2.1. Study Location and Design
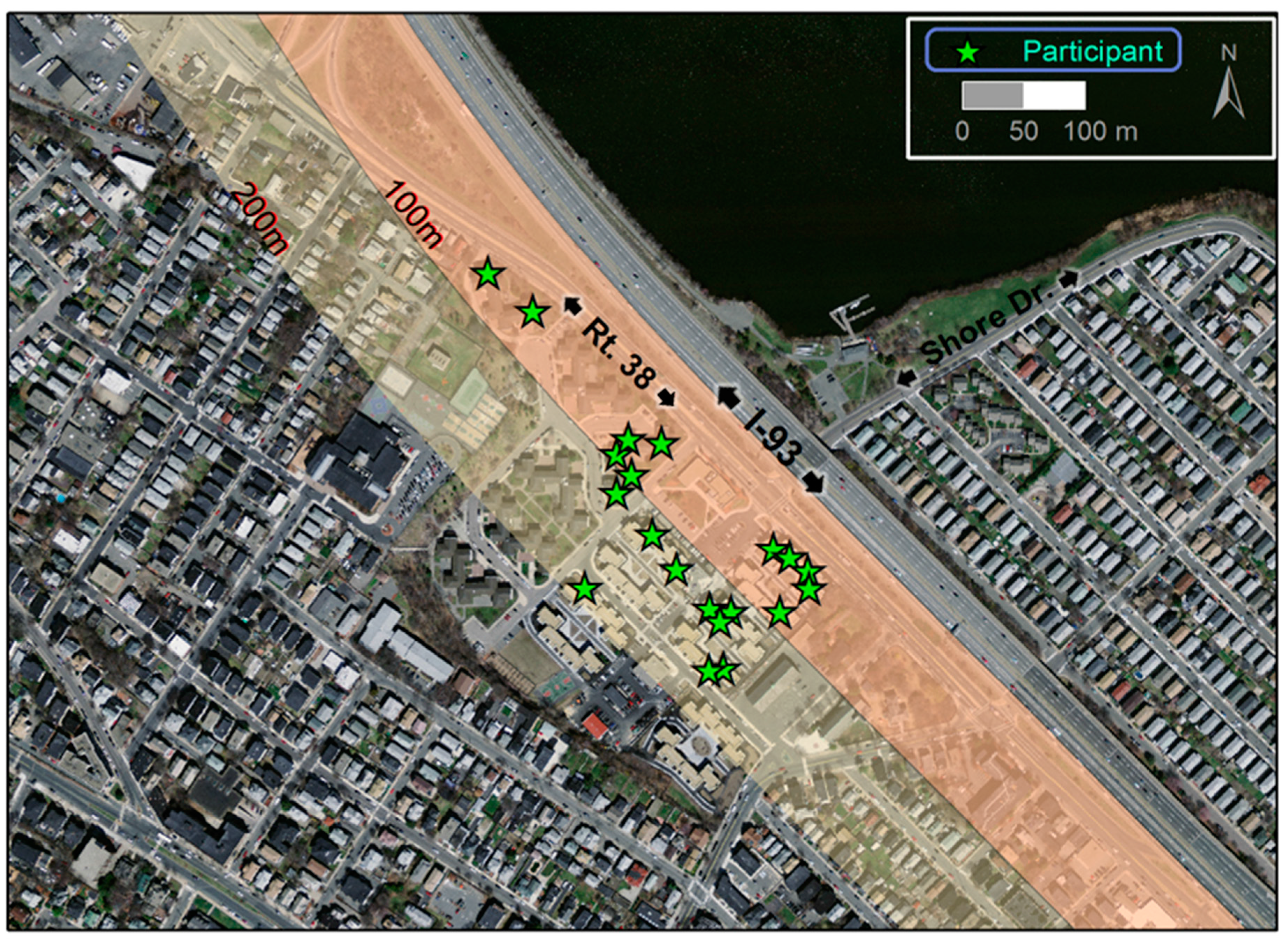
The study was conducted in 20 apartments (21 participants) in the Mystic View and Mystic River housing developments in Somerville. One apartment was excluded from the analysis due to a problem with the air monitoring equipment; thus, our final data set included 19 apartments and 20 participants. The two developments are adjacent to one another as well as to I-93 and Massachusetts State Highway 38 (Rt-38; >30,000 vehicles per day [
38];
Figure 1). I-93 rises to as high as 6-m-above grade next to the developments and is filled underneath except for the underpass at Shore Drive; Rt-38 runs at grade parallel to I-93. Participants were at least 40 years old, did not smoke or allow smoking inside their homes, and their apartments were within 200 m of I-93. Recruitment was in three languages: English, Haitian Creole and Spanish. Details of recruitment and our interaction with the participants are described elsewhere [
42].
Figure 1.
Map of study area and locations of participant apartments. Orthophoto was downloaded from MassGIS [
44].
Figure 1.
Map of study area and locations of participant apartments. Orthophoto was downloaded from MassGIS [
44].
The study design was a randomized, double-blind crossover trial with the goal of having 50% of participants start with HEPA filtration and 50% start with sham filtration. To facilitate scheduling, pairs of participants were studied in parallel with one participant starting with HEPA and the other with sham filtration with assignment randomized. The purpose of randomization was to minimize the effects of temporal variation in PNC and blood biomarker concentrations on the results. Each participant was exposed to HEPA-filtered air for 21 days and unfiltered (sham) air for 21 days. Regardless of which filter was in use (HEPA or sham), the sound and appearance of the equipment was the same; thus, participants did not know which filter was in use. Because each participant was exposed to both filtered and unfiltered air, they served as their own control.
Associations of PNC with CRP and IL-6 have been found for periods from as little as 1 to as many as 28 days in natural exposure [
11,
16] and controlled exposure studies [
17]. We used a 21-day exposure period because it allowed for testing exposure times toward the longer end of what is reported in the literature while also encompassing shorter time frames. In general, longer exposures to air pollution are associated with greater biological effects than are shorter exposures. For blood pressure we focused on shorter time frames, consistent with other studies that have found associations with air pollution in hours to two days [
13,
14,
15].
All participants signed an informed consent form and completed a survey containing questions on demographics, socio-economic status, residential history, time activity, window opening, air conditioner use, potential exposure to combustion sources (at home and work and on highways), and health status. Medication use was obtained by recording the names of medicines found in each apartment. In addition, at the end of the first intervention period and at the end of the study (t = 21 and 42 days, respectively), participants completed supplemental surveys to obtain information on time activity and health status during the preceding week. The time-activity questions obtained hour-by-hour estimates of time spent in five microenvironments—inside home, outside home, school/work, highway travel, and other—on week days and weekend days for unemployed participants and work days and non-work days for employed participants. The consent forms and surveys were forward and back translated and the surveys were conducted by independent translators fluent in both English and the second language. Each participant received stipends for the initial survey, each blood draw, and for electricity use. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Tufts University Institutional Review Board (Protocol #1008078). The study was conducted from February 2011 to November 2012.
2.2. Air Filtration and PNC Monitoring
Each apartment had a kitchen, dining area, living room, and two or three bedrooms. Window-mounted HEPAiRx air filtration units equipped with user-controlled air heating and cooling elements (Air Innovations, Inc., North Syracuse, NY, USA;
http://www.airinnovations.com/) were used in the study because they have been shown to reduce the severity of asthma in children [
33]. These units use a MERV 17 filter (rated to remove ≥99.97% of particles ≥0.3 μm in diameter) and can operate at ~10 exchanges/hour in a <28.3 m
3 (10
3 ft
3) room. The units were installed in the living room of each apartment as opposed to the bedroom because most participants indicated they spent more time each day in their living rooms as well as to minimize potential sleep disruption for participants due to instrument noise. To maximize particle removal, the HEPA units were operated at the highest possible fan speed and the side vents were blocked off so that there was no flow of outdoor air through the unit into the apartment. Filters were changed in each apartment after 21 days (HEPA for sham or vice versa). A new HEPA filter (MERV 17) was used in each apartment. The sham filter, a hollow box made from perforated 1-mm-thick sheet metal, was the same size and shape and had the same appearance as the metal frame around the HEPA filters. A sign was placed on the HEPA-unit cover asking participants (in multiple languages) not to tamper with or expose the filter. While we found no evidence that any of the filters had been tampered with, we cannot completely discount the possibility that some participants did not follow our instructions. Nevertheless, failure of blinding of participants to the filtration regime is of less concern in a study such as ours that has objective health attributes, blood biomarkers and blood pressure in our case, which are not under voluntary control of participants.
The number concentration of particles between 7 and 3000 nm in diameter was measured continuously over the 42-day trial in each apartment using a water-based condensation particle counter (CPC; TSI Model 3783). PNC was measured every second and one-minute averages were recorded. With the exception of apartments 3 and 9, the CPCs were installed in the living room along with the HEPA. Due to space limitations in the living rooms of these two apartments the CPC was installed in the dining rooms, which were immediately adjacent to the living rooms. Before the start of the intervention in each apartment, the air flow rate reported by the CPC was checked using a flow meter (TSI Model 4140) (no discrepancies were observed throughout the study), and the CPC vacuum was checked for leaks by placing a polyethersulfone membrane filter (rated at 99.96% removal efficiency for 0.45 µm particles) on the inlet to insure the CPC measured <100 particles per cm3. PNC data was collected weekly and checked for CPC temperature and flow errors flagged by the instrument. Data points with errors (typically <1% of all data) were removed from the data set. After each 42-day trial, the flow rate in the CPCs was measured again. Side-by-side comparisons of the CPCs performed in the laboratory resulted in an R2 of 0.91 with paired measurements differing by <10%.
Dimensions of the living rooms ranged from 3.1 to 3.9 m in width, from 4.0 to 5.1 m in length, and the ceiling height of all the apartments was 2.4 m. Thus, the total volume of the living rooms was 34.3 to 40.5 m
3. Each apartment had baseboard heaters (forced hot water) and no centralized air cooling system or forced-air ventilation. During the summer some participants installed window-mounted air conditioners (AC) and free-standing fans or opened windows to help cool their apartments. In apartments that had an AC in the living room, the AC was exchanged for a HEPAiRx unit, which also contained an AC, to comply with housing authority rules requiring at least one living room window be freely accessible as an emergency exit. Participants were asked to keep their windows closed during the study and to use the HEPAiRx to provide cooling. With the exception of stove fans, which were present in all of the apartments and vented outdoors, none of the apartments was equipped with additional air cleaning technology beyond the HEPAiRx filter units. Participants were instructed to run the HEPA unit and CPC at all times (24 hours a day, 7 days a week) during the 42-day study period. We found no evidence that participants turned off the HEPA units, an important consideration in long-term HEPA filtration studies [
45].
To better understand the factors affecting PNC reductions by HEPA and sham filtration in participant homes, experiments were performed in an unoccupied bedroom in a Somerville apartment that was >1 km from I-93 and was not in the Mystic View or Mystic River Apartment buildings. The bedroom was 27.8 m
3 (981 ft
3), furnished with a bed, bedside table, desk and chair, and had hardwood floors but no rugs or carpeting. Prior to the experiments the air vent and gaps around the door were sealed. Particle removal efficiencies were measured for three kinds of sources: (1) no source; (2) a continuous, low concentration source (
i.e., bedroom window open 2.8 × 10
3 cm
2 throughout the experiment); and (3) a discrete, high concentration source (
i.e., a burning candle lit for 45 min and then extinguished). Each experiment was performed in triplicate with a HEPA filter and in triplicate with a sham filter. PNC reductions were calculated using Equation (1):
where
PNCHEPA off was the mean PNC during the 30-min period immediately before the HEPA unit was turned on, and
PNCHEPA on was the mean PNC between 10 and 40 min after the HEPA unit was turned on (0–10 min was excluded because the new baseline was not yet reached). The PNC reduction for the candle experiments was calculated based on the change in PNC after the candle was extinguished with the HEPA running continuously.
2.3. Blood Biomarker and Pressure Measurements
Nurses from the Visiting Nurses Association (VNA) of Eastern Massachusetts performed three visits to each participant’s apartment: on day 1 just before HEPA/sham filtration was started, on day 21 1–2 h before the filters were changed, and on day 42 just before the end of the intervention. On the day-1 visit weight and height were recorded using a standard scale (SECA, Model #8761321009) and stadiometer (Model #905055, Shorr Productions LLC, Olney, MD, USA), and blood lipid profile was measured from a finger stick using a CardioChek PA device (Polymer Technology Systems, Inc., Indianapolis, IN, USA). On all three visits diastolic and systolic blood pressure were measured in the right and then left arms of seated participants using an automatic blood pressure machine (Model #HEM711ACN2, Omron Healthcare, Kyoto, Japan). A venous blood sample was collected during each visit and then transported to the Clinical & Epidemiologic Research Laboratory at Boston Children’s Hospital, where it was processed to plasma and stored at minus 80 ºC within 1–3 h of collection. Participants were instructed to fast overnight prior to the blood draws, which occurred between 8 and 10 AM. Samples were assayed in batches using immunoassay kits for hsCRP (SPQ High Sensitivity CRP Reagent Set; DiaSorin, Stillwater, MN, USA), fibrinogen (κ-Assay; Kamiya Biomedical, Seattle, WA, USA), TNF-RII (Quantitative, R&D Systems, Minneapolis, MN, USA) and IL-6 (Quantitative HS, R&D Systems). Quality assurance protocols developed by the lab were used to check the quality of the data. The lab was blinded to the intervention status of the blood samples.
2.4. Data Analysis
For the primary analysis, differences in blood biomarker and blood pressure measurements during exposure to HEPA and sham filtration, independent of filtration order, were assessed with a paired
t-test. In addition, the blood biomarker data was divided into four groups based on the treatment received (HEPA or sham) and the order participants were exposed to each filter, and then compared using generalized estimating equations (GEE) to account for non-independence of measurements [
46]. Blood biomarkers—hsCRP, Fibrinogen, TNF-RII and IL-6—were log transformed (natural log) prior to analysis. Results presented have been back transformed and are reported as percent changes. The GEE analysis was performed using the GENMOD procedure in SAS (v9.3, SAS Institute Inc., Cary, NC, USA) and was checked by a third party check for coding errors (there were none). The least squared means adjusted for baseline are used to report the change in blood biomarker concentrations during each three-week exposure period (either HEPA or sham). A
t-test showed a significant difference between treatment groups for IL-6 (
p = 0.05) at baseline, indicating that randomization for IL-6 was not ideal. Accordingly, we also analyzed IL-6 using a repeated measure analysis.
We conducted exploratory tests of the sensitivity of our results to PNC exposure by analyzing PNC at different exposure times prior to the collection of blood samples and blood pressure measurements. Exposure-time windows included Lag0, Lag1, and Lag2 (i.e., the median of all PNC measurements 0–24, 24–48 and 48–72 h before the biological measurements, respectively), and moving average (MA)3, MA14, and MA21 (i.e., the median of all PNC measurements from 0 to 3, 0 to 14, and 0 to 21 days prior to the biological measurements, respectively).
Because participants did not spend all of their time at home, we adjusted for time activity to reduce exposure misclassification. We considered three microenvironments of exposure: inside the apartment, outside the apartment, and school/work/other. We did not include time on highway in our adjustment because only two participants spent time on highways and the amount of time they spent was <1 h per day.
Inside Apartment was assigned the median indoor PNC obtained from measurements collected in each participant’s apartment. The PNC values assigned for
Outside Apartment and
School/Work/Other were obtained using a regression model of PNC developed for areas near I-93 and an area >1 km from I-93 in Somerville [
47].
Outside Apartment was assigned the annual median PNC on Rt-38 immediately adjacent to the Mystic housing development (40,000 particles/cm
3), and
School/Work/Other was assigned the annual median PNC for the area >1 km from I-93 (18,000 particles/cm
3).
The results of the time-activity surveys, performed at the end of the 3-week HEPA and 3-week sham periods, were used to estimate the fraction of time,
f, each participant spent in each microenvironment,
i, (n = 3 total) during an average 24-h period (average of five work days and two non-work days for employed participants and five week days and two weekend days for unemployed participants). We assumed each participant followed the same 7-day schedule during the three weeks preceding each of the two surveys. We then calculated the time-activity adjusted PNC (TAA-PNC) using Equation (2):
where
PNCi is the microenvironment-specific PNC estimate.
TAA-PNC exposure estimates were then analyzed for association with blood pressure and the blood biomarkers. We used the GENMOD procedure to assess the impact on diastolic, systolic and pulse pressure by the exposure allocation (either HEPA or sham accounting for crossover) and TAA-PNC for Lag0, Lag1, Lag2, and MA3. We also assessed the impact on blood biomarkers by exposure allocation (either HEPA or sham accounting for crossover), TAA-PNC for MA14 and MA21, adjusted for baseline levels of the same biomarker.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}


