Safety Assessment of Electronic Cigarettes and Their Relationship with Cardiovascular Disease

 ,
,
Abstract
:1. Introduction
2. Research Content of E-Cigarettes
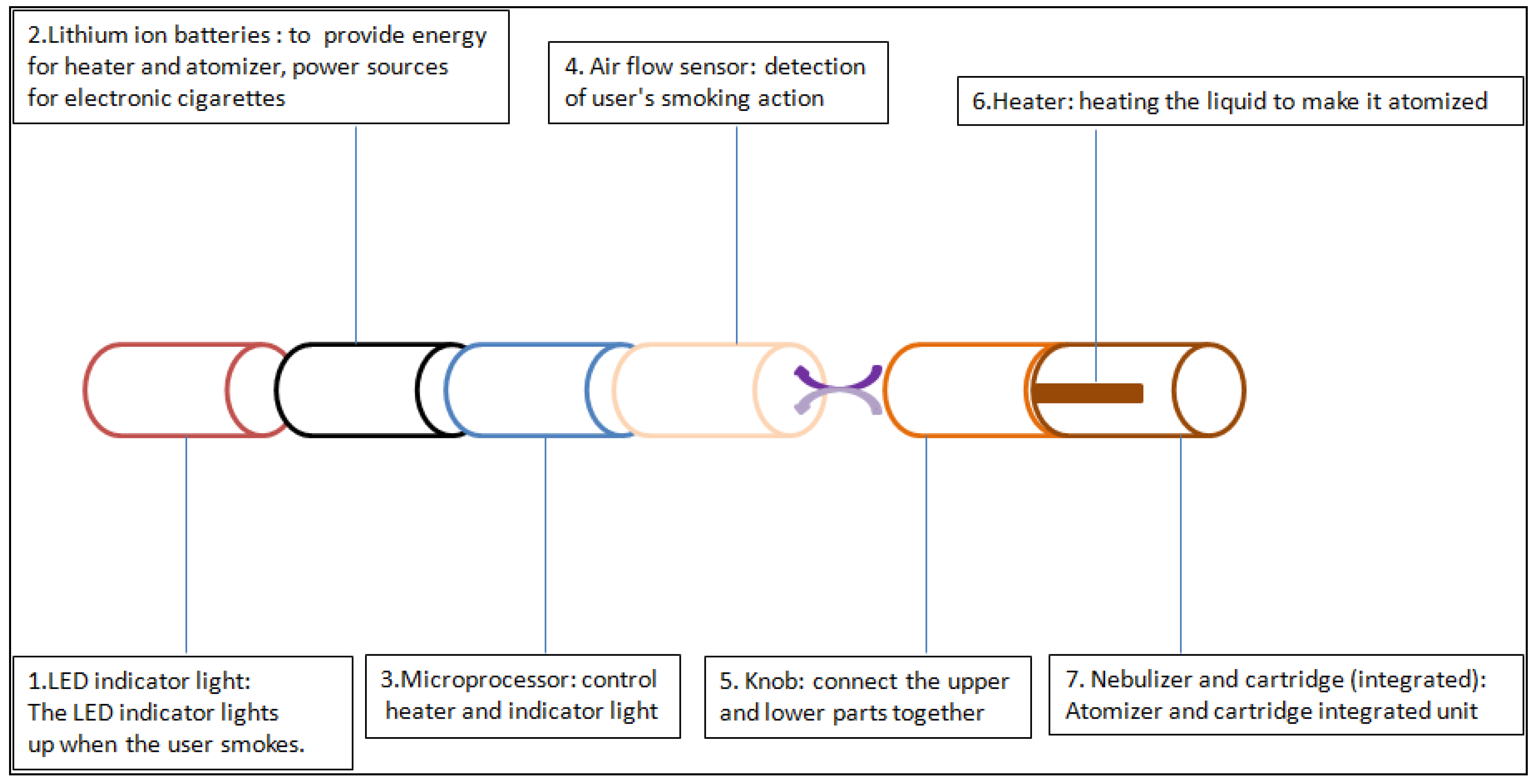
2.1. The Development of E-Cigarettes
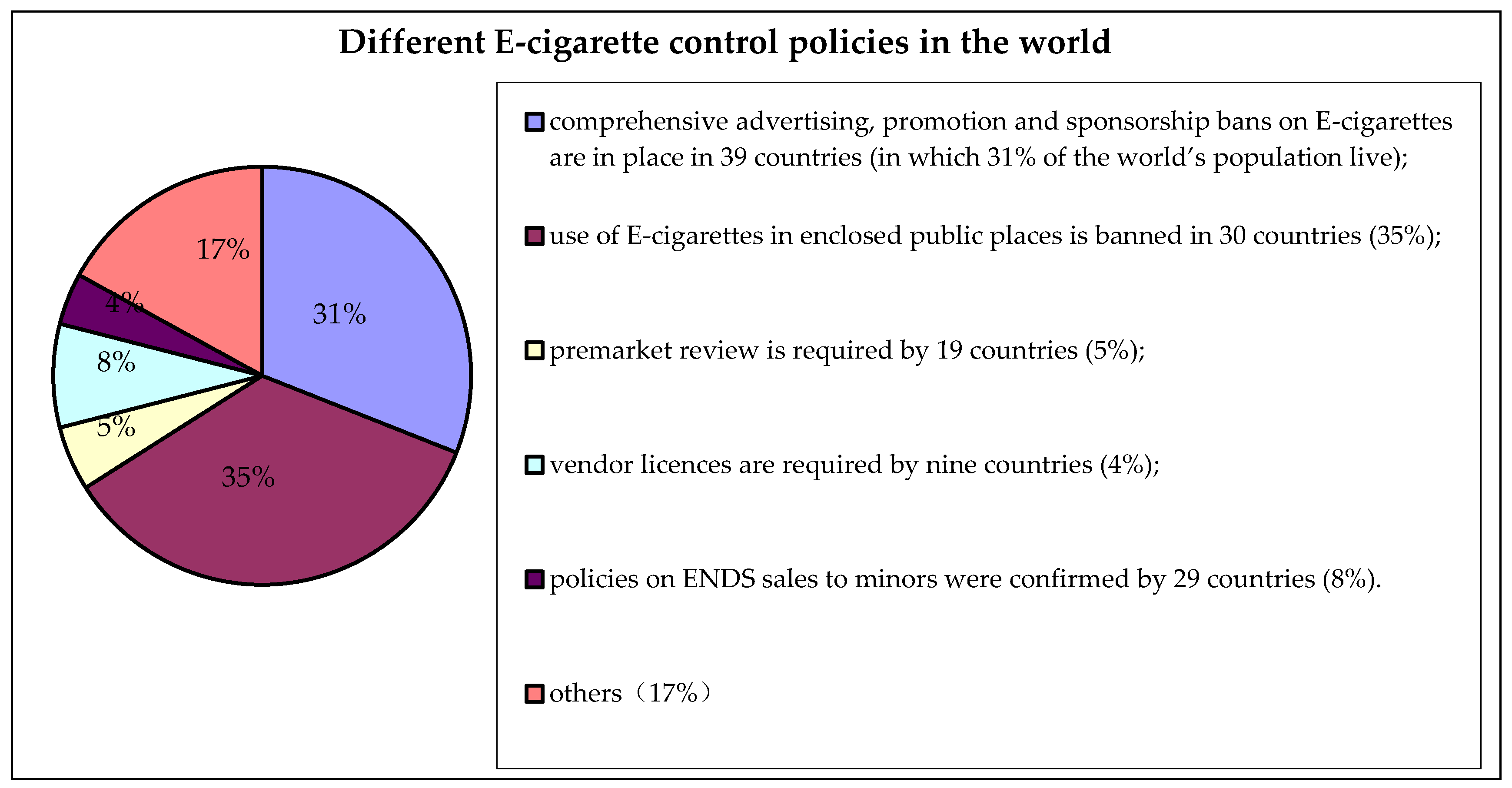
2.2. The Classification of E-Cigarettes in Different Countries Based on Its Properties
2.2.1. Tobacco Products
2.2.2. Pharmaceutical Products
2.2.3. Consumer Products
2.2.4. Other
2.3. Production Control
2.4. The Harm of E-Cigarettes
2.4.1. Main Components and Hazards of Gas Emissions from E-Cigarettes
- (1)
- For the carbonyl compounds, the heating of glycerol will produce harmful aldehydes related to temperature, including formaldehyde, acetaldehyde and acrolein. These three compounds were identified in almost all of the examined E-cigarettes [22]. The study of Gassee, F.R. et al. showed that the mixture of the above three compounds produced more sensory stimuli than those of a single compound [24]. Among them, formaldehyde was categorized as a Class 1 carcinogen in 2006. Acrolein stimulates the nasal cavity, damages the lungs and the inner walls of the blood vessels, and is a major factor leading to cardiovascular disease. Chronic inhalation of acrolein inhibits circulation of endothelial progenitor cells and promotes atherosclerosis, which accelerates the rate of hardening of the aorta by 1.6 times [25]. Ambrus, J.L. et al. also confirmed the presence of acrolein, toxic substances and mutagenic compounds in E-cigarette smoke. It was found that the carcinogenic metabolic enzymes in rats exposed to E-cigarette smoke increased significantly, inducing a greater carcinogenic risk of carcinogens in E-cigarette smoke [26].
- (2)
- Nicotine is the addictive component of tobacco. It induces adverse effects during pregnancy and contributes to the progress of cardiovascular disease. Although nicotine itself is not a carcinogen, it functions as a “tumor promoter”. Nicotine is involved in neurodegeneration and other malignant diseases. Therefore, the use of nicotine in children, adolescents, pregnant women and women of reproductive age should be treated with great caution, due to the effects of nicotine on the brain [2]. The effects of nicotine on the cardiovascular system will be elaborated in the following chapters.
- (3)
- Volatile organic compounds (VOCs) include toluene and meta xylene. In the study of Czogala, J. et al. almost all of the detected smokes contained toluene [27]. In the study of Goniewicz, M.L. et al. toluene and meta xylene were detected in almost all sample smokes. These VOCs are irritating to the skin and mucous membrane, and have an anesthetic effects on the central nervous system, as well as having certain carcinogenicity [22].
- (4)
- N′-nitrosonornicotine (NNN), 4-(methylonitrosoamino)-1-(3-pirydyl)-l-butanone (NNK) and N′-nitrosoanatabine (NAT) are the three most representative tobacco-specific nitrosamines (TSNAS) in E-cigarettes. Kim, H.J. et al. tested the content of TSNAS in e-liquid samples. There were various kinds of TSNAS tested in 105 samples, among which the maximum concentration of NAT reached 62.19 ug/L, significantly exceeding the requirement for cigarette companies [28]. Nitrosamines have strong carcinogenicity. Moreover, both nitrosamine and the polycyclic aromatic hydrocarbon benzopyrene can interact with DNA. These produced additives interfere DNA replication and the duplicated DNA produces purine free sites and triggers gene mutations [29]. The chemical mixture in the smoke of the E-cigarette will cause chromosome division, and may cause damage to mitotic spindles or filaments, thereby inducing mutations [21].
- (5)
- Heavy metals include lead, nickel, cadmium, and so on. In 2013, Williams, M. et al. found heavy metals such as tin, nickel, lead, chromium and other nanoparticles in the smoke of E-cigarettes [30]. The inhaled heavy metal nanoparticles can be deposited in the alveoli, inducing lung damage and leading to cough, dyspnea, chest pain, pulmonary edema, acute respiratory failure, as well as carcinogenicity, nephrotoxicity, and neurotoxicity [22]. For example, tin is cytotoxic to human lung fibroblasts [30]. In 2017, Williams, M. et al. continued to study the electronic flue gas sol. They selected 36 kinds of elements to detect, of which 35 kinds were detected in the electronic flue gas sol, while there were only 15 kinds of heavy metals detected in traditional cigarettes. These elements contain a variety of heavy metals, and the concentration is usually higher than that of traditional cigarette smoke [31]. The content of lead and chromium is equal to that of traditional cigarette smoke. Especially the nickel content is much higher than that of traditional cigarettes [30]. However, we still do not know the effects of inhaling heavy metal particles in aerosol on health.
- (6)
- There are studies that have investigated the cytotoxicity of the essence in E-cigarettes. Bahl, V. et al. used MTT (3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyl-2-H-tetrazolium bromide) assays to test the cytotoxicity of e-liquids. The results showed that some e-liquids were cytotoxic to human embryonic stem cells and mouse neural stem cells, and that the composition and concentration of chemical components played an important role. In addition, more evidences confirmed that the chemical properties and the concentration of essence added to the e-liquid, rather than the nicotine alone, are much more harmful [32]. Farsalinos, K.E. et al. used MTT tests to study the in vitro toxicity of the e-liquid of 20 E-cigarettes. The results showed that some electronic smoke liquid had a toxic effect on cardiac muscle cells after heating and atomizing, which would cause disease. The evidence indicated that the ingredients involved in the progress of diseases were related to the production process adopted by the liquid tobacco production company, as well as the flavor components added to cater to the public’s preference [33]. Cinnamylaldehyde and diacetyl are approved flavorings in food, but they will affect people’s health when inhaled [19]. Zeng, W.L. et al. collected tobacco smoke by cell culture medium, and studied the effect of smoke on the relative proliferation rate of Chinese hamster ovary cells (CHO cells) by MTT. The results showed that the relative proliferation rate of flue gas trapping liquid on CHO cells was 10 times higher than that of a 3R4F-reference-cigarette at 100% smoke concentration [34].
2.4.2. The Harm of Second-Hand Smoke from E-Cigarettes
2.4.3. E-Cigarettes and Smoking Cessation
2.5. E-Cigarettes and Cardiovascular Atherosclerotic Diseases
- (1)
- The harm of nicotine: smoking has become an independent risk factor for the formation of atherosclerosis, and the addictiveness of nicotine is known to all. Nicotine induces the release of catecholamine and cortisol, and causes hemodynamic changes (increase in heart rate, rise in blood pressure, and the vasoconstriction) and adverse effects on blood lipids (leading to activation of adenylate cyclase in adipose tissue and decomposition of triglycerides. The study found that the total lipid composition of the rats exposed to E-cigarettes smoke increased significantly, the content of saturated fatty acids increased significantly, while the content of unsaturated fatty acids decreased significantly), as well as the induction of insulin resistance [19,21]. Nicotine can also cause endothelial dysfunction, inhibit apoptosis, and enhance angiogenesis. This effect raises concerns with regard to nicotine promoting cancer development and accelerating atherosclerosis [46]. Researchers at Danderyd Hospital in Sweden have found that inhaling E-cigarettes only 10 times can cause signs of damage to the blood vessels. Subsequently, they further studied the effects on healthy people of inhaling E-cigarettes 30 times. Magnus Rudbeck, a doctor at Danderyd Hospital who participated in the study, believes that E-cigarette users have poor vascular elasticity, and the poor vascular elasticity may lead to heart disease and stroke. Researchers believe that the nicotine in E-cigarettes may lead to poor vascular elasticity [47]. The study of Flouris, A.D. et al. found that white blood cell count increased after smoking E-cigarettes, which reflected the inflammatory process of acute cardiovascular events [48]. The health status of E-cigarette users was analyzed. It was found that, compared with non-smokers, the former had an enhancement in cardiac sympathetic nerve excitability, and they were more prone to oxidative stress reactions. Professor Choupo Perk from European Society of Cardiology explained that the stimulation of atomized nicotine on sympathetic nerves can cause irregular beating of the heart and elevated blood pressure, and may cause long-term harmful effects on the growth of the vascular wall [49]. Vlachopoulos, C. et al. investigated cardiovascular risk factors among 24 young smokers in 4 different smoking scenarios, and used femoral artery to femoral pulse wave velocity (PWV) to assess aortic stiffness, finding that E-cigarette smoke increased young people’s arterial stiffness and blood pressure, and smoking E-cigarettes for over 30 min had an adverse effect on arterial stiffness that was similar to that of traditional cigarettes [50]. The study of Battista, L. et al. also showed that nicotine inhalation vapors produced the same pathophysiological cardiovascular effects as traditional cigarettes [51]. Farsalinos, K.E. et al. studied the acute effects of E-cigarette smoke on the cardiovascular system of exposed people, and the results showed that the cardiac output blood pressure of people exposed to E-cigarettes (11 mg/mL of nicotine content) increased slightly; when the heart of smokers contracted, cardiac output and heart rate were significantly increased. They also used the MTT test to authenticate that the atomized e-liquid has toxic effect on cultured myocardial cells [33].
- (2)
- The hazards of aerosol particles were also studied. Zhang, Y. et al. showed that 73~80% of the particles were in exhaled aerosols, while 7~18% of the particles were stored in the alveoli. It is estimated that 20~27% of the particles entered the circulatory system, which is equivalent to the proportion for traditional cigarette smoke [52]. Moreover, the size distribution and amount of particles of E-cigarettes are similar to those of traditional cigarettes, and some E-cigarettes produce more particles than traditional cigarettes. Particles may cause lung and systemic inflammation, and increase the risk of cardiovascular disease, respiratory disease and death [5].
3. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wang, Y. Development status and Future Research Ideas of Electronic Cigarettes. China Sci. Technol. Inf. 2017, 9, 49–50. [Google Scholar]
- FCTC (Framework Convention on Tobacco Control). COP/6/10: FCA Policy Briefing Electronic Nicotine Delivery Systems. Moscow. 2014. Available online: http://apps.who.int/gb/fctc/PDF/cop6/FCTC_COP6_10-en.pdf (accessed on 15 December 2014).
- Grana, R.; Benowitz, N.; Glantz, S.A. Background Paper on E-Cigarettes (Electronic Nicotine Delivery Systems). Center for Tobacco Control Research and Education, University of California, San Francisco, a WHO Collaborating Center on Tobacco Control. Prepared for World Health Organization Tobacco Free Initiative. December 2013. Available online: http://pvw.escholarship.org/uc/item/13p2b72n (accessed on 31 March 2014).
- Jin, X. Is E-cigarette Really Healthy? China Anti-Count. Rep. 2017, 2, 119–121. [Google Scholar]
- Grana, R.; Benowitz, N.; Glantz, S.A. E-cigarettes: A scientific review. Circulation 2014, 129, 1972–1986. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, H.A. Smokeless Non-Tobacco Cigarette. U.S. Patent No. 3200819 A, 17 August 1965. [Google Scholar]
- Li, H. Non-Combustible Electronic Atomizing Cigarette. CN Patent No. 2643681, 29 September 2004. [Google Scholar]
- Li, H. Aerosol Electronic Cigarette. International Patent Application No. PCT/CN2007/001575, 22 November 2007. [Google Scholar]
- Wei, A. Is E-cigarettes really “smoking cessation artifact”? Enterp. Stand. 2015, 8, 24–25. [Google Scholar]
- Ding, D. General situation of electronic cigarette control abroad and Its Enlightenment to China. Acta Tabacaria Sin. 2017, 23, 128–135. [Google Scholar]
- Fan, M.; Zhao, L.; Cui, H.; Guo, J.; Liu, S.; Chen, L.; Liu, H. Current situation and legislation progress of electronic cigarette control at home and abroad. Acta Tabacaria Sin. 2016, 22, 126–132. [Google Scholar]
- Li, B. A global perspective on electronic cigarette’s future development and related controversial and regulatory issues. Acta Tabacaria Sin. 2014, 4, 101–107. [Google Scholar]
- Li, Z. The Need of regulation on E-cigarette chaos. Pop. Stand. 2015, 10, 53. [Google Scholar]
- People Network. The Need of Change in E-Cigarette Industry Chaos. Available online: http://finance.people.com.cn/stock/GB/222942/16603305.html (accessed on 14 December 2011).
- Chen, I.-L. FDA Summary of Adverse Events on Electronic Cigarettes. Nicotine Tob. Res. 2013, 15, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Jing, J. The Continuous Explosion Events of E-cigarettes in the United States. China Qual. Super. 2017, 2, 82. [Google Scholar]
- Han, S.; Chen, H.; Liu, T.; Hou, H.; Hu, Q. Simultaneous Determination of Main Chemical Components in E-liquid by gas chromatography. J. Anhui Agric. Sci. 2014, 42, 8344–8347. [Google Scholar]
- Laugesen, M. Second safety report on the Ruyan® e-cigarette. Cell 2008, 8, 4375. [Google Scholar]
- Bhatnagar, A.; Whitsel, L.P.; Ribisl, K.M.; Bullen, C.; Chaloupka, F.; Piano, M.R.; Robertson, R.M.; McAuley, T.; Goff, D. Electronic cigarettes: A policy statement from the American Heart Association. Circulation 2014, 130, 1418–1436. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Anagnostopoulos, N.; Kougias, M.; Evangelopoulou, V.; Connolly, G.N.; Behrakis, P.K. Short-term pulmonary effects of using an electronic cigarette: Impact on respiratory flow resistance, impedance, and exhaled nitric oxide. Chest J. 2012, 141, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Canistro, D.; Vivarelli, F.; Cirillo, S.; Marquillas, C.B.; Buschini, A.; Lazzaretti, M.; Machi, L.; Cardenia, V.; Rodriguez-Estrada, M.T.; Lodovici, M.; et al. E-cigarettes induce toxicological effects that can raise the cancer risk. Sci. Rep. 2017, 7, 2028. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Hutzler, C.; Paschke, M.; Kruschinski, S.; Henkler, F.; Hahn, J.; Luch, A. Chemical hazards present in liquids and vapors of electronic cigarettes. Arch. Toxicol. 2014, 88, 1295–1308. [Google Scholar] [CrossRef] [PubMed]
- Cassee, F.R.; Arts, J.H.; Groten, J.P.; Feron, V.J. Sensory irritation to mixtures of formaldehyde, acrolein, and acetaldehyde in rats. Arch. Toxicol. 1996, 70, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Conklin, D.J.; Agarwal, A.; Sithu, S.; Zeller, I.; Haberzettl, P.; O’toole, T.E.; Bhatnagar, A.; Srivastava, S. Abstract15705: Chronic Inhaled Acrolein Depresses Circulating Endothelial Progenitor Cells and Promotes Atherosclerosis. Circulation 2015, 132, A15705. [Google Scholar]
- Ambrus, J.L.; Mink, I.B. Effect of Cigarette Smoking on Blood Coagulation. Clin. Pharmacol. Ther. 1964, 5, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Czogala, J.; Goniewicz, M.L.; Fidelus, B.; Zielinska-Danch, W.; Travers, M.J.; Sobczak, A. Secondhand exposure to vapors from electronic cigarettes. Nicotine Tob. Res. 2014, 16, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Shin, H.S. Determination of tobacco-specific nitrosamines in replacement liquids of electronic cigarettes by liquid chromatography-tandem mass spectrometry. J. Chromatogr. A 2013, 1291, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Yang, L.; Duan, Y.; Zhao, W.; Yang, J.; Gong, X.; Li, S.; Chen, Y. Safety and risk assessment of electronic nicotine delivery system. Sci. Technol. Rev. 2016, 34, 131–136. [Google Scholar]
- Williams, M.; Villarreal, A.; Bozhilov, K.; Lin, S.; Talbot, P. Metal and silicate particles including nanoparticles are present in electronic cigarette cartomizer fluid and aerosol. PLoS ONE 2013, 8, e57987. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.; Bozhilov, K.; Ghai, S.; Talbot, P. Elements including metals in the atomizer and aerosol of disposable electronic cigarettes and electronic hookahs. PLoS ONE 2017, 12, e0175430. [Google Scholar] [CrossRef] [PubMed]
- Bahl, V.; Lin, S.; Xu, N.; Davis, B.; Wang, Y.H.; Talbot, P. Comparison of electronic cigarette refill fluid cytotoxicity using embryonic and adult models. Reprod. Toxicol. 2012, 34, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Tsiapras, D.; Kyrzopoulos, S.; Savvopoulou, M.; Voudris, V. Acute effects of using an electronic nicotine-delivery device (electronic cigarette) on myocardial function: Comparison with the effects of regular cigarettes. BMC Cardiovasc. Disord. 2014, 14, 78. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Gao, Q.; Yang, Y.; Yao, J.; Song, C.; Li, X. Effect of Cigarette Smoke Trapping Liquid on the Relative Proliferation Rate of CHO Cells. Chem. Bioeng. 2015, 8, 67–69. [Google Scholar]
- Moritsugu, K.P. The 2006 Report of the Surgeon General: The health consequences of involuntary exposure to tobacco smoke. Am. J. Prev. Med. 2007, 32, 542–543. [Google Scholar] [CrossRef] [PubMed]
- Schripp, T.; Markewitz, D.; Uhde, E.; Salthammer, T. Does e-cigarette consumption cause passive vaping? Indoor Air 2013, 23, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Lee, L. Electronic cigarettes are a source of thirdhand exposure to nicotine. Nicotine Tob. Res. 2015, 17, 256–258. [Google Scholar] [CrossRef] [PubMed]
- Schober, W.; Szendrei, K.; Matzen, W.; Osiander-Fuchs, H.; Heitmann, D.; Schettgen, T.; Jörres, R.A.; Fromme, H. Use of electronic cigarettes (e-cigarettes) impairs indoor air quality and increases FeNO levels of e-cigarette consumers. Int. J. Hyg. Environ. Health 2014, 217, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Chorti, M.S.; Poulianiti, K.P.; Jamurtas, A.Z.; Kostikas, K.; Tzatzarakis, M.N.; Wallace Hayes, A.; Tsatsakis, A.M.; Koutedakis, Y. Acute impact of active and passive electronic cigarette smoking on serum cotinine and lung function. Inhal. Toxicol. 2013, 25, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Tendera, M.; Aboyans, V.; Bartelink, M.L.; Baumgartner, I.; Clement, D.; Collet, J.P.; Cremonesi, A.; De Carlo, M.; Erbel, R.; Fowkes, F.G.R.; et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: The Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2011, 32, 2851–2906. [Google Scholar] [PubMed]
- Vaz-Carneiro, A.; Costa, J. [Analysis of the Cochrane Review: Electronic Cigarettes for Smoking Cessation and Reduction. Cochrane Database Syst Rev. 2014, 12, CD010216]. Acta Med. Port. 2015, 28, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Li, N. Can E-cigarettes Really Stop Smoking? Sci. News 2013, 8, 50–51. [Google Scholar]
- Cai, J.; Chen, L.; Peng, B.; Yu, J.; Cui, H.; Wang, B.; Zhang, X.; Liu, H.; Liu, S. Simultaneous Determination of Nicotine, 1,2-propanediol and Glycerol in E-liquid by Gas Chromatography. Acta Tabacaria Sin. 2016, 5, 1–9. [Google Scholar]
- Zhang, G.; Chen, Y. Research Progress in Risk Factors of Atherosclerosis. Mod. Med. Health 2014, 17, 2603–2606. [Google Scholar]
- Chen, P.; Qin, W.; Zhang, Y. Research Progress in Nicotine Inducing Atherosclerosis. Chin. Med. Her. 2015, 19, 34–44. [Google Scholar]
- Balakumar, P.; Kaur, J. Is nicotine a key player or spectator in the induction and progression of cardiovascular disorders? Pharmacol. Res. 2009, 60, 361–368. [Google Scholar] [CrossRef] [PubMed]
- New Research Found That Electronic Cigarette Injury Blood Vessel. Invent. Innov. 2017, 6, 4. Available online: http://english.sina.com/news/2017-05-06/detail-ifyeycte8949668.shtml (accessed on 9 September 2017).
- Flouris, A.D.; Poulianiti, K.P.; Chorti, M.S.; Jamurtas, A.Z.; Kouretas, D.; Owolabi, E.O.; Tzatzarakis, M.N.; Tsatsakis, A.M.; Koutedakis, Y. Acute effects of electronic and tobacco cigarette smoking on complete blood count. Food Chem. Toxicol. 2012, 50, 3600–3603. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Evidence for Research on the Harm of E-cigarettes. Guangxi Quality Supervision Guide. Periodical 2017, 3, 9. [Google Scholar]
- Vlachopoulos, C.; Ioakeimidis, N.; Abdelrasoul, M.; Terentes-Printzios, D.; Georgakopoulos, C.; Pietri, P.; Stefanadis, C.; Tousoulis, D. Electronic Cigarette Smoking Increases Aortic Stiffness and Blood Pressure in Young Smokers. J. Am. Coll. Cardiol. 2016, 67, 2802–2803. [Google Scholar] [CrossRef] [PubMed]
- Battista, L.; Di Iorio, M.; Tancredi, M.; Acconcia, M.C.; Torromeo, C.; Barillà, F.; Paravati, V.; Gaudio, C.; Pannarale, G. Abstract16755: Cardiovascular Effects of Electronic Cigarettes. Circulation 2013, 128, A16755. [Google Scholar]
- Zhang, Y.; Sumner, W.; Chen, D.R. In vitro particle size distributions in electronic and conventional cigarette aerosols suggest comparable deposition patterns. Nicotine Tob. Res. 2013, 15, 501–508. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Product Attributes | Countries and Regions |
|---|---|
| consumer product | Slovenia, Bulgaria, Czech Republic, Ireland, Italy, India, Latvia, Holland, Poland, Russia, Cyprus, Spain, Ukraine, etc. |
| tobacco product | The United States, Brunei, South Korea, Lithuania, Malta, Singapore, Thailand, Togo, Vietnam, etc. |
| pharmaceutical product | Austria, Belgium, Canada, Denmark, Luxembourg, Britain, Japan, Finland, France, Greece, Hungary, New Zealand, Taiwan, Estonia, Portugal, Slovakia, Switzerland, Sweden, etc. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, G.; Wang, Z.; Zhang, K.; Hou, R.; Xing, C.; Yu, Q.; Liu, E. Safety Assessment of Electronic Cigarettes and Their Relationship with Cardiovascular Disease. Int. J. Environ. Res. Public Health 2018, 15, 75. https://doi.org/10.3390/ijerph15010075
Zhang G, Wang Z, Zhang K, Hou R, Xing C, Yu Q, Liu E. Safety Assessment of Electronic Cigarettes and Their Relationship with Cardiovascular Disease. International Journal of Environmental Research and Public Health. 2018; 15(1):75. https://doi.org/10.3390/ijerph15010075
Chicago/Turabian StyleZhang, Guangwei, Zhangli Wang, Kai Zhang, Rui Hou, Chunli Xing, Qi Yu, and Enqi Liu. 2018. "Safety Assessment of Electronic Cigarettes and Their Relationship with Cardiovascular Disease" International Journal of Environmental Research and Public Health 15, no. 1: 75. https://doi.org/10.3390/ijerph15010075