
The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review


Abstract
:1. Introduction
2. Objectives
3. Methods
3.1. Study Inclusion Criteria
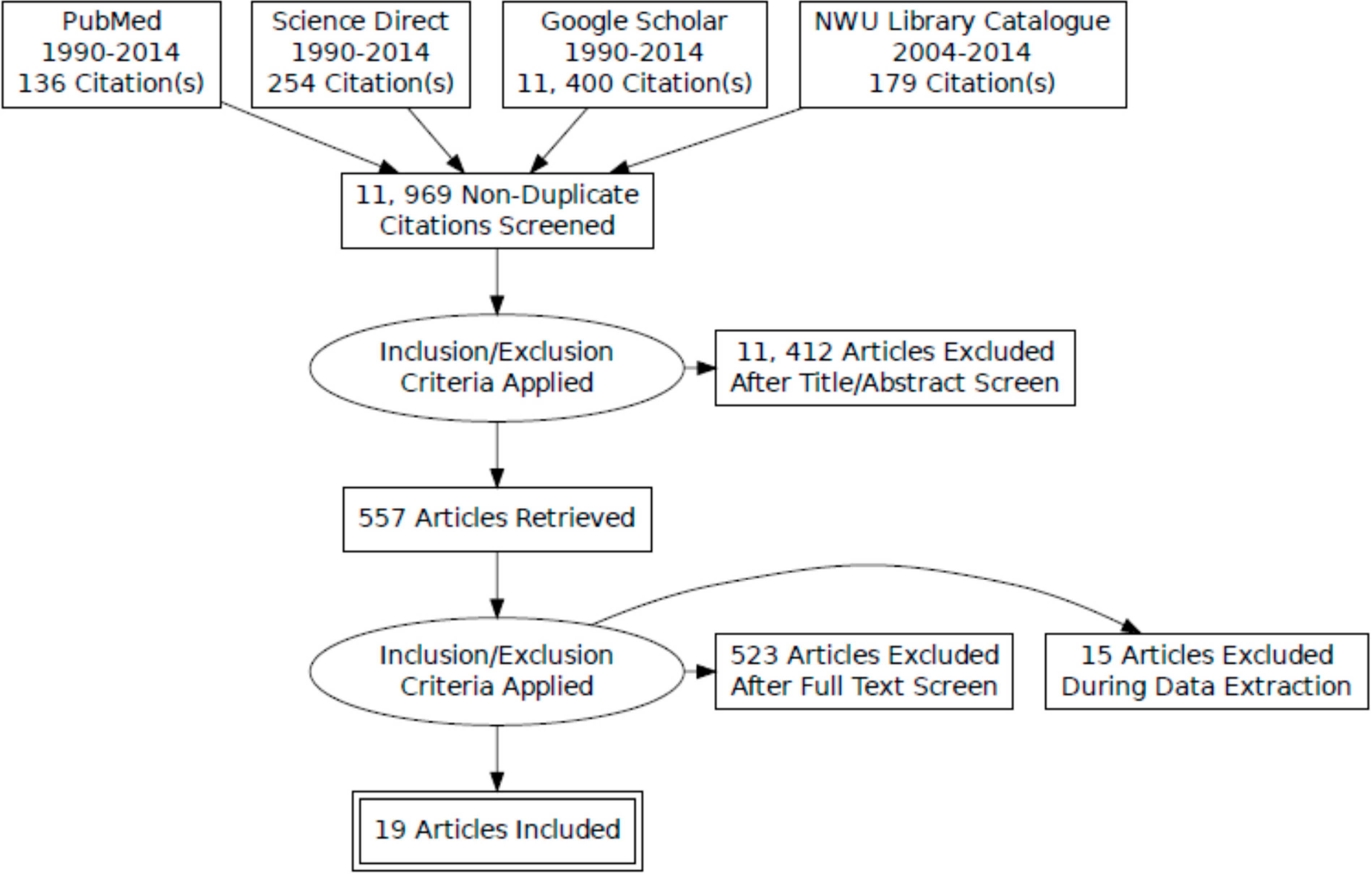
3.2. Search Strategy

3.3. Study Selection
3.4. Data Extraction and Analysis

{kind=link}
| Participants | Study Design | Growth Reference Standards | Outcome and Main Findings | |
|---|---|---|---|---|
| Shisana et al. [16] | South African National Health and Nutrition Examination Survey (0–14 years (yrs): N = 8629) (SANHANES-I). | National survey | WHO Child Growth Standard for 0–5 years. The WHO Reference 2007 for 5–19 years. | Outcome: proportions of stunting, wasting, underweight, overweight and obesity |
| Stunting Boys: 0–3 yrs = 26.9%; 4–6 yrs = 13.5%; 7–9 yrs = 10.0%; 10–14 yrs = 15.2% | ||||
| Wasting Boys: 0–3 yrs = 3.8%; 4–6 yrs = 2.6%; 7–9 yrs = 2.4%; 10–14 yrs = 5.6% | ||||
| Underweight Boys: 0–3 yrs = 8.2%; 4–6 yrs = 5.4%; 7–9 yrs = 8.6%; 10–14 yrs = 0% | ||||
| Overweight: Boys:17.5% (2–5 yrs); 4.5% (6–9 yrs);7.5%(10–14 yrs) | ||||
| Mamabolo et al. [17] | 181 (70 boys & 111 girls) aged 13–20 years from township in Potchefstroom, North West province. | Cross-sectional study design. | WHO Ref of 2007 for prevalence of stunting and underweight. BMI age-adjusted cut off points described Cole 2000 to estimate overweight and obesity. | Outcome: proportions of stunting, underweight, overweight and obesity |
| Stunting: 17.1% Boys; 18.9% Girls | ||||
| Underweight: 11.4% Boys; 0% Girls | ||||
| Overweight & Obesity: 4.1% Boys; 9.9% Girls. | ||||
| Monyeki et al. [12] | 256 (100 Boys; 156 Girls) aged 14 years from 4 township schools and 2 urban schools in Potchefstroom, North West province. | Cross-sectional | Age and sex-specific cut points described by Cole 2000 & 2007 to estimate, underweight, overweight and obesity. | Outcome: proportion of underweight, overweight and obesity |
| Underweight: 44% Boys; 30.7% Girls | ||||
| Overweight & Obesity: 8% Boys; 17.3% Girls | ||||
| Toriola & Monyeki [18] | 283 (111 Boys; 172 Girls) aged 14 years from 4 township schools in Potchefstroom North West province. | Cross-sectional | Age-specific BMI to estimate, underweight, overweight and obesity described by Cole 2000 & 2007. | Outcome: proportion of underweight, overweight and obesity |
| Underweight: 34.2% Boys; 26.6% Girls | ||||
| Overweight: 17.1% Boys; 32.4% Girls | ||||
| Tathian et al. [19] | 959 female learners in 31 primary schools from KwaZulu Natal. | Cross-sectional | WHO/NCHS for proportion of stunting and underweight. Age and gender-specific cut off point for overweight & obesity described by Cole 2000. | Outcome: proportion of stunting, underweight, overweight & obesity |
| Stunting: 9.2% | ||||
| Underweight: 4% | ||||
| Overweight: 9% | ||||
| Obesity: 3.8% | ||||
| Toriola et al. [20] | 1172 (541 Boys & 631 Girls) Black school children aged 10–16 years from two settlements in Limpopo province. | Cross-sectional | CDC BMI charts to classify participant’s under-weight, overweight and obesity status. | Outcome: proportion of underweight, overweight and obesity. |
| Underweight: 4.6% Boys; 5.2% Girls | ||||
| Overweight: 9.1% Boys; 11.0% Girls | ||||
| Obesity: 5.5% Boys; 4.4% Girls | ||||
| Puckree et al. [21] | 120 predominantly Indian children aged 10–12 years from six public schools in urban district of KwaZulu Natal. | Cross-sectional | WHO guidelines and advice from local paediatrician to estimate underweight and overweight. | Outcome: proportion of underweight and overweight |
| Underweight: 66% (Black 15%; Indian 51% | ||||
| Overweight: 5.03% | ||||
| Mamabolo et al. [22] | 162 children from rural villages in Limpopo province. | Prospective cohort study | WHO/NCHS for stunting, wasting and under-weight. IOTF reference for overweight and obesity. | Outcome: proportion of stunting, wasting, underweight, overweight and obesity |
| Stunting: 48% | ||||
| Underweight: 10% | ||||
| Wasting: 1% | ||||
| Overweight: 22% | ||||
| Obese: 24% | ||||
| Kimani-Murage et al. [4] | 3511 children and adolescents aged 1–20 years from Mpumalanga province. | Cross-sectional | 2006 WHO standard for 0–4 years and 1977 NCHS/WHO for 5–17 years to estimate stunting, wasting and underweight. IOTF BMI age and sex specific for overweight and obesity in 2–17 years. | Outcome: proportion of stunting, wasting, underweight, overweight & obesity |
| Underweight: 18% (1–4 yrs); 5% (5–9 yrs); 7% (10–14 yrs); 6% (15–20 yrs) | ||||
| Stunting: 10% (1–4 yrs); 6% (5–9 yrs); 7% (10–14 yrs); 8% (15–20 yrs) | ||||
| Wasting: 7% (1–4 yrs); 6% (5–9 yrs); 0% (10–14 yrs); 0% (15–20 yrs) | ||||
| Overweight: 7% (1–4 yrs); 4% (5–9 yrs); 6% (10–14 yrs); 8% (15–20 yrs) | ||||
| Obesity: 1% (1–4 yrs); 1% (5–9 yrs); 2% (10–14 yrs); 4% (15–20 yrs) | ||||
| Craig et al. [23] | 1519 children in grade 1, 5 and 7 with a mean ages 7, 11 and 15 years in KwaZulu Natal province. | Cross-sectional | BMI-for-age using WHO 2007, Cole-IOTF, & 1977 NCHS/WHO to estimate underweight, overweight and obesity. | Outcome: proportion of stunting, wasting, underweight, overweight & obesity |
| Underweight: | ||||
| (a) WHO 2007: 3.4% Boy; 1.2 Girl, 7 yrs; 5.2% Boy; 1.9% Girl, 11 yrs; 6.2% Boy; 1.9% Girls, 15 yrs | ||||
| (b) Cole-IOTF: 16% Boy; 15.1% Girl, 7 yrs; 12.9% Boy; 12.3% Girl, 11 yrs; 15.8% Boys; 8.2% Girls, 15 yrs | ||||
| (c) NCHS/WHO: 6.2% Boy; 2.8% Girl; 7 yrs; 3.9% Boy; 1.9% Girl, 11 yrs; 7.6% Boy; 1.0% Girls, 15 yrs | ||||
| Overweight: | ||||
| (a) WHO 2007: 8.4% Boy; 11.6% Girl, 7 yrs; 4.7% Boy; 11.9% Girl, 11 yrs; 5.7% Boy; 17.8% Girls, 15 yrs | ||||
| (b) Cole-IOTF: 3.0% Boy; 7.2% Girl, 7 yrs; 3.0% Boy; 8.6% Girl, 11 yrs; 4.9% Boy; 17.4% Girls, 15 yrs | ||||
| (c) NCHS/WHO: 9.6% Boy; 14.6% Girl, 7 yrs; 3.5% Boy; 6.0% Girl, 11 yrs; 4.4% Boy; 9.9% Girls, 15 yrs | ||||
| Obesity: | ||||
| (a) WHO 2007: 0.8% Boy, 2.0% Girl, 7 yrs; 3.4% Boy; 1.5% Girl, 11 yrs; 2.3% Boy; 8.0% Girls, 15 yrs | ||||
| (b) Cole-IOTF: 0.4%; 2.0% Girl, 7 yrs; 2.2% Boy; 1.1% Girl, 11 yrs; 1.2% Boy; 5.3% Girl, 11 yrs | ||||
| (c) NCHS/WHO: 3.1% Boy; 7.7% Girl, 7 yrs; 0.9% Boy; 1.1% Girl, 11 yrs; 0.6% Boy; 2.3% Girl 15 yrs | ||||
| 26.Jacobs & De Ridder [24] | 168 (79 Boys & 89 Girls) Black South African children in rural areas from the North West province. | Cross-sectional | ACSM 2006 to estimate underweight, over-weight and obesity. | Outcome: proportion of underweight, overweight and obesity |
| Underweight: 19% Boys; 11% Girls | ||||
| Overweight and obesity: 0% Boys; 7% Girls | ||||
| Ginsburg et al. [25] | 1613 (773 Boys & 840 Girls) of cohort South African urban children in Gauteng province. | Longitudinal | BMI Z-score using WHO reference to estimate mean BMI z-score. Age and sex-specific BMI by Cole 2000 & 2007 for underweight, over-weight and obesity. | Outcome: Mean BMI z-score and proportion of underweight, overweight & obesity |
| Mean BMI z-score: −0.47 Boys and 0.32 Girls | ||||
| Underweight: 20.3% Boys; 9.6 Girls | ||||
| Overweight: 5.4% Boys; 17.5 Girls | ||||
| Obese: 2.5% Boys; 7.5% Girls | ||||
| Reddy et al. [5] | 9224 school children aged 13–19 from grade 8–11 selected from public schools in all nine provinces. | National survey | Prevalence of underweight was based on WHO/NCHS. Overweight and obesity was based on Cole-IOTF. | Outcome: proportion of underweight, overweight and obesity |
| Underweight: 9% National (15.6% Boys & 3.9% Girls) | ||||
| Overweight: 16.9% National (6.9% Boys; 24.5% Girls) | ||||
| Obese:4% National (2.2% Boys; 5.3% Girls) | ||||
| Bosman et al. [26] | 1512 (52.8% Boys &47.2% Girls) children aged 1–5 years using data from 1999 NFCS database. | National survey | 1977 NCHS, 2000 CDC and 2006 WHO growth standard were used to estimate stunting, wasting underweight, overweight and obesity. | Outcome: proportion of stunting, wasting, underweight, overweight and obesity |
| Stunting: 2006 WHO Standard: 20.1%; 1977 NCHS: 17.1%; 2000 CDC: 14.2% | ||||
| Wasting: 2006 WHO standard: 10%; 1977 NCHS: 15%; 2000 CDC: 15% | ||||
| Underweight: 2006 WHO standard: 6.8%; 1977 NCHS: 9.7%; 2000 CDC: 9.9% | ||||
| Overweight: 2006 WHO standard: 20.6%; 1977 NCHS: 13.0%; 2000 CDC: 16.7% | ||||
| Obese: 2006 WHO standard: 9.5%; 1977 NCHS: 5.9%; 2000 CDC: 6.3% | ||||
| Jinabhai et al. [9] | 2398 Boys and 2924 Girls Black teenagers aged 13–18 years in the first South African Youth Risk Behaviour Survey (2002). | National survey | The NCHS and CDC used data from NHANES II which WHO recommended for international use to estimate stunting & underweight. Age-dependent BMI cut off by Cole 2000 for overweight and obesity. | Outcome: proportion of stunting, underweight and overweight |
| Stunting: 21.9% Boys; 9.4% Girls | ||||
| Underweight: 18.4% Boys; 2.6% Girls | ||||
| Overweight:4.2% Boys; 20.9% Girls | ||||
| Jinabhai et al. [27] | 802 children in grade 3 aged 8 and 11 years from 11 schools in rural district of Kwazulu Natal. | Cross-sectional | NCHS was used to estimate prevalence of stunting. Calculations for overweight and obesity were based on WHO (1995) and Cole-IOTF. | Outcome: prevalence of stunting, overweight and obesity |
| Stunting:31%–100% mild; 3%–25% moderate stunting; 0.6% severe stunting | ||||
| Overweight: 4.1% IOTF cut off point; 6.0% WHO definition | ||||
| Obesity: 0.6% IOTF; 0.9% WHO definition | ||||
| Monyeki et al. [28] | 1335 (684 Boys & 651 Girls) rural children aged 3–10 years from Ellisras, rural Limpopo province. | Cross-sectional | NHANES I & II or NCHS reference cut off point to determine prevalence of stunting and wasting. | Outcome: prevalence of stunting, wasting and WAZ (underweight) |
| WAZ (underweight): 20.9%–64.3% (highest in 9–11 yrs) | ||||
| HAZ (stunting): 3.7%–28.6% (highest in 10–11 yrs) | ||||
| WHZ (wasting): 27.7%–54.6% (highest in 3–3.9 yrs) | ||||
| Monyeki et al. [29] | 1339 (687 Boys & 652 Girls) children aged 3–10 years from Ellisras, rural Limpopo province. | Cross-sectional | WAZ, HAZ and WHZ were determined using NHANES III. | Outcome: prevalence of stunting and wasting |
| Stunting: 19.9%–51.0% | ||||
| Wasting: 22.8%–39.9% | ||||
| Labadarios et al. [7] | A national representative of 2613 children aged 1–9 years. | National survey | NCHS reference median to determine WAZ, HAZ and WHZ. Standard BMI cut off point for overweight and obesity. | Outcome: prevalence of stunting, underweight, wasting, overweight and obesity |
| Stunting: 21.6% National; 30.6% Commercial Farm; 16% Formal Urban; 19.3% Informal Urban; 16.7% Urban; 26.5% Rural | ||||
| Underweight: 10.3% National; 18.1% Commercial Farm; 7.8% Formal Urban; 7.6% Informal Urban; 7.7% Urban; 12.8% Rural | ||||
| Wasting: 3.7% National; 4.2% Commercial Farm; 2.6% Formal Urban; 2.1% Informal Urban; 2.4% Urban; 4.9% Rural | ||||
| Overweight: 12.1% National; 7.2% Farm; 13.9% Formal Urban; 7.5% Informal Urban; 11.6% Rural; 12.5% Urban | ||||
| Obese: 5.0% National; 3.5% Commercial Farm; 6.2% Formal Urban; 5.9% Informal Urban; 3.7% Rural; 6.1% Urban |
4. Results
5. National Demographics of Included Studies
6. Measurements
6.1. Assessment of Underweight, Stunting, and Wasting
6.2. Assessment of Overweight and Obesity
6.3. Prevalence of Underweight
6.4. Prevalence of Stunting
6.5. Prevalence of Wasting
6.6. Prevalence of Overweight
6.7. Prevalence of Obesity
6.8. The Trend in the Prevalence of Malnutrition in South African Children
7. Discussion
8. Government Interventions in Addressing Malnutrition in Children
9. Public Health and Future Implications Messages
10. Conclusions
Acknowledgments
Author Contributions
Disclaimer
Conflicts of Interest
References
- World Health Organisation (WHO). Children: Reducing Mortality; WHO: Geneva, Switzerland (Updated September 2013). Available online: http://www.who.int/mediacentre/factsheets/fs178/en/ (accessed on 16 February 2014).
- Horton, R. Maternal and child undernutrition: An urgent opportunity. Lancet 2008, 371. [Google Scholar] [CrossRef] [PubMed]
- Blake, R.; Allen, L.; Bhutta, Z.; Caulfield, L.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef] [PubMed]
- Kimani-Murage, E.; Kahn, K.; Pettifor, J.; Tollman, S.; Dunger, D.; Gomez-Olive, X.; Norris, S. The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Resnicow, K.; James, S.; Kambaran, N.; Omardien, R.; Mbewu, A. Underweight, overweight and obesity among South African adolescents: Results of the 2002 National Youth Risk Bevaviour Survey. Public Health Nutr. 2008, 12, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.D.; Kemper, H.C.; Makgae, P.J. Relationship between fat patterns, physical fitness and blood pressure of rural South African children: Ellisras longitudinal growth and health study. J. Hum. Hypertens. 2008, 22, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Labadarios, D.; Steyn, N.; Maunder, E.; MacIntryre, U.; Gericke, G.; Swart, R.; Huskisson, J.; Dannhauser, A.; Vorster, H.H.; Nesmvuni, A.E.; Nel, J.H. The national food consumption survey (NFCS): South Africa, 1999. Public Health Nutr. 2005, 8, 533–543. [Google Scholar] [PubMed]
- World Health Organisation (WHO). Obesity and Overweight; WHO: Geneva, Switzerland. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 20 August 2014).
- Jinabhai, C.; Taylor, M.; Reddy, P.; Monyeki, D.; Kamabaran, N.; Omardien, R.; Sullivan, K. Sex differences in under and over nutrition among school-going Black teenagers in South Africa: An uneven nutrition trajectory. Trop. Med. Int. Health 2007, 12, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Vorster, H.; Venter, C.; Wissing, M.; Margetts, B. The nutrition and health transition in the North West province of South Africa: A review of the THUSA (Transition and Health during Urbanisation of South Africans) study. Public Health Nutr. 2005, 8, 480–490. [Google Scholar] [PubMed]
- Stevens, G.; Finucane, M.; Paciorek, C.; Flaxman, S.; White, R.; Donner, A.; Ezzati, M. Nutrition Impact Model Study Group. Trends in mild, moderate, and severe stunting and underweight, and progress towards MDG 1 in 141 developing countries: A systematic analysis of population representative data. Lancet 2012, 380, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, M.A.; Neetens, R.; Moss, S.J.; Twisk, J. The relationships between body composition and physical fitness in 14 year old adolescents residing withing the Tlokwe local municipality, SA: The PAHL study. BMC 2012, 12. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, A.; Benfield, L.; Logue, J.; Tilling, K.; Howe, D.; Fraser, A.; Cherry, L.; Watt, P.; Ness, A.R.; Smith, G.D.; et al. Association between general and central adiposity in childhood, and change in these with cardiovascular risk factors in adolescence: Prospective cohort study. Brit. Med. J. 2010, 341. [Google Scholar] [CrossRef]
- Garnett, S.P.; Baur, L.A.; Cowell, C.T. Waist-to-height ratio: A simple option for determining excess central adiposity in young people. Int. J. Obes. 2008, 32, 1028–1030. [Google Scholar] [CrossRef]
- Savva, S.C.; Tornaritis, M.; Savva, M.E.; Kourides, Y.; Panagi, A.; Georgiou, C.; Kafatos, A. Waist circumference and waist-to-height ratio are better predictors of cardiovascular risk factors in children than body mass index. Int. J. Obes. 2000, 24, 1453–1458. [Google Scholar] [CrossRef]
- Shisana, O.; Labadarios, D.; Rehle, T.; Simbayi, I.; Zuma, K.; Dhansay, A.; Reddy, P.; Parker, W.; Hoosain, E.; Naidoo, P.; et al. South African National Health and Nutrition Examination Survey (SANHANES-I); HSRC Press: Cape Town, South Africa, 2014. [Google Scholar]
- Mamabolo, R.; Berti, C.; Monyeki, M.; Kruger, S. Association between insulin-like growth factor-1, measures of overnutrition and undernutrition and insulin resistance in Black adolescents living in the North-West Province, South Africa. Amer. J. Biol. 2014, 26, 189–197. [Google Scholar] [CrossRef]
- Toriola, O.; Monyeki, M. Health-related fitness, body composition and physical activity status among adolescent learners: The PAHL study. AJPHERD 2012, 18, 795–811. [Google Scholar]
- Tathian, N.; Moodley, I.; Mubaiwa, V.; Denny, L.; Taylor, M. South Africa’s nutritional transition: Overweight, obesity, underweight and stunting in female primary school learners in rural KwaZulu-Natal, South Africa. South Afr. Med. J. 2013, 103, 718–723. [Google Scholar] [CrossRef]
- Toriola, A.L.; Moselakgomo, V.; Shaw, B.; Goon, D. Overweight, obesity and underweight in rural black South African children. South Afr. J. Clin. Nutr. 2012, 25, 57–61. [Google Scholar]
- Puckree, T.; Naidoo, P.; Pillay, P.; Naidoo, T. Underweight and overweight in primary school children in eThekwini district in Kwazulu-natal, South Africa. Afr. J. Prim. Health Care Fam. Med. 2011. [Google Scholar] [CrossRef]
- Mamabolo, R.; Alberts, M.; Steyn, N.; Waal, H.; Levitt, N. Prevalence and determinants of stunting and overweight in 3-year-old black South African children residing in the central region of Limpopo provine. South Afr. Public Health Nutr. 2005, 8, 501–508. [Google Scholar]
- Craig, E.; Reilly, J.; Bland, R. Body fatness or anthropometry for assessment of unhealthy weight status: Comparison between methods in South African children and adolescents. Public Health Nutr. 2012, 16, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; de Ridder, J. Prevalence of overweight and underweight among black South African children from rural areas in the North-West province. South Afr. J. Res. Sport Phys. Educ. Recreat. 2012, 34, 41–51. [Google Scholar]
- Gimsburg, C.; Griffiths, P.; Richter, L.; Norris, S. Residential mobility, socioeconmic context and body mass index in a cohort urban South African adolescents. Health Place 2013, 19, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Bosman, L.; Herselman, M.; Kruger, S.; Labadarios, D. Secondary analysis of anthropometric data from a South African national food consumption survey, using growth reference standard. Maternal Child Health J. 2011, 15, 1372–1380. [Google Scholar] [CrossRef]
- Jinabhai, C.; Taylor, M.; Sullivan, K. Implications of the prevalence of stunting, overweight and obesity amongst South African promary school children: A possible nutritional transition? Eur. J. Clin. Nutr. 2003, 57, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.; Cameron, N.; Getz, B. Growth and nutritional status of rural South African children 3–10 years old: The Ellisras growth study. Amer. J. Hum. Biol. 2000, 12, 42–49. [Google Scholar] [CrossRef]
- Monyeki, K.; de Ridder, J.; Toriola, A.; Steyn, N.; van Lenthe, F.; Griebenauw, L. Physical Growth and Socio-Economic Status of South African rural children Aged 3–10 Years. In Proceedings of the 6th International Conference in Kinanthropometry, Adelaide, Australia, 13–16 October 1998.
- Kallman, K. Food for Thought: A Review of the National School Nutrition Programme; University of Cape Town: Cape Town, South Africa, 2005. [Google Scholar]
- Labadarios, D.; Mchiza, Z.; Steyn, N.; Gericke, G.; Maunder, E.; Davids, Y.; Parker, W. Food security in South Africa: A review of national surveys. Bull. WHO 2011, 89, 891–899. [Google Scholar] [PubMed]
- Marrodan, M.D.; Mesa, M.S.; Arechiga, J.; Perez-Magdaleno, A. Trend in menarcheal age in Spain: Rural and urban comparison during a recent period. Ann. Hum. Biol. 2000, 27, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Rayner, M. The burden of overweight and obesity-related ill health in the UK. Obes. Rev. 2007, 8, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.; Sandora, T.; Shih, M.; Ross-Degnan, D.; Goldman, D.; Gillman, M. The association of television and video viewing with fast food intake by preschool-age children. Obesity (Silver Spring) 2006, 14, 2034–2041. [Google Scholar] [CrossRef]
- Latt, E.; Maestu, J.; Raask, T.; Rubin, D.; Purge, P.; Saar, M.; Utsal, L.; Jürimäe, J.; Maasalu, K.; Jürimäe, T.; et al. Association of physical activity to cardiovascular fitness and fatness in 12–13 year-old boys in different weight status. J. Public Health 2013, 21, 231–239. [Google Scholar]
- Kelishadi, R.; Haghdoost, A.; Sadeghirad, B.; Khajehkazemi, R. Trend in the prevalence of overweight and obesity among Iranian children and adolescents: A systematic review and meta-analysis. Nutrition 2014, 30, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Epidemiology of childhood obesity-methodological aspects and guidelines: What is new? Int. J. Obes. Relat. Metab. Disord. 2004, 28, S21–S28. [Google Scholar] [CrossRef] [PubMed]
- Butta, Z.; Ahmed, T.; Black, R.; Cousens, S.; Dewey, K.; Glugliani, E.; Haider, B.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.S.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008. [Google Scholar] [CrossRef]
- Louw, R.; Bekker, E.; Wentzel-Viljoen, E. An External Evaluation of Certain Aspects of Primary Schools Feeding; Department of Health: Pretoria, South Africa, 2001. [Google Scholar]
- World Health Organisation (WHO). Global Strategy on Diet, Physical Activity and Health; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- De Ridder, J.H.; Coetzee, D. Childhood Obesity in South Africa: Are we sitting on a time bomb? Glob. J. Health Phys. Educ. Pedagog. 2013, 2, 239–249. [Google Scholar]
- National Development Plan 2030: Our Future—Make It Work. Available online: http://www.npconlineco.za/MediaLib/Downloads/Downloads/Executive%20Summary-NDP%202030%20-%20Our%20future%20-%20make%20it%20work.pdf (accessed on 8 January 2015).
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence based physical activity for school-age youth. J. Paediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monyeki, M.A.; Awotidebe, A.; Strydom, G.L.; De Ridder, J.H.; Mamabolo, R.L.; Kemper, H.C.G. The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 1156-1173. https://doi.org/10.3390/ijerph120201156
Monyeki MA, Awotidebe A, Strydom GL, De Ridder JH, Mamabolo RL, Kemper HCG. The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review. International Journal of Environmental Research and Public Health. 2015; 12(2):1156-1173. https://doi.org/10.3390/ijerph120201156
Chicago/Turabian StyleMonyeki, Makama Andries, Adedapo Awotidebe, Gert L. Strydom, J. Hans De Ridder, Ramoteme Lesly Mamabolo, and Han C. G. Kemper. 2015. "The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review" International Journal of Environmental Research and Public Health 12, no. 2: 1156-1173. https://doi.org/10.3390/ijerph120201156