
Content and Face Validation of a Novel, Interactive Nutrition Specific Physical Exam Competency Tool (INSPECT) to Evaluate Registered Dietitians’ Competence: A Delphi Consensus from the United States

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Item Generation and Initial Tool Design
2.2. Participant Selection
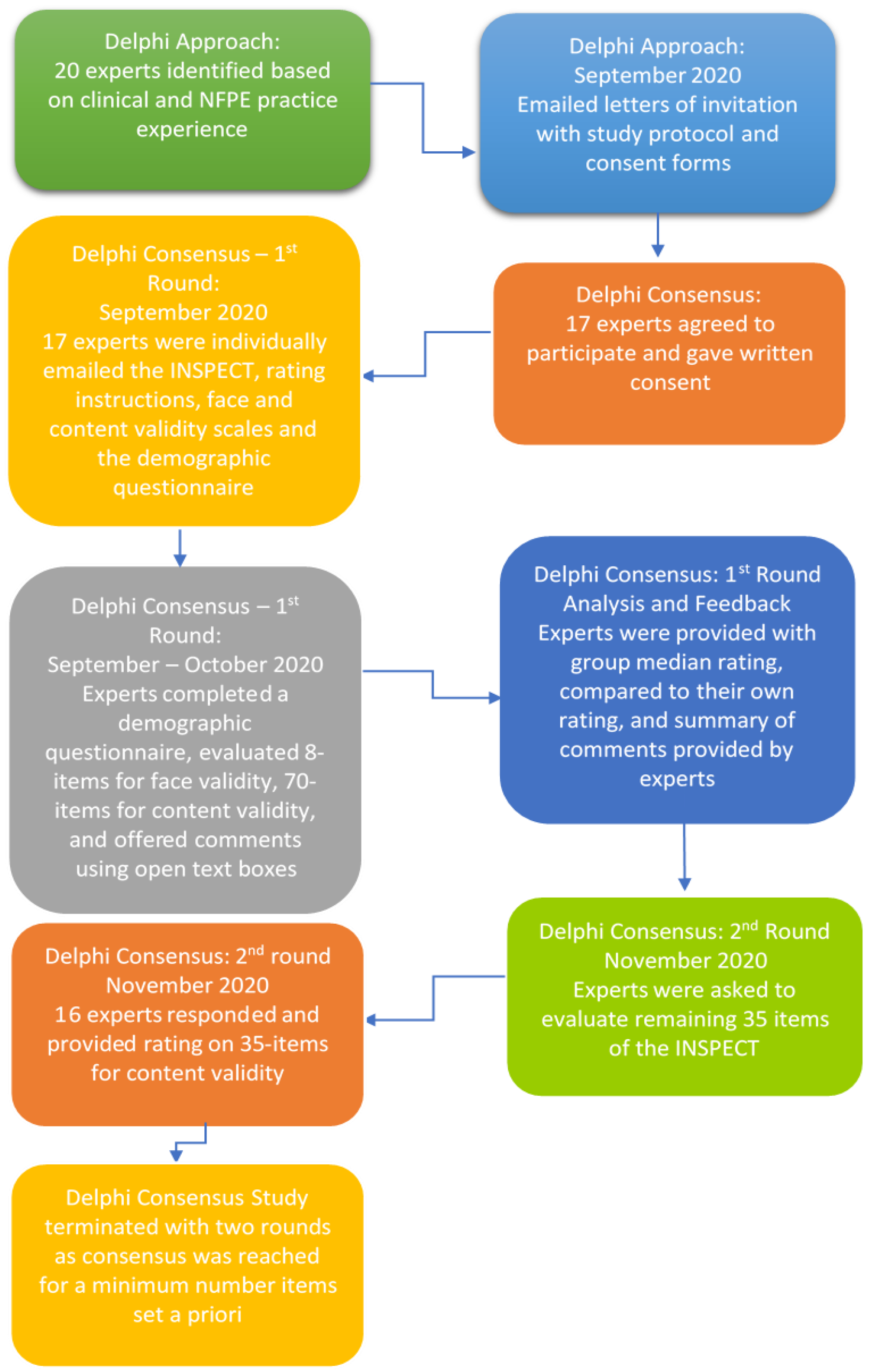
2.3. Delphi Methodology
2.4. Face Validity of the INSPECT
2.5. Content Validity of the INSPECT
2.6. Open Comments of the INSPECT
2.7. Statistical Analysis
3. Results
3.1. Face Validity of the INSPECT
3.2. Content Validity of the INSPECT
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Litchford, M. Putting the nutrition focused physical assessment into practice in long-term care settings. Ann. Long-Term Care Clin. Care Aging 2013, 21, 38–41. [Google Scholar]
- Hammond, K. Nutrition-Focused Physical Assessment. Home Healthc. Nurse 1999, 17, 354–355. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L.; Compher, C.; Sullivan, D.H.; Mullin, G.E. Recognizing malnutrition in adults: Definitions and characteristics, screening, assessment, and team approach. J. Parenter. Enter. Nutr. 2013, 37, 802–807. [Google Scholar] [CrossRef]
- Mordarski, B. Nutrition-Focused Physical Exam Hands-On Training Workshop. J. Acad. Nutr. Diet. 2016, 116, 868–869. [Google Scholar] [CrossRef] [PubMed]
- Stankorb, S.; Rigassio-Radler, D.; Hafiz, K.; Touger-Decker, R. The Professional Practices of Nutrition Focused Physical Examination among Registered Dietitians. J. Am. Diet. Assoc. 2009, 109, A9. [Google Scholar] [CrossRef]
- Touger-Decker, R. Physical Assessment Skills for Dietetics Practice: The Past, the Present, and Recommendations for the Future. Top. Clin. Nutr. 2006, 21, 190–198. [Google Scholar] [CrossRef]
- Accreditation Council for Education in Nutrition and Dietetics. Future education model standards for accredited graduate programs in dietetics; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2019; Available online: https://www.eatrightpro.org/acend/accreditation-standards-fees-and-policies/future-education-model (accessed on 15 July 2021).
- Accreditation Council for Education in Nutrition and Dietetics. Crosswalk of Knowledge and Competency Statements for CP, DI, DPD, FDE, IDE Programs; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2016; Available online: https://www.eatrightpro.org/~/media/eatrightpro%20files/acend/about%20program%20accreditation/accreditation%20standards/2017%20rdn%20program%20competency%20crosswalk%207%2029%2016.ashx (accessed on 15 July 2021).
- Lucey, C.R.; Thibault, G.E.; Ten Cate, O. Competency-Based, Time-Variable Education in the Health Professions: Crossroads. Acad. Med. 2018, 93, S1–S5. [Google Scholar] [CrossRef]
- Fan, J.-Y.; Wang, Y.H.; Chao, L.F.; Jane, S.-W.; Hsu, L.-L. Performance evaluation of nursing students following competency-based education. Nurse Educ. Today 2015, 35, 97–103. [Google Scholar] [CrossRef]
- Swing, S.R.; Clyman, S.G.; Holmboe, E.S.; Williams, R.G. Advancing resident assessment in graduate medical education. J. Grad. Med. Educ. 2009, 1, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Frank, J.R.; Danoff, D. The CanMEDS initiative: Implementing an outcomes-based framework of physician competencies. Med. Teach. 2007, 29, 642–647. [Google Scholar] [CrossRef]
- Linsenmeyer, M.; Wimsatt, L.; Speicher, M.; Powers, J.; Miller, S.; Katsaros, E. Assessment Considerations for Core Entrustable Professional Activities for Entering Residency. J. Am. Osteopath. Assoc. 2018, 118, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rekman, J.; Gofton, W.; Dudek, N.; Gofton, T.; Hamstra, S.J. Entrustability Scales: Outlining Their Usefulness for Competency-Based Clinical Assessment. Acad. Med. 2016, 91, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Academy Quality Management. Academy of Nutrition and Dietetics: Revised 2017 Standards of Practice in Nutrition Care and Standards of Professional Performance for Registered Dietitian Nutritionists. J. Acad. Nutr. Diet. 2018, 118, 132–140.e15. [Google Scholar] [CrossRef] [Green Version]
- The Joint Commission on Accreditation of Healthcare Organizations. The Joint Commission Guide to Patient and Family Education. Available online: https://www.jointcommission.org/standards/standard-faqs/health-care-staffing-services/human-resources-management-hshr/000001433/ (accessed on 17 July 2021).
- Fischer, M.; JeVenn, A.; Hipskind, P. Evaluation of muscle and fat loss as diagnostic criteria for malnutrition. Nutr. Clin. Pract. 2015, 30, 239–248. [Google Scholar] [CrossRef] [PubMed]
- MacQuillan, E.L.; Ford, J.; Baird, K. Clinical Competence Assessed Using Simulation: Development of a Standardized Tool to Assess Nutrition-Focused Physical Exam Skill Competence for Registered Dietitian Nutritionists. J. Nutr. Educ. Behav. 2020, 53, 174–182. [Google Scholar] [CrossRef]
- Zechariah, S.; Lehman, L.; Waller, J.L.; De Leo, G.; Stallings, J.; Gess, A.J. Item Generation in the Development of an Interactive Nutrition Specific Physical Exam Competency Tool (INSPECT): A Qualitative Study Utilizing Technology-Based Focus Groups in the United States. Healthcare 2021, 9, 576. [Google Scholar] [CrossRef]
- Oluwatayo, J.A. Validity and Reliability Issues in Educational Research. J. Educ. Soc. Res. 2012, 2, 391–400. [Google Scholar]
- Taherdoost, H. Validity and Reliability of the Research Instrument; How to Test the Validation of a Questionnaire/Survey in a Research. SSRN Electron. J. 2016, 5, 28–36. [Google Scholar] [CrossRef]
- Karras, D.J. Statistical methodology: II. Reliability and validity assessment in study design, Part B. Acad. Emerg. Med. 1997, 4, 144–147. [Google Scholar] [CrossRef]
- Cronbach, L.J. Test Validation; American Council on Education: Washington, DC, USA, 1971; pp. 443–507. [Google Scholar]
- Grant, J.S.; Davis, L.L. Selection and use of content experts for instrument development. Res. Nurs. Health 1997, 20, 269–274. [Google Scholar] [CrossRef]
- Larsson, H.; Tegern, M.; Monnier, A.; Skoglund, J.; Helander, C.; Persson, E.; Malm, C.; Broman, L.; Aasa, U. Content Validity Index and Intra- and Inter-Rater Reliability of a New Muscle Strength/Endurance Test Battery for Swedish Soldiers. PLoS ONE 2015, 10, e0132185. [Google Scholar]
- Ferrie, S.; Allman-Farinelli, M. Development of a tool to measure dietitians’ involvement in the intensive care setting. Nutr. Clin. Pract. 2011, 26, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar]
- Keeney, S.; McKenna, H.; Hasson, F. The Delphi Technique in Nursing and Health Research. In The Delphi Technique in Nursing and Health Research; Wiley-Blackwell: Chichester, UK, 2011. [Google Scholar]
- Banayan, J.; Blood, A.; Park, Y.S.; Shahul, S.; Scavone, B.M. A modified Delphi method to create a scoring system for assessing team performance during maternal cardiopulmonary arrest. Hypertens. Pregnancy 2015, 34, 314–331. [Google Scholar] [CrossRef] [PubMed]
- Kaijser, M.A.; van Ramshorst, G.H.; Emous, M.; Veeger, N.; van Wagensveld, B.A.; Pierie, J.E.N. A Delphi Consensus of the Crucial Steps in Gastric Bypass and Sleeve Gastrectomy Procedures in the Netherlands. Obes. Surg. 2018, 28, 2634–2643. [Google Scholar] [CrossRef] [Green Version]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Gliner, J.A.; Morgan, G.A.; Leech, N.L. Research Methods in Applied Settings: An Integrated Approach to Design and Analysis, 2nd ed.; Routledge/Taylor & Francis Group: New York, NY, USA, 2009; p. xvii 469. [Google Scholar]
- De Groef, A.; Van Kampen, M.; Moortgat, P.; Anthonissen, M.; Van den Kerckhove, E.; Christiaens, M.R.; Neven, P.; Geraerts, I.; Devoogdt, N. An evaluation tool for Myofascial Adhesions in Patients after Breast Cancer (MAP-BC evaluation tool): Concurrent, face and content validity. PLoS ONE 2018, 13, e0193915. [Google Scholar] [CrossRef]
- Lebet, R.M.; Asaro, L.A.; Zuppa, A.F.; Curley, M.A.Q. Face and content validity of variables associated with the difficult-to-sedate child in the paediatric intensive care unit: A survey of paediatric critical care clinicians. Aust. Crit. Care 2018, 31, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.; Booker, C.; Fox, R.; Windsor, C.; Osborne, S.; Gardner, G. Nursing physical assessment for patient safety in general wards: Reaching consensus on core skills. J. Clin. Nurs. 2016, 25, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Breimer, G.E.; Haji, F.A.; Hoving, E.W.; Drake, J.M. Development and content validation of performance assessments for endoscopic third ventriculostomy. Childs Nerv. Syst. 2015, 31, 1247–1259. [Google Scholar] [CrossRef]
- Green, B.; Jones, M.; Hughes, D.; Williams, A. Applying the Delphi technique in a study of GPs’ information requirements. Health Soc. Care Community 1999, 7, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Haring, C.M.; van der Meer, J.W.; Postma, C.T. A core physical examination in internal medicine: What should students do and how about their supervisors? Med. Teach. 2013, 35, e1472–e1477. [Google Scholar] [CrossRef] [PubMed]
- Gowda, D.; Blatt, B.; Fink, M.J.; Kosowicz, L.Y.; Baecker, A.; Silvestri, R.C. A Core Physical Exam for Medical Students: Results of a National Survey. Acad. Med. 2014, 89, 436–442. [Google Scholar] [CrossRef] [PubMed]
- von der Gracht, H.A. Consensus measurement in Delphi studies. Technol. Forecast. Soc. Chang. 2012, 79, 1525–1536. [Google Scholar] [CrossRef]
- Weir, C.R.; Hicken, B.L.; Rappaport, H.S.; Nebeker, J.R. Crossing the quality chasm: The role of information technology departments. Am. J. Med. Qual. 2006, 21, 382–393. [Google Scholar] [CrossRef]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Brender, J.; Ammenwerth, E.; Nykänen, P.; Talmon, J. Factors influencing success and failure of health informatics systems-a pilot Delphi study. Methods Inf. Med. 2006, 45, 125–136. [Google Scholar] [PubMed]
- Lafave, L.M.Z. Creating a healthy eating and active environment survey (CHEERS) for childcare: An inter-rater, intra-rater reliability and validity study. BMC Public Health 2019, 19, 1384. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications; Addison-Wesley Pub. Co. Advanced Book Program: Reading, MA, USA, 1975. [Google Scholar]
- Bickley, L.S.; Szilagyi, P.G.; Hoffman, R.M. Bates’ Guide to Physical Examination and History Taking; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Secker, D.J.; Jeejeebhoy, K.N. How to perform Subjective Global Nutritional assessment in children. J. Acad. Nutr. Diet. 2012, 112, 424–431.e6. [Google Scholar] [CrossRef]
- Dalkey, N.; Helmer, O. An Experimental Application of the Delphi Method to the Use of Experts. Manag. Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; McKee, C.M.; Sanderson, C.F.; Askham, J.; Marteau, T. Consensus development methods, and their use in clinical guideline development. Health Technol. Assess. 1998, 2, i-88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jairath, N.; Weinstein, J. The Delphi methodology (Part one): A useful administrative approach. Can. J. Nurs. Adm. 1994, 7, 29–42. [Google Scholar]
- Powell, C. The Delphi technique: Myths and realities. J. Adv. Nurs. 2003, 41, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Litchford, M.D. Nutrition Focused Physical Assessment: Making Clinical Connections; Case Software & Books: Greensboro, NC, USA, 2015. [Google Scholar]
- Malone, A.; Hamilton, C. The Academy of Nutrition and Dietetics/The American Society for Parenteral and Enteral Nutrition Consensus Malnutrition Characteristics: Application in Practice. Nutr. Clin. Pract. 2013, 28, 639–650. [Google Scholar] [CrossRef]
- Patel, V.; Romano, M.; Corkins, M.R.; DiMaria-Ghalili, R.A.; Earthman, C.; Malone, A.; Miller, S.; Sabino, K.; Wooley, J.; Guenter, P. Nutrition Screening and Assessment in Hospitalized Patients: A Survey of Current Practice in the United States. Nutr. Clin. Pract. 2014, 29, 483–490. [Google Scholar] [CrossRef] [Green Version]
- WHO. Malnutrition-Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 6 August 2021).
- Esper, D.H. Utilization of nutrition-focused physical assessment in identifying micronutrient deficiencies. Nutr. Clin. Pract. 2015, 30, 194–202. [Google Scholar] [CrossRef]
- Yetley, E.A. Multivitamin and multimineral dietary supplements: Definitions, characterization, bioavailability, and drug interactions. Am. J. Clin. Nutr. 2007, 85, 269s–276s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, S.C.; Streit, S.M.; Beebe, M.L.; Maxwell, P.J., IV. Micronutrient Needs of the Elderly. Nutr. Clin. Pract. 2014, 29, 435–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litchford, M.D. Counteracting the Trajectory of Frailty and Sarcopenia in Older Adults. Nutr. Clin. Pract. 2014, 29, 428–434. [Google Scholar] [CrossRef]
- Favaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430). Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 3 September 2021).
- Accreditation Council for Education in Nutrition and Dietetics. 2022 ACEND Accreditation Standards. Available online: https://www.eatrightpro.org/acend/accreditation-standards-fees-and-policies/2022-standards (accessed on 3 September 2021).
- Downing, S.M. Validity: On meaningful interpretation of assessment data. Med. Educ. 2003, 37, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J. Adv. Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable (n = 17) | Median (Q1–Q3) ^ | n | % |
|---|---|---|---|
| Age (years) * | 48.5 (36.2–60.7) | ||
| Gender | |||
| Females | 17 | 100 | |
| Ethnic Background | |||
| White, non-Hispanic | 17 | 100 | |
| Highest Degree Earned | |||
| Bachelors | 5 | 29.4 | |
| Masters | 7 | 41.2 | |
| Doctoral | 5 | 29.4 | |
| Primary Job Role | |||
| Clinical Dietitian/Specialist | 7 | 41.1 | |
| Clinical Nutrition Manager/Lead Dietitian | 6 | 35.3 | |
| Educator/Researchers | 4 | 23.5 | |
| Primary Work Location | |||
| Inpatient Hospital | 11 | 64.7 | |
| Outpatient Clinic | 2 | 11.8 | |
| Academic Institutions | 4 | 23.5 | |
| Years of Practice as Clinical Dietitian | 13 (6.5–31.5) | ||
| Years of Experience in Performing NFPE | 6 (4.5–21.5) |
| Face Validity Items (n = 17) | Clear | Not Clear | 95% Confidence Interval for Clear | |
|---|---|---|---|---|
| % | % | LB * | UB ^ | |
| Instructions on completing the tool are clear and easy to understand | 64.7 | 35.3 | 39 | 65 |
| The tool is organized in a logical way, following a head to toe assessment | 76.5 | 23.5 | 54 | 76 |
| Tool scoring system is clear and easy to use | 88.2 | 11.8 | 71 | 88 |
| Each item within each subset is clearly written | 64.7 | 35.3 | 39 | 65 |
| Each item has a consistent style in language | 70.6 | 29.4 | 46 | 71 |
| Subset scores calculate accurately taking into account ‘not-applicable’ items | 82.4 | 17.6 | 62 | 82 |
| Overall tool score calculates accurately | 88.2 | 11.8 | 71 | 88 |
| The layout of the tool is good | 82.4 | 17.6 | 62 | 82 |
| Delphi Round 1 (n = 17) (Items = 70) | Delphi Round 2 (n = 16) (Items = 35) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| INSPECT Categories | Items | Median | Quartiles | Agreement (>50% with ≥4) | Retain, Reject or Reassess | Median | Quartiles | Agreement (>50% with ≥3) | Retain, Reject or Reassess | ||
| Q1 * | Q3 ^ | Q1 * | Q3 ^ | ||||||||
| Preparation & Initial Steps | Washes/Sanitizes Hands | 5 | 5 | 5 | 94% | Retain | |||||
| Utilizes PPE | 5 | 5 | 5 | 94% | Retain | ||||||
| Introduces Self/Exam | 5 | 5 | 5 | 94% | Retain | ||||||
| Verbal Consent | 5 | 3 | 5 | 77% | Retain | ||||||
| Head & Hair Exam | Asks Hair Changes | 3 | 3 | 4 | 47% | Reassess | 3 | 2 | 4 | 69% | Retain |
| Inspects Dry/Dull Hair | 3 | 3 | 4 | 44% | Reassess | 3 | 2 | 4 | 53% | Retain | |
| Brittle Hair Pluckability | 3 | 3 | 4 | 47% | Reassess | 3 | 2 | 4 | 56% | Retain | |
| Seborrheic Dermatitis | 3 | 2 | 4 | 36% | Reassess | 3 | 2 | 4 | 50% | Reject | |
| Alopecia | 3 | 2 | 4 | 24% | Reassess | 2 | 2 | 3 | 44% | Reject | |
| Face Exam | Flakiness -Nasolabial area | 4 | 3 | 4 | 65% | Retain | |||||
| Facial Movements | 3 | 2 | 4 | 35% | Reassess | 2 | 2 | 3 | 31% | Reject | |
| Temporal Muscles | 5 | 4 | 5 | 94% | Retain | ||||||
| Buccal Fad Pads | 5 | 3 | 5 | 88% | Retain | ||||||
| Temporomandibular Joint Range of Motion | 2 | 2 | 4 | 29% | Reassess | 2 | 1 | 3 | 50% | Reject | |
| Eye Exam | Conjunctivae Color | 4 | 3 | 5 | 59% | Retain | |||||
| Bitots Spots | 3 | 3 | 4 | 47% | Reassess | 3 | 2 | 4 | 56% | Retain | |
| Nystagmus | 3 | 2 | 4 | 35% | Reassess | 2 | 1 | 4 | 25% | Reject | |
| Orbital Fat Pads | 5 | 4 | 5 | 77% | Retain | ||||||
| Mouth & Oral Cavity Exam | Dentures | 2 | 2 | 4 | 41% | Reassess | 4 | 1 | 4 | 75% | Retain |
| Perioral Areas | 4 | 3 | 5 | 53% | Retain | ||||||
| Angular Stomatitis/Cheilosis | 4 | 3 | 5 | 59% | Retain | ||||||
| Oral Ulcer/Lesions | 3 | 2 | 4 | 35% | Reassess | 4 | 2 | 4 | 69% | Retain | |
| Inspects Gums/Teeth | 4 | 3 | 5 | 53% | Retain | ||||||
| Inspects Buccal Mucosa | 3 | 2 | 4 | 29% | Reassess | 2 | 2 | 4 | 31% | Reject | |
| Inspects Tongue Filiform Papillary Atrophy | 3 | 3 | 5 | 47% | Reassess | 4 | 3 | 5 | 81% | Retain | |
| Magenta/Beefy Red Tongue | 4 | 3 | 5 | 53% | Retain | ||||||
| Glossitis | 4 | 3 | 4 | 53% | Retain | ||||||
| Inspects Uvula Midline Soft Palate Rising | 2 | 2 | 4 | 29% | Reassess | 2 | 1 | 3 | 25% | Reject | |
| Inspects Tongue Protrusion Movement | 2 | 2 | 5 | 29% | Reassess | 2 | 1 | 3 | 38% | Reject | |
| Neck Exam | Inspects Swallow | 2 | 2 | 5 | 29% | Reassess | 2 | 1 | 3 | 31% | Reject |
| Sternocleidomastoid Muscles Resistance | 2 | 1 | 4 | 24% | Reassess | 2 | 1 | 3 | 31% | Reject | |
| Trapezius Muscles Resistance | 2 | 2 | 4 | 35% | Reassess | 3 | 2 | 4 | 50% | Reject | |
| Inspects/Palpates Thyroid | 2 | 1 | 2 | 6% | Reassess | 2 | 1 | 2 | 6% | Reject | |
| Clavicular/Thoracic Region Exam | Palpates Pectoralis | 4 | 3 | 5 | 71% | Retain | |||||
| Inspects/Palpates Deltoids | 4 | 4 | 5 | 88% | Retain | ||||||
| Inspects Acromion Protrusion | 5 | 4 | 5 | 82% | Retain | ||||||
| Inspects/Palpates Intercostal Muscles | 4 | 3 | 5 | 71% | Retain | ||||||
| Palpates Muscles along Midaxillary Line | 4 | 2 | 5 | 53% | Retain | ||||||
| Inspects Iliac Crest Prominence | 4 | 3 | 5 | 53% | Retain | ||||||
| Abdomen Exam | Palpates Abdomen | 2 | 2 | 3 | 18% | Reassess | 2 | 1 | 3 | 38% | Reject |
| Percussion of Abdomen | 2 | 2 | 3 | 18% | Reassess | 2 | 1 | 3 | 38% | Reject | |
| Auscultation of Abdomen | 2 | 2 | 2 | 18% | Reassess | 2 | 1 | 3 | 25% | Reject | |
| Back/Scapular Region Exam | Examine Back Skin | 3 | 2 | 4 | 29% | Reassess | 3 | 2 | 4 | 50% | Reject |
| Inspects/Palpates Posterior Trapezius | 4 | 3 | 4 | 65% | Retain | ||||||
| Inspects/Palpates Scapula | 4 | 3 | 5 | 71% | Retain | ||||||
| Upper Extremities Exam | Skin exam on upper & lower arm | 3 | 3 | 5 | 47% | Reassess | 3 | 2 | 4 | 69% | Retain |
| Follicular Hyperkeratosis | 3 | 2 | 4 | 41% | Reassess | 3 | 2 | 4 | 69% | Retain | |
| Corkscrew Hair | 3 | 2 | 4 | 29% | Reassess | 3 | 2 | 4 | 69% | Retain | |
| Lanugo Hair | 3 | 2 | 4 | 29% | Reassess | 3 | 2 | 4 | 69% | Retain | |
| Palpates Triceps | 4 | 3 | 5 | 71% | Retain | ||||||
| Inspects Nail Color | 4 | 3 | 5 | 53% | Retain | ||||||
| Koilonychia | 4 | 3 | 5 | 53% | Retain | ||||||
| Beau’s Lines | 3 | 3 | 5 | 35% | Reassess | 3 | 2 | 4 | 63% | Retain | |
| Splinter Hemorrhage | 3 | 3 | 4 | 41% | Reassess | 3 | 2 | 4 | 63% | Retain | |
| Clubbing Nails | 3 | 3 | 4 | 47% | Reassess | 3 | 2 | 4 | 63% | Retain | |
| Capillary Refill | 3 | 2 | 4 | 41% | Reassess | 2 | 2 | 4 | 44% | Reject | |
| Inspects/Palpates Interosseous Muscles | 4 | 3 | 5 | 71% | Retain | ||||||
| Inspects/Palpates Thenar Muscles | 4 | 2 | 5 | 59% | Retain | ||||||
| Lower Extremities Exam | Inspects Petechiae | 3 | 2 | 5 | 35% | Reassess | 4 | 2 | 4 | 75% | Retain |
| Inspects Purpura | 3 | 2 | 4 | 29% | Reassess | 3 | 2 | 4 | 69% | Retain | |
| Inspects/Palpates Quadriceps | 5 | 4 | 5 | 76% | Retain | ||||||
| Inspects/Palpates Gastrocnemius | 5 | 4 | 5 | 76% | Retain | ||||||
| Inspects/Palpates Pitting Edema | 4 | 3 | 5 | 71% | Retain | ||||||
| Functional Grip Strength Exam | Handgrip dynamometer (objective measure) | 2 | 2 | 3 | 12% | Reassess | 2 | 2 | 3 | 38% | Reject |
| Handshake/Grip Fingers (subjective measure) | 3 | 2 | 5 | 41% | Reassess | 3 | 3 | 4 | 81% | Retain | |
| Bedside Manner & Etiquette | Bilateral Inspection & Palpation | 4 | 3 | 5 | 59% | Retain | |||||
| Respect Patient Privacy | 5 | 5 | 5 | 82% | Retain | ||||||
| Patient Dignity | 5 | 4 | 5 | 77% | Retain | ||||||
| Returns Patient Arms, Legs | 4 | 4 | 5 | 94% | Retain | ||||||
| Interviews Patient | 5 | 4 | 5 | 94% | Retain | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zechariah, S.; Waller, J.L.; De Leo, G.; Stallings, J.; Gess, A.J.; Lehman, L. Content and Face Validation of a Novel, Interactive Nutrition Specific Physical Exam Competency Tool (INSPECT) to Evaluate Registered Dietitians’ Competence: A Delphi Consensus from the United States. Healthcare 2021, 9, 1225. https://doi.org/10.3390/healthcare9091225
Zechariah S, Waller JL, De Leo G, Stallings J, Gess AJ, Lehman L. Content and Face Validation of a Novel, Interactive Nutrition Specific Physical Exam Competency Tool (INSPECT) to Evaluate Registered Dietitians’ Competence: A Delphi Consensus from the United States. Healthcare. 2021; 9(9):1225. https://doi.org/10.3390/healthcare9091225
Chicago/Turabian StyleZechariah, Sunitha, Jennifer L. Waller, Gianluca De Leo, Judith Stallings, Ashley J. Gess, and Leigh Lehman. 2021. "Content and Face Validation of a Novel, Interactive Nutrition Specific Physical Exam Competency Tool (INSPECT) to Evaluate Registered Dietitians’ Competence: A Delphi Consensus from the United States" Healthcare 9, no. 9: 1225. https://doi.org/10.3390/healthcare9091225