Exposure to Ambient Fine Particulate Air Pollution in Utero as a Risk Factor for Child Stunting in Bangladesh


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Galasso, E.; Wagstaff, A. The Economic Costs of Stunting and How to Reduce Them. 2016. Available online: http://pubdocs.worldbank.org/en/536661487971403516/PRN05-March2017-Economic-Costs-of-Stunting.pdf (accessed on 8 November 2017).
- Onis, M.; Dewey, K.G.; Borghi, E.; Onyango, A.W.; Blössner, M.; Daelmans, B.; Piwoz, E.; Branca, F. The world health organization’s global target for reducing childhood stunting by 2025: Rationale and proposed actions. Matern. Child Nutr. 2013, 9, 6–26. [Google Scholar] [CrossRef] [PubMed]
- Shekar, M.; Kakietek, J.; D’Alimonte, M.R.; Rogers, H.E.; Eberwein, J.D.; Akuoku, J.K.; Pereira, A.; Soe-Lin, S.; Hecht, R. Reaching the global target to reduce stunting: An investment framework. Health Policy Plan. 2017, 32, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Andrews, K.G.; Sudfeld, C.R.; Fink, G.; McCoy, D.C.; Peet, E.; Sania, A.; Fawzi, M.C.S.; Ezzati, M.; Fawzi, W.W. Risk factors for childhood stunting in 137 developing countries: A comparative risk assessment analysis at global, regional, and country levels. PLoS Med. 2016, 13, e1002164. [Google Scholar] [CrossRef] [PubMed]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Goldizen, F.C.; Sly, P.D.; Knibbs, L.D. Respiratory effects of air pollution on children. Pediatr. Pulmonol. 2016, 51, 94–108. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.; Franchini, M. Health effects of ambient air pollution in developing countries. Int. J. Environ. Res. Public Health 2017, 14, 1048. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Parker, J.; Bell, M.L.; Bonzini, M.; Brauer, M.; Darrow, L.A.; Gehring, U.; Glinianaia, S.V.; Gouveia, N.; Ha, E.H. Maternal exposure to particulate air pollution and term birth weight: A multi-country evaluation of effect and heterogeneity. Environ. Health Perspect. 2013, 121, 267–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischer, N.L.; Merialdi, M.; van Donkelaar, A.; Vadillo-Ortega, F.; Martin, R.V.; Betran, A.P.; Souza, J.P.; O’Neill, M.S. Outdoor air pollution, preterm birth, and low birth weight: Analysis of the world health organization global survey on maternal and perinatal health. Environ. Health Perspect. 2014, 122, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Rich, D.Q.; Liu, K.; Zhang, J.; Thurston, S.W.; Stevens, T.P.; Pan, Y.; Kane, C.; Weinberger, B.; Ohman-Strickland, P.; Woodruff, T.J. Differences in birth weight associated with the 2008 Beijing Olympics air pollution reduction: Results from a natural experiment. Environ. Health Perspect. 2015, 123, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Aryastami, N.K.; Shankar, A.; Kusumawardani, N.; Besral, B.; Jahari, A.B.; Achadi, E. Low birth weight was the most dominant predictor associated with stunting among children aged 12–23 months in Indonesia. BMC Nutr. 2017, 3, 16. [Google Scholar] [CrossRef]
- Rahman, M.S.; Howlader, T.; Masud, M.S.; Rahman, M.L. Association of low-birth weight with malnutrition in children under five years in Bangladesh: Do mother’s education, socio-economic status, and birth interval matter? PLoS ONE 2016, 11, e0157814. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, A.; Khan, A.; Yusuf, S.; Adams, A. Trends and determinants of inequities in childhood stunting in Bangladesh from 1996/7 to 2014. Int. J. Equity Health 2016, 15, 186. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.; Alexandre, N.; Cohen, S.; Jao, P.; Khusainova, E.; Mosteller, D.; Peng, Y.; Rosengarten, C.; Schwartz, J.D.; Spawn, A.; et al. 2016 Environmental Performance Index; Yale University: New Haven, CT, USA, 2016; Available online: http://epi.yale.edu/sites/default/files/2016EPI_Full_Report_opt.pdf (accessed on 8 November 2017).
- Mehta, S.; Shin, H.; Burnett, R.; North, T.; Cohen, A.J. Ambient particulate air pollution and acute lower respiratory infections: A systematic review and implications for estimating the global burden of disease. Air Qual. Atmos. Health 2013, 6, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Hsu, N.C.; Kahn, R.A.; Levy, R.C.; Lyapustin, A.; Sayer, A.M.; Winker, D.M. Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 2016, 50, 3762–3772. [Google Scholar] [CrossRef] [PubMed]
- Alam, G. Environmental Pollution of Bangladesh—It’s Effect and Control. Available online: http://www.bangladeshenvironment.com/index.php/polution-s/294-environmental-pollution-of-bangladesh-it-s-effect-and-control (accessed on 8 November 2017).
- Darain, K.; Rahman, A.; Ahsan, A.; Islam, A.; Yusuf, B. Brick manufacturing practice in Bangladesh: A review of energy efficacy and air pollution scenarios. J. Hydrol. Environ. Res. 2013, 1, 60–69. [Google Scholar]
- Smith, K.R.; Bruce, N.; Balakrishnan, K.; Adair-Rohani, H.; Balmes, J.; Chafe, Z.; Dherani, M.; Hosgood, H.D.; Mehta, S.; Pope, D.; et al. Millions dead: How do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. In Annual Review of Public Health; Fielding, J.E., Ed.; Annual Reviews: Palo Alto, CA, USA, 2014; Volume 35, pp. 185–206. [Google Scholar]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2013, 380, 2224–2260. [Google Scholar] [CrossRef]
- Heinrich, J.; Slama, R. Fine particles, a major threat to children. Int. J. Hyg. Environ. Health 2007, 210, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Dunea, D.; Iordache, S.; Pohoata, A. Fine particulate matter in urban environments: A trigger of respiratory symptoms in sensitive children. Int. J. Environ. Res. Public Health 2016, 13, 1246. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Rutstein, S.O.; Rojas, G. Guide to DHS Statistics; ORC Macro: Calverton, MD, USA, 2006. [Google Scholar]
- Corsi, D.J.; Neuman, M.; Finlay, J.E.; Subramanian, S.V. Demographic and health surveys: A profile. Int. J. Epidemiol. 2012, 41, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Perez-Haydrich, C.; Warren, J.L.; Burgert, C.R.; Emch, M.E. Guidelines on the Use of DHS GPS Data; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Dey, S.; Di Girolamo, L.; van Donkelaar, A.; Tripathi, S.N.; Gupta, T.; Mohan, M. Variability of outdoor fine particulate (PM2.5) concentration in the Indian Subcontinent: A remote sensing approach. Remote Sens. Environ. 2012, 127, 153–161. [Google Scholar] [CrossRef]
- Brauer, M.; Freedman, G.; Frostad, J.; van Donkelaar, A.; Martin, R.V.; Dentener, F.; van Dingenen, R.; Estep, K.; Amini, H.; Apte, J.S.; et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ. Sci. Technol. 2016, 50, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Assaf, S.; Kothari, M.T.; Pullum, T.W. An Assessment of the Quality of DHS Anthropometric Data, 2005–2014; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Jedrychowski, W.A.; Perera, F.P.; Maugeri, U.; Mroz, E.; Klimaszewska-Rembiasz, M.; Flak, E.; Edwards, S.; Spengler, J.D. Effect of prenatal exposure to fine particulate matter on ventilatory lung function of preschool children of non-smoking mothers. Paediatr. Perinat. Epidemiol. 2010, 24, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Fussell, J.C. Size, source and chemical composition as determinants of toxicity attributable to ambient particulate matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Šrám, R.J.; Binková, B.; Dejmek, J.; Bobak, M. Ambient air pollution and pregnancy outcomes: A review of the literature. Environ. Health Perspect. 2005, 113, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; Gehring, U.; Beelen, R.; Wang, M.; Giorgis-Allemand, L.; Andersen, A.-M.N.; Basagana, X.; Bernard, C.; Cirach, M.; Forastiere, F.; et al. Elemental constituents of particulate matter and newborn’s size in eight european cohorts. Environ. Health Perspect. 2016, 124, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Boys, B.L. Use of satellite observations for long-term exposure assessment of global concentrations of fine particulate matter. Environ. Health Perspect. 2015, 123, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Elkies, N.; Fink, G.; Bärnighausen, T. “Scrambling” geo-referenced data to protect privacy induces bias in distance estimation. Popul. Environ. 2015, 37, 83–98. [Google Scholar] [CrossRef]
- Cohen, A.J.; Anderson, H.R.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Kunzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health A 2005, 68, 1301–1307. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yu, L.Y.; Mu, H.J.; Xing, L.Y.; Li, Y.X.; Pan, G.W. Shape of concentration-response curves between long-term particulate matter exposure and morbidities of chronic bronchitis: A review of epidemiological evidence. J. Thorac. Dis. 2014, 6, S720–S727. [Google Scholar] [PubMed]
- Burnett, R.T.; Pope, C.A.; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Finlay, J.E.; Özaltin, E.; Canning, D. The association of maternal age with infant mortality, child anthropometric failure, diarrhoea and anaemia for first births: Evidence from 55 low- and middle-income countries. BMJ Open 2011, 1, e000226. [Google Scholar] [CrossRef] [PubMed]
- Balabanova, D.; Mills, A.; Conteh, L.; Akkazieva, B.; Banteyerga, H.; Dash, U.; Gilson, L.; Harmer, A.; Ibraimova, A.; Islam, Z. Good health at low cost 25 years on: Lessons for the future of health systems strengthening. Lancet 2013, 381, 2118–2133. [Google Scholar] [CrossRef]
- Global Administrative Areas. GADM Database of Global Administrative Areas, Version 2.8. 2015. Available online: http://www.gadm.org/ (accessed on 8 November 2017).
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Naz, S.; Page, A.; Agho, K. Household air pollution and under-five mortality in Bangladesh (2004–2011). Int. J. Environ. Res. Public Health 2015, 12, 12847–12862. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.; Retherford, R.D. Does biofuel smoke contribute to anaemia and stunting in early childhood? Int. J. Epidemiol. 2007, 36, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Kyu, H.H.; Georgiades, K.; Boyle, M.H. Maternal smoking, biofuel smoke exposure and child height-for-age in seven developing countries. Int. J. Epidemiol. 2009, 38, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Mauderly, J.L.; Burnett, R.T.; Castillejos, M.; Ozkaynak, H.; Samet, J.M.; Stieb, D.M.; Vedal, S.; Wyzga, R.E. Is the air pollution health research community prepared to support a multipollutant air quality management framework? Inhal. Toxicol. 2010, 22, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Maugeri, U.; Jedrychowska-Bianchi, I. Body growth rate in preadolescent children and outdoor air quality. Environ. Res. 2002, 90, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Bobak, M.; Richards, M.; Wadsworth, M. Relation between children’s height and outdoor air pollution from coal-burning sources in the British 1946 birth cohort. Int. Arch. Occup. Environ. Health 2004, 77, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zeger, S.; Breysse, P.; Katz, J.; Checkley, W.; Curriero, F.C.; Tielsch, J.M. Estimating indoor PM2.5 and CO concentrations in households in Southern Nepal: The Nepal cookstove intervention trials. PLoS ONE 2016, 11, e0157984. [Google Scholar] [CrossRef] [PubMed]
- Bangladesh—Demographic and Health Survey 2014. Available online: https://dhsprogram.com/pubs/pdf/FR311/FR311.pdf (accessed on 8 November 2017).




{kind=link}
{kind=link}
{kind=link}
| Variable | N | BDHS 2004 | BDHS 2007 | BDHS 2011 | BDHS 2014 | Total |
|---|---|---|---|---|---|---|
| Outcome | ||||||
| Stunting | 23,187 | 0.43 | 0.36 | 0.35 | 0.30 | 0.36 |
| Wasting | 23,188 | 0.13 | 0.16 | 0.15 | 0.13 | 0.14 |
| Underweight | 23,187 | 0.47 | 0.46 | 0.43 | 0.40 | 0.44 |
| Small birth size | 11,870 | - | - | 0.18 | 0.19 | 0.18 |
| In utero PM2.5 (µg/m3) | ||||||
| 19.6–40.2 µg/m3 | 6617 | 0.40 | 0.25 | 0.21 | 0.17 | 0.25 |
| 40.3–45.8 µg/m3 | 6593 | 0.26 | 0.27 | 0.26 | 0.21 | 0.25 |
| 45.9–51.9 µg/m3 | 6512 | 0.22 | 0.26 | 0.26 | 0.26 | 0.25 |
| 52.0–72.9 µg/m3 | 6614 | 0.12 | 0.22 | 0.27 | 0.37 | 0.25 |
| Variable, Outcome | Stunting | Wasting | Underweight | Small Birth Size |
|---|---|---|---|---|
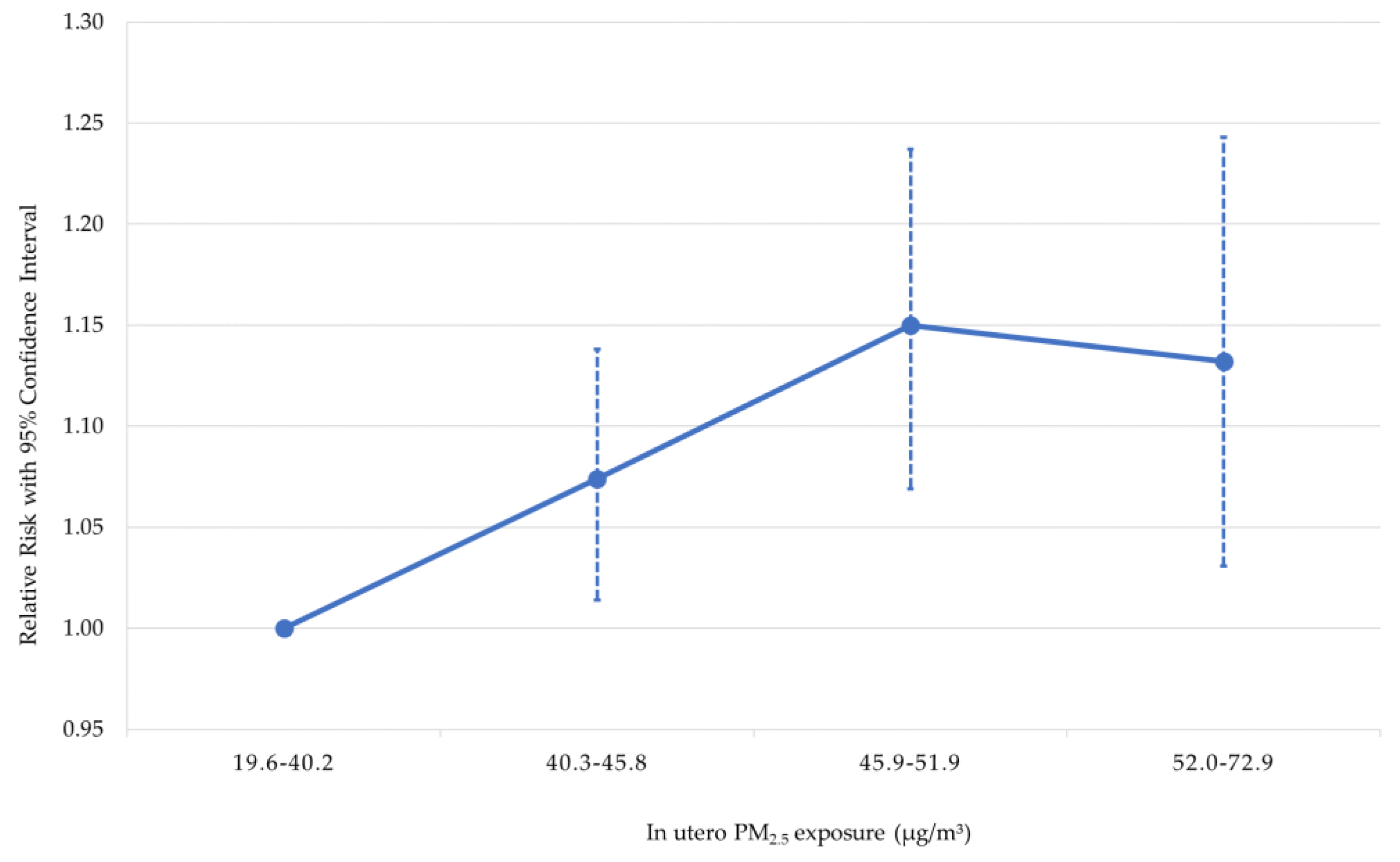
| PM2.5 exposure in utero, 40.3–45.8 µg/m3 | 1.074 [1.014, 1.138] | 1.109 [0.990, 1.243] | 1.118 [1.063,1.176] | 1.040 [0.879, 1.230] |
| PM2.5 exposure in utero, 45.9–51.9 µg/m3 | 1.150 [1.069, 1.237] | 1.247 [1.082, 1.437] | 1.156 [1.087, 1.231] | 1.100 [0.906, 1.335] |
| PM2.5 exposure in utero, 52.0–72.9 µg/m3 | 1.132 [1.031, 1.243] | 1.272 [1.069, 1.512] | 1.127 [1.041, 1.220] | 1.209 [0.965, 1.516] |
| Age of child (months) | 1.013 [1.012, 1.014] | 1.002 [1.000, 1.004] | 1.011 [1.010, 1.012] | - |
| Twin or triplet | 1.615 [1.424, 1.831] | 0.957 [0.659, 1.390] | 1.500 [1.339, 1.679] | 2.205 [1.720, 2.827] |
| Female | 1.048 [1.014, 1.083] | 1.017 [0.955, 1.083] | 1.092 [1.062, 1.123] | 1.188 [1.105, 1.278] |
| First child | 0.968 [0.918, 1.021] | 0.895 [0.812, 0.986] | 0.966 [0.925, 1.009] | 1.171 [1.048, 1.309] |
| Birth interval < 12 months | 1.113 [0.896, 1.383] | 0.779 [0.460, 1.320] | 0.957 [0.775, 1.182] | 0.904 [0.481, 1.699] |
| Birth interval 12–23 months | 1.146 [1.090, 1.205] | 0.921 [0.819, 1.036] | 1.097 [1.048, 1.148] | 1.015 [0.867, 1.188] |
| Had diarrhea in last two weeks | 1.121 [1.054, 1.192] | 1.397 [1.251, 1.559] | 1.180 [1.122, 1.242] | - |
| Maternal height < 160 cm | 2.115 [1.819, 2.459] | 1.105 [0.925, 1.319] | 1.605 [1.446, 1.782] | 1.215 [0.986, 1.498] |
| Maternal body mass index < 18.5 kg/m2 | 1.178 [1.137, 1.220] | 1.608 [1.501, 1.723] | 1.325 [1.286, 1.365] | 1.109 [1.018, 1.209] |
| Age of mother at birth < 18 years | 1.153 [1.086, 1.224] | 1.122 [1.004, 1.254] | 1.110 [1.057, 1.165] | 1.164 [1.020, 1.329] |
| Age of mother at birth 18–19 years | 1.040 [0.987, 1.096] | 1.036 [0.932, 1.151] | 1.020 [0.973, 1.069] | 0.946 [0.829, 1.080] |
| Mother completed primary school | 0.993 [0.953, 1.036] | 1.041 [0.954, 1.136] | 1.002 [0.966, 1.040] | 0.902 [0.803, 1.012] |
| Mother completed secondary school | 0.913 [0.864, 0.965] | 0.922 [0.830, 1.024] | 0.927 [0.885, 0.970] | 0.835 [0.729, 0.956] |
| Mother completed tertiary level | 0.704 [0.608, 0.815] | 0.859 [0.704, 1.048] | 0.745 [0.666, 0.833] | 0.661 [0.520, 0.839] |
| Partner completed primary school | 0.975 [0.936, 1.016] | 1.045 [0.963, 1.134] | 0.995 [0.960, 1.031] | 0.941 [0.847, 1.047] |
| Partner completed secondary school | 0.855 [0.809, 0.903] | 1.062 [0.967, 1.166] | 0.940 [0.899, 0.982] | 0.888 [0.784, 1.006] |
| Partner completed tertiary level | 0.688 [0.619, 0.764] | 1.001 [0.857, 1.171] | 0.818 [0.753, 0.888] | 0.877 [0.725, 1.061] |
| Improved water source in household | 0.950 [0.869, 1.039] | 0.965 [0.812, 1.147] | 0.946 [0.875, 1.022] | 0.785 [0.623, 0.990] |
| Improved sanitation in household | 0.958 [0.920, 0.998] | 1.001 [0.930, 1.076] | 0.967 [0.934, 1.000] | 0.924 [0.843, 1.012] |
| Cooking with solid fuel | 1.045 [0.949, 1.151] | 0.948 [0.811, 1.107] | 1.074 [0.990, 1.167] | 1.053 [0.877, 1.264] |
| Urban residence | 1.041 [0.990, 1.095] | 0.934 [0.855, 1.020] | 1.025 [0.984, 1.068] | 1.102 [0.991, 1.225] |
| Wealth index quintile: poor | 0.886 [0.846, 0.928] | 0.978 [0.891, 1.073] | 0.936 [0.901, 0.972] | 0.946 [0.838, 1.069] |
| Wealth index quintile: middle | 0.847 [0.804, 0.892] | 0.886 [0.799, 0.982] | 0.866 [0.828, 0.905] | 0.921 [0.806, 1.052] |
| Wealth index quintile: rich | 0.761 [0.715, 0.809] | 0.811 [0.718, 0.916] | 0.795 [0.754, 0.840] | 0.853 [0.737, 0.987] |
| Wealth index quintile: richest | 0.555 [0.506, 0.609] | 0.789 [0.675, 0.923] | 0.636 [0.589, 0.687] | 0.872 [0.720, 1.056] |
| Survey fixed effect: 2007 wave | 0.821 [0.777, 0.868] | 1.220 [1.096, 1.357] | 0.962 [0.916, 1.010] | - |
| Survey fixed effect: 2011 wave | 0.835 [0.791, 0.882] | 1.180 [1.060, 1.313] | 0.938 [0.895, 0.982] | - |
| Survey fixed effect: 2014 wave | 0.757 [0.712, 0.805] | 1.076 [0.960, 1.207] | 0.900 [0.854, 0.948] | 1.118 [1.026, 1.218] |
| District fixed effects | Yes | Yes | Yes | Yes |
| N | 23,187 | 23,188 | 23,187 | 11,870 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goyal, N.; Canning, D. Exposure to Ambient Fine Particulate Air Pollution in Utero as a Risk Factor for Child Stunting in Bangladesh. Int. J. Environ. Res. Public Health 2018, 15, 22. https://doi.org/10.3390/ijerph15010022
Goyal N, Canning D. Exposure to Ambient Fine Particulate Air Pollution in Utero as a Risk Factor for Child Stunting in Bangladesh. International Journal of Environmental Research and Public Health. 2018; 15(1):22. https://doi.org/10.3390/ijerph15010022
Chicago/Turabian StyleGoyal, Nihit, and David Canning. 2018. "Exposure to Ambient Fine Particulate Air Pollution in Utero as a Risk Factor for Child Stunting in Bangladesh" International Journal of Environmental Research and Public Health 15, no. 1: 22. https://doi.org/10.3390/ijerph15010022