
Investigating Discontinuity of Age Relations in Cognitive Functioning, General Health Status, Activity Participation, and Life Satisfaction between Young-Old and Old-Old Age

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.2.1. Cognitive Abilities
2.2.2. General Health Status
2.2.3. Activity Participation
2.2.4. Life Satisfaction
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.2. Examining the Pattern of Age Relations across Old Age
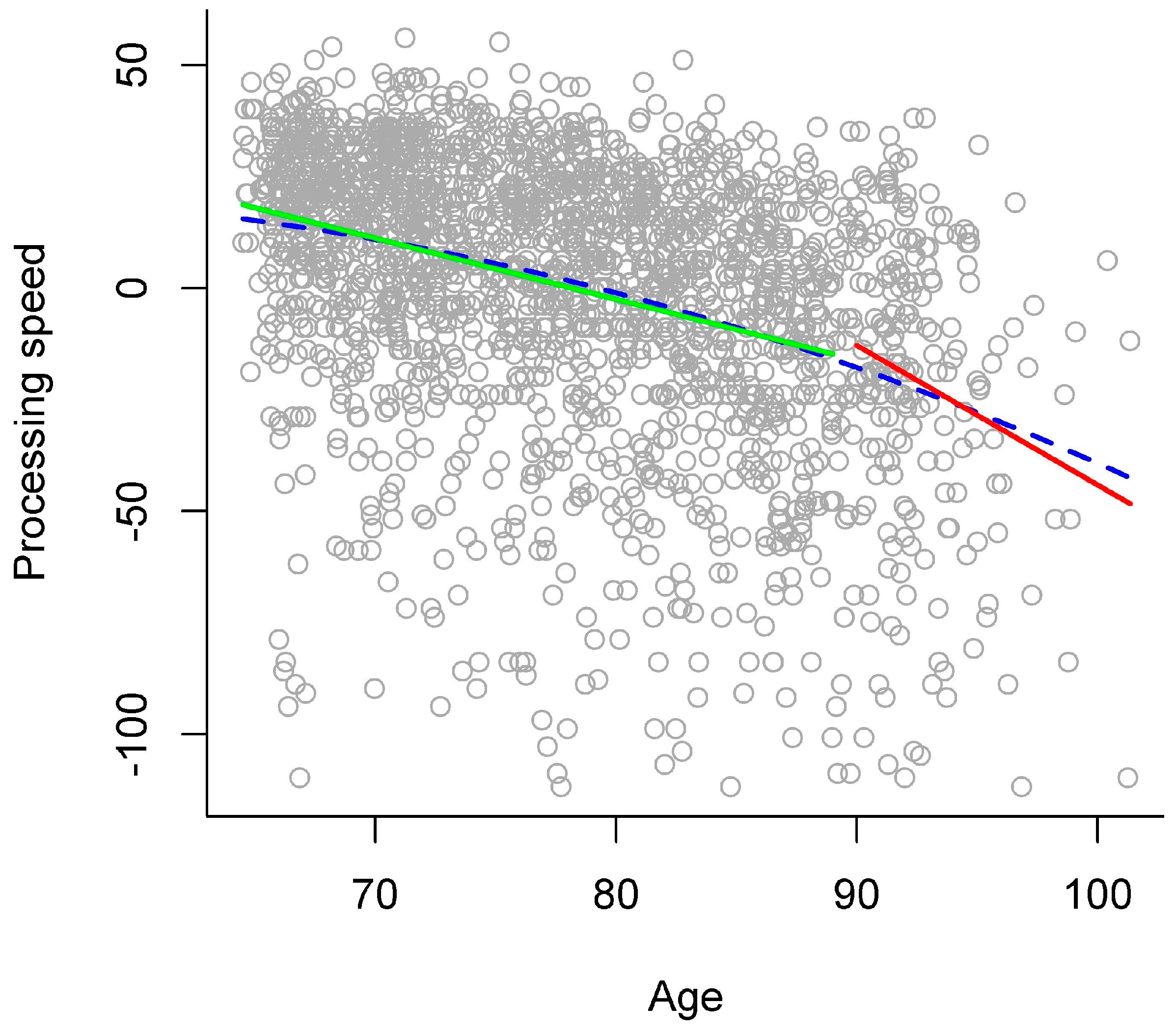
3.2.1. Processing Speed
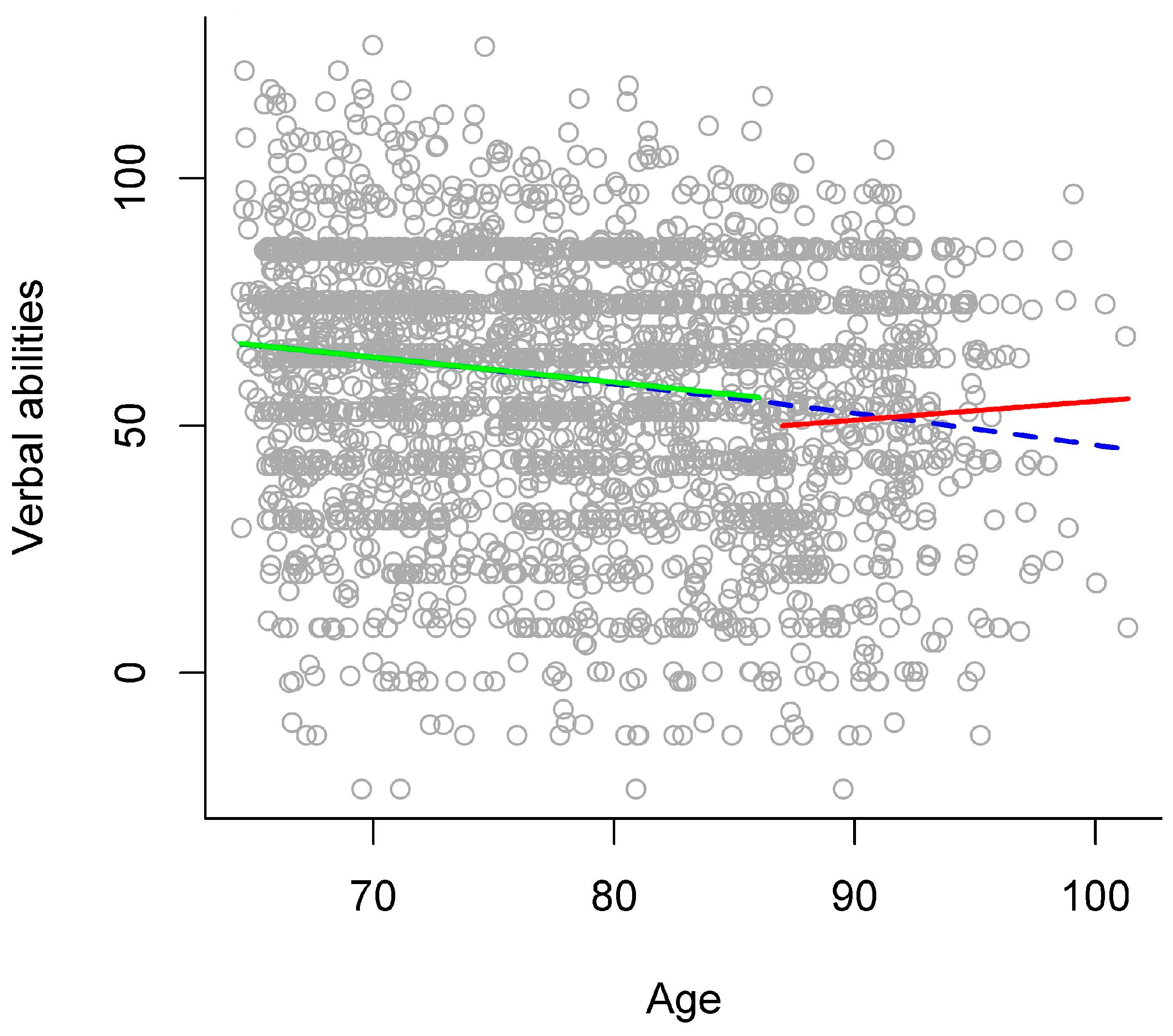
3.2.2. Verbal Abilities
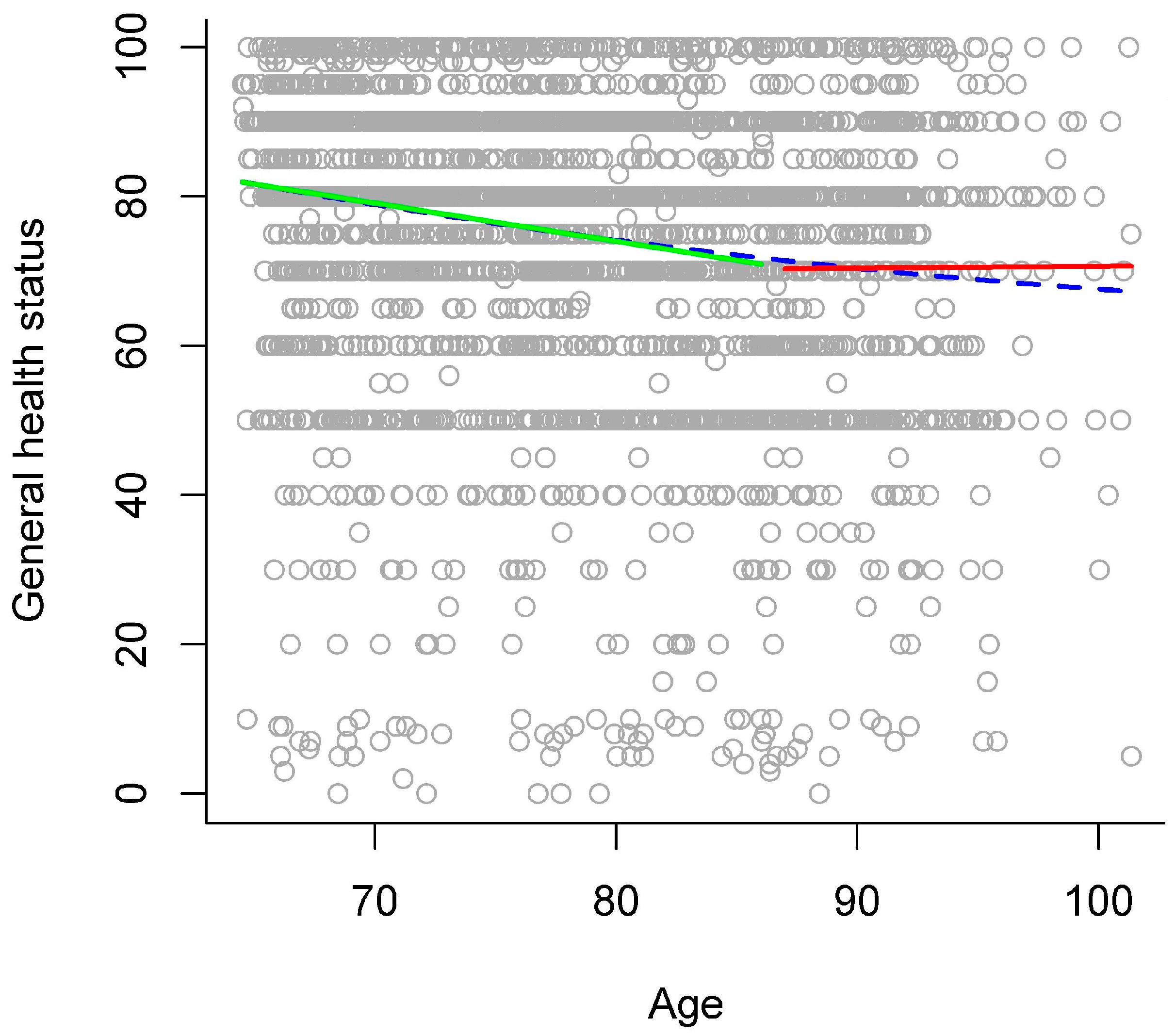
3.2.3. General Health Status
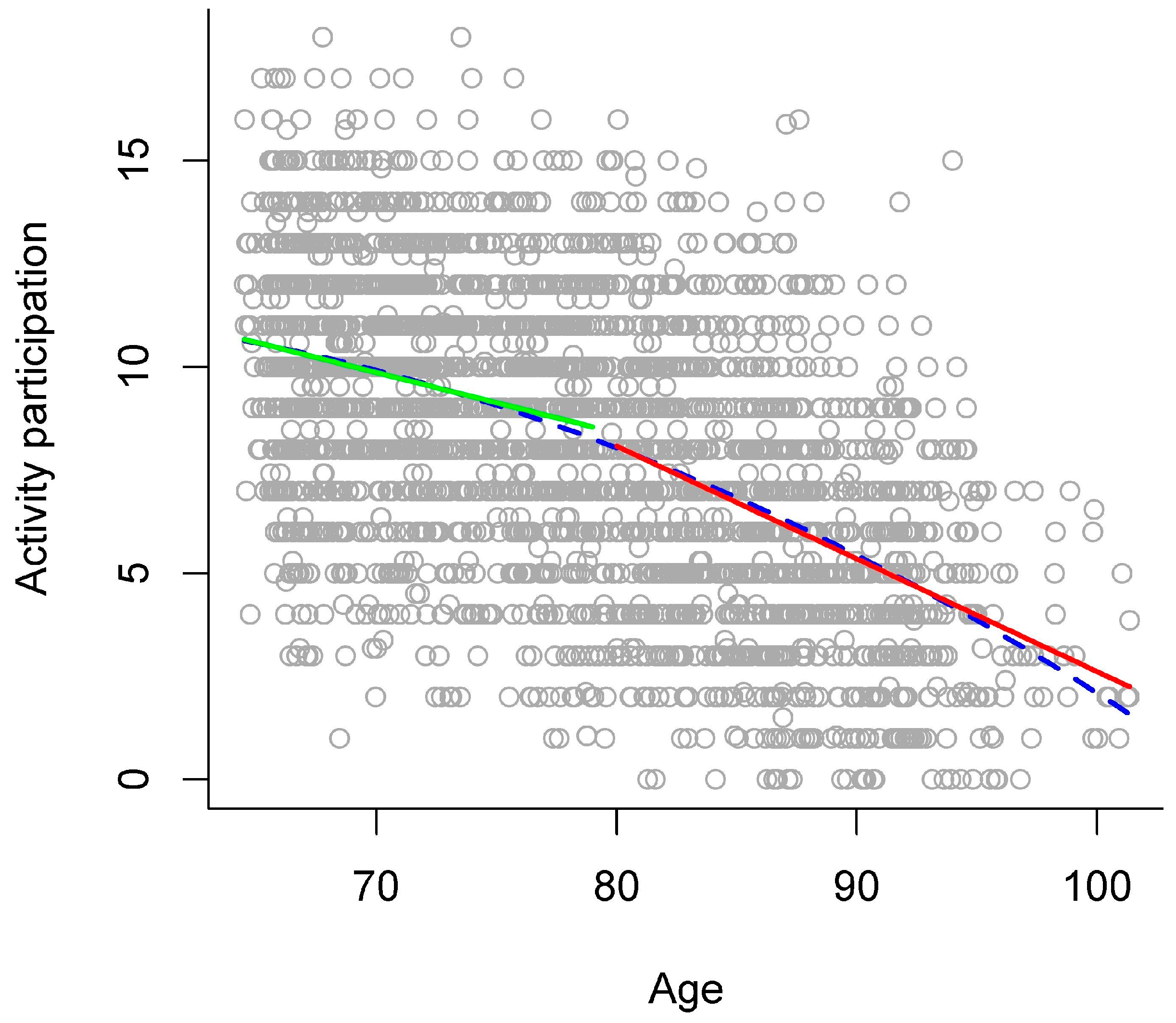
3.2.4. Activity Participation
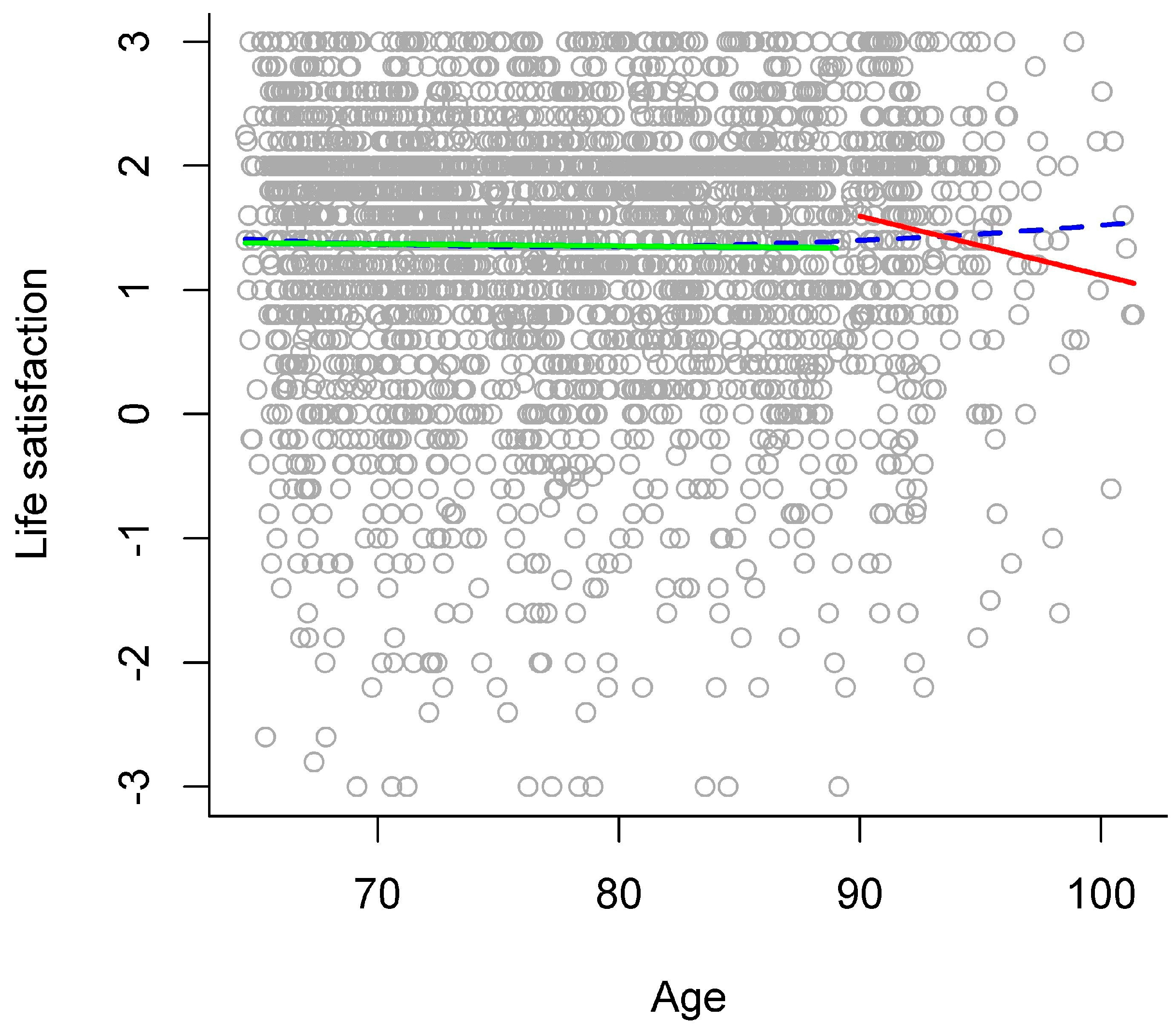
3.2.5. Life Satisfaction
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Baltes, M.M. The psychology of the oldest-old: The fourth age. Curr. Opin. Psychiatry 1998, 11, 411–415. [Google Scholar] [CrossRef]
- Baltes, P.B.; Smith, J. New frontiers in the future of aging: From successful aging of the young old to the dilemmas of the fourth age. Gerontology 2003, 49, 123–135. [Google Scholar] [CrossRef]
- Paggi, M.E.; Jopp, D.; Hertzog, C. The importance of leisure activities in the relationship between physical health and well-being in a life span sample. Gerontology 2016, 62, 450–458. [Google Scholar] [CrossRef]
- Baltes, P.B. On the incomplete architecture of human ontogeny—Selection, optimization, and compensation as foundation of developmental theory. Am. Psychol. 1997, 52, 366–380. [Google Scholar] [CrossRef]
- McGinnis, D. Susceptibility to Distraction during Reading in Young, Young-Old, and Old-Old Adults. Exp. Aging Res. 2012, 38, 370–393. [Google Scholar] [CrossRef]
- Singer, T.; Lindenberger, U.; Baltes, P.B. Plasticity of Memory for New Learning in Very Old Age: A Story of Major Loss? Max Planck Institute for Human Development: Berlin, Germany, 2001. [Google Scholar]
- Wright, A.M.; Holliday, R.E. Enhancing the recall of young, young-old and old-old adults with cognitive interviews. Appl. Cogn. Psychol. 2007, 21, 19–43. [Google Scholar] [CrossRef]
- Ebly, E.M.; Parhad, I.M.; Hogan, D.B.; Fung, T.S. Prevalence and Types of Dementia in the Very Old—Results from the Canadian-Study-of-Health-and-Aging. Neurology 1994, 44, 1593–1600. [Google Scholar] [CrossRef]
- Brumback-Peltz, C.; Balasubramanian, A.B.; Corrada, M.M.; Kawas, C.H. Diagnosing dementia in the oldest-old. Maturitas 2011, 70, 164–168. [Google Scholar] [CrossRef]
- Adams, K.B.; Roberts, A.R.; Cole, M.B. Changes in Activity and Interest in the Third and Fourth Age: Associations with Health, Functioning and Depressive Symptoms. Occup. Ther. Int. 2011, 18, 4–17. [Google Scholar] [CrossRef]
- Higgs, P.; Gilleard, C. Frailty, abjection and the “othering” of the fourth age. Health Sociol. Rev. 2014, 23, 10–19. [Google Scholar] [CrossRef]
- Smith, J.; Baltes, P.B. Profiles of psychological functioning in the old and oldest old. Psychol. Aging 1997, 12, 458–472. [Google Scholar] [CrossRef]
- Olshansky, S.J.; Carnes, B.A.; Desesquelles, A. Demography—Prospects for human longevity. Science 2001, 291, 1491–1492. [Google Scholar] [CrossRef]
- Oris, M.; Lerch, M. La transition ultime. Longévité et mortalité aux grands âges dans le bassin lémanique. In Transitions dans le Parcours de Vie et Construction des Inégalités; Oris, M., Widmer, E., De Ribaupierre, A., Joye, D., Spini, D., Labouvie-Vief, G., Falter, J.M., Eds.; Presses polytechniques et universitaires romandes: Lausanne, Switzerland, 2009; pp. 407–432. [Google Scholar]
- Vaupel, J.W.; Carey, J.R.; Christensen, K.; Johnson, T.E.; Yashin, A.I.; Holm, N.V.; Iachine, I.A.; Kannisto, V.; Khazaeli, A.A.; Liedo, P.; et al. Biodemographic trajectories of longevity. Science 1998, 280, 855–860. [Google Scholar] [CrossRef]
- Abdel-Ghany, M.; Sharpe, D.L. Consumption patterns among the young-old and old-old. J. Consum. Aff. 1997, 31, 90–112. [Google Scholar] [CrossRef]
- Alterovitz, S.S.R.; Mendelsohn, G.A. Relationship goals of middle-aged, young-old, and old-old internet daters: An analysis of online personal ads. J. Aging Stud. 2013, 27, 159–165. [Google Scholar] [CrossRef]
- Gayzur, N.D.; Langley, L.K.; Kelland, C.; Wyman, S.V.; Saville, A.L.; Ciernia, A.T.; Padmanabhan, G. Reflexive orienting in response to short- and long-duration gaze cues in young, young-old, and old-old adults. Atten. Percept. Psychophys. 2014, 76, 407–419. [Google Scholar] [CrossRef]
- Yoshimura, K.; Yamada, M.; Kajiwara, Y.; Nishiguchi, S.; Aoyama, T. Relationship between depression and risk of malnutrition among community-dwelling young-old and old-old elderly people. Aging Ment. Health 2013, 17, 456–460. [Google Scholar] [CrossRef] [Green Version]
- Ansah, J.P.; Malhotra, R.; Lew, N.; Chiu, C.T.; Chan, A.; Bayer, S.; Matchar, D.B. Projection of young-old and old-old with functional disability: Does accounting for the changing educational composition of the elderly population make a difference? PLoS ONE 2015. [Google Scholar] [CrossRef]
- Bodner, E.; Palgi, Y.; Kaveh, D. Does the Relationship Between Affect Complexity and Self-Esteem Differ in Young-Old and Old-Old Participants? J. Gerontol. B Psychol. Sci. Soc. Sci. 2013, 68, 665–673. [Google Scholar] [CrossRef]
- Kliegel, M.; Jäger, T. Delayed-execute prospective memory performance: The effects of age and working memory. Dev. Neuropsychol. 2006, 30, 819–843. [Google Scholar] [CrossRef]
- Menec, V.H.; Chipperfield, J.G. The interactive effect of perceived control and functional status on health and mortality among young-old and old-old adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 1997, 52, 118–126. [Google Scholar] [CrossRef]
- Zinke, K.; Zeintl, M.; Rose, N.S.; Putzmann, J.; Pydde, A.; Kliegel, M. Working Memory Training and Transfer in Older Adults: Effects of Age, Baseline Performance, and Training Gains. Dev. Psychol. 2014, 50, 304–315. [Google Scholar] [CrossRef]
- Calero, M.D.; Perez-Diaz, A.G.L.; Gonzalez, E.N.; Calero-Garcia, M.J. Cognitive plasticity, cognitive functioning and quality of life (QoL) in a sample of young-old and old-old adults in southern Spain. Aging Clin. Exp. Res. 2013, 25, 35–42. [Google Scholar] [CrossRef]
- Wu, Y.J.; Shi, Z.Y.; Wang, M.J.; Zhu, Y.B.; Li, C.; Li, G.D.; Marcantonio, E.R.; Xie, Z.C.; Shen, Y. Different MMSE score is associated with postoperative delirium in young-old and old-old Adults. PLoS ONE 2015. [Google Scholar] [CrossRef]
- Buch, K.B.N.; Padberg, F.; Nolde, T.; Teipel, S.J.; Stubner, S.; Haslinger, A.; Schwarz, M.J.; Sunderland, T.; Arai, H.; Rapoport, S.I.; et al. Cerebrospinal fluid tau protein shows a better discrimination in young old (<70 years) than in old old patients with Alzheimer’s disease compared with controls. Neurosci. Lett. 1999, 277, 21–24. [Google Scholar]
- Kvavilashvili, L.; Cockburn, J.; Kornbrot, D.E. Prospective memory and ageing paradox with event-based tasks: A study of young, young-old, and old-old participants. Q. J. Exp. Psychol. 2013, 66, 864–875. [Google Scholar] [CrossRef] [Green Version]
- Gavazzi, G.; Mallaret, M.R.; Couturier, P.; Iffenecker, A.; Franco, A. Bloodstream infection: Differences between young-old, old, and old-old patients. J. Am. Geriatr. Soc. 2002, 50, 1667–1673. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Atkinson, T.M.; Berish, D.E. Executive functioning as a potential mediator of age-related cognitive decline in normal adults. J. Exp. Psychol. Gen. 2003, 132, 566–594. [Google Scholar] [CrossRef]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef]
- Schaie, K.W. The course of adult intellectual-development. Am. Psychol. 1994, 49, 304–313. [Google Scholar] [CrossRef]
- Gana, K.; Bailly, N.; Saada, Y.; Joulain, M.; Alaphilippe, D. Does life satisfaction change in old age: Results from an 8-year longitudinal study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2013, 68, 540–552. [Google Scholar] [CrossRef]
- Karp, A.; Paillard-Borg, S.; Wang, H.X.; Silverstein, M.; Winblad, B.; Fratiglioni, L. Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dement. Geriatr. Cogn. Disord. 2006, 21, 65–73. [Google Scholar] [CrossRef]
- Tolppanen, A.M.; Solomon, A.; Kulmala, J.; Kareholt, I.; Ngandu, T.; Rusanen, M.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Leisure-time physical activity from mid- to late life, body mass index, and risk of dementia. Alzheimers Dement. 2015, 11, 434–443. [Google Scholar] [CrossRef]
- Gerstorf, D.; Ram, N.; Estabrook, R.; Schupp, J.; Wagner, G.G.; Lindenberger, U. Life satisfaction shows terminal decline in old age: Longitudinal evidence from the german socio-economic panel study (soep). Dev. Psychol. 2008, 44, 1148–1159. [Google Scholar] [CrossRef]
- Carmel, S.; Shrira, A.; Shmotkin, D. The will to live and death-related decline in life satisfaction. Psychol. Aging 2013, 28, 1115–1123. [Google Scholar] [CrossRef]
- Reitan, R.M. Validity of the trail making test as an indicator of organic brain damage. Percept. Mot. Skills 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Deltour, J. Echelle de Vocabulaire Mill Hill de J. C. Raven. (Raven Mill Hill Vocabulary Scale); Editions L’application des techniques modernes: Braine-le Chateau, Belgium, 1993. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Hultsch, D.F.; Hertzog, C.; Small, B.J.; Dixon, R.A. Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging? Psychol. Aging 1999, 14, 245–263. [Google Scholar] [CrossRef]
- Cheng, S.T.; Fung, H.; Chan, A. Maintaining self-rated health through social comparison in old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, 277–285. [Google Scholar] [CrossRef]
- Deary, I.J.; MacLennan, W.J.; Starr, J.M. Is age kinder to the initially more able?: Differential ageing of a verbal ability in the healthy old people in Edinburgh study. Intelligence 1998, 26, 357–375. [Google Scholar] [CrossRef]
- Kunzmann, U.; Little, T.D.; Smith, J. Is age-related stability of subjective well-being a paradox? Cross-sectional and longitudinal evidence from the Berlin Aging Study. Psychol. Aging 2000, 15, 511–526. [Google Scholar] [CrossRef]
- Ihle, A.; Oris, M.; Fagot, D.; Kliegel, M. No cross-sectional evidence for an increased relation of cognitive and sensory abilities in old age. Aging Ment. Health 2015. [Google Scholar] [CrossRef]
- Rabbitt, P. Does It All Go Together When It Goes – the 19th Bartlett Memorial Lecture. Quart. J. Exp. Psychol. A 1993, 46, 385–434. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stratification Variables | Overall N = 3080 | |
|---|---|---|
| Age group | 65–69: 573 (18.6%) | 70–74: 609 (19.8%) |
| 75–79: 567 (18.4%) | 80–84: 495 (16.1%) | |
| 85–89: 463 (15.0%) | 90+: 373 (12.1%) | |
| Sex | Women: 1485 (48.2%) | Men: 1595 (51.8%) |
| Canton | Basel: 636 (20.6%) | Bern: 684 (22.2%) |
| Geneva: 578 (18.8%) | Ticino: 606 (19.7%) | |
| Valais: 576 (18.7%) | ||
| Variable | M | SD |
|---|---|---|
| Processing speed (seconds) | 66.20 | 30.61 |
| Verbal abilities (percent correct) | 59.4 | 25.7 |
| General health status (rating 0 to 100) | 75.24 | 20.13 |
| Activities (number) | 8.15 | 3.50 |
| Life satisfaction (rating −3 to +3) | 1.37 | 1.07 |
| Variable | Gradual Model | Stage Model | |||||||
|---|---|---|---|---|---|---|---|---|---|
| blinear | bquadratic | R2 | Age Break | blinear | bagegroup | binteraction | R2 | ΔR2 | |
| Processing speed | 2.35 ns | −0.02 * | 0.14 *** | 90 | −3.13 *** | 22.83 *** | 1.76 * | 0.14 *** | < 0.001 ns |
| Verbal abilities | −0.15 ns | −0.003 ns | 0.03 *** | 87 | 0.38 ns | 9.99 *** | −0.88 * | 0.03 *** | 0.003 ** (8.1%) |
| General health status | −1.22 ns | 0.005 ns | 0.03 *** | 87 | 0.02 ns | 6.07 *** | −0.53 * | 0.03 *** | 0.001 * (4.0%) |
| Activities | 0.36 ** | −0.004 *** | 0.29 *** | 80 | −0.27 *** | 3.29 *** | 0.12 *** | 0.29 *** | 0.001 * (0.4%) |
| Life satisfaction | −0.06 ns | 0.0004 ns | 0.0006 ns | 90 | −0.05 * | −0.11 ns | 0.05 ns | 0.003 ns | 0.002 * (312.2%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ihle, A.; Jopp, D.S.; Oris, M.; Fagot, D.; Kliegel, M. Investigating Discontinuity of Age Relations in Cognitive Functioning, General Health Status, Activity Participation, and Life Satisfaction between Young-Old and Old-Old Age. Int. J. Environ. Res. Public Health 2016, 13, 1092. https://doi.org/10.3390/ijerph13111092
Ihle A, Jopp DS, Oris M, Fagot D, Kliegel M. Investigating Discontinuity of Age Relations in Cognitive Functioning, General Health Status, Activity Participation, and Life Satisfaction between Young-Old and Old-Old Age. International Journal of Environmental Research and Public Health. 2016; 13(11):1092. https://doi.org/10.3390/ijerph13111092
Chicago/Turabian StyleIhle, Andreas, Daniela S. Jopp, Michel Oris, Delphine Fagot, and Matthias Kliegel. 2016. "Investigating Discontinuity of Age Relations in Cognitive Functioning, General Health Status, Activity Participation, and Life Satisfaction between Young-Old and Old-Old Age" International Journal of Environmental Research and Public Health 13, no. 11: 1092. https://doi.org/10.3390/ijerph13111092