. 2012, 32, 1053–1063. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | ||
|---|---|---|
| n | % | |
| Gender | ||
| Male | 3820 | 69.18% |
| Female | 1702 | 30.82% |
| Age at HCC diagnosis, years (mean ± SD) | 63.81 ± 13.58 | |
| Age group, years | ||
| <45 | 536 | 9.71% |
| 45–55 | 964 | 17.46% |
| 55–65 | 1338 | 24.23% |
| >65 | 2684 | 48.61% |
| CCI score (mean ± SD) (excluding liver-related diseases) | 1.79 ± 0.78 | |
| 0 | 1486 | 26.91% |
| 1 | 1619 | 29.32% |
| 2 | 810 | 14.67% |
| ≥3 | 1607 | 29.10% |
| Prior liver disease | ||
| None | 2316 | 41.94% |
| HBV only | 1532 | 27.74% |
| HCV only | 1240 | 22.46% |
| ALD only | 87 | 1.58% |
| HBV + HCV (or ≥2 items liver diseases *) | 347 | 6.28% |
| Prior complications | ||
| Nonalcoholic cirrhosis | 3020 | 54.69% |
| Biliary cirrhosis | 23 | 0.42% |
| Alcoholic cirrhosis | 385 | 6.97% |
| Ascites | 578 | 10.47% |
| Variceal bleeding | 619 | 11.21% |
| Hepatic encephalopathy | 313 | 5.67% |
| Other decompensated cirrhosis | 326 | 5.90% |
| Prior liver transplantation | 12 | 0.22% |
| Overall (n = 5522) | Compensated Cirrhosis (n = 2007) | Decompensated Cirrhosis (n = 1392) | Others (n = 2122) | |||||
|---|---|---|---|---|---|---|---|---|
| Liver transplantation | 61 | 1.1% | 30 | 1.5% | 23 | 1.7% | 8 | 0.4% |
| Hepatecotomy | 902 | 16.3% | 372 | 18.5% | 87 | 6.2% | 443 | 20.9% |
| TACE | 1737 | 31.5% | 862 | 42.9% | 295 | 21.2% | 580 | 27.3% |
| TIPS | 6 | 0.1% | 2 | 0.1% | 4 | 0.3% | 0 | 0 |
| Prescriptions drugs | 4230 | 76.6% | 1743 | 86.8% | 1033 | 74.2% | 1454 | 68.5% |
| NUC | 659 | 11.9% | 320 | 15.9% | 157 | 11.3% | 182 | 8.6% |
| INFs/RBV | 143 | 2.6% | 77 | 3.8% | 23 | 1.7% | 43 | 2.0% |
| Diuretics | 2802 | 50.7% | 1159 | 57.7% | 860 | 61.7% | 783 | 36.9% |
| Propranolol | 1443 | 26.1% | 595 | 29.6% | 412 | 29.6% | 436 | 20.5% |
| Liver protectants | 3214 | 58.2% | 1376 | 68.6% | 773 | 55.5% | 1065 | 50.2% |
| All-cause mortality | 2432 | 44.0% | 817 | 40.7% | 755 | 54.2% | 860 | 40.5% |
| Patient | Health Services and Costs | ||||||
|---|---|---|---|---|---|---|---|
| n | % | Mean | SD | Median | 25th | 75th | |
| Follow-up, years | 5522 | 2.7 | 3.3 | 1.4 | 0.3 | 3.7 | |
| Total cost | |||||||
| US$ per person | 16,711 | 21,350 | 10,512 | 4800 | 21,093 | ||
| US$ PPPM | 2143 | 5184 | 797 | 323 | 2177 | ||
| Hospitalization | 5522 | ||||||
| Number of hospitalization per person | 4.3 | 4.4 | 3 | 1 | 6 | ||
| LOS, days | 10.0 | 12.5 | 7 | 3 | 12 | ||
| US$ per person | 9721 | 11,811 | 5946 | 2533 | 12,544 | ||
| US$ PPPM | 1793 | 4560 | 504 | 148 | 1706 | ||
| Outpatient/emergency department visit | 5522 | ||||||
| Number of visit per person | 81.4 | 115.1 | 38 | 8 | 110 | ||
| US$ per person | 6989 | 14,726 | 2922 | 666 | 8063 | ||
| US$ PPPM | 349 | 1417 | 166 | 87 | 305 | ||
| Prescription for liver disease (US$ per person) | 4230 | 76.6% | 533 | 1389 | 49 | 7 | 285 |
| NUC | 659 | 11.9% | 1818 | 2206 | 943 | 182 | 2742 |
| INFs/RBV | 143 | 2.6% | 3867 | 2364 | 3735 | 2548 | 4715 |
| Diuretics | 2802 | 50.7% | 23 | 58 | 5 | 1 | 21 |
| Propranolol | 1443 | 26.1% | 17 | 1120 | 74 | 0 | 488 |
| Liver protectants | 3214 | 58.2% | 129 | 230 | 34 | 7 | 139 |
| Surgery or procedure (US$ per person) | |||||||
| Liver transplantation | 61 | 1.1% | 3908 | 12,474 | 1743 | 1152 | 2800 |
| Hepatecotomy | 902 | 16.3% | 1007 | 3186 | 480 | 251 | 953 |
| TACE | 1737 | 31.5% | 1273 | 2998 | 716 | 385 | 1337 |
| TIPS | 6 | 0.1% | 2111 | 1085 | 1664 | 1307 | 3210 |
| Compensated Cirrhosis | Decompensated Cirrhosis | Other Chronic Liver Diseases | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | |
| Follow-up, years | 3.0 | 3.1 | 2.0 | 0.6 | 4.4 | 1.6 | 2.4 | 0.5 | 0.1 | 1.8 | 3.2 | 3.8 | 1.5 | 0.3 | 4.7 |
| Total cost | |||||||||||||||
| US$ per person | 18,892 | 20,852 | 12,998 | 6350 | 24,284 | 13,992 | 20,888 | 7646 | 3269 | 16,865 | 16,431 | 21,896 | 10,230 | 5004 | 19,899 |
| US$ PPPM | 1643 | 4652 | 654 | 310 | 1465 | 3212 | 5002 | 1626 | 557 | 3881 | 1913 | 5658 | 689 | 253 | 1923 |
| Hospitalization | |||||||||||||||
| Number of hospitalization per person | 5.1 | 4.7 | 4 | 2 | 7 | 3.6 | 3.9 | 2 | 1 | 4 | 4 | 4.4 | 2 | 1 | 5 |
| LOS, days | 9.2 | 11.7 | 6 | 3 | 11 | 11.4 | 13.2 | 7 | 4 | 14 | 10.2 | 12.9 | 7 | 3 | 13 |
| US$ per person | 10,878 | 12,258 | 7035 | 3088 | 14,400 | 9378 | 13,146 | 5039 | 2188 | 11,378 | 8852 | 10,270 | 5562 | 2343 | 11,468 |
| US$ PPPM | 1320 | 4444 | 380 | 139 | 1015 | 2824 | 4461 | 1132 | 316 | 3512 | 1565 | 4628 | 409 | 98 | 1399 |
| Outpatient/emergency department visit | |||||||||||||||
| Number of visit per person | 95.1 | 115.5 | 59 | 18 | 131 | 45.7 | 75.2 | 12 | 20 | 57 | 91.8 | 130.5 | 41 | 11 | 121 |
| US$ per person | 8014 | 13,502 | 4393 | 1304 | 9800 | 4614 | 11,464 | 1310 | 211 | 4916 | 7579 | 17,342 | 2893 | 795 | 8354 |
| US$ PPPM | 323 | 730 | 174 | 105 | 294 | 388 | 1194 | 179 | 79 | 355 | 348 | 1946 | 151 | 75 | 281 |
| Variable | Coefficient | 95% CI | p Value | |
|---|---|---|---|---|
| Intercept | 9.10 | 8.9215 | 9.2776 | <0.0001 |
| Male vs. female | 0.898 | −0.0221 | 0.2016 | 0.1156 |
| 45–55 vs. ≤45 years | 0.0418 | −0.0721 | 0.1557 | 0.4716 |
| 55–65 vs. ≤45 years | −0.0515 | −0.1873 | 0.0843 | 0.4575 |
| >65 vs. ≤45 years | −0.3015 | −0.5133 | −0.0896 | 0.0053 |
| Compensated cirrhosis * | −0.016 | −0.1276 | 0.0957 | 0.7792 |
| Decompensated cirrhosis * | 0.0982 | −0.0351 | 0.2315 | 0.1487 |
| INFs/RBV vs. none | −0.06 | −0.2672 | 0.1472 | 0.5701 |
| Liver transplantation | 1.4699 | 1.348 | 1.5918 | <0.0001 |
| Hepatectomy | 0.1526 | 0.0422 | 0.2629 | 0.007 |
| TACE | 0.4448 | 0.3434 | 0.5462 | <0.0001 |
| TIPS | 0.4796 | −0.6079 | 1.5672 | 0.3874 |
| CCI score | 0.0745 | 0.0451 | 0.1039 | <0.0001 |
| Length of follow-up | 0.0064 | 0.0056 | 0.0073 | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguang, S.-H.; Wu, C.-K.; Liang, C.-M.; Tai, W.-C.; Yang, S.-C.; Ku, M.-K.; Yuan, L.-T.; Wang, J.-W.; Tseng, K.-L.; Hung, T.-H.; et al. Treatment and Cost of Hepatocellular Carcinoma: A Population-Based Cohort Study in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2655. https://doi.org/10.3390/ijerph15122655
Nguang S-H, Wu C-K, Liang C-M, Tai W-C, Yang S-C, Ku M-K, Yuan L-T, Wang J-W, Tseng K-L, Hung T-H, et al. Treatment and Cost of Hepatocellular Carcinoma: A Population-Based Cohort Study in Taiwan. International Journal of Environmental Research and Public Health. 2018; 15(12):2655. https://doi.org/10.3390/ijerph15122655
Chicago/Turabian StyleNguang, Seng-Howe, Cheng-Kun Wu, Chih-Ming Liang, Wei-Chen Tai, Shih-Cheng Yang, Ming-Kun Ku, Lan-Ting Yuan, Jiunn-Wei Wang, Kuo-Lun Tseng, Tsung-Hsing Hung, and et al. 2018. "Treatment and Cost of Hepatocellular Carcinoma: A Population-Based Cohort Study in Taiwan" International Journal of Environmental Research and Public Health 15, no. 12: 2655. https://doi.org/10.3390/ijerph15122655